Ultrasound-Guided Internal Jugular Access

of 8
-
Upload
matias-flamm -
Category
Documents
-
view
213 -
download
0
Transcript of Ultrasound-Guided Internal Jugular Access
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
1/8
Ultrasound-Guided Internal Jugular Access*
A Proposed Standardized Approach andImplications for Training and Practice
David Feller-Kopman, MD, FCCP
In 2001, the Agency for Healthcare Research and Quality recommended the use of ultrasound for the placement of central venous catheters (CVCs) as one of their 11 practices to improve patientcare. These recommendations were based on the results of several randomized clinical trialsshowing significantly improved overall success as well as reductions in complications. This article
will describe the practical aspects of using ultrasound to guide placement of CVCs in the internal jugular vein in a “how I do it” approach, as well as review the practice management and trainingaspects related to incorporating ultrasound into daily practice.
(CHEST 2007; 132:302–309)
Key words: central venous catheter; complications; internal jugular vein; outcomes; ultrasound
Abbreviations: CPT current procedural terminology; CVC central venous catheter; IJ internal jugular
More than 5 million central venous catheters
(CVC) are placed each year in the UnitedStates, with an associated complication rate of 15%.1,2 Mechanical complications such as arterialpuncture and pneumothorax are seen in up to 21%,and up to 35% of insertion attempts are not success-ful.3–5 The risk of complications depends on severalfactors, including (but not limited to) operator expe-rience, urgency of placement, as well as patientfactors such as obesity, prior difficult cannulation,and coagulopathy.4,6,7 Although the above-men-tioned studies were performed in the 1970s throughthe 1990s, there have been several more prospective/
randomized trials,8–16 as well as two metaanaly-
ses17,18 that suggest the use of ultrasound has been
associated with a reduction in complication rate andan improved first-pass success when placing cathe-ters in the internal jugular (IJ) vein. Although factorsother than the use of ultrasound may be responsiblefor the improved outcomes, these data have led theAgency for Healthcare Research and Quality torecommend the use of ultrasound as one of their 11practices to improve patient care in their landmark2001 publication, “Making Health Care Safer: aCritical Analysis of Patient Safety Practices.”19,20 TheNational Institute of Clinical Excellence21 in theUnited Kingdom has also fully supported the use of
ultrasound guidance for CVC placement.Unfortunately, the incorporation of these recom-
mendations into clinical practice has been met withresistance. A survey of 250 anesthetists in the UnitedKingdom found that 41% disagreed or strongly disagreed with the recommendation that ultrasoundimaging should be the preferred method for inser-tion of a CVC into the IJ vein.22 Although 84% of respondents believed that those using ultrasoundimaging should have appropriate training, 67% of respondents believed the level of training providedfor ultrasound-guided CVC placement was inade-
*From the Medical Procedure Service, Harvard Medical School,Boston, MA.The author has no conflict of interest to disclose.Manuscript received November 7, 2006; revision accepted Feb-ruary 17, 2007.Reproduction of this article is prohibited without written permissionfrom the American College of Chest Physicians (www.chestjournal.org/misc/reprints.shtml).Correspondence to: David Feller-Kopman, MD, FCCP, Interven-
tional Pulmonology, Beth Israel Deaconess Medical Center, OneDeaconess Rd, Suite 201, Boston, MA 02215; e-mail:[email protected]: 10.1378/chest.06-2711
CHEST Topics in Practice Management
302 Topics in Practice Management
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
2/8
quate.22 Likewise, a study 23 in the United States alsofound that 15% of surgery, anesthesia, emergency medicine, internal medicine, and family medicinehousestaff used ultrasound guidance for most CVCplacements.
This article will discuss the practical aspects of performing ultrasound-guided CVC placement, andaddress recommendations for training in ultrasound-
guided CVC placement. The reader is referred to theabove-referenced studies for detailed discussionsconcerning the improvement in success and reduc-tion in complications with the use of ultrasound forCVC placement. Additionally, as the data suggestingultrasound guidance for other sites, including thesubclavian, femoral, and axillary veins, are less ro-bust, discussion will focus on the use of ultrasoundfor IJ CVCs.
