
Ultrasound-guided percutaneous cholecystostomy in high-risk surgical patients
6
Received: 26 June 2000 Accepted: 26 January 2001 Published online: 11 April 2001 © Springer-Verlag 2001 Abstract Background and aims: In critically ill patients, cholecystec- tomy is associated with a high mortality rate. The aim of this study was to evaluate the safety, efficacy and long-term outcome of ultra- sound-guided percutaneous chole- cystostomy (USGPC) in critically ill patients with acute cholecystitis. Materials and methods: Clinical re- cords of 51 patients, all considered high-risk surgical patients, with acute cholecystitis treated with USGPC between 1987 and 1999, were retrospectively reviewed. Response was defined as improve- ment in clinical symptoms and signs, and/or reduction in c-reactive protein and white blood count levels within 72 h. Long-term results were evaluated by means of clinical records and written correspondence. Results: Gallbladder stones were seen in 28 patients whereas 23 had acalculous cholecystitis. Ninety per- cent showed clinical improvement after USGPC. Cholecystectomy was performed in 16%, of which 6% af- ter recurrent cholecystitis. Recur- rence of cholecystitis occurred in 22%. Hospital mortality was 16%. None of the deaths was procedure related or related to acute cholecysti- tis alone. Major complications relat- ing to the USGPC were rare (4%), while minor catheter-related complications were quite common. Conclusions: USGPC is a procedure with few complications and a high success rate. In patients with acalculous cholecystitis as well as in many patients with calculous cholecystitis, no further treatment was needed. Keywords Acute cholecystitis · Percutaneous drainage · Ultrasound · Critically ill patients Langenbeck’s Arch Surg (2001) 386:212–217 DOI 10.1007/s004230100211 ORIGINAL ARTICLE Anna Granlund Britt-Marie Karlson Anders Elvin Ib Rasmussen Ultrasound-guided percutaneous cholecystostomy in high-risk surgical patients Introduction Acute cholecystitis is a commonly occurring disease with an annual incidence in Sweden of 5.8 per 100,000 inhabitants [1]. The incidence increases with age [2], and cholecystitis is an important contributing factor to mor- bidity and mortality in elderly and debilitated patients. Cholecystectomy, laparoscopic or conventional, is the standard treatment for acute calculous cholecystitis (ACC), with an operative mortality rate of less than 0.8% [3, 4, 5]. However, the mortality rate of cholecys- tectomy among patients with ACC rises to 14–19% in critically ill patients suffering from serious underlying diseases [6, 7]. Acute acalculous cholecystitis (AAC) is an uncom- mon but serious condition which mainly occurs in seri- ously ill patients and could be a diagnostic challenge. In 1996, AAC represented 6.5% of all patients registered with acute cholecystitis in Sweden [1]. The mortality of the disease has in some reports been twice as high as for cholecystitis due to gallstones [8]. Risk factors associat- ed with AAC include severe trauma, major surgery, sep- sis, burns, long-term fasting with or without total paren- teral nutrition, major cardiac infarctions, diabetes melli- tus and acquired immunodeficiency syndrome among A. Granlund · B.-M. Karlson ( ✉ ) I. Rasmussen Department of Surgery, University Hospital, 75185 Uppsala, Sweden e-mail: [email protected] Fax: +46-18-556808 A. Elvin Department of Diagnostic radiology, University Hospital, Uppsala, Sweden
Transcript of Ultrasound-guided percutaneous cholecystostomy in high-risk surgical patients
Received: 26 June 2000Accepted: 26 January 2001Published online: 11 April 2001© Springer-Verlag 2001
Abstract Background and aims:In critically ill patients, cholecystec-tomy is associated with a high mortality rate. The aim of this studywas to evaluate the safety, efficacyand long-term outcome of ultra-sound-guided percutaneous chole-cystostomy (USGPC) in critically ill patients with acute cholecystitis.Materials and methods: Clinical re-cords of 51 patients, all consideredhigh-risk surgical patients, withacute cholecystitis treated with USGPC between 1987 and 1999,were retrospectively reviewed. Response was defined as improve-ment in clinical symptoms and signs,and/or reduction in c-reactive protein and white blood count levelswithin 72 h. Long-term results wereevaluated by means of clinical records and written correspondence.Results: Gallbladder stones wereseen in 28 patients whereas 23 had
acalculous cholecystitis. Ninety per-cent showed clinical improvementafter USGPC. Cholecystectomy wasperformed in 16%, of which 6% af-ter recurrent cholecystitis. Recur-rence of cholecystitis occurred in22%. Hospital mortality was 16%.None of the deaths was procedure related or related to acute cholecysti-tis alone. Major complications relat-ing to the USGPC were rare (4%),while minor catheter-related complications were quite common.Conclusions: USGPC is a procedurewith few complications and a highsuccess rate. In patients withacalculous cholecystitis as well as in many patients with calculous cholecystitis, no further treatmentwas needed.
