
Unbranded Rheumatoid Arthritis Booklet
11
© 2005 Bristol-Myers Squibb Company B5-D0003 5/05 Printed in USA Managing rheumatoid arthritis Seize the moment Discovering the Next Future ™ Discovering the Next Future ™ Crystal Kaczkowski writing sample
-
Upload
ckaczk -
Category
Health & Medicine
-
view
1.126 -
download
11
description
Unbranded Rheumatoid Arthritis Booklet written for BMS while working at Corbett Accel.
Transcript of Unbranded Rheumatoid Arthritis Booklet

© 2005 Bristol-Myers Squibb Company B5-D0003 5/05 Printed in USA
Managing rheumatoid arthritis
Seize the moment
Discovering the Next Future™ Discovering the Next Future™
Crystal
Kac
zkow
ski w
riting
sample

3
Diagnosis of RA can be difficult, particularly in theearly stages of the disease.1 Patients will often firstself-treat their symptoms before seeing a generalpractitioner (GP). Considering the subjective nature of RA symptoms, many GPs have difficultydetermining the etiology of the patient’s complaintsdue to their limited experience in diagnosis and management. Difficulties such as these may delaythe correct diagnosis of RA and subsequent treatment.3,4
According to one thought leader, the median timeto diagnosis of early RA is 18 weeks.4 Only 6% to14% of GPs refer patients to a rheumatologist within6 weeks. Most GPs refer new arthritic patients to arheumatologist within 3 months, but many wait torefer patients from 3 to 6 months.5 Thus, the majority of patients appear to be waiting longerthan they should for treatment, even though 70%of RA cases can be diagnosed by a rheumatologistwithin 2 weeks of the first visit.4 The AmericanCollege of Rheumatology (ACR) guidelines state thatthe majority of newly diagnosed patients should bestarted on DMARDs within 3 months of diagnosis.1
Considering the average delay before an RA patientreceives treatment, it is imperative for a physician,especially a rheumatologist, to diagnose RA as earlyas possible and initiate the appropriate treatment inorder to potentially reduce disease progression.7
Initial EvaluationThe initial RA patient evaluation may incorporateboth objective and subjective measures including1:
n physical examination
n laboratory tests
n radiography
n duration and degree of joint pain, morning stiffness, and fatigue
n actively inflamed joints (eg, synovitis)
n functional status
n mechanical joint problems
n extraarticular disease
Comorbidities and other assessments of active RAdamage should also be documented. Baseline datacan be collected regarding quality of life (QOL),patients’ and physicians’ pain assessments of diseaseactivity using visual analog scales (VAS), or othervalidated QOL measurement tools.1 There is growingevidence that these QOL measures, such as theStanford Health Assessment Questionnaire (HAQ),are correlated with underlying structural damageand long-term reduction in functional ability.8,9
A baseline laboratory assessment should include a complete blood cell count with white blood celldifferential and platelet counts; measurement oferythrocyte sedimentation rate (ESR) or C-reactiveprotein (CRP); and measurement of rheumatoid factor (RF). Hepatic and renal function should be
Establishing Diagnosis
RA treatment is often delayed
n Many patients wait >3 months from symptom onset to first GP appointment6
n Many patients wait >3 months for aspecialist referral6
n Only 6% to 14% of GPs refer patients toa rheumatologist within 6 weeks5
n DMARD therapy delayed even after seeinga specialist6
Crystal
Kac
zkow
ski w
riting
sample

54
evaluated since many antirheumatic agents can causetoxicity problems and would be contraindicated iforgans are impaired.1
Radiographs of the hands, feet, and other affectedjoints should be used to establish a baseline for futureassessment of structural damage.1
Estimating Prognosis
Creating a plan for treatment requires an estimateof prognosis. Earlier age of disease onset, elevatedESR, high titer of RF, and swelling of 20 or morejoints are associated with a poorer prognosis. Otherfactors that may be related to poor prognosisinclude: extraarticular manifestations of RA (eg,rheumatoid nodules), Sjögren’s syndrome, episcleritisand scleritis, interstitial lung disease, systemic vasculitis, pericardial involvement, and Felty’s syndrome.1
Studies have demonstratedthat patients with active polyarticular, RF-positive RA have more than a 70%chance of developing structural damage (joint damage or erosions) within 2 years. Because of this, it
is now widely accepted that aggressive treatmentshould be initiated as soon as diagnosis is madesince numerous studies have concluded that DMARDscan inhibit disease progression in patients with earlyRA. For those patients with unfavorable prognosticfactors, early DMARD treatment should be initiatedimmediately upon diagnosis.1
Baseline assessment of disease activityA patient’s prognosis is closely related to disease activityat onset since it has been shown that persistentinflammation of the joint leads to joint destruction.7
In early RA, analysis of the feet is critical since damageusually occurs there first.10 A consistent predictor oflater damage is the radiological score of the feetand/or hands in the first 3 years of disease.11,12
However, not all patients haveradiographic evidence of structualdamage in the first year.11
Predictive models to determineprogressive disease have beendeveloped based on some of theprognostic markers discussed inthe previous section12,13; however,there is a need for validation ofthese models in early and persistent RA.10
Radiographs are an important tool in establishing a diagnosis of RA and estimating baseline diseaseactivity/joint damage. Disease progression can be monitored with subsequent x-rays.