Ultrasound-Guided IJ CVC Placement:How I Do It
Two types of ultrasound guidance are available:Doppler and B-mode (also referred to as two-dimensional ultrasound). Doppler ultrasound trans-forms the sound waves reflected from a movingobject (RBC in this case) into an amplified audiosignal. The respirophasic venous waveform is dis-tinctly different from arterial pulsations, and Dopp-ler ultrasound is frequently used to assess arterialpatency in the lower extremities and aid in arterialcatheters. The data behind Doppler ultrasound for
vascular access, however, is associated with a longerlearning curve than B-mode ultrasound, longer in-sertion times, and higher costs.24–26As such, IJ CVCcatheter placement is performed with B-mode ultra-sound; from here on, the generic reference to ultra-sound will imply B-mode.
B-mode ultrasound converts the reflected sound waves into a real-time gray scale image. Fluid ( ie,blood) is hypoechoic and appears dark on the screen, while tissue is more isoechoic and appears gray. TheIJ vein is typically seen anterior and lateral to theartery; however, significant anatomic variation exists
where the vein can overly the artery and even bemedial to the artery.27,28 The IJ vein and artery canbe distinguished by the fact that the vein is com-pressible, nonpulsatile, and distensible by the Tren-delenberg position or the Valsalva maneuver. Theuse of ultrasound is an excellent teaching tool todemonstrate the following: (1) excessive pressureduring carotid palpation decreases IJ vein diameter(one cannot move the artery medially away from the vein as they lie in the same sheath); (2) extremecontralateral head rotation can decrease IJ vein diam-eter and increase overlap on the carotid artery; and (3)
the Trendelenberg position and correct head position-ing can significantly increase IJ vein diameter.29–32
I recommend that one perform an ultrasoundassessment of the anticipated side prior to creating asterile field in order to assess the degree of overlap of the carotid artery by the IJ vein, the compressibility of the vein, and the presence of internal echoes thatmay signify clot. If there is significant overlap of the
carotid artery, the operator should try to reexaminethe neck with the head in the neutral position,instead of with the head turned to the contralateralside.31,32 If the vein is not compressible or a clot is visualized, the other IJ vein should be examined.Color power Doppler can also be used to visualizethe distinct arterial and venous pulsations, althoughthere have not been any studies ascribing specificbenefit to its use.
Once the appropriate vein is selected, the site issterilized and draped as per standard technique withfull barrier precautions33 and the ultrasound probe is
placed in a sterile sheath. This step generally re-quires an assistant to hold the probe vertically andapply conducting gel to the uncovered probe. Thesterile operator can also drop sterile conducting gelon the probe. The operator then inserts a hand intothe sheath, holds the probe, and then inverts thesheath over the probe, making the probe and cablesterile. Additional gel is then placed on the outside of the sheath to ensure adequate coupling.
The two most commonly used methods for ultra-sound guidance are the “one-handed” or the “three-handed” methods. In the one-handed method, the
operator controls the ultrasound probe with thenondominant hand and the needle with the domi-nant hand. The three-handed method requires anassistant (with full sterile barrier precautions) to holdthe probe while the operator controls the needle andperforms the procedure under real-time guidance.The one-handed method is quite easy to learn,improves first-pass success and overall success whencompared with the three-handed method,34 and isthe method we currently teach to our fellows. Usingthe ultrasound to mark the skin and proceed withoutreal-time guidance is not recommended given the
significant increase in success rates for dynamicguidance as compared with the “X marks the spot”technique.34
Regardless of the method used, the IJ vein andcarotid artery are identified with ultrasound andcentered on the screen. The lidocaine needle is theninserted through the skin directly anterior to the vessel (in the center of the probe), and the wheal of subcutaneous lidocaine is visualized with the ultra-sound as an enlarging hypoechoic area. It is oftenhelpful to “jiggle” the lidocaine needle to improve visualization of the hyperechoic needle. As the pro-
www.chestjournal.org CHEST / 132 / 1 / JULY, 2007 303
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
3/8
cedure is performed in real-time, a “finder” needle isnot required, and the introducer needle is theninserted in the same location. The only caveat oneneeds to be aware of for the one-handed method isthat the operator usually needs to put down theultrasound probe in order to make the skin insertionsite taught for easy passage of the introducer needle.Once the introducer needle is through the skin, theprobe is picked up with the nondominant hand andused to guide the needle into the vessel. The intro-ducer needle will indent the anterior IJ vein walland, depending on the diameter of the vessel, may penetrate the posterior wall, resulting in a flash of venous blood on withdrawal of the needle. As such,orienting the patient’s neck as well as the ultrasoundprobe in such a way as to minimize arterial overlap isimportant. The primary advantage of ultrasound inthis setting is that this can be visualized.
