Umbilical Cord Milking Versus Delayed Cord Clamping in Preterm … · which the unclamped umbilical...
11
Umbilical Cord Milking Versus Delayed Cord Clamping in Preterm Infants Anup C. Katheria, MD a , Giang Truong, MD b , Larry Cousins, MD c , Bryan Oshiro, MD d , Neil N. Finer, MD a abstract BACKGROUND AND OBJECTIVE: Delayed cord clamping (DCC) is recommended for premature infants to improve blood volume. Most preterm infants are born by cesarean delivery (CD), and placental transfusion may be less effective than in vaginal delivery (VD). We sought to determine whether infants ,32 weeks born by CD who undergo umbilical cord milking (UCM) have higher measures of systemic blood flow than infants who undergo DCC. METHODS: This was a 2-center trial. Infants delivered by CD were randomly assigned to undergo UCM or DCC. Infants delivered by VD were also randomly assigned separately. UCM (4 strippings) or DCC (45–60 seconds) were performed. Continuous hemodynamic measurements and echocardiography were done at site 1. RESULTS: A total of 197 infants were enrolled (mean gestational age 28 6 2 weeks). Of the 154 infants delivered by CD, 75 were assigned to UCM and 79 to DCC. Of the infants delivered by CD, neonates randomly assigned to UCM had higher superior vena cava flow and right ventricular output in the first 12 hours of life. Neonates undergoing UCM also had higher hemoglobin, delivery room temperature, blood pressure over the first 15 hours, and urine output in the first 24 hours of life. There were no differences for the 43 infants delivered by VD. CONCLUSIONS: This is the first randomized controlled trial demonstrating higher systemic blood flow with UCM in preterm neonates compared with DCC. UCM may be a more efficient technique to improve blood volume in premature infants delivered by CD. WHAT’S KNOWN ON THIS SUBJECT: Delayed cord clamping is recommended for all premature births, despite some studies suggesting a decreased placental transfusion at cesarean delivery. WHAT THIS STUDY ADDS: Umbilical cord milking appears to improve systemic blood flow and perfusion in preterm infants delivered by cesarean delivery more efficiently than delayed cord clamping. a Neonatal Research Institute and c San Diego Perinatology, Sharp Mary Birch Hospital for Women and Newborns, San Diego, California; Departments of b Pediatrics, and d Obstetrics, Loma Linda Medical University, Loma Linda, California Dr Katheria conceptualized and designed the study, drafted the initial manuscript, designed the data collection instruments, and coordinated and supervised data collection at two of the sites; Drs Truong, Cousins, Oshiro, and Finer carried out the initial analyses and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted. This trial has been registered at clinicaltrials.gov (identifier NCT01866982). www.pediatrics.org/cgi/doi/10.1542/peds.2015-0368 DOI: 10.1542/peds.2015-0368 Accepted for publication Apr 20, 2015 Address correspondence to Anup C. Katheria, MD, Neonatal Research Institute at Sharp Mary Birch Hospital for Women and Newborns, 8555 Aero Dr, Suite 104, San Diego, CA 92123. E-mail: anup. [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics PEDIATRICS Volume 136, number 1, July 2015 ARTICLE by guest on October 7, 2020 www.aappublications.org/news Downloaded from
Transcript of Umbilical Cord Milking Versus Delayed Cord Clamping in Preterm … · which the unclamped umbilical...

Umbilical Cord Milking Versus DelayedCord Clamping in Preterm InfantsAnup C. Katheria, MDa, Giang Truong, MDb, Larry Cousins, MDc, Bryan Oshiro, MDd, Neil N. Finer, MDa
abstractBACKGROUND AND OBJECTIVE: Delayed cord clamping (DCC) is recommended for premature infantsto improve blood volume. Most preterm infants are born by cesarean delivery (CD),and placental transfusion may be less effective than in vaginal delivery (VD). Wesought to determine whether infants ,32 weeks born by CD who undergo umbilicalcord milking (UCM) have higher measures of systemic blood flow than infants whoundergo DCC.
METHODS: This was a 2-center trial. Infants delivered by CD were randomly assigned toundergo UCM or DCC. Infants delivered by VD were also randomly assigned separately.UCM (4 strippings) or DCC (45–60 seconds) were performed. Continuous hemodynamicmeasurements and echocardiography were done at site 1.
RESULTS: A total of 197 infants were enrolled (mean gestational age 28 6 2 weeks). Of the 154infants delivered by CD, 75 were assigned to UCM and 79 to DCC. Of the infants delivered byCD, neonates randomly assigned to UCM had higher superior vena cava flow and rightventricular output in the first 12 hours of life. Neonates undergoing UCM also had higherhemoglobin, delivery room temperature, blood pressure over the first 15 hours, and urineoutput in the first 24 hours of life. There were no differences for the 43 infants delivered byVD.
