
Ultrasound predictors of placental invasion: the Placenta ... · OBSTETRICS Ultrasound predictors...
7
OBSTETRICS Ultrasound predictors of placental invasion: the Placenta Accreta Index Martha W. F. Rac, MD; Jodi S. Dashe, MD; C. Edward Wells, MD; Elysia Moschos, MD; Donald D. McIntire, PhD; Diane M. Twickler, MD OBJECTIVE: We sought to apply a standardized evaluation of ultra- sound parameters for the prediction of placental invasion in a high-risk population. STUDY DESIGN: This was a retrospective review of gravidas with 1 prior cesarean delivery who received an ultrasound diagnosis of placenta previa or low-lying placenta in the third trimester at our institution from 1997 through 2011. Sonographic images were reviewed by an investigator blinded to pregnancy outcome and so- nography reports. Parameters assessed included loss of retroplacental clear zone, irregularity and width of uterine-bladder interface, smallest myometrial thickness, presence of lacunar spaces, and bridging vessels. Diagnosis of placental invasion was based on histologic confirmation. Statistical analyses were performed using linear logistic regression and multiparametric analyses to generate a predictive equation evaluated using a receiver operating characteristic curve. RESULTS: Of 184 gravidas who met inclusion criteria, 54 (29%) had invasion confirmed on hysterectomy specimen. All sonographic pa- rameters were associated with placental invasion (P < .001). Con- structing a receiver operating characteristic curve, the combination of smallest sagittal myometrial thickness, lacunae, and bridging vessels, in addition to number of cesarean deliveries and placental location, yielded an area under the curve of 0.87 (95% confidence interval, 0.80e0.95). Using logistic regression, a predictive equation was generated, termed the “Placenta Accreta Index.” Each parameter was weighted to create a 9-point scale in which a score of 0-9 provided a probability of invasion that ranged from 2e96%, respectively. CONCLUSION: Assignment of the Placenta Accreta Index may be helpful in predicting individual patient risk for morbidly adherent placenta. Key words: accreta, invasion, ultrasound Cite this article as: Rac MWF, Dashe JS, Wells CE, et al. Ultrasound predictors of placental invasion: the Placenta Accreta Index. Am J Obstet Gynecol 2015;212:343.e1-7. T he morbidly adherent placenta (accreta, increta, and percreta) has emerged as a significant obstetric challenge over the last decade. Once a rare diag- nosis, 1 morbidly adherent placenta now complicates as many as 1 per 500 preg- nancies. 2 Antenatal diagnosis of placental invasion has the potential to improve maternal and fetal outcomes. 3,4 Predeliv- ery knowledge of morbidly adherent placenta allows for multidisciplinary planning and delivery before the onset of labor and/or vaginal bleeding. 5 This approach has lowered overall maternal morbidity rates, including less blood loss, as well as fewer transfusion requirements and intraoperative urologic injuries. 3,6 Sonography with grayscale and color Doppler imaging is the recommended first-line modality for diagnosing mor- bidly adherent placenta. 5,7,8 Although more elaborate forms of imaging are promising in defining the topography of the placenta, such as 3-dimensional Doppler and volume contrast ultra- sound, validation studies are lacking as well as generalized applicability of tech- nique. 9,10 The diagnosis of morbidly adherent placenta involves a number of different ultrasound variables, some qualitative and others that have been quantified. These markers include an inability to visualize the normal retro- placental clear zone, irregularity and attenuation of the uterine-bladder inter- face, retroplacental myometrial thickness, presence of intraplacental lacunar spaces, and bridging vessels between the placenta and bladder wall when using color Doppler. 11-16 A recent metaanalysis of 23 studies explored the contribution of these ultrasound parameters to the overall prediction of morbidly adherent placenta and found a promising sensitivity of 91% and specificity of 97%. 17 A logical next step in predicting morbidly adherent placenta by ultra- sound would be to determine the sig- nificance of each ultrasound finding, to estimate the probability of invasion based on a multiparametric analysis. Our objective was to develop a predictive equation for probability of invasion based on a combination of ultrasound parameters and clinical characteristics in a cohort of women at increased risk for placental invasion. MATERIALS AND METHODS This was a retrospective review of grav- idas with 1 prior cesarean deliveries From the Departments of Obstetrics and Gynecology (all authors) and Radiology (Dr Twickler), University of Texas Southwestern Medical Center, Dallas, TX. Received May 20, 2014; revised July 28, 2014; accepted Oct. 15, 2014. The authors report no conflict of interest. Presented at the 34th annual meeting of the Society for Maternal-Fetal Medicine, New Orleans, LA, Feb. 3-8, 2014. Corresponding author: Martha W. F. Rac, MD. [email protected] 0002-9378/$36.00 ª 2015 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ajog.2014.10.022 MARCH 2015 American Journal of Obstetrics & Gynecology 343.e1 Research ajog.org
Transcript of Ultrasound predictors of placental invasion: the Placenta ... · OBSTETRICS Ultrasound predictors...

Research ajog.org
OBSTETRICS
Ultrasound predictors of placental invasion:the Placenta Accreta IndexMartha W. F. Rac, MD; Jodi S. Dashe, MD; C. Edward Wells, MD; Elysia Moschos, MD;Donald D. McIntire, PhD; Diane M. Twickler, MD
OBJECTIVE: We sought to apply a standardized evaluation of ultra- RESULTS: Of 184 gravidas who met inclusion criteria, 54 (29%) had
sound parameters for the prediction of placental invasion in a high-riskpopulation.STUDY DESIGN: This was a retrospective review of gravidas with �1prior cesarean delivery who received an ultrasound diagnosis ofplacenta previa or low-lying placenta in the third trimester at ourinstitution from 1997 through 2011. Sonographic images werereviewed by an investigator blinded to pregnancy outcome and so-nography reports. Parameters assessed included loss of retroplacentalclear zone, irregularity and width of uterine-bladder interface, smallestmyometrial thickness, presence of lacunar spaces, and bridgingvessels. Diagnosis of placental invasion was based on histologicconfirmation. Statistical analyses were performed using linear logisticregression and multiparametric analyses to generate a predictiveequation evaluated using a receiver operating characteristic curve.