Passage of the introducer needle into the IJ vein
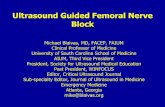
can be performed either with a transverse (short axis) view or a longitudinal (long axis) view (Fig 1).Benefits of the transverse view are that it is generally associated with a shorter learning curve and it can beeasier to visualize small vessels. The primary advan-tage of the longitudinal view is allows better visual-ization of the advancing needle tip, which may reduce perforation of the posterior vessel wall. It isfor this reason that the longitudinal view is recom-mended by the American College of Emergency Physicians.35 If using the transverse view, it is crucialto follow the advancing needle tip with the ultra-sound, making sure the plane of the ultrasound is nottoo proximal or distal. Some ultrasound units canprovide simultaneous transverse and longitudinal views.
One can also use a needle guide to help withinsertion of the introducer needle. This is a piece of plastic that angles the needle so it will intersect thecenter of the vessel. A randomized trial36 found thatneedle guides were associated with improved first-pass and second-pass success rates, but no differencein arterial sticks when compared to ultrasound-
guided CVC placement without the use of a needleguide. This being said, the needle guides can beslightly cumbersome; and once experienced withultrasound-guided CVC placement, additional ben-efit may not be present.
Once the IJ vein is entered with the introducerneedle, the ultrasound probe is placed on the fieldand the typical modified Seldinger technique is usedto place the CVC. A study 37 suggested immediateuse of the ultrasound after the procedure to confirmline placement and rule out pneumothorax. Obviousbenefits include being able to use the line immedi-
ately, instead of waiting for a chest radiograph,minimizing radiation exposure, and the lack of needto reposition the patient.
Ultrasound Machine Requirements
Over the last several years, ultrasound machineshave become quite small and portable. Although not
Figure 1. Top, A: Transverse view showing the IJ vein anteriorand lateral to the carotid artery. Note the significant overlap of the artery. Center, B: Same image as seen in top with lesscontralateral head rotation producing less overlap of the artery.
Bottom, C: Longitudinal view of the IJ vein.
304 Topics in Practice Management
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
4/8
essential, this portability makes these smaller ma-chines extremely well suited for the ICU environ-ment, especially when procedures need to be per-formed in geographically separate units. Severalmachines are available, each with their own pros andcons. For vascular access, one should use a 7.5- to10-MHz linear array transducer because this pro- vides excellent resolution and sufficient penetration.
Some ultrasound units are specifically made for vascular access, whereas other units allow the trans-ducers to be interchanged, permitting the sonogra-pher to use the same machine for pleural/chest,cardiac (including transesophageal echocardiography),and abdominal ultrasound. Although not necessary,color power Doppler is a useful added feature to thestandard vascular ultrasound unit, and if one plans onperforming more advanced ultrasound/echocardiogra-phy, the availability of M-mode, computation software,and videotape storage may be beneficial.
In addition to the ultrasound unit and transducer,
one will need to invest in the sterile sheaths andsterile ultrasound gel. Peripherals such as largermonitors, docking stations, needle guides, and aprinter may be nice to have but are not essential. Asdiscussed below, in order to properly bill for ultra-sound-guided CVC placement, documentation of theultrasound image with patient identifiers is required.This can be either electronic or on paper, andtherefore one will need either a printer to place animage in the medical record, or a method of trans-ferring the ultrasound images to a computer. Clearly,image storage requires disk space, with each image
being approximately 902 kilobytes. Over a 1-yearperiod, we archived 1.7 gigabytes for our chest and vascular images. Many hospitals now have picturearchiving and communication systems, and integra-tion with these systems is certainly possible. Addi-tionally, images can be “burned” onto inexpensivecompact discs for permanent storage as well.
Implications for Training
The use of ultrasound is not limited to radiologists.
The American Medical Association policy on privi-leging for ultrasound imaging states the following38:
Ultrasound imaging is within the scope of practice of appro-priately trained physicians. . . broad and diverse use andapplication of ultrasound imaging technologies exist in med-ical practice. . . privileging of the physician to perform ultra-sound imaging procedures in a hospital setting should be afunction of hospital medical staffs and should be specifically delineated on the Department’s Delineation of Privilegesform. . . each hospital medical staff should review and ap-prove criteria for granting ultrasound privileges based onbackground and training for the use of ultrasound technology and strongly recommends that these criteria are in accor-
dance with recommended training and education standardsdeveloped by each physician’s respective specialty.