CONCLUSIONS: This is the first randomized controlled trial demonstrating higher systemic bloodflow with UCM in preterm neonates compared with DCC. UCM may be a more efficienttechnique to improve blood volume in premature infants delivered by CD.
WHAT’S KNOWN ON THIS SUBJECT: Delayed cordclamping is recommended for all prematurebirths, despite some studies suggestinga decreased placental transfusion at cesareandelivery.
WHAT THIS STUDY ADDS: Umbilical cord milkingappears to improve systemic blood flow andperfusion in preterm infants delivered bycesarean delivery more efficiently than delayedcord clamping.
aNeonatal Research Institute and cSan Diego Perinatology, Sharp Mary Birch Hospital for Women and Newborns,San Diego, California; Departments of bPediatrics, and dObstetrics, Loma Linda Medical University, Loma Linda,California
Dr Katheria conceptualized and designed the study, drafted the initial manuscript, designed thedata collection instruments, and coordinated and supervised data collection at two of the sites;Drs Truong, Cousins, Oshiro, and Finer carried out the initial analyses and reviewed and revised themanuscript; and all authors approved the final manuscript as submitted.
This trial has been registered at clinicaltrials.gov (identifier NCT01866982).
www.pediatrics.org/cgi/doi/10.1542/peds.2015-0368
DOI: 10.1542/peds.2015-0368
Accepted for publication Apr 20, 2015
Address correspondence to Anup C. Katheria, MD, Neonatal Research Institute at Sharp Mary BirchHospital for Women and Newborns, 8555 Aero Dr, Suite 104, San Diego, CA 92123. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
PEDIATRICS Volume 136, number 1, July 2015 ARTICLE by guest on October 7, 2020www.aappublications.org/newsDownloaded from

In December 2012, the AmericanCollege of Obstetricians andGynecologists (ACOG) recommendeda 30- to 60-second delay in umbilicalcord clamping for all pretermdeliveries.1 Although delayed cordclamping (DCC) has decreased theoverall incidence of intraventricularhemorrhage (IVH), the enthusiasmfor DCC is tempered by the lack ofbenefit for severe IVH and the smallnumber of infants included in thesetrials.2 The lack of benefit couldreflect the lack of adequateplacental transfusion during DCCfor infants delivered by cesareandelivery (CD).3–5 Three trials ofDCC that stratified by mode ofdelivery found no difference inhematocrit levels or tagged redblood cells in infants delivered byCD.3–5 The ACOG statementacknowledges that there are limiteddata indicating whether DCCperformed during CD can improveplacental transfusion.1
An alternative to DCC is umbilicalcord milking (UCM), or stripping, inwhich the unclamped umbilical cordis grasped and blood is pushedtoward the infant several timesbefore it is clamped to autoinfuseblood into the preterm neonate. Thisprocedure can be performed within20 seconds.6 A recent meta-analysisof 7 randomized controlled trials ofUCM in infants delivered at ,33weeks demonstrated that infants whoundergo UCM have higherhemoglobin (Hb) and a lower risk foroxygen requirement at 36 weeks andIVH of all grades compared withthose who undergo immediate cordclamping (ICC).7
A recently published studycompared UCM with DCC (n = 58) ininfants delivered at ,33 weeks’gestational age.8 Although no majorclinical differences were foundbetween UCM and DCC, this trial didnot analyze any outcomes by modeof delivery. To date there have beenno trials comparing UCM and DCC atCD. Given that up to 90% of preterm
infants are delivered by CD, there isa critical need to determine whichtherapy should be given to preterminfants.9 We hypothesized that UCMat CD could improve perfusion, orsystemic blood flow (SBF), inpreterm neonates as measured bysuperior vena cava (SVC) flow andright ventricular output (RVO) andwould be associated with decreasedneonatal morbidities compared withDCC, and that UCM may stabilizeblood pressure and cerebraloxygenation as measured by near-infrared spectroscopy (NIRS).
METHODS
This randomized controlled trial wasconducted at 2 tertiary care centers(Sharp Mary Birch Hospital forWomen and Newborns [SMBHWN]and Loma Linda University MedicalCenter) and was approved by eachinstitutional review board. Pregnantwomen dated by their earliestultrasound or last menstrual periodat ,32 weeks’ gestation wereidentified and recruited from thelabor and delivery and antepartumfloors. Both interventions were partof standard practice and wereconsidered minimally risky.
In this study, antenatal consent wasnot practical because it wouldexclude the potentially sickestnewborns.10,11 UCM and DCC areboth standard practices at SMBHWNand as such are left to thepreference of the obstetrician.There are no current guidelines fortheir use in the preterm infant, andthey are of equivalent low risk. Ourstudy met the criteria for delayedconsent based on the inability toconduct the trial without a waiverand minimal risk of eitherintervention. As with our previoustrial using delayed consent, parentswere notified of the intervention bythe obstetrician or research teamand were approached immediatelyafter birth to provide writtenconsent to enroll their newborn forcontinued data collection before any
study-related procedures (eg,ultrasounds, additionalmonitoring).12 If a parent did notwant to enroll their child in thestudy, we removed the subject fromour study and destroyed all datathat had been collected.