From the Departments of Obstetrics and Gynecology (all authors) and RadioUniversity of Texas Southwestern Medical Center, Dallas, TX.
Received May 20, 2014; revised July 28, 2014; accepted Oct. 15, 2014.
The authors report no conflict of interest.
Presented at the 34th annual meeting of the Society for Maternal-Fetal MedicFeb. 3-8, 2014.
Corresponding author: Martha W. F. Rac, MD. Martha.Rac@utsouthwestern
0002-9378/$36.00 � ª 2015 Elsevier Inc. All rights reserved. � http://dx.doi.org/10.1
invasion confirmed on hysterectomy specimen. All sonographic pa-rameters were associated with placental invasion (P < .001). Con-structing a receiver operating characteristic curve, the combination ofsmallest sagittal myometrial thickness, lacunae, and bridging vessels,in addition to number of cesarean deliveries and placental location,yielded an area under the curve of 0.87 (95% confidence interval,0.80e0.95). Using logistic regression, a predictive equation wasgenerated, termed the “Placenta Accreta Index.” Each parameter wasweighted to create a 9-point scale in which a score of 0-9 provided aprobability of invasion that ranged from 2e96%, respectively.
CONCLUSION: Assignment of the Placenta Accreta Index may be helpfulin predicting individual patient risk for morbidly adherent placenta.
Key words: accreta, invasion, ultrasound
Cite this article as: Rac MWF, Dashe JS, Wells CE, et al. Ultrasound predictors of placental invasion: the Placenta Accreta Index. Am J Obstet Gynecol 2015;212:343.e1-7.
he morbidly adherent placenta
T (accreta, increta, and percreta) hasemerged as a significant obstetric challengeover the last decade. Once a rare diag-nosis,1 morbidly adherent placenta nowcomplicates as many as 1 per 500 preg-nancies.2 Antenatal diagnosis of placentalinvasion has the potential to improvematernal and fetal outcomes.3,4 Predeliv-ery knowledge of morbidly adherentplacenta allows for multidisciplinaryplanning and delivery before the onset oflabor and/or vaginal bleeding.5 Thisapproach has lowered overall maternalmorbidity rates, including less blood loss,as well as fewer transfusion requirementsand intraoperative urologic injuries.3,6Sonography with grayscale and colorDoppler imaging is the recommendedfirst-line modality for diagnosing mor-bidly adherent placenta.5,7,8 Althoughmore elaborate forms of imaging arepromising in defining the topography ofthe placenta, such as 3-dimensionalDoppler and volume contrast ultra-sound, validation studies are lacking aswell as generalized applicability of tech-nique.9,10 The diagnosis of morbidlyadherent placenta involves a number ofdifferent ultrasound variables, somequalitative and others that have beenquantified. These markers include aninability to visualize the normal retro-placental clear zone, irregularity and
logy (Dr Twickler),
ine, New Orleans, LA,
.edu
016/j.ajog.2014.10.022
MARCH 2015 Ameri
attenuation of the uterine-bladder inter-face, retroplacentalmyometrial thickness,presence of intraplacental lacunar spaces,and bridging vessels between the placentaand bladder wall when using colorDoppler.11-16 A recent metaanalysis of 23studies explored the contribution of theseultrasound parameters to the overallprediction of morbidly adherent placentaand found a promising sensitivity of 91%and specificity of 97%.17
A logical next step in predictingmorbidly adherent placenta by ultra-sound would be to determine the sig-nificance of each ultrasound finding, toestimate the probability of invasionbased on a multiparametric analysis.Our objective was to develop a predictiveequation for probability of invasionbased on a combination of ultrasoundparameters and clinical characteristics ina cohort of women at increased risk forplacental invasion.
MATERIALS AND METHODS
This was a retrospective review of grav-idas with �1 prior cesarean deliveries
can Journal of Obstetrics & Gynecology 343.e1
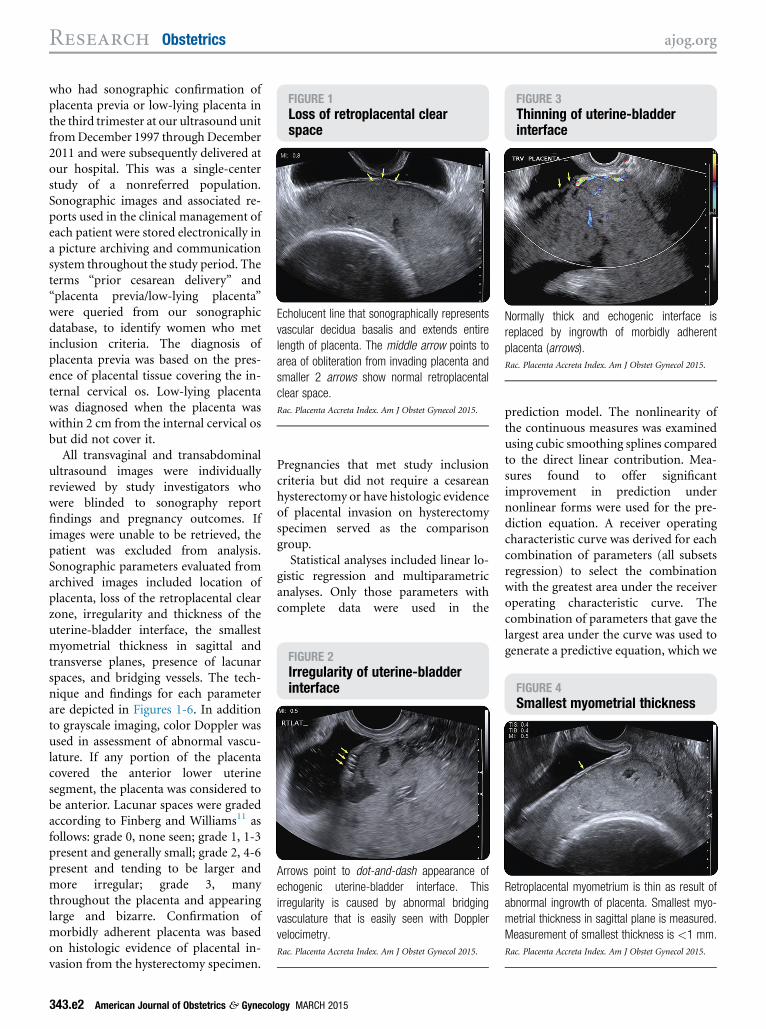
FIGURE 1Loss of retroplacental clearspace
Echolucent line that sonographically represents
vascular decidua basalis and extends entire
length of placenta. The middle arrow points to
area of obliteration from invading placenta and
smaller 2 arrows show normal retroplacental
clear space.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
FIGURE 3Thinning of uterine-bladderinterface
Normally thick and echogenic interface is
replaced by ingrowth of morbidly adherent
placenta (arrows).