It is therefore our responsibility to develop trainingguidelines and incorporate them into our daily prac-tice as well as our fellowship programs.
The American College of Emergency Physiciansand the American College of Surgeons have set the
standard by developing policy statements addressingthe scope of practice, training and proficiency rec-ommendations, quality improvement, and documen-tation issues regarding the use of ultrasonography inthe emergency setting.39,40 Both of these documentsstrongly support the use of ultrasound by membersof their societies and address ways to obtain andmaintain competency, as well as ensuring quality control.
To gain the skills required to incorporate ultra-sonography in clinical practice, the nonradiologistneeds to become proficient in both cognitive and
psychomotor skill sets. Training in image acquisitionand interpretation needs to include didactic lectures,demonstrations and, most importantly, proctoring by a skill sonographer.
As compared to the broad use of ultrasound in thetrauma setting, for example, two key factors allow fora much more rapid learning curve for ultrasoundguidance for CVC placement. Firstly, ultrasound-guided CVC placement is not performed as a diag-nostic test as is the focused abdominal sonography for trauma examination or echocardiography, andtherefore the clinical implications that result from
interpretation of the ultrasound image are signifi-cantly less. Secondly, if the CVC was going to beplaced anyway, ultrasound imaging can only serve toimprove outcome. That is to say, misinterpretation of ultrasound imaging may not adversely affect out-come when compared to placing a CVC with thelandmark technique. For example, even if an intralu-minal thrombus is missed and the line is attempted,it would have been attempted at that site without theaid of ultrasound. Nonetheless, there is always someelement of diagnosis in all cases. For example, if athrombus is seen in the right IJ, in addition to
perhaps placing the catheter in the left IJ, appropri-ate evaluation and treatment of the right IJ thrombusis required.
For a single application, the American College of Emergency Physicians suggests 3 to 4 h of didactics,2 to 4 h of laboratory training, and 25 proctoredexaminations.39 Didactics should include lectures onthe basic physics and principles of ultrasound,“knobology” (how to actually work the ultrasoundmachine), image acquisition, identification and inter-pretation of ultrasound artifacts, identification of therelevant anatomy, and knowledge of anatomic varia-
www.chestjournal.org CHEST / 132 / 1 / JULY, 2007 305
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
5/8
tion. From the trauma literature, an 8-h courseincluding 4 h of didactic and 4 h of proctoredexaminations on 15 normal patients, followed by 50trauma examinations proctored by credentialedsonographer or verified by standard diagnostic eval-uations was shown to be sufficient to produce well-trained trauma surgeon sonographers.41 Others42
suggest 8 h of didactics, 10 normal proctored exam-inations, and 10 proctored, focused abdominalsonography for trauma examinations may be ade-quate, depending on the prevalence of the diseasebeing sought (hemoperitoneum in this study).
Clearly there is some aspect of gaining a proce-dural skill that is numbers based. For CVC insertion,the only data available relating experience to com-plications come from the preultrasound era, andsuggest that operators who have performed 50insertions have half the complication rate of opera-tors who have performed 50 insertions.4 The
Royal College of Radiology recommends 25 lineinsertions but also acknowledges that “differenttrainees will acquire the necessary skills at differentrates and the end point of the training programshould be judged by an assessment of competen-cies.”43 For bronchoscopy and other interventionalpulmonary procedures, the numbers published by the American College of Chest Physicians44 aregenerally less, in the range of 10 to 20 line insertions.
Given the rapid learning curve for US guidance of CVCs, especially for the physician who is already experienced in the landmark method of CVC place-
ment, I would suggest approximately 2 h of didactics,2 h of laboratory training, and 5 to 10 proctoredexaminations. It should be pointed out that thesenumbers are based on the above suggestions as well ourexperience with a medical procedure service. Clearly,these suggestions should be prospectively validated with trials comparing a group who receives formaleducation/simulation training to a group educatedthrough other means such as mentorship. Laboratory training should include exposure to a variety of ultra-sound units to ensure familiarity with knobology, exam-ination of normal vascular anatomy on healthy volun-
teers, as well as hands-on simulation with vascularaccess models. Available models range in sophisticationfrom Jell-O (Kraft Foods; Northfield, IL)/Metamucil(Proctor & Gamble; Cincinnati, OH)/Penrose (Sher- wood-Davis & Geck; St. Louis, MO) drains, to the BluePhantom (www.bluephantom.org) [Blue PhantomLLC; Kirkland, WA] to CentralLineMan (http://www.simulab.com/CentraLineMan.htm) [Simulab Corpora-tion; Seattle, WA]. Ideally, some of the laboratory training would include visualization of abnormal anat-omy ( ie, the obese patient, intraluminal thrombus, orsignificant overlay of the carotid artery by the IJ vein).