Exclusion criteria includedmonochorionic multiples,incarcerated mothers, placentaprevia, concern for abruptions, Rhsensitization, hydrops, congenitalanomalies, or the obstetriciandeclining to perform the intervention(ie, unaware of the study protocol).We did included infants withperinatal depression because it wouldnot be feasible to detect perinataldepression at the time of delivery.Entry criteria included a gestationalage of 23 0/7 to 31 6/7 weeks.
Infants were randomly assigned byopaque, sealed envelopesimmediately before delivery.Computer-generated randomizationwas stratified by gestational age andmode of delivery (23–27 6/7 or28–31 6/7 weeks) to ensure equalnumbers of neonates born at ,28weeks’ gestation in each arm. Theobstetricians were made aware of therandomization by the neonatologyteam immediately before delivery ofthe infant. Multiples (twins ortriplets) received the same randomassignment.
Using the Apgar timer on theresuscitation bed, the advanced lifesupport (ALS) nurses or labor anddelivery staff attending the deliveryrecorded and counted out loud thetime elapsed from when the infantwas delivered until the time theumbilical cord was clamped by theobstetrician in both arms of the study.UCM was performed by holding theinfant at or ∼20 cm below the level ofthe placenta. The cord was pinched asclose to the placenta as possible andmilked toward the infant overa 2-second duration. The cord wasthen released and allowed to refillwith blood for a brief 1- to 2-secondpause between each milking motion.
62 KATHERIA et al by guest on October 7, 2020www.aappublications.org/newsDownloaded from

This was repeated for a total of 4times. After completion, the cord wasclamped, and the neonate washanded to the resuscitation team.8
DCC was performed by holding theinfant at or ∼20 cm below the level ofthe placenta and waiting at least 45seconds before clamping the cord. Inboth arms infants were dried andwrapped with sterile towels until thecord was clamped.
Hemodynamic measurements wereonly performed at site 1 (SMBHWN).These measures included an earlyechocardiogram (target 6–12 hours oflife) and continuous hemodynamicrecordings. The echocardiogram was
performed with the Vivid E9cardiovascular ultrasound systemwith a 12S phased array transducer(GE Medical Systems, Milwaukee, WI).At the time of the first scan allneonates also had a bedside headultrasound to document evidence ofIVH. Formal head ultrasounds wereperformed on the second or third dayof life according to our unit protocol.
Blinded echocardiograms and headultrasounds were performed mainly(.90%) by the principal investigator(A.C.K.). None of the investigatorsperforming echocardiograms wereinvolved in the randomization or therecording of the intervention. All
images were analyzed and measuredoffline by using EchoPAC software(GE HealthCare, Horten, Norway) andwere analyzed without knowledge ofthe assigned group by the principalinvestigator. The blinding wasachieved by allowing only the ALSnurse attending the delivery andthe obstetrician performing theintervention to be aware of theallocation arm. This was possiblebecause all high-risk deliveriesoccurred in a room adjacent to theresuscitation suite where seniorphysicians, nurses, and respiratorytherapists are in attendance at bothsites. No documentation of the
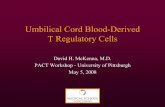
FIGURE 1CONSORT diagram: study enrollment, intended randomization, and actual randomization.
PEDIATRICS Volume 136, number 1, July 2015 63 by guest on October 7, 2020www.aappublications.org/newsDownloaded from

intervention was made in thephysician or ALS notes. Therandomization cards assigneda subject identification number thatwas kept by the researchcoordinator.
Measures of superior vena cava (SVC)flow, right ventricular output (RVO),left ventricular output (LVO),diameter and direction of flowthrough the patent ductus arteriosus,and diameter and direction of flowthrough the foramen ovale wereobtained on each examination.
Flow measures were calculated byusing previously describedtechniques.13
The primary outcome was the SVCflow within the first 12 hours. Infantswere resuscitated according to eachunit’s protocol. We attacheda cerebral oxygen saturation monitorusing 4 different wavelengths (FORE-SIGHT; Casmed, Branford, CT) to theinfant by placing a sensor on theinfant’s forehead within the first2 hours of life. Cerebral saturationwas recorded for the first 24 hours oflife.
Electrical cardiometry (EC) was usedas a continuous noninvasive measureof cardiac output. EC uses theproperties of bioimpedance tononinvasively measure bodycomposition and blood flow viasurface adhesive electrodes. Changesin thoracic impedance during deliveryof a low-voltage current indicatecardiac output. We validated the useof EC compared withechocardiographic measures of rightand left ventricular output and SVCflow.14 All infants had EC sensorsplaced on their chest by 2 hours andhad data recorded for the first24 hours of life. Cerebral oxygensaturation, pulse oxygen saturation,heart rate, respiratory rate, bloodpressure, cardiac output, and strokevolume were recorded every2 seconds on a purpose-built dataacquisition system.