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
FIGURE 2Irregularity of uterine-bladderinterface
Arrows point to dot-and-dash appearance of
echogenic uterine-bladder interface. This
irregularity is caused by abnormal bridging
vasculature that is easily seen with Doppler
velocimetry.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
FIGURE 4Smallest myometrial thickness
Retroplacental myometrium is thin as result of
abnormal ingrowth of placenta. Smallest myo-
metrial thickness in sagittal plane is measured.
Measurement of smallest thickness is <1 mm.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
Research Obstetrics ajog.org
who had sonographic confirmation ofplacenta previa or low-lying placenta inthe third trimester at our ultrasound unitfromDecember 1997 through December2011 and were subsequently delivered atour hospital. This was a single-centerstudy of a nonreferred population.Sonographic images and associated re-ports used in the clinical management ofeach patient were stored electronically ina picture archiving and communicationsystem throughout the study period. Theterms “prior cesarean delivery” and“placenta previa/low-lying placenta”were queried from our sonographicdatabase, to identify women who metinclusion criteria. The diagnosis ofplacenta previa was based on the pres-ence of placental tissue covering the in-ternal cervical os. Low-lying placentawas diagnosed when the placenta waswithin 2 cm from the internal cervical osbut did not cover it.
All transvaginal and transabdominalultrasound images were individuallyreviewed by study investigators whowere blinded to sonography reportfindings and pregnancy outcomes. Ifimages were unable to be retrieved, thepatient was excluded from analysis.Sonographic parameters evaluated fromarchived images included location ofplacenta, loss of the retroplacental clearzone, irregularity and thickness of theuterine-bladder interface, the smallestmyometrial thickness in sagittal andtransverse planes, presence of lacunarspaces, and bridging vessels. The tech-nique and findings for each parameterare depicted in Figures 1-6. In additionto grayscale imaging, color Doppler wasused in assessment of abnormal vascu-lature. If any portion of the placentacovered the anterior lower uterinesegment, the placenta was considered tobe anterior. Lacunar spaces were gradedaccording to Finberg and Williams11 asfollows: grade 0, none seen; grade 1, 1-3present and generally small; grade 2, 4-6present and tending to be larger andmore irregular; grade 3, manythroughout the placenta and appearinglarge and bizarre. Confirmation ofmorbidly adherent placenta was basedon histologic evidence of placental in-vasion from the hysterectomy specimen.
343.e2 American Journal of Obstetrics & Gynecol
Pregnancies that met study inclusioncriteria but did not require a cesareanhysterectomy or have histologic evidenceof placental invasion on hysterectomyspecimen served as the comparisongroup.Statistical analyses included linear lo-
gistic regression and multiparametricanalyses. Only those parameters withcomplete data were used in the
ogy MARCH 2015
prediction model. The nonlinearity ofthe continuous measures was examinedusing cubic smoothing splines comparedto the direct linear contribution. Mea-sures found to offer significantimprovement in prediction undernonlinear forms were used for the pre-diction equation. A receiver operatingcharacteristic curve was derived for eachcombination of parameters (all subsetsregression) to select the combinationwith the greatest area under the receiveroperating characteristic curve. Thecombination of parameters that gave thelargest area under the curve was used togenerate a predictive equation, which we
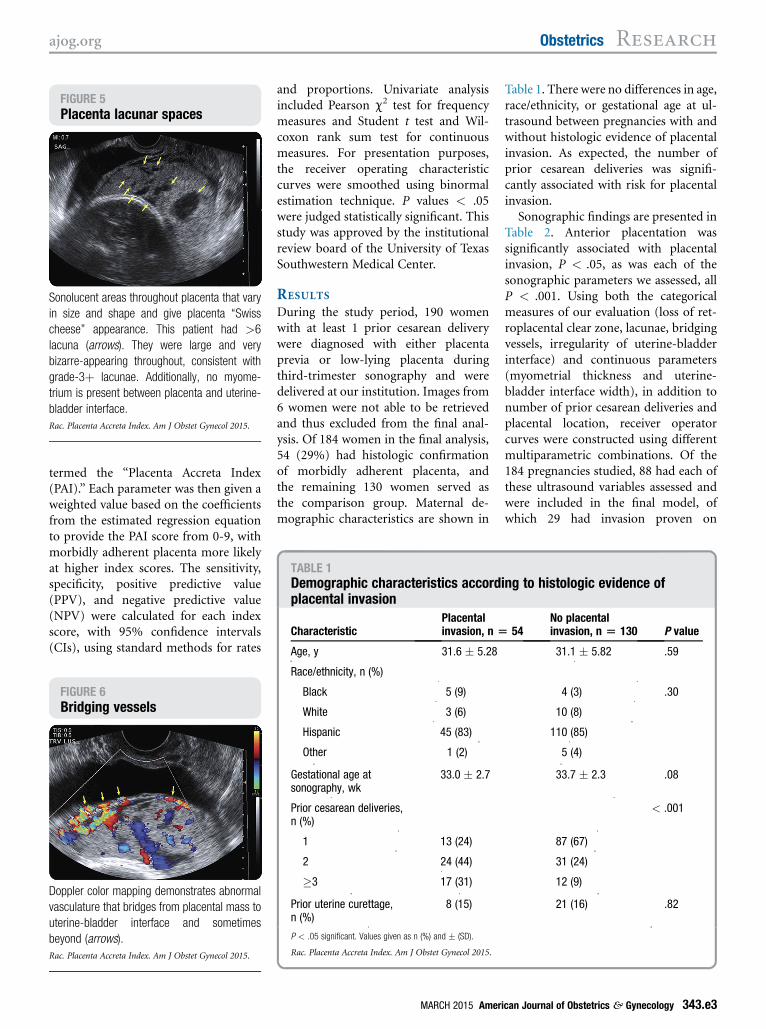
FIGURE 5Placenta lacunar spaces
Sonolucent areas throughout placenta that vary
in size and shape and give placenta “Swiss
cheese” appearance. This patient had >6
lacuna (arrows). They were large and very
bizarre-appearing throughout, consistent with
grade-3þ lacunae. Additionally, no myome-
trium is present between placenta and uterine-
bladder interface.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
TABLE 1Demographic characteristics according to histologic evidence ofplacental invasion
CharacteristicPlacentalinvasion, n [ 54
No placentalinvasion, n [ 130 P value
Age, y 31.6 � 5.28 31.1 � 5.82 .59
ajog.org Obstetrics Research
termed the “Placenta Accreta Index(PAI).” Each parameter was then given aweighted value based on the coefficientsfrom the estimated regression equationto provide the PAI score from 0-9, withmorbidly adherent placenta more likelyat higher index scores. The sensitivity,specificity, positive predictive value(PPV), and negative predictive value(NPV) were calculated for each indexscore, with 95% confidence intervals(CIs), using standard methods for rates
FIGURE 6Bridging vessels
Doppler color mapping demonstrates abnormal
vasculature that bridges from placental mass to
uterine-bladder interface and sometimes
beyond (arrows).