The 5 to 10 proctored examinations should be brokendown into 3 to 5 ultrasound examinations of normalanatomy/vascular access models, followed by 5 to 7proctored procedures on vascular access models/simu-lators. For the physician who is already an expert atCVC placement, I recommend two proctored exami-nations on real patients followed by review of the nextfive ultrasound-guided CVCs. This would include re- viewing the stored static picture/videotape as well asoutcome (success, complications, number of needlepasses), and discussion about factors that may haveinfluenced the outcome. Additionally, I recommend apostinstruction assessment of the basics covered in thedidactic and hands-on session. This can include staticimages and videotape, asking the operator to identify anatomy, as well as questions relating to the use of theultrasound unit. These numbers are clearly subjective,as are other procedural recommendations based onnumber,44 and the main determinant in determining
competence should be the evaluation of the proctor.Additional cognitive instruction can be provided
via textbooks, continuing medical education courses/ syllabi, digital video disk, and Web-based curricula.Continuous quality improvement measures need tobe in place such that all complications are reviewedin addition to several random cases during thelearning period. Skill maintenance is also crucial, andat least 10 ultrasound-guided CVCs should be per-formed each year in order to maintain proficiency.
All of these issues have clear implications oncredentialing. As stated above, privileging is a localhospital issue. Credentialing committees will need toreview their policy and likely incorporate some for-mal training to ensure quality. Most likely, theprocess will be department specific ( ie, the Depart-ment of Medicine signing off on members of thePulmonary and Critical Care Division). The issue of “grandfathering” also needs to be addressed becausethere are clearly physicians who have been usingultrasound for CVC placement for some time. It may be sufficient for this group to just take a quick quizdocumenting their knowledge, or even just verify
they have performed “X” number of ultrasound-guided CVC placements without incident.
It remains crucial that operators still receive train-ing and become proficient in the standard/landmarkmethod of CVC insertion.21 Although one can makethe argument that learning the ultrasound-guidedtechnique first will make operators dependant ontechnology, it has been our experience that theanatomic knowledge gained by using ultrasoundmakes one a better operator when the ultrasound isnot available, such as may be the case during acardiac arrest.
306 Topics in Practice Management
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
6/8
Billing and Documentation
The American Medical Association also supportsreimbursement for “appropriately trained physicians.”It is the physicians’ responsibility to review the currentprocedural terminology (CPT) codes with their localbilling expert as well as their local third-party payers asreimbursements vary between regions, and even within
a state. The codes most commonly used codes forultrasound-guided CVC placement include 36556 and76937. Though the reimbursements vary regionally,CPT codes are created through the American MedicalAssociation and are the same throughout the UnitedStates. Code 36556 describes “insertion of nontunneledcentrally inserted central venous catheter; age 5 yearsor older” and has an associated Medicare payment of approximately $132–140 (facility, in Massachusetts,Greater Boston area) [https://catalog.ama-assn.org/ Catalog/cpt/cpt_search.jsp?_requestid 244532;http://www.cms.hhs.gov/apps/pfslookup/]. Code 76937
describes “ultrasound guidance for vascular access re-quiring ultrasound evaluation of potential access sites,documentation of selected vessel patency, concurrentreal-time ultrasound visualization of vascular needleentry, with permanent recording and reporting (Listseparately in addition to code for primary procedure)”and has an associated Medicare payment of approxi-mately $35–40 (facility, in Massachusetts, Greater Bos-ton area) [see above Web sites]. It should be noted,however, that 76937 includes the technical componentassociated with the procedure (supplies, technicalstaff). The professional component is billed by using
the “-26” modifier. In metropolitan Boston, the reim-bursement for code 76937 is $39.94 ($22.26 technical,$17.68 professional component) [http://www.cms.hhs.gov/apps/pfslookup/].