Ongoing Assessment of Disease Activity
The physician should assess whether the patient’sdisease is active or inactive at each follow-up visit.Symptoms of active disease, functional status, mechanical joint problems, presence of extraarticulardisease, and radiographic damage should be documented.1
Symptoms of inflammation including prolongedmorning stiffness, fatigue, and active synovitis onjoint examination indicate active disease and maynecessitate treatment modifications. Because theexamination of joints may not always adequatelygauge disease activity, periodic assessments of functional status, ESR or CRP measurement, and radiography should also be made.1
Functional status may be assessed by a questionnairesuch as the HAQ. The HAQ is an indicator of diseaseoutcome and severity. It is important to determinewhether a functional decline is due to inflammation,mechanical damage, or both. Strategies for treatment will differ according to the cause of the functional decline.1
While the ACR response criteria and the diseaseactivity score (DAS) are routinely used in clinical trialsto measure efficacy, these scales should not be usedas the only measure to monitor an individualpatient’s clinical response. A combination of clinical
Baseline evaluation of disease activity and damage1
Subjectiven Degree of joint painn Duration of morning stiffnessn Duration of fatiguen Limitation of function
Physical Examinationn Actively inflamed joints
(tender and swollen joint counts)n Mechanical joint problems: loss of motion,
crepitus, instability, malalignment,and/or deformity
n Extraarticular manifestations
Laboratoryn Erythrocyte sedimentation rate/C-reactive
protein leveln Rheumatoid factorn Complete blood cell countn Electrolyte levelsn Creatinine leveln Hepatic enzyme levels (AST, ALT, and albumin)n Urinalysisn Synovial fluid analysisn Stool guaiac
Othern Functional status or quality of life assessments
using standardized questionnairesn Physician’s Global Assessment of Disease Activityn Patient’s Global Assessment of Disease Activity
Radiographyn Radiographs of selected involved joints
Crystal
Kac
zkow
ski w
riting
sample
76
judgment and quantitative measures should be usedin addition to other validated measures such as1:
n VAS
n scales of global response or pain by the patient
n scales of global response by the physician
n joint tenderness and/or swelling
n laboratory data
These measures should be followed in each patient to gauge improvement. In addition to monitoringdisease activity and progression, a patient’s tolerance of adverse events (or side effects) andconcern of risks (such as infections) should beaddressed.14 Patients with an incomplete responseor who are intolerant of their medication may needa different treatment plan.15
Biomarkers that assess ongoing disease activityWith the advent of new treatment strategies and therapeutic options, there is a need for a predictivemodel for use in clinical practice in order to designthe most appropriate therapeutic strategy for patientsin early and persistent RA. The ideal prognostic indexwould include reliable markers such as10:
n RF (positivity and titer)
n radiographic scores within the first year of disease onset
n HAQ
n CRP or ESR
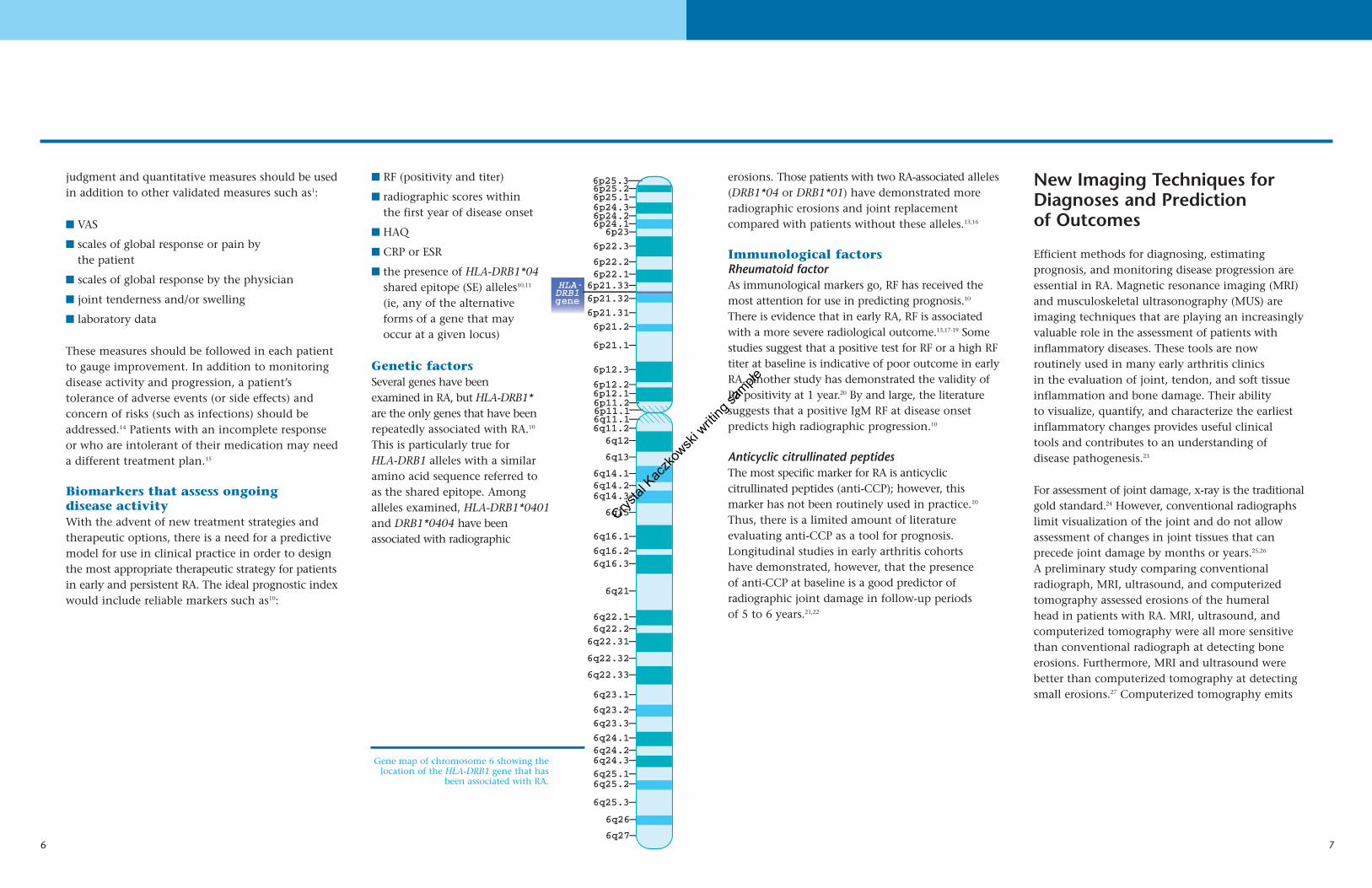
n the presence of HLA-DRB1*04shared epitope (SE) alleles10,11
(ie, any of the alternative forms of a gene that may occur at a given locus)
Genetic factorsSeveral genes have been examined in RA, but HLA-DRB1*are the only genes that have beenrepeatedly associated with RA.10