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
and proportions. Univariate analysisincluded Pearson c2 test for frequencymeasures and Student t test and Wil-coxon rank sum test for continuousmeasures. For presentation purposes,the receiver operating characteristiccurves were smoothed using binormalestimation technique. P values < .05were judged statistically significant. Thisstudy was approved by the institutionalreview board of the University of TexasSouthwestern Medical Center.
RESULTS
During the study period, 190 womenwith at least 1 prior cesarean deliverywere diagnosed with either placentaprevia or low-lying placenta duringthird-trimester sonography and weredelivered at our institution. Images from6 women were not able to be retrievedand thus excluded from the final anal-ysis. Of 184 women in the final analysis,54 (29%) had histologic confirmationof morbidly adherent placenta, andthe remaining 130 women served asthe comparison group. Maternal de-mographic characteristics are shown in
Race/ethnicity, n (%)
Black 5 (9)
White 3 (6)
Hispanic 45 (83)
Other 1 (2)
Gestational age atsonography, wk
33.0 � 2.7
Prior cesarean deliveries,n (%)
1 13 (24)
2 24 (44)
�3 17 (31)
Prior uterine curettage,n (%)
8 (15)
P < .05 significant. Values given as n (%) and � (SD).
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
MARCH 2015 Ameri
Table 1. There were no differences in age,race/ethnicity, or gestational age at ul-trasound between pregnancies with andwithout histologic evidence of placentalinvasion. As expected, the number ofprior cesarean deliveries was signifi-cantly associated with risk for placentalinvasion.
Sonographic findings are presented inTable 2. Anterior placentation wassignificantly associated with placentalinvasion, P < .05, as was each of thesonographic parameters we assessed, allP < .001. Using both the categoricalmeasures of our evaluation (loss of ret-roplacental clear zone, lacunae, bridgingvessels, irregularity of uterine-bladderinterface) and continuous parameters(myometrial thickness and uterine-bladder interface width), in addition tonumber of prior cesarean deliveries andplacental location, receiver operatorcurves were constructed using differentmultiparametric combinations. Of the184 pregnancies studied, 88 had each ofthese ultrasound variables assessed andwere included in the final model, ofwhich 29 had invasion proven on
4 (3) .30
10 (8)
110 (85)
5 (4)
33.7 � 2.3 .08
< .001
87 (67)
31 (24)
12 (9)
21 (16) .82
can Journal of Obstetrics & Gynecology 343.e3
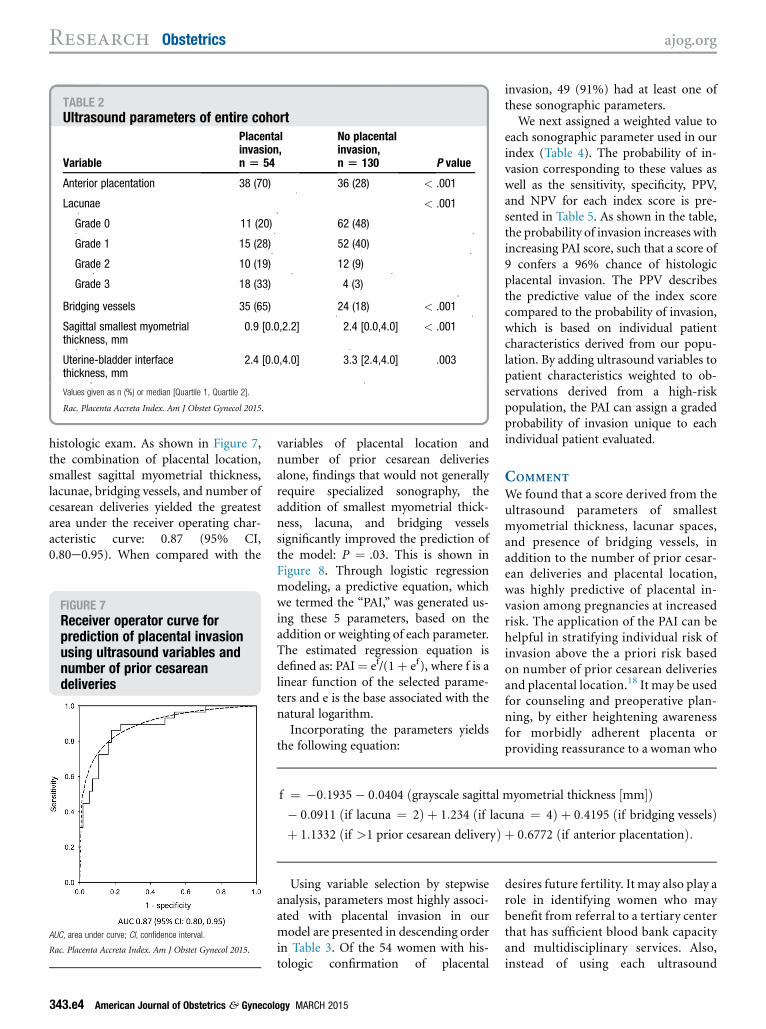
TABLE 2Ultrasound parameters of entire cohort
Variable
Placentalinvasion,n [ 54
No placentalinvasion,n [ 130 P value
Anterior placentation 38 (70) 36 (28) < .001
Lacunae < .001
Grade 0 11 (20) 62 (48)
Grade 1 15 (28) 52 (40)
Grade 2 10 (19) 12 (9)
Grade 3 18 (33) 4 (3)
Bridging vessels 35 (65) 24 (18) < .001
Sagittal smallest myometrialthickness, mm
0.9 [0.0,2.2] 2.4 [0.0,4.0] < .001
Uterine-bladder interfacethickness, mm
2.4 [0.0,4.0] 3.3 [2.4,4.0] .003
Values given as n (%) or median [Quartile 1, Quartile 2].