As with all billing practices, it is the physician’sresponsibility to ensure proper billing and documen-tation, and the reader is urged to review localrequirements with their insurance companies andbilling experts. It is also crucial to discuss reimburse-ment with ones third-party payers as they may wishto have a letter from the chief of radiology at yourinstitution stating you have achieved competency.
This is yet another reason why our societies need totake an active role in advocating for our own ability to determine competency.
In addition to using the proper CPT codes, ade-quate documentation is a must. For ultrasound,either a hard copy or electronic copy of the pertinentimages need to be saved in the medical record. Thisneeds to be done in accordance with the HealthInsurance Portability and Accountability Act guide-lines, and all patient identifiers need to be safe-guarded if the images are to be stored electronically.Documentation for procedural billing that utilizes
imaging techniques includes a formal report thatdescribes the sonographic findings in the procedurenote including location, adequate compressibility of the vessel, and the fact that the ultrasound was usedfor real-time guidance of the needle insertion.
Limitations to Ultrasonography
There are some realities one needs to face, how-ever, prior to embracing ultrasound for all IJ CVCs.First, there are no blinded randomized trials provingimproved outcome with infection (catheter-relatedblood stream infection), ICU/hospital length of stay,or mortality as end points. For the time being, wetherefore need to rely on the current evidenceshowing improvements in success and arterial injury.
Clearly, experienced physicians can perform IJCVC placement safely without ultrasound guidance.
At this time, each of the relevant risks and benefits of performing IJ CVC placement with or without ultra-sound guidance need to be assessed on a case by casebasis. Given the recommendations by Agency forHealthcare Research and Quality and National In-stitute of Clinical Excellence, ultrasound guidancefor IJ CVC placement will almost certainly becomestandard of care. We may soon find ourselves in theposition of needing to explain why an IJ CVC wasplaced without ultrasound guidance.
Secondly, there are numerous ultrasound ma-chines available, each with their own advantages anddisadvantages, and although “bells and whistles” may be nice to have, they are not required, and simple/ older machines can be adequate for most needs. Theinitial financial investment can be quite significant(approximately $25,000 to $40,000), although new and used equipment can even be found on Internetsites such as ebay.com for significantly less money.Additionally, maintenance costs and costs of addi-tional supplies such as sterile sheaths and a printerneed to be budgeted for. Unfortunately, the dataregarding cost/benefit analysis for ultrasound guid-
ance is extremely small. Calvert et al21,45
performeda decision analysis with estimations of net benefitsand costs. With relatively conservative assumptions,they found a significant cost savings associated withthe use of ultrasound of £2,000 for every 1,000patients treated. Clearly, this is a model, and realcost/benefit analyses are required that will includethe number of ultrasound machines per hospital orspecific unit. Thirdly, and perhaps most importantly,quality assurance for both the ultrasound unit as wellas the physicians performing and interpreting theultrasound needs to be high on all of our priorities.
www.chestjournal.org CHEST / 132 / 1 / JULY, 2007 307
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
7/8
Summary
Ultrasonography is an easily learned procedurethat not only enhances the physical examination buthas the distinct advantages of being a portable toolthat can provide real-time guidance for IJ CVCplacement with significant improvements in first-pass success, overall success, and arterial injury. As
chest physicians/intensivists, we need to embrace thebroad clinical applications of ultrasound, not only forIJ CVC placement, but in our patients with pleuraldisease, ascites, shock, and who have sustainedtrauma. It is crucial that we take the lead in advo-cating that ultrasound become part of our daily practice, create educational opportunities for mem-bers of our societies, and incorporate ultrasoundtraining in our fellowship programs.