Data Collection (Both Sites)
A single study-related blood draw(hematocrit at 12 hours froma central or venipuncture) and headultrasound on day 1 were collected aspart of the research protocol.Admission complete blood cell countand head ultrasounds on the secondor third day of life were part ofroutine care. All other relevantprenatal and neonatal data wereobtained from the medical records ofmother and infant.
Statistical Analysis
An initial pilot study of 30 infants wascompleted to determine the feasibilityand efficacy of the study and revealeda 25% difference in SVC flow at 6hours between infants treated withUCM and controls. We based oursample calculations on the basis ofour previous results and thepreliminary evaluation of the firstpilot infants. A sample size calculationdetermined that $40 neonates in
each group were needed todemonstrate at least a 25% differencein SVC at 12 hours between neonatestreated with UCM those treated withDCC with a 2-sided a of .05 and 80%power. However, when a second sitethat could not performhemodynamics was added, thesample size was increased (n = 600)to detect change in the incidence ofIVH, based on a 50% reduction in IVHfrom Rabe et al (22% vs 11%, P =.32). This change was added asa secondary outcome to the trial.
We performed statistical analyses byusing PASW Statistics 18.0 (Chicago,IL). Normally distributed continuousoutcome variables were comparedwith the unpaired Student’s t test,and nonparametric continuousoutcome variables were analyzedwith the Mann–Whitney U test. Forrepeated measurements tests, R (RFoundation for Statistical Computing,Vienna, Austria) and lme4 (linearmixed-effects models using Eigen and
TABLE 1 Perinatal Outcomes for Infants Delivered by CD
UCM (n = 75) DCC (n = 79)
Maternal age, y 31 6 5 30 6 6Gestational age, wk 28 6 2 28 6 2Birth wt, g 1255 6 413 1132 6 392Placenta wt, g 257 6 95 245 6 109Female 46 48Diabetes (gestational or type 1 or 2) 11 15Chorioamnionitis 20 20Pregnancy-induced hypertension 22 25Labor or uterotonics before delivery 27 20Narcotics given before delivery 16 19Lowest maternal Hb (48 h after delivery), g/dL 10 6 2.7 9.8 6 1.6Duration of rupture of membranes, h 63 6 169 67 6 147General anesthesia 6 2Full course antenatal steroids 69 75Antenatal magnesium 72 64
Data are presented as mean 6 SD. There were no significant group differences at baseline.
TABLE 2 Delivery Room Outcomes for Infants Delivered by CD
UCM, N = 75 DCC, N = 79
Time clamp cord, s** 20 6 10 42 6 12Delivery room temperature, °C 36.8 6 0.4 36.6 6 0.4Admission temperature, °C 36.8 6 0.6 36.7 6 0.4Apgar score, 1 min, 5 min (median) 5, 7 5, 7Needed PPV 57 56Intubation in delivery room 28 33
Data are presented as mean 6 SD unless otherwise stated. PPV, positive-pressure ventilation.**P , .001.
64 KATHERIA et al by guest on October 7, 2020www.aappublications.org/newsDownloaded from

S4) were used to perform linearmixed-effects regression (lmer)analysis of the relationship betweenthe respective treatments (ie, UCMand DCC). Two-sided P ,.05 wasconsidered significant.
RESULTS
Interim analysis after 197 infantswere enrolled (August 2013–August2014) demonstrated that althoughthe primary outcome (SVC flow) wasstatistically different (Table 4), theincidence of IVH was much lowerthan anticipated (expected 22% vs11%; Rabe et al).8 Based on an actualobserved IVH difference of 6% (13%vs 7%), with a = .05 and b = .8, wewould have needed at least 780 ineach arm. This would have taken 7years for a 2-center study tocomplete. Therefore, the trial wasstopped on the grounds of futility forthe outcome of IVH (154 were
delivered by CD; Fig 1). All data wereanalyzed as intent to treat. From site1, 150 subjects were enrolled; 140(n = 70 each group) had completehemodynamics (functionalechocardiography, NIRS, EC, andbedside monitoring performed), and10 had no or partial hemodynamicdata because of unavailability of staff.For site 2 clinical outcomes werecollected.
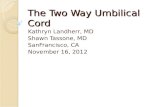
Data for infants delivered by CD areshown in Tables 1, 2, 3, and 4.Neonates who underwent UCM hadhigher admission Hb, higher urineoutput (Table 3), and highermeasures of SBF (SVC flow and RVO,Table 4). There were no differences incerebral saturation, pulse oxygensaturation, cardiac output byimpedance, or heart rate over24 hours (Fig 2). Blood pressure washigher in the first 15 hours of life inthe UCM group (Fig 2).