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
Research Obstetrics ajog.org
histologic exam. As shown in Figure 7,the combination of placental location,smallest sagittal myometrial thickness,lacunae, bridging vessels, and number ofcesarean deliveries yielded the greatestarea under the receiver operating char-acteristic curve: 0.87 (95% CI,0.80e0.95). When compared with the
FIGURE 7Receiver operator curve forprediction of placental invasionusing ultrasound variables andnumber of prior cesareandeliveries
AUC, area under curve; CI, confidence interval.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
343.e4 American Journal of Obstetrics & Gynecol
variables of placental location andnumber of prior cesarean deliveriesalone, findings that would not generallyrequire specialized sonography, theaddition of smallest myometrial thick-ness, lacuna, and bridging vesselssignificantly improved the prediction ofthe model: P ¼ .03. This is shown inFigure 8. Through logistic regressionmodeling, a predictive equation, whichwe termed the “PAI,” was generated us-ing these 5 parameters, based on theaddition or weighting of each parameter.The estimated regression equation isdefined as: PAI¼ ef/(1þ ef), where f is alinear function of the selected parame-ters and e is the base associated with thenatural logarithm.Incorporating the parameters yields
the following equation:
f ¼ �0:1935� 0:0404 ðgrayscale sagittal myometrial thickness ½mm�Þ� 0:0911 ðif lacuna ¼ 2Þ þ 1:234 ðif lacuna ¼ 4Þ þ 0:4195 ðif bridging vesselsÞþ 1:1332 ðif >1 prior cesarean deliveryÞ þ 0:6772 ðif anterior placentationÞ:
Using variable selection by stepwiseanalysis, parameters most highly associ-ated with placental invasion in ourmodel are presented in descending orderin Table 3. Of the 54 women with his-tologic confirmation of placental
ogy MARCH 2015
invasion, 49 (91%) had at least one ofthese sonographic parameters.
We next assigned a weighted value toeach sonographic parameter used in ourindex (Table 4). The probability of in-vasion corresponding to these values aswell as the sensitivity, specificity, PPV,and NPV for each index score is pre-sented in Table 5. As shown in the table,the probability of invasion increases withincreasing PAI score, such that a score of9 confers a 96% chance of histologicplacental invasion. The PPV describesthe predictive value of the index scorecompared to the probability of invasion,which is based on individual patientcharacteristics derived from our popu-lation. By adding ultrasound variables topatient characteristics weighted to ob-servations derived from a high-riskpopulation, the PAI can assign a gradedprobability of invasion unique to eachindividual patient evaluated.
COMMENT
We found that a score derived from theultrasound parameters of smallestmyometrial thickness, lacunar spaces,and presence of bridging vessels, inaddition to the number of prior cesar-ean deliveries and placental location,was highly predictive of placental in-vasion among pregnancies at increasedrisk. The application of the PAI can behelpful in stratifying individual risk ofinvasion above the a priori risk basedon number of prior cesarean deliveriesand placental location.18 It may be usedfor counseling and preoperative plan-ning, by either heightening awarenessfor morbidly adherent placenta orproviding reassurance to a woman who
desires future fertility. It may also play arole in identifying women who maybenefit from referral to a tertiary centerthat has sufficient blood bank capacityand multidisciplinary services. Also,instead of using each ultrasound
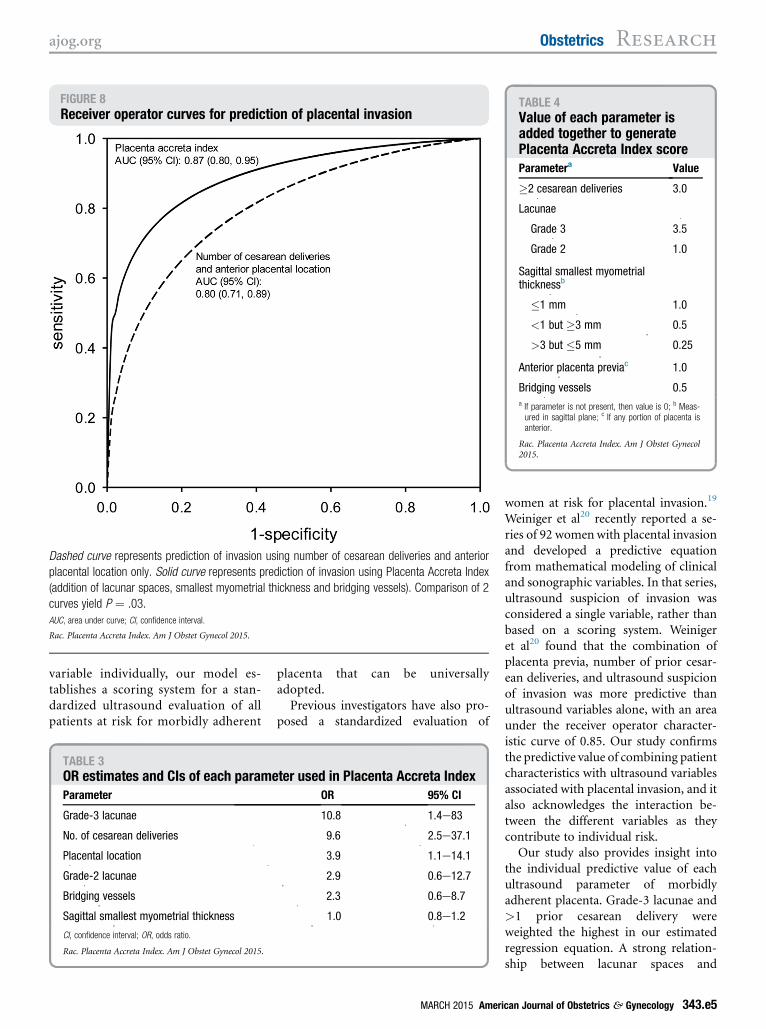
FIGURE 8Receiver operator curves for prediction of placental invasion
Dashed curve represents prediction of invasion using number of cesarean deliveries and anterior
placental location only. Solid curve represents prediction of invasion using Placenta Accreta Index
(addition of lacunar spaces, smallest myometrial thickness and bridging vessels). Comparison of 2
curves yield P ¼ .03.