This is particularly true for HLA-DRB1 alleles with a similar amino acid sequence referred to as the shared epitope. Among alleles examined, HLA-DRB1*0401and DRB1*0404 have been associated with radiographic
erosions. Those patients with two RA-associated alleles(DRB1*04 or DRB1*01) have demonstrated moreradiographic erosions and joint replacement compared with patients without these alleles.13,16
Immunological factorsRheumatoid factorAs immunological markers go, RF has received themost attention for use in predicting prognosis.10
There is evidence that in early RA, RF is associatedwith a more severe radiological outcome.13,17-19 Somestudies suggest that a positive test for RF or a high RFtiter at baseline is indicative of poor outcome in earlyRA. Another study has demonstrated the validity ofRF positivity at 1 year.20 By and large, the literaturesuggests that a positive IgM RF at disease onset predicts high radiographic progression.10
Anticyclic citrullinated peptidesThe most specific marker for RA is anticyclic citrullinated peptides (anti-CCP); however, this marker has not been routinely used in practice.10
Thus, there is a limited amount of literature evaluating anti-CCP as a tool for prognosis.Longitudinal studies in early arthritis cohorts have demonstrated, however, that the presence of anti-CCP at baseline is a good predictor of radiographic joint damage in follow-up periods of 5 to 6 years.21,22
New Imaging Techniques forDiagnoses and Prediction of Outcomes
Efficient methods for diagnosing, estimating prognosis, and monitoring disease progression areessential in RA. Magnetic resonance imaging (MRI)and musculoskeletal ultrasonography (MUS) areimaging techniques that are playing an increasinglyvaluable role in the assessment of patients withinflammatory diseases. These tools are now routinely used in many early arthritis clinics in the evaluation of joint, tendon, and soft tissueinflammation and bone damage. Their ability to visualize, quantify, and characterize the earliestinflammatory changes provides useful clinical tools and contributes to an understanding of disease pathogenesis.23
For assessment of joint damage, x-ray is the traditionalgold standard.24 However, conventional radiographslimit visualization of the joint and do not allowassessment of changes in joint tissues that can precede joint damage by months or years.25,26
A preliminary study comparing conventional radiograph, MRI, ultrasound, and computerizedtomography assessed erosions of the humeral head in patients with RA. MRI, ultrasound, andcomputerized tomography were all more sensitivethan conventional radiograph at detecting boneerosions. Furthermore, MRI and ultrasound werebetter than computerized tomography at detectingsmall erosions.27 Computerized tomography emits
Gene map of chromosome 6 showing thelocation of the HLA-DRB1 gene that has
been associated with RA.
6p21.33— HLA- DRB1 gene 6p21.32—
6p22.1—6p22.2—
6p22.3—6p23—
6p24.1—6p24.2—6p24.3—6p25.1—6p25.2—6p25.3—
6p21.31—6p21.2—
6p21.1—
6p12.3—
6p12.2—6p12.1—6p11.2—6p11.1—6q11.1—6q11.2—
6q12—
6q13—
6q14.1—6q14.2—6q14.3—
6q15—
6q16.1—
6q16.2—6q16.3—
6q21—
6q22.1—6q22.2—6q22.31—
6q22.32—
6q22.33—
6q23.1—
6q23.2—6q23.3—
6q24.1—6q24.2—6q24.3—6q25.1—6q25.2—
6q25.3—
6q26—
6q27—
Crystal
Kac
zkow
ski w
riting
sample

98
ionizing radiation28 and its sensitivity to detect small erosive changes is inferior toMRI or MUS27,28; thus, it is rarelyused in clinical practice.