There were no differences invaginally delivered infants(Supplemental Table 5).
DISCUSSION
Our study is the largest studycomparing UCM with DCC in infantsdelivered by CD and the first todemonstrate improvements inplacental transfusion, as seen byhigher Hb at birth, improvedhemodynamics (higher measures ofblood flow and improved bloodpressure), and improved urine outputwith UCM compared with DCC inpremature infants delivered by CD. Inaddition, although there are 15randomized controlled trials ofa $60-second delay in cord clampingin term infants, this is the firststudy of preterm infants evaluatinga delay .30 seconds.15
Rabe et al randomly assigned 58neonates born at ,33 weeks’gestation to UCM (4 times) or toa 30-second delay in cord clamping.Although they did not find anydifferences in outcomes or Hblevels, the infants treated withDCC had a lower CD rate (58% vs78%).8 Because a greater number ofinfants undergoing DCC weredelivered by VD, the lowerproportion of CD in this group mayhave reduced the difference seenbetween the 2 approaches.Aladangady et al3 reported lowercirculating red cell volume with DCCin neonates born by CD comparedwith VD. One could speculatewhether more blood remains in theplacenta when a neonate isdelivered by CD because theanesthetic and surgicalinterventions interfere with theactive contraction of the uterinemuscles to expel the placenta.
SVC flow and RVO were higher ininfants treated with UCM. SVC flow,a measure of SBF, is an importantmarker of neonatal transition. SVCflow represents cardiac input andtherefore is not affected by thepresence of fetal shunts. It is
TABLE 3 Neonatal Outcomes for Infants Delivered by CD
UCM, N = 75 DCC, N = 79
Birth Hb, g/dL* 16.3 6 2.4 15.6 6 2.2Polycythemia (hematocrit .65%) 2 4Urine output first 24 h, mL/kg per h* 4.42 6 1.3 3.99 6 1.2Need for transfusion 31 41Peak bilirubin, mg/dL 8.1 6 2.9 7.3 6 2.2Necrotizing enterocolitis 1 0Retinopathy necessitating surgery 1 2Spontaneous intestinal perforation 3 2Oxygen at 36 wk corrected 16 12Any IVH 5 10Severe IVH ($grade 3)a 3 3Sepsis (culture positive) 5 3Death 2 6
Data are presented as mean 6 SD unless otherwise stated. * P , .05.a One infant had early-onset sepsis (blood culture positive at birth); otherwise, all sepsis was late onset.
TABLE 4 Hemodynamic Outcomes for Infants Delivered by CD
UCM, N = 75 DCC, N = 79
Time of echocardiogram, h:min 7:23 6 5:53 6:28 6 5:15SVC flow, mL/kg per min* 93 6 24 81 6 29RVO, mL/kg per min** 261 6 80 216 6 73Diameter of atrial shunt, mm 1.78 6 0.81 1.58 6 0.65Diameter of PDA, mm 1.44 6 0.67 1.45 6 0.66LVO, mL/kg per min 189 6 67 206 6 79Need for pressors 9 18PDA necessitating treatment 17 25PDA ligation 4 1
Data are presented as mean 6 SD unless otherwise stated. PDA, patent ductus arteriosus.*P , .05; **P , .001.
PEDIATRICS Volume 136, number 1, July 2015 65 by guest on October 7, 2020www.aappublications.org/newsDownloaded from

therefore a useful measure of SBFin the newborn heart. We alsofound that RVO was higher afterUCM but not LVO. Previousinvestigators have demonstrated
that decreased RVO was closelyassociated with worseningrespiratory disease (defined byfraction of inspired oxygenrequirement), severe IVH, and
death.11 The higher overall SBFs areprobably related to an increasedblood volume from placentaltransfusion, resulting in improvedhemodynamics.
FIGURE 2Continuous hemodynamic measurements over 24 hours of life. Dotted line, UCM; solid line, DCC; CO, cardiac output by electrical cardiometry; HR, heartrate; MAP, mean arterial pressure; SpO2, pulse oxygen saturation; SV, stroke volume by electrical cardiometry; StO2, cerebral saturations by near-infraredspectroscopy. *Paired t test = P , .05 for hourly averages. MAP was significantly higher in UCM infants treated with UCM for the first 15 hours (HR 3–15beats per minute; x2 = 5.05, P = .02).
66 KATHERIA et al by guest on October 7, 2020www.aappublications.org/newsDownloaded from

We did not demonstrate a differencein LVO by echocardiography orcardiac output measured by electricalimpedance. We demonstrated ina previous trial that cardiac outputcorrelated better with LVO thanwith RVO or SVC flow.14 The mainconcern with LVO as a measure ofearly SBF during the cardiovasculartransition from fetal to newborn lifeis the extent to which it isconfounded by a left to right ductalshunt, which may be particularlylarge in preterm infants. In thepresence of a ductal shunt, LVOmeasures both SBF and the flowacross the patent ductus arteriosusand therefore significantlyoverestimates SBF. Therefore, it isnot surprising that there was noimprovement in cardiac output withUCM.