Keywords Acute cholecystitis · Percutaneous drainage · Ultrasound · Critically ill patients
Langenbeck’s Arch Surg (2001) 386:212–217DOI 10.1007/s004230100211 O R I G I N A L A RT I C L E
Anna GranlundBritt-Marie KarlsonAnders ElvinIb Rasmussen
Ultrasound-guided percutaneous cholecystostomy in high-risk surgical patients
Introduction
Acute cholecystitis is a commonly occurring diseasewith an annual incidence in Sweden of 5.8 per 100,000inhabitants [1]. The incidence increases with age [2], andcholecystitis is an important contributing factor to mor-bidity and mortality in elderly and debilitated patients.Cholecystectomy, laparoscopic or conventional, is thestandard treatment for acute calculous cholecystitis(ACC), with an operative mortality rate of less than0.8% [3, 4, 5]. However, the mortality rate of cholecys-tectomy among patients with ACC rises to 14–19% in
critically ill patients suffering from serious underlyingdiseases [6, 7].
Acute acalculous cholecystitis (AAC) is an uncom-mon but serious condition which mainly occurs in seri-ously ill patients and could be a diagnostic challenge. In1996, AAC represented 6.5% of all patients registeredwith acute cholecystitis in Sweden [1]. The mortality ofthe disease has in some reports been twice as high as forcholecystitis due to gallstones [8]. Risk factors associat-ed with AAC include severe trauma, major surgery, sep-sis, burns, long-term fasting with or without total paren-teral nutrition, major cardiac infarctions, diabetes melli-tus and acquired immunodeficiency syndrome among
A. Granlund · B.-M. Karlson (✉ )I. RasmussenDepartment of Surgery, University Hospital, 75185 Uppsala, Swedene-mail: [email protected]: +46-18-556808
A. ElvinDepartment of Diagnostic radiology, University Hospital, Uppsala, Sweden

213
others [8, 9, 10, 11, 12]. The operative mortality rate inthese critically ill patients has been reported to be ashigh as 30% [10].
To those considered as high-risk patients for chole-cystectomy, percutaneous cholecystostomy can be a safeand simple alternative treatment. The first percutaneouscholecystostomy was reported in 1980 by Radder et al.[13]. Ultrasound-guided percutaneous cholecystostomy(USGPC) is a rapid and minimally invasive procedurerequiring only local anaesthesia, and the procedure canbe performed bedside. The technique has also been per-formed under computed tomography (CT) guidance. Re-ports have shown few complications and a high successrate [14, 15, 16, 17]. The patients usually present instan-taneous improvement with regard to clinical appearanceand laboratory values.
In seriously ill patients with ACC, USGPC is often per-formed as a temporary procedure, allowing the patient'scondition to stabilise prior to an elective cholecystectomy.In patients with AAC, USGPC has by many authors beenadvocated as being preferable to surgery [16, 17, 18, 19,20, 21] and, in most cases, no further treatment is needed.USGPC also brings opportunities for antegrade cholangi-ography, which can be used for both diagnostic and evalu-ating purposes. Further on, the procedure facilitates sam-pling for bacteriologic cultures from the bile fluid.