References
1 McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med 2003; 348:1123–1133
2 Merrer J, De Jonghe B, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically illpatients: a randomized controlled trial. JAMA 2001; 286:700–707
3 Bernard RW, Stahl WM. Subclavian vein catheterizations: aprospective study: i. Non-infectious complications. Ann Surg1971; 173:184–190
4 Sznajder JI, Zveibil FR, Bitterman H, et al. Central veincatheterization: failure and complication rates by three per-cutaneous approaches. Arch Intern Med 1986; 146:259–261
5 Defalque RJ. Percutaneous catheterization of the internal jugular vein. Anesth Analg 1974; 53:116 –121
6 Goldfarb G, Lebrec D. Percutaneous cannulation of theinternal jugular vein in patients with coagulopathies: anexperience based on 1,000 attempts. Anesthesiology 1982;56:321–323
7 Mansfield PF, Hohn DC, Fornage BD, et al. Complicationsand failures of subclavian-vein catheterization. N Engl J Med1994; 331:1735–1738
8 Mallory DL, McGee WT, Shawker TH, et al. Ultrasoundguidance improves the success rate of internal jugular veincannulation: a prospective, randomized trial. Chest 1990;98:157–160
9 Troianos CA, Jobes DR, Ellison N. Ultrasound-guided can-nulation of the internal jugular vein: a prospective, random-ized study. Anesth Analg 1991; 72:823–826
10 Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted can-nulation of the internal jugular vein: a prospective comparisonto the external landmark-guided technique. Circulation 1993;87:1557–1562
11 Slama M, Novara A, Safavian A, et al. Improvement of internal jugular vein cannulation using an ultrasound-guidedtechnique. Intensive Care Med 1997; 23:916–919
12 Teichgraber UK, Benter T, Gebel M, et al. A sonographically guided technique for central venous access. AJR Am JRoentgenol 1997; 169:731–733
13 Nadig C, Leidig M, Schmiedeke T, et al. The use of ultrasound for the placement of dialysis catheters. NephrolDial Transplant 1998; 13:978–981
14 Hayashi H, Amano M. Does ultrasound imaging beforepuncture facilitate internal jugular vein cannulation? Prospec-
tive randomized comparison with landmark-guided puncturein ventilated patients. J Cardiothorac Vasc Anesth 2002;16:572–575
15 Leung J, Duffy M, Finckh A. Real-time ultrasonographically-guided internal jugular vein catheterization in the emergency department increases success rates and reduces complica-tions: a randomized, prospective study. Ann Emerg Med2006; 48:540–547
16 Karakitsos D, Labropoulos N, De Groot E, et al. Real-time
ultrasound guided catheterization of the internal jugular vein:a prospective comparison to the landmark technique incritical care patients. Crit Care 2006; 10:R162
17 Randolph AG, Cook DJ, Gonzales CA, et al. Ultrasoundguidance for placement of central venous catheters: a meta-analysis of the literature. Crit Care Med 1996; 24:2053–2058
18 Hind D, Calvert N, McWilliams R, et al. Ultrasonic locatingdevices for central venous cannulation: meta-analysis. BMJ2003; 327:361
19 Rothschild, J. M. Ultrasound guidance of central vein cathe-terization. 2001. Available at: http://www.ahrq.gov/clinic/ ptsafety/chap21.htm. Accessed June 4, 2007
20 Making health care safer: a critical analysis of patient safety practices. 2001. Available at: http://www.ahrq.gov/clinic/ ptsafety/. Accessed June 4, 2007
21 Calvert N, Hind D, McWilliams RG, et al. The effectivenessand cost-effectiveness of ultrasound locating devices forcentral venous access: a systematic review and economicevaluation. Health Technol Assess 2003; 7:1–84
22 Howard S. A survey measuring the impact of NICE guidance49: the use of ultrasound locating devices for placing central
venous catheters. 2004. Available at: http://www.nice.org.uk/pdf/ Final_CVC_placement_survey_report.pdf. Accessed June 4,2007
23 Girard TD, Schectman JM. Ultrasound guidance duringcentral venous catheterization: a survey of use by house staff physicians. J Crit Care 2005; 20:224–229
24 Legler D, Nugent M. Doppler localization of the internal jugular vein facilitates central venous cannulation. Anesthesi-
ology 1984; 60:481–48225 Gilbert TB, Seneff MG, Becker RB. Facilitation of internal
jugular venous cannulation using an audio-guided Dopplerultrasound vascular access device: results from a prospective,dual-center, randomized, crossover clinical study. Crit CareMed 1995; 23:60–65
26 Bold RJ, Winchester DJ, Madary AR et al. Prospective,randomized trial of Doppler-assisted subclavian vein cathe-terization. Arch Surg 1998; 133:1089–1093
27 Troianos CA, Kuwik RJ, Pasqual JR, et al. Internal jugular vein and carotid artery anatomic relation as determined by ultrasonography. Anesthesiology 1996; 85:43–48
28 Gordon AC, Saliken JC, Johns D, et al. US-guided punctureof the internal jugular vein: complications and anatomic
considerations. J Vasc Interv Radiol 1998; 9:333–33829 Parry G. Trendelenburg position, head elevation and a mid-line position optimize right internal jugular vein diameter.Can J Anaesth 2004; 51:379–381
30 Bazaral M, Harlan S. Ultrasonographic anatomy of the inter-nal jugular vein relevant to percutaneous cannulation. CritCare Med 1981; 9:307–310
31 Sulek CA, Gravenstein N, Blackshear RH, et al. Headrotation during internal jugular vein cannulation and the riskof carotid artery puncture. Anesth Analg 1996; 82:125–128
32 Lieberman JA, Williams KA, Rosenberg AL. Optimal headrotation for internal jugular vein cannulation when relying onexternal landmarks. Anesth Analg 2004; 99:982–988
33 O’Grady NP, Alexander M, Dellinger EP, et al. Guidelinesfor the prevention of intravascular catheter-related infections.