Magnetic resonanceimagingMagnetic resonance imaging ofthe joints has stimulated greatinterest as a research tool.29 Themain advantage of MRI is that itallows 3-dimensional assessmentof a large number of anatomicalstructures in and around a joint.23
The multiplanar properties of MRI and its ability to identify small cortical defects allow superior sensitivity to conventional radiography for detecting bone erosions.23 MRI can assess osseouschanges and has the ability to visualize soft tissuewith high spatial resolution and good contrast.25,29
The increased popularity of MRI is a result of betteraccess, reduction in cost, and developments in resolution, sequences, and software. It is contended thatthese features make MRI an ideal technique for detecting the earliest pathological changesassociated with inflammatoryarthritis.23 Furthermore, there is evidence that using MRI inpatients with early RA can assist in identifying those withaggressive disease.30,31
UltrasoundTraditional MUS has been used for some time for detecting joint and soft tissue inflammation.32 It hasalso been described as the gold standard imaging technique for evaluating tendon involvement in rheumatic diseases.33 Morerecent MUS techniques, suchas Doppler, have shown promise for assessing patientswith inflammation. Doppler is a technique that makes
noninvasive measurements of blood flow. PowerDoppler is valuable for assessing low-velocity vascular flow in small vessels such as the synovium. Therefore, it can measure and detectchanges in the vascularity of joints and soft tissuedue to inflammation.32 A study in patients withinflammatory arthritis proposes that MUS may evenhave more sensitivity than MRI for the detection ofsynovitis in finger joints.34 However, further
validation is required regarding the potential use ofultrasound in early RA.23 There are still very limiteddata regarding the diagnostic and prognostic valueof ultrasound, as well as areas such as the monitoringof joint inflammation and destruction. Ultrasound is a more accessible, lower-in-cost, and patient-friendlytechnology than MRI.35 In the near future, it maybecome a routinely used clinical tool for therheumatologist.36
Certainly, the fact that rheumatoid activity anddamage can be imaged and measured in new ways using MRI and ultrasound opens a new frontierin disease management for rheumatologists.Opportunities for clinical practice include earlierand more accurate diagnoses and meticulous evaluation of therapeutic response. These techniques provide optimal opportunities fordisease control.7,35 There are technical challenges,however, with MRI and ultrasound, for instance, instandardizing scoring systems.23,29,30,36,37 A thoroughvalidation of MRI findings as a substitute for radiographic outcome measures is required beforeroutine use in clinical trials is recommended. Butthese tools have a possible future in the diagnosisand management of RA.
The advantages and disadvantages ofMRI and ultrasound35
A sonogram of the wrist produced by ultrasound can beused as a diagnostic tool for RAand to monitor ongoing diseaseprogression.
MRI of a hand early in the RA diseaseprocess. Edema is apparent on the thirdand fourth metacarpophalangeal jointsindicating inflammation and diseaseactivity. Reproduced with permission from the Arthritis Research Campaign(www.arc.org.uk).
Advantages Disadvantages
n Safe
n No ionizing radiation
n No increased risk ofmalignancies
n Allergic reactions tocontrast agents are rare
n Higher costs thanradiography
n Less availability thanradiography
n Longer examinationtime
n Evaluation of only afew joints per session
n Time required to evaluate an MRI examination
n Physical limitations(ie, not all areas areaccessible, thus wholejoint assessment israrely possible)
n Dependency on askilled operator
n Poor objective documentation of findings
n Noninvasive
n Relatively inexpensive
n No ionizing radiation
n Ability to visualizeboth inflammatoryand destructive disease mechanisms
n Easily repeated
n Possibility of examining severaljoints in 1 session
n Potential for being performed byrheumatologists inoutpatient clinics
n Potential for guidinginterventions
MR
IU
ltra
sou
nd
Crystal
Kac
zkow
ski w
riting
sample

1110
RemissionThe notion of setting remission as a treatment goalfor RA is becoming more prominent within clinicalsettings.9 The challenge of introducing remission asthe standard goal of treatment lies in establishing auniversally accepted definition that can be easilyassessed and is accurately quantified. It is essentialto define the point at which disease activity hasbeen stably reduced or repressed sufficiently.Furthermore, in order to set remission as a studyendpoint within a clinical trial, concise criteria thatcan be easily measured and provide reliable datamust be identified.8,40,42,43
Currently, there is much discussion on what constitutesremission in RA. For many years, major clinicalstudies had equated a response of ACR 70 orgreater40 and/or a DAS28 score less than 2.6 with a state of remission.43 Another recently introduced measure is the major clinical response (MCR), inwhich a response of an ACR 70 or greater is maintained for at least 6 consecutive months.44
Previous studies have traditionally reserved responsesof ACR 70 or DAS28 <2.6 as secondary endpoints,using ACR 20 and ACR 50 criteria as the primarymeasurements to indicate clinical efficacy. Recent statistics demonstrating an increased probability ofwork disability in patients only achieving responses of ACR 20 or ACR 50, but never experiencing ACR 70, suggest that ACR 20 and ACR 50 are notadequate responses and, therefore, not reliablyreflective of treatment efficacy. There has been
some suggestion that the standard primary endpoint of RA clinical trials should be a responseof ACR 70 or greater to more accurately indicatetreatment efficacy.9
In addition to the discussion over which accumulativemeasurement should be used to indicate a state ofremission, there is also debate over which core criteria most accurately reflect the degree of diseaseprogression.8,9,43 Some experts argue that, althoughswollen joint counts and tender joint counts areimportant indicators of disease activity, only radiographic analysis can provide objective evidenceof joint degradation and true disease progression.8,9
Neither ACR nor DAS standards include radiographicassessment in their core analytical criteria. Advocatesof more advanced methods of visualizing diseaseactivity suggest that even more sensitive methods,such as MRI, be utilized to better detect early erosionsand pre-erosive inflammation that cannot be seenon early radiographs.26
Achieving remission for more RA patients is becomingincreasingly possible with the introduction ofDMARDs. With the reality of remission, however,comes the necessity to identify the most accurate criteria for monitoring treatment efficacy and measuring patient success so that remission can betargeted and measured as a new treatment goal.