The aim of this study was to evaluate the safety, effi-cacy and long-term outcome of USGPC in high-risk pa-tients with acute calculous or acalculous cholecystitis.
Methods
All patients treated with USGPC between January 1987 and Janu-ary 1999 were identified through a registry at the Department ofDiagnostic Radiology, University Hospital, Uppsala. The registry,with consecutive registration, contains information on the patientsnational identification number (a unique ten-digit number for ev-ery inhabitant in Sweden), ultrasound (Us) diagnosis, referral de-partment and any intervention. Clinical records were retrospec-tively reviewed. The diagnosis was based on physical examina-tion, laboratory findings and radiological imaging. Acute chole-cystitis, calculous or acalculous, was suspected upon right upperquadrant tenderness with or without local muscular rigidity, and/orelevated c-reactive protein (CRP) and leukocyte (WBC) levels.Alkaline phosphatases (ALPs) and bilirubin levels were also re-corded. Diagnosis was confirmed radiologically by abdominal CTimaging or Us. The specific radiological findings suggestive ofacute cholecystitis (thickness of the gallbladder wall, perichole-cystic fluid, tenderness over the gallbladder) were noted as well assubsequent admission for gallbladder or bile duct diseases and sur-gical procedures. Response to USGPC was defined as improve-ment in clinical symptoms and signs and/or significant reduction(>10%) in CRP and WBC levels within 72 h. Written correspon-dence was performed to those patients who were still alive inApril 1999 (n=14) with a response rate of 11 out of 14. Informa-tion on later symptoms of gallbladder or bile duct diseases andsurgical procedures was obtained. Dates of deaths were obtainedthrough linkage to the Swedish Population Registry. The patientswere followed until cholecystectomy, date of death, or April 1999.The study was approved by the local ethics committee.
Ultrasound
The drainage procedures were all performed under Us guidance. Avector or linear transducer (Acuson, Mountain View, Calif.) wasused depending on the depth of the gallbladder (Fig. 1). Afterplacing a small amount of local anaesthetic subcutaneously at thesite of the gallbladder, a skin incision was made through which thecatheter was introduced. A 7-Fr pigtail catheter was used in allcases (TCD Set, PBN Medicals, Denmark). If possible, the cathe-ter was introduced into the gallbladder after passing through theliver. The catheter was thereafter fixed, either by an internal lock-ing device or by means of a suture to the skin. The catheter wasrinsed with saline solution daily in order to prevent clogging.
The patients
In total, 51 patients with acute cholecystitis with or without gall-stones were identified as having USGPC. Of these, 59% were menand the mean age (range) was 71 years (18–94 years). All patientswere considered as high-risk surgical patients (ASA class 4) dueto serious underlying diseases or prior severe trauma (Table 1).Twelve patients were in the intensive care unit (ICU) at the time ofdiagnosis of acute cholecystitis, including five patients on me-chanical ventilators. The diagnosis of cholecystitis was settled us-
Fig. 1 Ultrasonography in a patient with calculous acute chole-cystitis
Table 1 The underlying and concomitant diagnoses among thepatients
Diagnosis Number of patients
Cardiopulmonary disorder 25Sepsis* 11Malignancies 6After surgical procedures 5Trauma 4
Total 51
*Unrelated to acute calculous cholecystitis and acute acalculouscholecystitis
214
ing Us in the majority of patients (96%), and stones in the gall-bladder were identified in 28 patients (55%). Of 51 patients, 42 re-ceived i.v. antibiotics following diagnosis. However, bile fluidsamples for bacteriological cultures were taken in 38 patients, ofwhich 22 (12 ACC, 10 AAC) cultures (58%) were positive. Thedistribution of clinical and biochemical signs indicating acute cho-lecystitis among the patients is shown in Table 2 and 3.