308 Topics in Practice Management
wnloaded From: http://journal.publications.chestnet.org/ on 03/31/2016
-
8/18/2019 Ultrasound-Guided Internal Jugular Access
8/8
Centers for Disease Control and Prevention. MMWR MorbMortal Wkly Rep 2002; 55:1–26
34 Milling TJ Jr, Rose J, Briggs WM, et al. Randomized,controlled clinical trial of point-of-care limited ultrasonogra-phy assistance of central venous cannulation: the ThirdSonography Outcomes Assessment Program (SOAP-3) trial.Crit Care Med 2005; 33:1764–1769
35 American College of Emergency Physicians. Emergency ul-trasound imaging criteria compendium. 2006. Available at:
http://www.acep.org/NR/rdonlyres/34C01AF7–713E-4789–9CB8–D2B330418E54/0/emergultraimgcriteria0406.pdf. Ac-cessed June 4, 2007
36 Augoustides JG, Horak J, Ochroch AE, et al. A randomizedcontrolled clinical trial of real-time needle-guided ultrasoundfor internal jugular venous cannulation in a large university anesthesia department. J Cardiothorac Vasc Anesth 2005;19:310–315
37 Maury E, Guglielminotti J, Alzieu M, et al. Ultrasonicexamination: an alternative to chest radiography after central
venous catheter insertion? Am J Respir Crit Care Med 2001;164:403–405
38 American Medical Association. Res. 802, I-99 and Reaffirmed:Sub.Res. 108, A-00; privileging for ultrasound imaging. 2005.Available at: http://www.ama-assn.org/apps/pf new/pf online?f
nbrowse&docpolicyfiles/HnE/H-230.960.HTM. AccessedMarch 15, 2006
39 American College of Emergency Physicians. AECP policy state-
ment: emergency ultrasound guidelines. 2001. Available at:http://www.acep.org/NR/rdonlyres/8024079E–28E8–4875-93E6– 6867EA705A2A/0/ultrasound_guidelines.pdf. AccessedJune 4, 2007
40 American College of Surgeons. Ultrasound examinations by surgeons. 1998. Available at: http://www.facs.org/fellows_info/ statements/st-31.html. Accessed June 4, 2007
41 Thomas B, Falcone RE, Vasquez D, et al. Ultrasound evalu-ation of blunt abdominal trauma: program implementation,
initial experience, and learning curve. J Trauma 1997; 42:384–388
42 Shackford SR, Rogers FB, Osler TM, et al. Focused abdom-inal sonogram for trauma: the learning curve of nonradiologistclinicians in detecting hemoperitoneum. J Trauma 1999;46:553–562
43 Board of the Faculty of Clinical Radiology, The Royal Collegeof Radiologists. Ultrasound training recommendations formedical and surgical specialties. 2004. Available at: http://
www.rcr.ac.uk/docs/radiology/pdf/ultrasound.pdf. AccessedJune 4, 2007
44 Ernst A, Silvestri GA, Johnstone D. Interventional pulmonary procedures: guidelines from the American College of ChestPhysicians. Chest 2003; 123:1693
45 Calvert N, Hind D, McWilliams R, et al. Ultrasound forcentral venous cannulation: economic evaluation of cost-effectiveness. Anaesthesia 2004; 59:1116–1120
www.chestjournal.org CHEST / 132 / 1 / JULY, 2007 309