We found no difference in cerebraloxygenation as measured by NIRS.Because infants had no difference inoxygenation or cardiac output, it isnot surprising that cerebraloxygenation was not different. Inaddition, there may have beena component of cerebralautoregulation that could haveaffected our results.
Despite no difference in cerebralsaturations or impedance-derivedcardiac output or stroke volume,infants undergoing UCM had higherurine output and blood pressure,suggesting that these infants hadsome improvement in organperfusion within the first 24 hoursof life. Improved perfusion duringthis critical time period may preventIVH from occurring by stabilizingthe fluctuations in SBF that havebeen proposed as a mechanism forlate IVH.16 Although we did not seea statistically significant difference(P = .29) in IVH between groups, wedid not have the power to assessthis outcome based on the observedoccurrence in our study. However,there were fewer absolute numbersof neonates with total and severeIVH in the UCM group, which is
consistent with Rabe et al8
comparing UCM with DCC.
An additional advantage for UCM isthe rapid time frame for UCM tooccur. This not only allowsa minimal delay of resuscitationbut also reduces the time forthe newborn to be cooled in theoperative field. Although thedifference between the 2 groups inour trial was only 20 seconds,infants undergoing UCM had highertemperatures in the delivery room(at 5 minutes) than infantsundergoing DCC. Studies haveshown that low birth weight infantsundergoing DCC are warmer thanthose undergoing ICC, possiblybecause of the warm placentalblood entering the newborn.17 UCMallows rapid placement of thenewborn under the radiant warmer.The admission temperatures werenot different between groups. Wesuggest that centers with concernsabout hypothermia that areconsidering implementing DCC orUCM monitor temperatures in thedelivery room. We have sinceimplemented the use of a warmingbed (Lifestart Trolley; Inditherm,Rotherham, UK) that can be usedon the sterile field in addition towarm sterile towels to ensure thatthere is minimal temperature dropin infants in the operating room.
An important limitation of our trialwas the lack of an ICC group.Because both DCC and UCM providea placental transfusion regardless ofthe mode of delivery, it wasexpected that we would not seesubstantial differences in clinicaloutcomes. Because therecommendations by ACOGdemonstrated that DCC improvedclinical outcomes,1 we did not haveequipoise to randomly assigninfants to a third group that did notreceive a placental transfusion.
However, 18 infants delivered by CDwho were randomly assigned to DCCwere thought to be too unstable inthe opinion of the obstetrician and
underwent ICC. Therefore, the meantime in our trial, by intent to treat,for DCC was 42 seconds. There were2 neonates in the UCM group whounderwent early clamping. Whenthese neonates, who were randomlyassigned to either group (UCM orDCC) but underwent ICC, wereremoved from the analysis therewas still a difference in Hb, SVCflow, RVO, and urine output (datanot shown).
Another limitation of our study isthe small number of infants born at,29 weeks’ gestational age (n =94). Recently, a pilot study of 75extremely premature neonates(born at ,29 weeks’ gestation age)randomly assigned to UCM or ICCdemonstrated a 50% reduction intotal IVH.18 In a recentretrospective study of UCM in 318infants born at ,30 weeks, UCMwas associated with reductions inIVH, necrotizing enterocolitis, anddeath before hospital discharge.19
As suggested by these authors, it ispossible that UCM may have greaterbenefits in smaller, more immatureneonates.
Despite the concerns that UCM mayprovide a rapid bolus of blood, ourdata are consistent with other studiesthat found that UCM is beneficial withminimal risk. Placental blood duringUCM is directed toward the lungsduring a time when there is a rapidfall in pulmonary resistance unlikeany other period when volume isgiven. Concerns about rapid changesin venous pressure during cordmilking were addressed in an earlytrial that demonstrated no greaterincrease in venous pressures withUCM compared with uterinecontractions or a newborn cry duringintact placental circulation.20
Although there are limited data onneurodevelopmental outcomes inpremature infants,21 UCM has beenstudied in 7 randomized controlledtrials and 9 controlled trials overthe past 60 years in term andpreterm infants (n = 1904),
PEDIATRICS Volume 136, number 1, July 2015 67 by guest on October 7, 2020www.aappublications.org/newsDownloaded from

documenting its safety andefficacy.6,20,22–31 A recent meta-analysis evaluating the safety andefficacy of UCM at birth concludedthat there was a lower risk foroxygen requirement at 36 weeksand IVH of all grades.7 Therefore,UCM should no longer beconsidered experimental; rather, itis a proven intervention thatensures that premature newbornsreceive an adequate placentaltransfusion at birth.