Results
USGPC was performed successfully in all 51 patients.The catheter was inserted transhepatically in 47 (92%)patients. In 4 patients, the individual anatomy demandeda transperitoneal route. Median drainage time was 7 days(range 1–30 days, mean 8 days). Of 51 patients, 46(90%) responded to treatment within 72 h, of which 37patients (80%) were on antibiotic treatment (Table 2). Ofthe 51 patients, 38 (75%) had a positive response withinthe first 48 h. Five patients did not respond to the treat-ment and four of them had pericholecystic fluid. All non-responding patients were on antibiotic treatment.
Ninety-three percent of patients (26/28) with ACCshowed clinical improval, whereas two did not respond.One of these two, suffering from primary liver cancerwith metastases, died in the hospital within a week dueto a myocardial infarction. The other patient developedbile peritonitis due to bile leakage after the catheter in-sertion and underwent cholecystectomy 2 days after theprocedure. The postoperative course was uneventful.
Eighty-seven percent of patients(20/23) with AAC didrespond to the treatment. All three patients who did notrespond died from their underlying diseases within a fewdays.
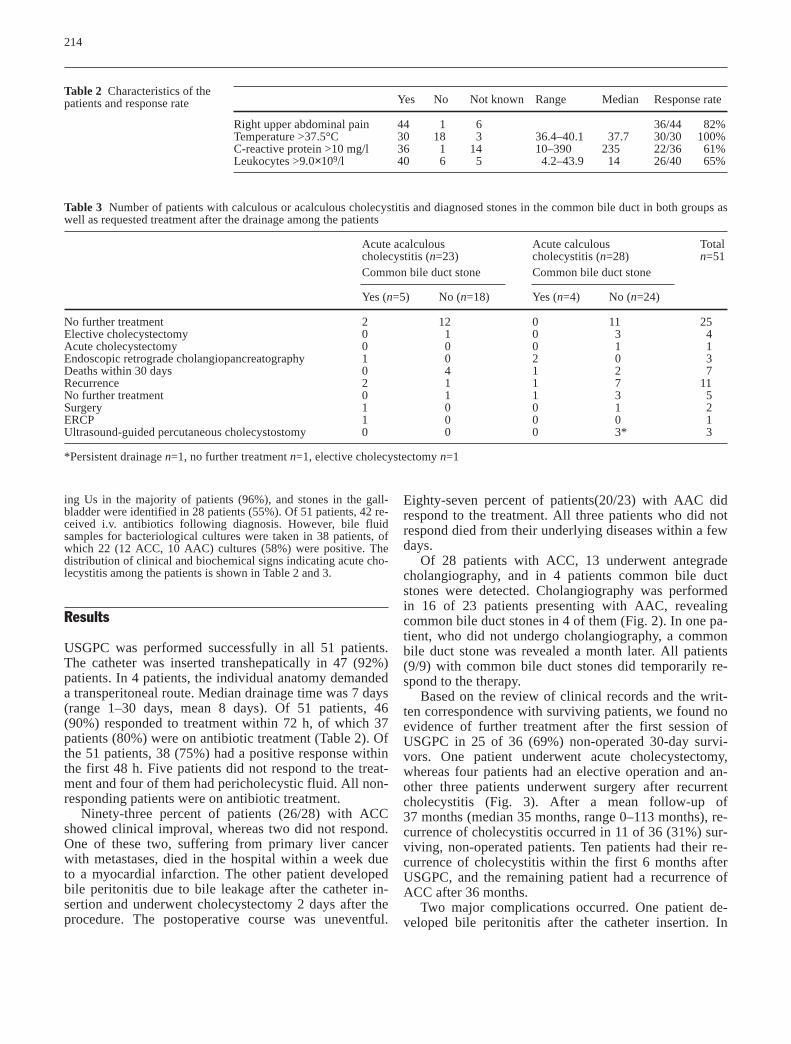
Of 28 patients with ACC, 13 underwent antegradecholangiography, and in 4 patients common bile ductstones were detected. Cholangiography was performedin 16 of 23 patients presenting with AAC, revealingcommon bile duct stones in 4 of them (Fig. 2). In one pa-tient, who did not undergo cholangiography, a commonbile duct stone was revealed a month later. All patients(9/9) with common bile duct stones did temporarily re-spond to the therapy.