From a physician’s perspective, goals central to thetreatment of RA include decreasing pain, preventingloss of function, improving QOL, and inhibitingstructural damage.1,38 While patients may benefit fromthe outcomes of these goals, they often rate the following symptoms as most important: functionalability, pain, cognition, gastrointestinal side effects,fatigue, and sleep.39 Since RA is a complex, chronicautoimmune disease that is prone to periods ofincreasing and decreasing severity, patient involvement in the development of a long-term treatment plan is important for improving outcomes.Key opinion leaders recommend that physicians andpatients should first discuss treatment options.Discussions should revolve around1:
n the patient’s prognosis and treatment options
n associated costs
n possible adverse effects
n when the patient may expect a response
n risk factors
n comorbid conditions
n what drug monitoring is needed
n patient preferences
n patient expectations of treatment
n potential barriers to treatment recommendations
Current therapeutic options allow physicians theability to treat RA patients at any stage of disease.Although early intervention is important, so isassessing the efficacy of treatment and controllingdisease long term for patients with more advanceddisease or who are nonresponsive to therapy.
While efficacy is critical for successful clinical outcomes, good tolerability is also important. Thus, both safety and tolerability should be monitoredas patients progress on therapy.
Treatment Goals
Common definitions of remission in RA40,41
ACR DAS28
Def
init
ion
Futu
re
Originally defined in 1981. These criteria are still preliminary. The ACR definition has been criticized for being too stringent, since few patientsachieve remission by these criteria.
The DAS28 criteria for remission arebecoming widely used in today’s clinicaltrials. The DAS28 is considered to be lessrestrictive than the ACR definition forremission.
n 28 tender joint counts
n 28 swollen joint counts
n Patient global assessment of disease activity
n ESR or CRP
n No fatigue
n No joint pain
n Normal ESR
n No tender joints
n No swollen joints
n Morning stiffness<15 minutes
5 of the following for at least 2 months:
DAS28 <2.6DAS28 score calculated from:
Crystal
Kac
zkow
ski w
riting
sample

The guidelines for RA treatment are as follows1:
n Establish diagnosis of RA early
n Document baseline disease activity and damage
n Estimate prognosis
Periodically assess disease activity
Rh
eum
atol
ogis
t
Prim
ary
Car
e Ph
ysic
ian
Change/Add DMARDs
Multiple DMARD failure
Surgery
Symptomatic and/or structural joint damage
MTX* naive
Other mono Rx
MTX Combination Rx
Suboptimal MTX response
Other mono Rx
Combination Rx
Biologics
Mono Rx Combination Rx
Adequate response with decreased disease activity
Inadequate response (ie, ongoing
active disease after 3 months of
maximal therapy)
Initiate therapy
n Patient education
n Start DMARD(s) within 3 months
n Consider NSAID
n Consider local or low-dose systemic steroids
n Physical therapy/occupational therapy
1312
Pharmacological Options
Since preventing loss of function, decreasing pain,improving patient QOL, and inhibiting structuraldamage are central goals of treatment, drug therapyshould be tailored to achieve these outcomes. Inaddition, some things to be considered when selecting a medication include the ability to deliveran adequate response, the incidence and seriousnessof adverse events, and the likelihood of patient compliance.1 Therapies that achieve an ideal balanceof efficacy, safety, and tolerability deliver true clinical effectiveness.
In order to achieve optimal patient outcomes, pharmacological therapy usually consists of a combination of NSAIDS, DMARDs, and/or steroids(corticosteroids).1
NSAIDsThese drugs reduce inflammation and have analgesicproperties, but they do not prevent joint destructionor alter the disease course.1
Steroids Corticosteroids work quickly to alleviate damagingand painful inflammation. They are associated withpotential side effects like brittle bones, cataracts, andelevated blood sugar, especially if they are taken inhigh doses or over the long term. Inflammationmay be controlled in a few affected joints by injecting a corticosteroid compound directly into inflamed joint(s).38
DMARDsAlthough NSAIDs and corticosteroids may reduceinflammation and alleviate pain, they do not interfere
with RA immunopathology. However, DMARDshave the ability to alter the disease through reductionor prevention of joint damage, and preservation ofjoint integrity and function.1
All RA patients are considered candidates for DMARDtherapy. DMARD therapy should be initiated within3 months in patients with confirmed diagnoses whocontinue to have the following symptoms despiteadequate NSAID treatment1:
n ongoing joint pain
n considerable morning stiffness or fatigue
n active synovitis
n continuous elevation of ESR or CRP levels
n radiographic joint damage
Any untreated patient with persistent synovitis andjoint damage should be immediately started onDMARD treatment to prevent or slow further damage.1
TraditionalTraditional DMARDs have been used in RA therapyto successfully reduce inflammation and associatedsymptoms.1,45
Rheumatologists often select traditional DMARDtherapy initially, especially for patients with moreactive disease.1
Biologic DMARDs Six years ago, if a patient had RA and did notrespond to traditional DMARDs, there was little arheumatologist could do. Today there is the optionof biologic DMARDs.