CONCLUSIONS
UCM provides a greater placentaltransfusion, as demonstrated byhigher initial Hb, higher bloodpressure, and improved SBF and urineoutput for infants delivered by CD.UCM may be preferable in preterminfants delivered by CD, particularly in
newborns when immediateresuscitation is needed. Althoughmore larger trials are needed toconfirm our observations, UCM shouldbe considered as a beneficial optionfor preterm infants delivered by CD.
ACKNOWLEDGMENTS
The authors acknowledge WadeRich, Kathy Arnell, Jane Steen, andDeb Poeltler for their assistance indesigning the protocol, collectingand analyzing the data, and editingthe manuscript. We alsoacknowledge the San Diegoneonatology physicians andadvanced life support nurses fortheir assistance in randomizing,ensuring compliance with theprotocol, and collecting data in thedelivery room.
ABBREVIATIONS
ACOG: American College ofObstetricians andGynecologists
ALS: advanced life supportCD: cesarean deliveryDCC: delayed cord clampingEC: electrical cardiometryHb: hemoglobinICC: immediate cord clampingIVH: intraventricular hemorrhageLVO: left ventricular outputNIRS: near-infrared spectroscopyRVO: right ventricular outputSBF: systemic blood flowSMBHWN: Sharp Mary Birch
Hospital for Womenand Newborns
SVC: superior vena cavaUCM: umbilical cord milkingVD: vaginal delivery
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: All phases of this study were supported by a National Institutes of Health (NIH) grant 5R03HD072934-02. Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found on page 177, and online at www.pediatrics.org/cgi/doi/10.1542/peds.2015-1545.
REFERENCES
1. Committee on Obstetric Practice, AmericanCollege of Obstetricians and Gynecologists.Committee opinion no. 543: Timing ofumbilical cord clamping after birth. ObstetGynecol. 2012;120(6):1522–1526
2. Rabe H, Diaz-Rossello JL, Duley L,Dowswell T. Effect of timing of umbilicalcord clamping and other strategies toinfluence placental transfusion atpreterm birth on maternal and infantoutcomes. Cochrane Database Syst Rev.2012;8:CD003248
3. Aladangady N, McHugh S, Aitchison TC,Wardrop CA, Holland BM. Infants’ bloodvolume in a controlled trial of placentaltransfusion at preterm delivery.Pediatrics. 2006;117(1):93–98
4. Strauss RG, Mock DM, Johnson K, et al.Circulating RBC volume, measured withbiotinylated RBCs, is superior to the Hctto document the hematologic effects ofdelayed versus immediate umbilicalcord clamping in preterm neonates.Transfusion. 2003;43(8):1168–1172
5. McDonnell M, Henderson-Smart DJ.Delayed umbilical cord clamping inpreterm infants: a feasibility study. JPaediatr Child Health. 1997;33(4):308–310
6. Katheria AC, Leone TA, Woelkers D,Garey DM, Rich W, Finer NN. Theeffects of umbilical cord milking onhemodynamics and neonataloutcomes in premature neonates. JPediatr. 2014;164(5):1045–1050,e1041
7. Al-Wassia H, Shah PS. Efficacy andsafety of umbilical cord milking atbirth: a systematic review and meta-analysis. JAMA Pediatr. 2015;169(1):18–25
8. Rabe H, Jewison A, Alvarez RF, et al;Brighton Perinatal Study Group. Milkingcompared with delayed cord clamping toincrease placental transfusion inpreterm neonates: a randomizedcontrolled trial. Obstet Gynecol. 2011;117(2 pt 1):205–211
9. Bettegowda VR, Dias T, Davidoff MJ,Damus K, Callaghan WM, Petrini JR. Therelationship between cesarean deliveryand gestational age among US singletonbirths. Clin Perinatol. 2008;35(2):309–323, v–vi
10. Rich W, Finer NN, Gantz MG, et al;SUPPORT and Generic DatabaseSubcommittees of the Eunice KennedyShriver National Institute of Child Healthand Human Development NeonatalResearch Network. Enrollment ofextremely low birth weight infants ina clinical research study may not berepresentative. Pediatrics. 2012;129(3):480–484
11. Rich WD, Auten KJ, Gantz MG, et al;National Institute of Child Health andHuman Development Neonatal ResearchNetwork. Antenatal consent in theSUPPORT trial: challenges, costs, andrepresentative enrollment. Pediatrics.2010;126(1). Available at: www.pediatrics.org/cgi/content/full/126/1/e215
68 KATHERIA et al by guest on October 7, 2020www.aappublications.org/newsDownloaded from

12. Katheria AC, Sauberan JB, Akotia D, RichW, Durham J, Finer NN. A pilotrandomized controlled trial of earlyversus routine caffeine in extremelypremature infants [published onlineahead of print January 21, 2015]. Am JPerinatol. 2015. Available at: http://www.ncbi.nlm.nih.gov/pubmed/25607226
13. Katheria A, Leone T. Altered transitionalcirculation in infants of diabetic motherswith strict antenatal obstetricmanagement: a functionalechocardiography study. J Perinatol.2012;32(7):508–513