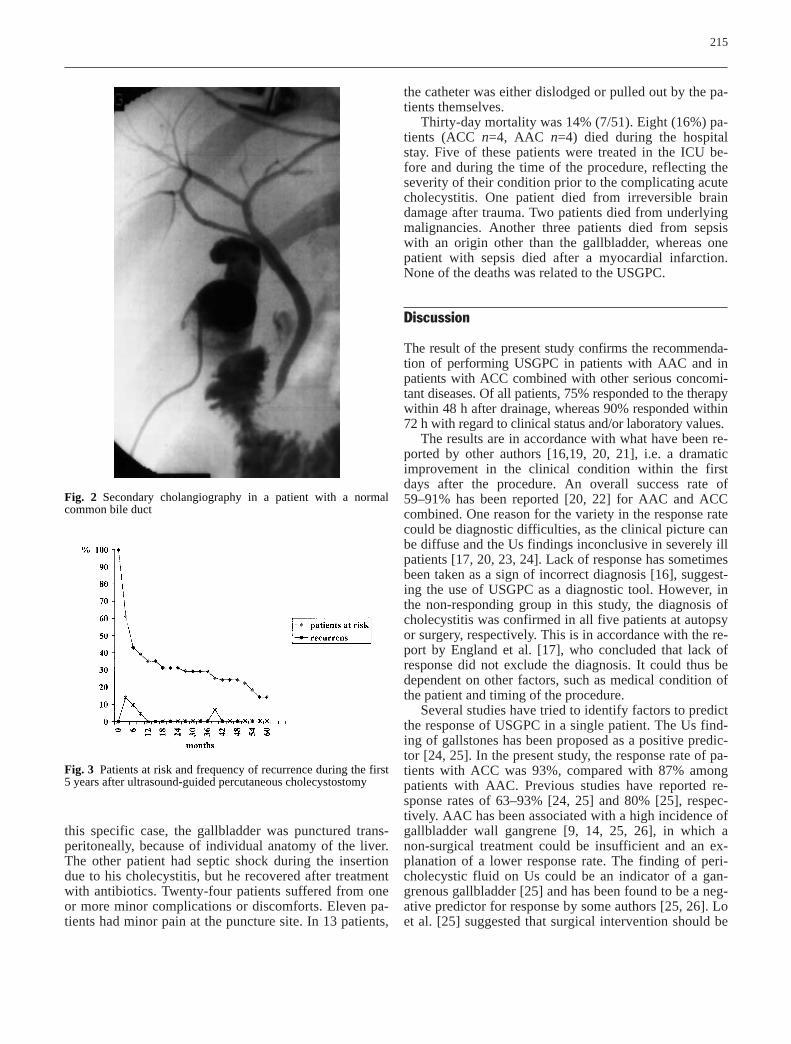
Based on the review of clinical records and the writ-ten correspondence with surviving patients, we found noevidence of further treatment after the first session ofUSGPC in 25 of 36 (69%) non-operated 30-day survi-vors. One patient underwent acute cholecystectomy,whereas four patients had an elective operation and an-other three patients underwent surgery after recurrentcholecystitis (Fig. 3). After a mean follow-up of37 months (median 35 months, range 0–113 months), re-currence of cholecystitis occurred in 11 of 36 (31%) sur-viving, non-operated patients. Ten patients had their re-currence of cholecystitis within the first 6 months afterUSGPC, and the remaining patient had a recurrence ofACC after 36 months.