Treatment Options
*MTX = Methotrexate
Crystal
Kac
zkow
ski w
riting
sample
1514
Biologic DMARDs continuedCurrent guidelines recommend a combination ofNSAIDs, corticosteroids, and early introduction of bothtraditional and biologic DMARDs. The more recentavailability of targeted therapeutics for the treatment ofRA has led to a significant difference in the ability toinhibit disease progression and improve patientresponse and quality of life. Moreover, it has openedthe door for major advances in the treatment of RAand led to more aggressive treatment guidelines.1
The American College of Rheumatology’s most recentposition statement dictates that, when clinically appropriate, all patients with serious rheumatic diseasemust have these biologic agents.46
Although the genetically engineered biologicDMARDs all work in different ways, they all block proteins called cytokines, which contribute toinflammation.38 This development has been a majoradvance in RA treatment.
Some of the most effective anticytokine drugs are antagonists to TNFα, which is a critical mediator ofthe RA inflammatory cascade. Clinical trials have shownthese drugs improve clinical signs and symptoms, measured by ACR 20, 50, and/or 70 scores. These drugshave demonstrated efficacy in combination therapy withtraditional DMARDs when administered to patients withongoing active RA despite sufficient doses.1
The use of traditional DMARDs and the introduction of the biologic DMARDs have begun to redefine expectations for the effectiveness of RA therapies.1,47
DMARDs have allowed physicians to go beyond just treating symptoms and start inhibiting diseaseprogression and joint destruction, while also preserving joint function.1
Advances in biologic treatments for autoimmune disease have set a new standard for RA therapy, andelaborate research of immune pathways has led to amore intricate understanding of RA immunopathology.As a result, potential new therapeutic targets withinRA immunopathology, such as IL-6, B cells, and T-cell activation, have been investigated. Hopefully,new alternatives will be identified to stop disease progression and prevent permanent disability whilepreserving patient immune response.47
Nonpharmacological optionsOptimum treatment requires more than just drug therapy. Sometimes, RA patients may require periodsof rest, job modification or time off from work, achange of occupation, or termination of work altogether. Patients will likely benefit from instructionin joint protection, energy conservation, and creationof a home exercise program (joint range of motionand strength exercises).1
Treatment starts with educating the patient about thedisease. Patients will have to learn to live with RA andbecome involved in the treatment processdecisions. Emotional difficulties may ariseif treatment does not fully control thischronic disease. The patient should bemade aware that RA is associated with
flares and concomitant loss of function. Cognitive-behavioral programs that help patients take a greaterrole in their disease management can improve patienthealth and reduce health care utilization.1
The risks and benefits of existing treatment plansshould also be reviewed with the patient. The healthcare team may use an interdisciplinary approach.Rheumatologists, primary care physicians, nurses, andother health care staff members often play a significantrole in educating patients and their families about thedisease and how to offer long-term supportive care.
Patients may find consultations withphysical therapists, occupational therapists, patient educators, andsocial workers beneficial.1,38
Low-impact exercises such as pool therapy are beneficial for RA patients asnonpharmacological treatment options.
Crystal
Kac
zkow
ski w
riting
sample
1716
Advances in RA treatment are allowing physiciansto provide better patient care than ever before, ushering in an unprecedented era of optimism andsuccess. It is now acknowledged that treating patientsearly and aggressively with new therapies such asTNFα inhibitors is essential for optimal care, andcan potentially slow or even prevent permanentjoint damage.
With this success, however, have come new challengesand issues for rheumatologists. New technologicaladvancements such as MRI and ultrasound aremaking the diagnosis of RA possible earlier thanever with more accurate prognoses by permittingrheumatologists to detect pathological changes injoints before they appear on traditional radiographs.
These new technologies may also enhance the abilityto assess disease progression and activity with moreaccuracy than heretofore possible. The role of biologic markers in diagnosis and prognosis is also being clarified with more research and clinicalexperience. Remission is now a viable treatmentgoal, and a consensus is beginning to emerge onwhat constitutes a remissive state. As cliniciansaddress the meaning of adequate and inadequateresponse with the new class of biologic DMARDs,questions such as when to switch biologic agentsand how to determine optimal treatment alternativesare being investigated, taking into considerationsuch factors as mechanism of action and side effectand tolerability profile. The practice of rheumatologyhas never been more exciting.
References:1. American College of Rheumatology Subcommittee
on Rheumatoid Arthritis Guidelines. Guidelines forthe management of rheumatoid arthritis: 2002update. Arthritis Rheum. 2002;46:328-346.
2. Anderson JJ, Wells G, Verhoeven AC, Felson DT.Factors predicting response to treatment in rheumatoid arthritis: the importance of disease duration. Arthritis Rheum. 2000;43:22-29.