14. Song R, Rich W, Kim JH, Finer NN,Katheria AC. The use of electricalcardiometry for continuous cardiacoutput monitoring in preterm neonates:a validation study. Am J Perinatol. 2014;31(12):1105–1110
15. McDonald SJ, Middleton P, Dowswell T,Morris PS. Effect of timing of umbilicalcord clamping of term infants onmaternal and neonatal outcomes.Cochrane Database Syst Rev. 2013;7:CD004074
16. Kluckow M, Evans N. Low superior venacava flow and intraventricularhaemorrhage in preterm infants. ArchDis Child Fetal Neonatal Ed. 2000;82(3):F188–F194
17. Kaempf JW, Tomlinson MW, Kaempf AJ,et al. Delayed umbilical cord clamping inpremature neonates. Obstet Gynecol.2012;120(2 pt 1):325–330
18. March MI, Hacker MR, Parson AW,Modest AM, de Veciana M. The effects ofumbilical cord milking in extremelypreterm infants: a randomizedcontrolled trial. J Perinatol. 2013;33(10):763–767
19. Patel S, Clark EA, Rodriguez CE, Metz TD,Abbaszadeh M, Yoder BA. Effect ofumbilical cord milking on morbidity andsurvival in extremely low gestational ageneonates. Am J Obstet Gynecol. 2014;211(5):519, e511–517
20. McCausland AM, Holmes F, SchumannWR. Management of cord and placentalblood and its effect upon the newborn.Calif Med. 1949;71(3):190–196
21. Ghavam S, Batra D, Mercer J, et al.Effects of placental transfusion inextremely low birthweight infants: meta-analysis of long- and short-termoutcomes. Transfusion. 2014;54(4):1192–1198
22. Colozzi AE. Clamping of the umbilicalcord; its effect on the placentaltransfusion. N Engl J Med. 1954;250(15):629–632
23. Erickson-Owens DA, Mercer JS, Oh W.Umbilical cord milking in term infantsdelivered by cesarean section:a randomized controlled trial. JPerinatol. 2012;32(8):580–584
24. Oh W. Cord milking at delivery improvesthe iron status of term infants at 6weeks. Evid Based Med. 2013;18(6):e58
25. Takami T, Suganami Y, Sunohara D, et al.Umbilical cord milking stabilizescerebral oxygenation and perfusion ininfants born before 29 weeks ofgestation. J Pediatr. 2012;161(4):742–747
26. Upadhyay A, Gothwal S, Parihar R, et alEffect of umbilical cord milking in termand near term infants: randomizedcontrol trial. Am J Obstet Gynecol. 2013;208(2):120, e121–126
27. Whipple GA, Sisson TR, Lund CJ. Delayedligation of the umbilical cord; itsinfluence on the blood volume of thenewborn. Obstet Gynecol. 1957;10(6):603–610
28. Lanzkowsky P. Effects of early and lateclamping of umbilical cord on infant’shaemoglobin level. BMJ. 1960;2(5215):1777–1782
29. Siddall RS, Richardson RP. Milking orstripping the umbilical cord; effect onvaginally delivered babies. ObstetGynecol. 1953;1(2):230–233
30. Siddall RS, Crissey RR, Knapp WL. Effecton cesarean section babies of strippingor milking of the umbilical cords. Am JObstet Gynecol. 1952;63(5):1059–1064
31. Alan S, Arsan S, Okulu E, et al. Effects ofumbilical cord milking on the need forpacked red blood cell transfusions andearly neonatal hemodynamic adaptationin preterm infants born #1500 g:a prospective, randomized, controlledtrial. J Pediatr Hematol Oncol. 2014;36(8):e493–e498
PEDIATRICS Volume 136, number 1, July 2015 69 by guest on October 7, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-0368 originally published online June 29, 2015; 2015;136;61Pediatrics
Anup C. Katheria, Giang Truong, Larry Cousins, Bryan Oshiro and Neil N. FinerUmbilical Cord Milking Versus Delayed Cord Clamping in Preterm Infants
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/1/61including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/136/1/61#BIBLThis article cites 31 articles, 6 of which you can access for free at:
Subspecialty Collections
ers_subhttp://www.aappublications.org/cgi/collection/cardiovascular_disordCardiovascular Disordershttp://www.aappublications.org/cgi/collection/cardiology_subCardiologyhttp://www.aappublications.org/cgi/collection/neonatology_subNeonatologysubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on October 7, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-0368 originally published online June 29, 2015; 2015;136;61Pediatrics
Anup C. Katheria, Giang Truong, Larry Cousins, Bryan Oshiro and Neil N. FinerUmbilical Cord Milking Versus Delayed Cord Clamping in Preterm Infants
http://pediatrics.aappublications.org/content/136/1/61located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2015/06/23/peds.2015-0368.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2015has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on October 7, 2020www.aappublications.org/newsDownloaded from