Two major complications occurred. One patient de-veloped bile peritonitis after the catheter insertion. In
Table 2 Characteristics of thepatients and response rate
Table 3 Number of patients with calculous or acalculous cholecystitis and diagnosed stones in the common bile duct in both groups aswell as requested treatment after the drainage among the patients
Acute acalculous Acute calculous Totalcholecystitis (n=23) cholecystitis (n=28) n=51Common bile duct stone Common bile duct stone
Yes (n=5) No (n=18) Yes (n=4) No (n=24)
No further treatment 2 12 0 11 25Elective cholecystectomy 0 1 0 3 4Acute cholecystectomy 0 0 0 1 1Endoscopic retrograde cholangiopancreatography 1 0 2 0 3Deaths within 30 days 0 4 1 2 7Recurrence 2 1 1 7 11No further treatment 0 1 1 3 5Surgery 1 0 0 1 2ERCP 1 0 0 0 1Ultrasound-guided percutaneous cholecystostomy 0 0 0 3* 3
*Persistent drainage n=1, no further treatment n=1, elective cholecystectomy n=1
Yes No Not known Range Median Response rate
Right upper abdominal pain 44 1 6 36/44 82%Temperature >37.5°C 30 18 3 36.4–40.1 37.7 30/30 100%C-reactive protein >10 mg/l 36 1 14 10–390 235 22/36 61%Leukocytes >9.0×109/l 40 6 5 4.2–43.9 14 26/40 65%
the catheter was either dislodged or pulled out by the pa-tients themselves.
Thirty-day mortality was 14% (7/51). Eight (16%) pa-tients (ACC n=4, AAC n=4) died during the hospitalstay. Five of these patients were treated in the ICU be-fore and during the time of the procedure, reflecting theseverity of their condition prior to the complicating acutecholecystitis. One patient died from irreversible braindamage after trauma. Two patients died from underlyingmalignancies. Another three patients died from sepsiswith an origin other than the gallbladder, whereas onepatient with sepsis died after a myocardial infarction.None of the deaths was related to the USGPC.
Discussion
The result of the present study confirms the recommenda-tion of performing USGPC in patients with AAC and inpatients with ACC combined with other serious concomi-tant diseases. Of all patients, 75% responded to the therapywithin 48 h after drainage, whereas 90% responded within72 h with regard to clinical status and/or laboratory values.
The results are in accordance with what have been re-ported by other authors [16,19, 20, 21], i.e. a dramaticimprovement in the clinical condition within the firstdays after the procedure. An overall success rate of59–91% has been reported [20, 22] for AAC and ACCcombined. One reason for the variety in the response ratecould be diagnostic difficulties, as the clinical picture canbe diffuse and the Us findings inconclusive in severely illpatients [17, 20, 23, 24]. Lack of response has sometimesbeen taken as a sign of incorrect diagnosis [16], suggest-ing the use of USGPC as a diagnostic tool. However, inthe non-responding group in this study, the diagnosis ofcholecystitis was confirmed in all five patients at autopsyor surgery, respectively. This is in accordance with the re-port by England et al. [17], who concluded that lack ofresponse did not exclude the diagnosis. It could thus bedependent on other factors, such as medical condition ofthe patient and timing of the procedure.
Several studies have tried to identify factors to predictthe response of USGPC in a single patient. The Us find-ing of gallstones has been proposed as a positive predic-tor [24, 25]. In the present study, the response rate of pa-tients with ACC was 93%, compared with 87% amongpatients with AAC. Previous studies have reported re-sponse rates of 63–93% [24, 25] and 80% [25], respec-tively. AAC has been associated with a high incidence ofgallbladder wall gangrene [9, 14, 25, 26], in which anon-surgical treatment could be insufficient and an ex-planation of a lower response rate. The finding of peri-cholecystic fluid on Us could be an indicator of a gan-grenous gallbladder [25] and has been found to be a neg-ative predictor for response by some authors [25, 26]. Loet al. [25] suggested that surgical intervention should be
215
this specific case, the gallbladder was punctured trans-peritoneally, because of individual anatomy of the liver.The other patient had septic shock during the insertiondue to his cholecystitis, but he recovered after treatmentwith antibiotics. Twenty-four patients suffered from oneor more minor complications or discomforts. Eleven pa-tients had minor pain at the puncture site. In 13 patients,
Fig. 2 Secondary cholangiography in a patient with a normalcommon bile duct
Fig. 3 Patients at risk and frequency of recurrence during the first5 years after ultrasound-guided percutaneous cholecystostomy

216
considered if pericholecystic fluid is present in a non-responder. Four of the five non-responders in the presentstudy had pericholecystic fluid on Us or CT comparedwith 12 of 46 (26%) in the responding group, which sup-ports the theory of pericholecystic fluid as a negativepredictor for response. However, others have suggestedpericholecystic fluid to be a positive predictor [17, 24]and still others are uncertain of its significance at all assmall amounts of ascites are found in many severely illpatients [20]. Another suggested predictor of positive re-sponse has been right upper quadrant abdominal tender-ness or pain [17, 20]; this was confirmed in the presentstudy. Of the 46 positive responders, 41 (89%) had rightupper quadrant abdominal pain compared with 3 of 5 ofthe non-responders.