AUC, area under curve; CI, confidence interval.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
TABLE 4Value of each parameter isadded together to generatePlacenta Accreta Index scoreParametera Value
�2 cesarean deliveries 3.0
Lacunae
Grade 3 3.5
Grade 2 1.0
Sagittal smallest myometrialthicknessb
�1 mm 1.0
<1 but �3 mm 0.5
>3 but �5 mm 0.25
Anterior placenta previac 1.0
Bridging vessels 0.5a If parameter is not present, then value is 0; b Meas-ured in sagittal plane; c If any portion of placenta isanterior.
Rac. Placenta Accreta Index. Am J Obstet Gynecol2015.
ajog.org Obstetrics Research
variable individually, our model es-tablishes a scoring system for a stan-dardized ultrasound evaluation of allpatients at risk for morbidly adherent
TABLE 3OR estimates and CIs of each parameParameter
Grade-3 lacunae
No. of cesarean deliveries
Placental location
Grade-2 lacunae
Bridging vessels
Sagittal smallest myometrial thickness
CI, confidence interval; OR, odds ratio.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
placenta that can be universallyadopted.Previous investigators have also pro-
posed a standardized evaluation of
ter used in Placenta Accreta IndexOR 95% CI
10.8 1.4e83
9.6 2.5e37.1
3.9 1.1e14.1
2.9 0.6e12.7
2.3 0.6e8.7
1.0 0.8e1.2
MARCH 2015 Ameri
women at risk for placental invasion.19
Weiniger et al20 recently reported a se-ries of 92 womenwith placental invasionand developed a predictive equationfrom mathematical modeling of clinicaland sonographic variables. In that series,ultrasound suspicion of invasion wasconsidered a single variable, rather thanbased on a scoring system. Weinigeret al20 found that the combination ofplacenta previa, number of prior cesar-ean deliveries, and ultrasound suspicionof invasion was more predictive thanultrasound variables alone, with an areaunder the receiver operator character-istic curve of 0.85. Our study confirmsthe predictive value of combining patientcharacteristics with ultrasound variablesassociated with placental invasion, and italso acknowledges the interaction be-tween the different variables as theycontribute to individual risk.
Our study also provides insight intothe individual predictive value of eachultrasound parameter of morbidlyadherent placenta. Grade-3 lacunae and>1 prior cesarean delivery wereweighted the highest in our estimatedregression equation. A strong relation-ship between lacunar spaces and
can Journal of Obstetrics & Gynecology 343.e5
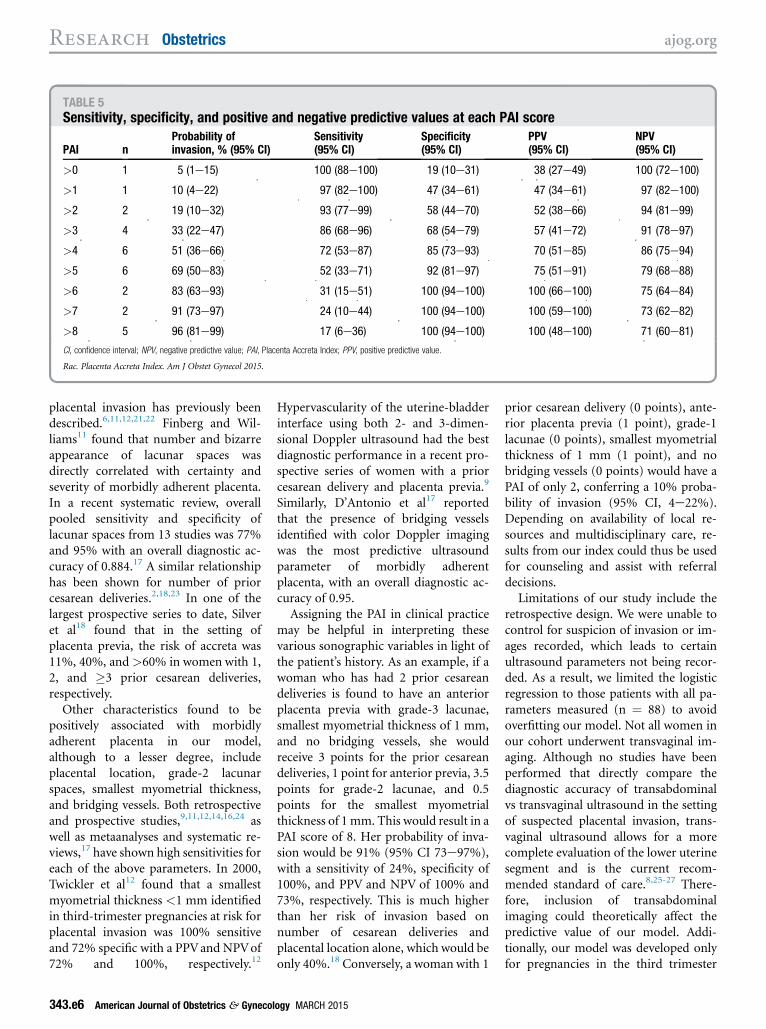
TABLE 5Sensitivity, specificity, and positive and negative predictive values at each PAI score
PAI nProbability ofinvasion, % (95% CI)
Sensitivity(95% CI)
Specificity(95% CI)
PPV(95% CI)
NPV(95% CI)
>0 1 5 (1e15) 100 (88e100) 19 (10e31) 38 (27e49) 100 (72e100)
>1 1 10 (4e22) 97 (82e100) 47 (34e61) 47 (34e61) 97 (82e100)
>2 2 19 (10e32) 93 (77e99) 58 (44e70) 52 (38e66) 94 (81e99)
>3 4 33 (22e47) 86 (68e96) 68 (54e79) 57 (41e72) 91 (78e97)
>4 6 51 (36e66) 72 (53e87) 85 (73e93) 70 (51e85) 86 (75e94)
>5 6 69 (50e83) 52 (33e71) 92 (81e97) 75 (51e91) 79 (68e88)
>6 2 83 (63e93) 31 (15e51) 100 (94e100) 100 (66e100) 75 (64e84)
>7 2 91 (73e97) 24 (10e44) 100 (94e100) 100 (59e100) 73 (62e82)
>8 5 96 (81e99) 17 (6e36) 100 (94e100) 100 (48e100) 71 (60e81)
CI, confidence interval; NPV, negative predictive value; PAI, Placenta Accreta Index; PPV, positive predictive value.