3. Rat AC, Henegariu V, Boissier MC. Do primary care physicians have a place in the management of rheumatoid arthritis? Joint Bone Spine.2004;71:190-197.
4. Emery P, Breedveld FC, Dougados M, Kalden JR,Schiff MH, Smolen JS. Early referral recommendationfor newly diagnosed rheumatoid arthritis: evidencebased development of a clinical guide. Ann RheumDis. 2002;61:290-297.
5. Aletaha D, Eberl G, Nell VP, Machold KP, Smolen JS.Practical progress in realisation of early diagnosisand treatment of patients with suspected rheumatoid arthritis: results from two matched questionnaires within three years. Ann Rheum Dis.2002;61:630-634.
6. Potter T, Mulherin D, Pugh M. Early interventionwith disease-modifying therapy for rheumatoidarthritis: where do the delays occur? Rheumatology(Oxford). 2002;41:953-955.
7. Emery P, Seto Y. Role of biologics in early arthritis.Clin Exp Rheumatol. September 2003;21(suppl31):S191-S194.
8. Scott DL. Pursuit of optimal outcomes in rheumatoidarthritis. Pharmacoeconomics. 2004;22(suppl 2):13-26.
9. Pincus T, Sokka T, Kavanaugh A. Relative versusabsolute goals of therapies for RA: ACR 20 or ACR 50responses versus target values for “near remission” ofDAS or single measures. Clin Exp Rheumatol.September 2004;22(suppl 35):S50-S56.
10. Morel J, Combe B. How to predict prognosis in earlyrheumatoid arthritis. Best Pract Res Clin Rheumatol.2005;19:137-146.
11. Dixey J, Solymossy C, Young A. Is it possible to predict radiological damage in early rheumatoidarthritis (RA)? A report on the occurrence, progression,and prognostic factors of radiological erosions overthe first 3 years in 866 patients from the Early RAStudy (ERAS). J Rheumatol Suppl. 2004;69:48-54.
12. Visser H, le Cessie S, Vos K, Breedveld FC, Hazes JM.How to diagnose rheumatoid arthritis early: a prediction model for persistent (erosive) arthritis.Arthritis Rheum. 2002;46:357-365.
13. Combe B, Dougados M, Goupille P, et al. Prognosticfactors for radiographic damage in early rheumatoidarthritis: a multiparameter prospective study.Arthritis Rheum. 2001;44:1736-1743.
14. Braun J, Sieper J, van der Heijde D. Definition of discontinuation of anti-tumour necrosis factor therapy in rheumatoid arthritis: a preliminary proposal. Ann Rheum Dis. 2003;62:1023-1024.
15. Furst DE, Keystone EC, Breedveld FC, et al. Updated consensus statement on tumour necrosis factorblocking agents for the treatment of rheumatoidarthritis and other rheumatic diseases. Ann RheumDis. 2001;60(suppl 3):iii2-iii5.
16. Weyand CM, Hicok KC, Conn DL, Goronzy JJ. Theinfluence of HLA-DRB1 genes on disease severity inrheumatoid arthritis. Ann Intern Med. 1992;117:801-806.
17. Brennan P, Harrison B, Barrett E, et al. A simple algorithm to predict the development of radiologicalerosions in patients with early rheumatoid arthritis:prospective cohort study. BMJ. 1996;313:471-476.
18. Paimela L, Palosuo T, Leirisalo-Repo M, Helve T, AhoK. Prognostic value of quantitative measurement ofrheumatoid factor in early rheumatoid arthritis. Br JRheumatol. 1995;34:1146-1150.
Future Directions
Crystal
Kac
zkow
ski w
riting
sample
18
19. Young A, Corbett M, Winfield J, et al. A prognosticindex for erosive changes in the hands, feet, and cervical spines in early rheumatoid arthritis. Br JRheumatol. 1988;27:94-101.
20. Mottonen T, Paimela L, Leirisalo-Repo M, KautiainenH, Ilonen J, Hannonen P. Only high disease activityand positive rheumatoid factor indicate poor prognosis in patients with early rheumatoid arthritistreated with “sawtooth” strategy. Ann Rheum Dis.1998;57:533-539.
21. Meyer O, Labarre C, Dougados M, et al. Anticitrullinatedprotein/peptide antibody assays in early rheumatoidarthritis for predicting five year radiographic damage.Ann Rheum Dis. 2003;62:120-126.
22. Kroot EJ, de Jong BA, van Leeuwen MA, et al. The prognostic value of anti-cyclic citrullinated peptideantibody in patients with recent-onset rheumatoidarthritis. Arthritis Rheum. 2000;43:1831-1835.
23. Brown AK, Wakefield RJ, Conaghan PG, Karim Z,O’Connor PJ, Emery P. New approaches to imagingearly inflammatory arthritis. Clin Exp Rheumatol.September 2004;22(suppl 35):S18-S25.
24. Brower AC. Use of the radiograph to measure thecourse of rheumatoid arthritis: the gold standard versus fool’s gold. Arthritis Rheum. 1990;33:316-324.
25. Foley-Nolan D, Stack JP, Ryan M, et al. Magnetic resonance imaging in the assessment of rheumatoidarthritis: a comparison with plain film radiographs. Br J Rheumatol. 1991;30:101-106.