The drainage time is shorter in this study, with a meandrainage time of 8 days (median 7 days), than in severalprevious studies [16, 17, 20, 27]. Boland et al. [20] pro-posed a minimum drainage time of 3 weeks to be opti-mal, thereby avoiding the risk of bile leakage at catheterremoval. Despite our shorter drainage time, we found noevidence of bile leakage due to an early removal. Fur-thermore, there was no difference in drainage time be-tween patients with recurrence and those without.
The recurrence rate of 31% (11/36) among non-operat-ed surviving patients is in accordance with reported ratesfound in the literature [27]. Different thresholds for sur-gery could be one explanation for the variability of re-ported rates of recurrence. Only three patients with ACCwere found suitable for elective cholecystectomy and, af-ter a recurrence, another two patients had an elective op-
eration. The majority of our patients with recurrence hadACC, as also has been demonstrated by other authors[27]. Two of the three patients with recurrence after AAChad a stone in the common bile duct. Three (27%) of ourrecurrences underwent cholecystectomy, and no compli-cations to the surgical procedures were found.
USGPC has been suggested as a safe alternative tocholecystectomy because of its effectiveness and lowcomplication rate. In the literature, a complication rate of7.8–26% [28, 29] has been reported. The majority ofthese complications are minor, often consisting of painsat the place of the puncture. Major complications oc-curred in two patients (4%) in this study and are in ac-cordance with others [14, 20, 25, 28]. Dislodgement ofthe catheter was the most common minor complication(n=13), leading to an undesired shortage of the drainageperiod. In the majority of these patients, a skin suturewas used to secure the catheter.
The total mortality rate was 16%; none of the deathswere evidently related to the procedure. As the patientsincluded in the study by definition were at high risk, theresult is in line with previous studies, showing a widerange in mortality rate of 2–59% [14, 17]. The proce-dure-related mortality rate reported in the literature isvery low, below 2% [17, 21, 22, 24].
In summary, according to the results of the presentstudy, USGPC is an effective treatment for both ACC andAAC in high-risk surgical patients. In AAC, no furthertreatment is needed in most patients, as in several critical-ly ill patients with ACC. The method is safe with lowprocedure-related mortality and few major complications.