Rac. Placenta Accreta Index. Am J Obstet Gynecol 2015.
Research Obstetrics ajog.org
placental invasion has previously beendescribed.6,11,12,21,22 Finberg and Wil-liams11 found that number and bizarreappearance of lacunar spaces wasdirectly correlated with certainty andseverity of morbidly adherent placenta.In a recent systematic review, overallpooled sensitivity and specificity oflacunar spaces from 13 studies was 77%and 95% with an overall diagnostic ac-curacy of 0.884.17 A similar relationshiphas been shown for number of priorcesarean deliveries.2,18,23 In one of thelargest prospective series to date, Silveret al18 found that in the setting ofplacenta previa, the risk of accreta was11%, 40%, and >60% in women with 1,2, and �3 prior cesarean deliveries,respectively.
Other characteristics found to bepositively associated with morbidlyadherent placenta in our model,although to a lesser degree, includeplacental location, grade-2 lacunarspaces, smallest myometrial thickness,and bridging vessels. Both retrospectiveand prospective studies,9,11,12,14,16,24 aswell as metaanalyses and systematic re-views,17 have shown high sensitivities foreach of the above parameters. In 2000,Twickler et al12 found that a smallestmyometrial thickness <1 mm identifiedin third-trimester pregnancies at risk forplacental invasion was 100% sensitiveand 72% specific with a PPVand NPVof72% and 100%, respectively.12
343.e6 American Journal of Obstetrics & Gynecol
Hypervascularity of the uterine-bladderinterface using both 2- and 3-dimen-sional Doppler ultrasound had the bestdiagnostic performance in a recent pro-spective series of women with a priorcesarean delivery and placenta previa.9
Similarly, D’Antonio et al17 reportedthat the presence of bridging vesselsidentified with color Doppler imagingwas the most predictive ultrasoundparameter of morbidly adherentplacenta, with an overall diagnostic ac-curacy of 0.95.Assigning the PAI in clinical practice
may be helpful in interpreting thesevarious sonographic variables in light ofthe patient’s history. As an example, if awoman who has had 2 prior cesareandeliveries is found to have an anteriorplacenta previa with grade-3 lacunae,smallest myometrial thickness of 1 mm,and no bridging vessels, she wouldreceive 3 points for the prior cesareandeliveries, 1 point for anterior previa, 3.5points for grade-2 lacunae, and 0.5points for the smallest myometrialthickness of 1 mm. This would result in aPAI score of 8. Her probability of inva-sion would be 91% (95% CI 73e97%),with a sensitivity of 24%, specificity of100%, and PPV and NPV of 100% and73%, respectively. This is much higherthan her risk of invasion based onnumber of cesarean deliveries andplacental location alone, which would beonly 40%.18 Conversely, a woman with 1
ogy MARCH 2015
prior cesarean delivery (0 points), ante-rior placenta previa (1 point), grade-1lacunae (0 points), smallest myometrialthickness of 1 mm (1 point), and nobridging vessels (0 points) would have aPAI of only 2, conferring a 10% proba-bility of invasion (95% CI, 4e22%).Depending on availability of local re-sources and multidisciplinary care, re-sults from our index could thus be usedfor counseling and assist with referraldecisions.
Limitations of our study include theretrospective design. We were unable tocontrol for suspicion of invasion or im-ages recorded, which leads to certainultrasound parameters not being recor-ded. As a result, we limited the logisticregression to those patients with all pa-rameters measured (n ¼ 88) to avoidoverfitting our model. Not all women inour cohort underwent transvaginal im-aging. Although no studies have beenperformed that directly compare thediagnostic accuracy of transabdominalvs transvaginal ultrasound in the settingof suspected placental invasion, trans-vaginal ultrasound allows for a morecomplete evaluation of the lower uterinesegment and is the current recom-mended standard of care.8,25-27 There-fore, inclusion of transabdominalimaging could theoretically affect thepredictive value of our model. Addi-tionally, our model was developed onlyfor pregnancies in the third trimester

ajog.org Obstetrics Research
with prior cesarean delivery and placentaprevia or low-lying placenta, those atgreatest risk for placental invasion, andwould not apply in lower-risk pregnan-cies. Factors such as maternal age, parity,and history of other uterine surgicalprocedures that have been associatedwith morbidly adherent placenta, suchas dilation and curettage, myomectomy,and endometrial ablation,7 were notincluded in our model. It is not knownwhether ultrasound parameters used toidentify morbidly adherent placenta aresimilarly predictive for cases outside ofthe lower uterine segment or in lower-risk populations. Further studies areneeded in these populations to optimizeantenatal diagnosis of morbidlyadherent placenta. Finally, despitemethodological flaws inherent to retro-spective studies, our model provides thegroundwork for which parametersshould be prospectively evaluated.