26. Peterfy CG. MRI of the wrist in early rheumatoidarthritis. Ann Rheum Dis. 2004;63:473-477.
27. Alasaarela E, Suramo I, Tervonen O, Lahde S, TakaloR, Hakala M. Evaluation of humeral head erosions in rheumatoid arthritis: a comparison of ultrasonography, magnetic resonance imaging, computed tomography and plain radiography. Br J Rheumatol. 1998;37:1152-1156.
28. Ghozlan R, Vacher H. Where is imaging going inrheumatology? Baillieres Best Pract Res ClinRheumatol. 2000;14:617-633.
29. Goldbach-Mansky R, Mahadevan V, Yao L, Lipsky PE.The evaluation of bone damage in rheumatoidarthritis with magnetic resonance imaging. Clin ExpRheumatol. September 2003;21(suppl 31):S50-S53.
30. McQueen FM. Magnetic resonance imaging in earlyinflammatory arthritis: what is its role? Rheumatology(Oxford). 2000;39:700-706.
31. Ostergaard M, Hansen M, Stoltenberg M, et al. Newradiographic bone erosions in the wrists of patientswith rheumatoid arthritis are detectable with magneticresonance imaging a median of two years earlier.Arthritis Rheum. 2003;48:2128-2131.
32. Wakefield RJ, Brown AK, O’Connor PJ, Emery P. PowerDoppler sonography: improving disease activity assessment in inflammatory musculoskeletal disease.Arthritis Rheum. 2003;48:285-288.
33. Grassi W, Filippucci E, Farina A, Cervini C.Sonographic imaging of tendons. Arthritis Rheum.2000;43:969-976.
34. Backhaus M, Kamradt T, Sandrock D, et al. Arthritisof the finger joints: a comprehensive approach comparing conventional radiography, scintigraphy,ultrasound, and contrast-enhanced magnetic resonanceimaging. Arthritis Rheum. 1999;42:1232-1245.
35. Ostergaard M, Ejbjerg B, Szkudlarek M. Imaging inearly rheumatoid arthritis: roles of magnetic resonance imaging, ultrasonography, conventionalradiography and computed tomography. Best PractRes Clin Rheumatol. 2005;19:91-116.
36. Manger B, Kalden JR. Joint and connective tissue ultrasonography—a rheumatologic bedside procedure? A German experience. Arthritis Rheum.1995;38:736-742.
37. McQueen FM, Benton N, Crabbe J, et al. What is the fate of erosions in early rheumatoid arthritis?Tracking individual lesions using x rays and magneticresonance imaging over the first two years of disease.Ann Rheum Dis. 2001;60:859-868.
Crystal
Kac
zkow
ski w
riting
sample
Rheumatoid arthritis (RA) is a systemic autoimmune disorder of unknown etiology that is characterized by symmetric, erosive synovitis, and often extraarticular symptoms. Despite therapy, most patients experience a chronic, fluctuating disease course that may result in progressive joint destruction, deformity and disability, and even premature death.1 For these reasons, early diagnosisand treatment of RA is critical. Research has shownthat patients who present quickly to a rheumatologistafter symptom onset have better outcomes than thosewho delay treatment.2 With the advent of therapiessuch as biologic disease-modifying antirheumaticdrugs (DMARDs), the opportunity to intervene earlier has never been more promising. With this
new opportunity, however, havecome new questions regarding the management of RA.
2
38. The Arthritis Foundation. The Arthritis Foundation2004. Available at: http://www.arthritis.org. AccessedJanuary 20, 2005.
39. Wolfe F, Michaud K. Fatigue, rheumatoid arthritis,and anti-tumor necrosis factor therapy: an investigation in 24,831 patients. J Rheumatol.2004;31:2115-2120.
40. Paulus HE. Defining remission in rheumatoid arthritis: what is it? Does it matter? J Rheumatol.2004;31:1-4.
41. Department of Rheumatology, University MedicalCenter Nijmegan, the Netherlands. Available at:http://www.das-score_nl/www.das-score.nl/. Accessed April 27, 2005.
42. Cohen MD. Raising expectations for arthritis treatment: biologic response modifiers are makingremission possible. Postgrad Med. 2004;116:41-50.
43. Balsa A, Carmona L, Gonzalez-Alvaro I, BelmonteMA, Tena X, Sanmarti R. Value of Disease ActivityScore 28 (DAS28) and DAS28-3 compared toAmerican College of Rheumatology-defined remission in rheumatoid arthritis. J Rheumatol.2004;31:40-46.
44. Food and Drug Administration. Guidance for industry.Clinical development programs for drugs, devices, and biological products for the treatment of rheumatoid arthritis. Rockville, Md: Food and DrugAdministration; 1999.
45. Smolen JS, Steiner G. Therapeutic strategies forrheumatoid arthritis. Nat Rev Drug Discov. 2003;2:473-488.
46. American College of Rheumatology. New agents forarthritis. Available at:http://www.rheumatology.org/publications/position/dmard.asp?aud=mem. Accessed January 25, 2005.
47. Choy EH, Panayi GS. Cytokine pathways and jointinflammation in rheumatoid arthritis. N Engl J Med.2001;344:907-916.
19
MOMENTS of CHANGE
Issues in the Next Future of RA
Managing rheumatoid arthritis:diagnosis, treatment,and future directions
Crystal
Kac
zkow
ski w
riting
sample