References
1. Centre of Epidemiology (1996) The inpatient registry. The National Boardof Health and Welfare, Stockholm
2. Glenn F (1981) Surgical managementof acute cholecystitis in patients 65 years of age and older. Ann Surg 193:56–59
3. Pickleman J, Gonzales RP (1986) The improving results of cholecystec-tomy. Arch Surg 121:930–934
4. McSherry CK (1989) Cholecystecto-my: the gold standard. Am J Surg158:174–178
5. Gilliland TM, Traverso W (1990)Modern standards for comparison ofcholecystectomy with alternative treatments for symptomatic cholelithia-sis with emphasis on long term relief of symptoms. Surg Gynecol Obstet170:39–44
6. Huber DF, Martin EW Jr, CoopermanM (1983) Cholecystectomy in elderlypatients. Am J Surg 146:719–722
7. Houghton PW, Jenkinson LR, Donaldson LA (1985) Cholecystecto-my in the elderly: a prospective study.Br J Surg 72:220–222
8. Glenn F, Becker CG (1982) Acuteacalculous cholecystitis. An increasingentity. Ann Surg 195:131–136
9. Howard RJ (1981) Acute acalculouscholecystitis. Am J Surg 141:194–198
10. Frazee RC, Nagorney DM, Mucha P Jr(1989) Acute acalculous cholecystitis.Mayo Clin Proc 64:163–167
11. Iannuzzi C, Belghiti J, Erlinger S, et al (1990) Cholangitis associated withcholecystitis in patients with acquiredimmunodeficiency syndrome. Arch Surg 125:1211–1213
12. Savoca PE, Longo WE, Zucker KA, etal (1990) The increasing prevalence ofacalculous cholecystitis in outpatients.Results of a 7-year study. Ann Surg211:433–437
13. Radder RW (1980) Ultrasonicallyguided percutaneous catheter drainagefor gallbladder empyema. Diagn Imag-ing 49:330–333
14. Vogelzang RL, Nemcek AA Jr (1988)Percutaneous cholecystostomy: diag-nostic and therapeutic efficacy. Radiology 168:29–34
15. McGahan JP, Lindfors KK (1989) Percutaneous cholecystostomy: an al-ternative to surgical cholecystostomyfor acute cholecystitis? Radiology173:481–485
16. Vauthey JN, Lerut J, Martini M, et al(1993) Indications and limitations ofpercutaneous cholecystostomy foracute cholecystitis. Surg Gynecol Obstet 176:49–54
217
17. England RE, McDermott VG, SmithTP, et al (1997) Percutaneous chole-cystostomy: who responds? Am J Roentgenol 168:1247–1251
18. Eggermont AM, Lameris JS, Jeekel J(1985) Ultrasound-guided percutane-ous transhepatic cholecystostomy for acute acalculous cholcystitis. Arch Surg 120:1354–1356
19. Shirai Y, Tsukada K, Kawaguchi H, et al (1993) Percutaneous transhepaticcholecystostomy for acute acalculouscholecystitis. Br J Surg 80:1440–1442
20. Boland GW, Lee MJ, Leung J, et al(1994) Percutaneous cholecystostomyin critically ill patients: early responseand final outcome in 82 patients. Am J Roentgenol 163:339–342
21. van Overhagen H, Meyers H, TilanusHW, et al (1996) Percutaneous chole-cystostomy for patients with acute cholecystitis and an increased surgicalrisk. Cardiovasc Intervent Radiol19:72–76
22. Boggi U, Di Candio G, Campatelli A,et al (1999) Percutaneous cholecystos-tomy for acute cholcystitis in criticallyill patients. Hepatogastroenterology46:121–125
23. Lee MJ, Saini S, Brink JA, et al (1991)Treatment of critically ill patients with sepsis of unknown cause: value of percutaneous cholecystostomy. Am J Roentgenol 156:1163–1166
24. Browning PD, McGahan JP, Gerscovich EO (1993) Percutaneouscholecystostomy for suspected acutecholcystitis in the hospitalized patient.J Vasc Interv Radiol 4:531–537
25. Lo LD, Vogelzang RL, Braun MA, etal (1995) Percutaneous cholecystosto-my for the diagnosis and treatment ofacute calculous and acalculous chol-cystitis. J Vasc Interv Radiol6:629–634
26. Teplick SK, Harshfield DL, BrandonJC, et al (1991) Percutaneous chole-cystostomy in critically ill patients.Gastrointest Radiol 16:154–156
27. Hamy A, Visset J, Likholatnikov D, et al (1997) Percutaneous cholecystos-tomy for acute cholecystitis in critical-ly ill patients. Surgery 121:398–401
28. Teplick SK, Brandon JC, Wolferth CC,et al (1990) Percutaneous interventio-nal gallbladder procedures: personalexperience and literature review. Gastrointest Radiol 15:133–136
29. Kiviniemi H, Makela JT, Autio R, et al (1998) Percutaneous cholecystos-tomy in acute cholecystitis in high-riskpatients: an analysis of 69 patients. Int Surg 83:299–302


