Despite these limitations, strengths ofour study include the size of the cohort, ablinded review process, and use of his-tologic confirmation of invasion. As aresult, our model is designed to identifypatients with clinically significantplacental invasion requiring cesareanhysterectomy. Additionally, we reportprobability of invasion, which is a moreclinically relevant method of riskgradation compared to an absolute cut-off value of invasion vs no invasion. Inconclusion, our study shows that astandardized risk assessment based onnumber of previous cesarean deliveriesand ultrasound findings can identifythose women at highest risk formorbidly adherent placenta. If verifiedprospectively, assignment of the PAI maybe helpful for patient counseling anddelivery planning, all of which may ul-timately improve pregnancy outcomes
in women with morbidly adherentplacenta. -
REFERENCES
1. Hertig IC. A study of placenta accreta. J SurgGynecol Obstet 1937;64:178-200.2. Wu S, Kocherginsky M, Hibbard JU.Abnormal placentation: twenty-year analysis.Am J Obstet Gynecol 2005;192:1458-61.3. Warshak CR, Ramos GA, Eskander R, et al.Effect of predelivery diagnosis in 99 consecutivecases of placenta accreta. Obstet Gynecol2010;115:65-9.4. Grosvenor A, Silver R, Porter TF,Zempolich K. Optimal management of placentaaccreta. Am J Obstet Gynecol 2006;10:261.5. Eller AG, Porter TF, Soisson P, Silver RM.Optimal management strategies for placentaaccreta. BJOG 2009;116:648-54.6. Abuhamad A. Morbidly adherent placenta.Semin Perinatol 2013;37:359-64.7. Society of Maternal-Fetal Medicine. Placentaaccreta. Am J Obstet Gynecol 2010;203:430-9.8. American College of Obstetricians and Gy-necologists. Placenta accreta. ACOG commit-tee opinion no. 529. Obstet Gynecol 2012;120:207-11.9. Cali G, Giambanco L, Puccio G, Foriani F.Morbidly adherent placenta: evaluation of ultra-sound diagnostic criteria and differentiation ofplacenta accreta from placenta percreta. Ultra-sound Obstet Gynecol 2013;41:406-12.10. Shih JC, Palacios Jaraquemada JM, Su YN,et al. Role of three-dimensional power Doppler inthe antenatal diagnosis of placenta accreta:comparison with gray-scale and color Dopplertechniques. Ultrasound Obstet Gynecol2009;33:193-203.11. Finberg HJ, Williams JW. Placenta accreta:prospective sonographic diagnosis in patientswith placenta previa and prior cesarean section.J Ultrasound Med 1992;11:333-43.12. Twickler DM, Lucas MJ, Balis AB, et al.Color flow mapping for myometrial invasion inwomen with a prior cesarean delivery. J MaternFetal Med 2000;9:330-5.13. Comstock CH. The antenatal diagnosis ofplacental attachment disorders. Curr OpinObstet Gynecol 2011;23:117-22.14. Guy GP, Peisner DB, Timor-Tritsch IE. Ul-trasonographic evaluation of uteroplacentalblood flow patterns of abnormally located and
MARCH 2015 Ameri
adherent placentas. Am J Obstet Gynecol1990;163:723-7.15. Lerner JP, Deane S, Timor-Tritsch IE. Char-acterization of placenta accreta using transvaginalsonography and color Doppler imaging. Ultra-sound Obstet Gynecol 1995;5:198-201.16. Chou MM, Ho ESC, Lee YH. Prenataldiagnosis of placenta previa accreta by trans-abdominal color Doppler ultrasound. UltrasoundObstet Gynecol 2000;15:28-35.17. D’Antonio F, Iacovella C, Bhide A. Pre-natal identification of invasive placentationusing ultrasound: systematic review andmeta-analysis. Ultrasound Obstet Gynecol2013;42:509-17.18. Silver RM, Landon MD, Rouse DJ, et al.Maternal morbidity associated with multiplerepeat cesarean deliveries. Obstet Gynecol2006;107:1226-32.19. Wong HS, Cheung YK, Zuccollo J, et al.Evaluation of sonographic diagnostic criteria forplacenta accreta. J Clin Ultrasound 2008;36:551-9.20. Weiniger CF, Einav S, Deutsch L, Ginosar Y,Ezra Y, Eid L. Outcomes of prospectively-collected consecutive cases of antenatal-suspected placenta accreta. Int J ObstetAnesth 2013;22:273-9.21. Yang JI, Lim YK, Kim HS, Chang KH,Lee YP, Ryu HS. Sonographic findings ofplacental lacunae and the prediction of adherentplacenta in women with placenta previa totalisand prior cesarean section. Ultrasound ObstetGynecol 2006;28:178-82.22. Comstock CH, Bronsteen RA. The ante-natal diagnosis of placenta accreta. BJOG2014;121:171-81.23. Miller DA, Chollet JA, Goodwin TA. Clinicalrisk factors for placenta previa-placenta accreta.Am J Obstet Gynecol 1997;177:210-4.24. Comstock CH. Antenatal diagnosis ofplacenta accreta: a review. Ultrasound ObstetGynecol 2005;26:89-96.25. Smith RS, Lauria MR, Comstock CH, et al.Transvaginal ultrasonography for all placentas thatappear to be low-lying or over the internal cervicalos. Ultrasound Obstet Gynecol 1997;9:22-4.26. Farine D, Fox HE, Jakobson S, Timor-Tritsch IE. Vaginal ultrasound for diagnosis ofplacenta previa. Am J Obstet Gynecol1988;159:566-9.27. Lahoria K, Malhotra S, Bagga R. Trans-abdominal and transvaginal ultrasonography ofplacenta previa. Int J Gynaecol 2007;98:258-9.
can Journal of Obstetrics & Gynecology 343.e7


















