
Ultrasound assisted thrombolysis for vte turkish experience
28
A. KURSAT BOZKURT, MD University of Istanbul Cerrahpasa Medical Faculty 2013 Ultrasound assisted thrombolysis for VTE: Turkish experience
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
132 -
download
0
Transcript of Ultrasound assisted thrombolysis for vte turkish experience

A. KURSAT BOZKURT, MD
University of Istanbul
Cerrahpasa Medical Faculty
2013
Ultrasound assisted
thrombolysis for VTE:
Turkish experience

Pulmonary embolism:
a silent killer
Cause of Death # of annual deaths2
PE Up to 200,0002,3
AIDS 18,017
Breast Cancer 40,870
• Most patients who die from PE are not diagnosed at premortem, and are not even suspected premortem
Study AutopsiesPE
present
PE suspected
premortem
Rubenstein et al4 1.276 44 14 (32%)
Stein and Henry5 404 59 6 (30%)
Lau6 11,044 116 27 (23%)
Pulido et al7 1.032 231 42 (18%)
1. Dalen et al. Prog Cardiovasc Dis. 1975;17:259-70.
2. Wood. Chest 2002;121;877-905.
3. Silverstein et al. Arch intern Med 1998;158:585-93.
4. Rubenstein et al. Arch Intern Med. 1988 Jun;148(6):1425-6.
5. Stein and Henry. Chest 1995 Oct;108(4):978-81
6. Lau. Ann Acad Med Singapore. 1995 May;24(3):356-65.
7. Pulido et al. Chest. 2006 May;129(5):1282-7

Risk stratificationPatient risk stratification (per AHA 2011 guidelines)
Massive PE Submassive PE Minor/Nonmassive PE
High risk Moderate risk Low risk
•Sustained hypotension (systolic BP <90
mmHg for 15 min)
•Inotropic support
•Pulselessness
•Persistent profound bradycardia (HR <40
bpm with signs or symptoms of shock)
•Systemically normotensive
(systolic BP 90 mmHg)
•RV dysfunction
•Myocardial necrosis
•Systemically normotensive
(systolic BP 90 mmHg)
•No RV dysfunction
•No myocardial necrosis
RV dysfunction• RV/LV ratio > 0.9 or RV systolic dysfunction on echo
• RV/LV ratio > 0.9 on CT
• Elevation of BNP (>90 pg/mL)
• Elevation of NTpro-BNP (>500 pg/mL)
• ECG changes
• new complete or incomplete RBBB
• anteroseptal ST elevation or depression
• anteroseptal T-wave inversion
Jaff et al. Circulation 2011;123(16):1788-1830.

Why treat submassive PE
aggressively?RV/LV ratio > 0.9 is an independent predictor of mortality1-4
Patients with persistent RV dysfunction at discharge:
• 8 times more likely to have recurrent PE• 4 times higher mortality rate
than patients with RV dysfunction regressed at discharge5
1-year follow-up, 44% of PE patients with RV dysfunction at hospital discharge will have chronic pulmonary hypertension6
1. Quiroz, Circ 2004; 109:2401-24042. Frémont, Chest 2008; 133;558-362
3. Schoef, Circ 2004; 110:3276-3280
4. Kucher, Arch Intern Med 2005; 165:1777-1781
5. Grifoni, Arch Intern Med 2006; 166:2151-215
6. Ribeiro, Circ 1999;99:1352-1330

ULTIMA Trial
A Prospective, Randomized, Controlled study of
ULTrasound Accelerated ThrombolysIs for the
Treatment of Acute PulMonAry Embolism
- Acute Symptomatic PE confirmed w/ CTA chest
- RV/LV ratio > 1 on echo

1.28
0.99 0.95
0.5
1.0
1.5
Baseline 24 hrs 90 days
RV
/LV
Rat
io
EKOS®+Heparin
1.20 1.17
0.98
Baseline 24 hrs 90 days
Heparin
P<0.0001
P<0.0001
P=0.31
P<0.0001
RV/LV ratio (echo)
Kucher 2013

0.300.38
0.0
0.2
0.4
0.6
Baselineto 24 hrs
Baselineto 90 days
Re
du
ctio
n in
RV
/LV
Rat
io
EKOS®+Heparin
0.030.22
Baselineto 24 hrs
Baselineto 90 days
Heparin
P<0.0001
P=0.03
Primary endpoint: Reduction in RV/LV ratio (echo)
Kucher 2013

Conclusions
In PE pts at intermediate risk of death, low-dose catheter-
directed ultrasound-accelerated thrombolysis (< 20 mg rt-
PA/15 hrs) was superior to anticoagulation with heparin alone
in reversing RV dilatation & dysfunction @ 24 hrs, w/o an
increase in bleeding complications
Although there was a late “catch-up” w/heparin alone, there
was greater improvement
SEATTLE II Study
Submassive and massive pulmonary Embolism
treatment with AcceleraTed ThromboLysis thErapy
STUDY CHAIR: Sam Z. Goldhaber, MD
Women And Brigham’s Hospital, Boston, MA
PURPOSE
Determine if the EKOS EkoSonic® Endovascular Device when
used in conjunction with recombinant t-PA as a treatment for
acute pulmonary embolism (PE) will decrease the ratio of RV
to LV diameter
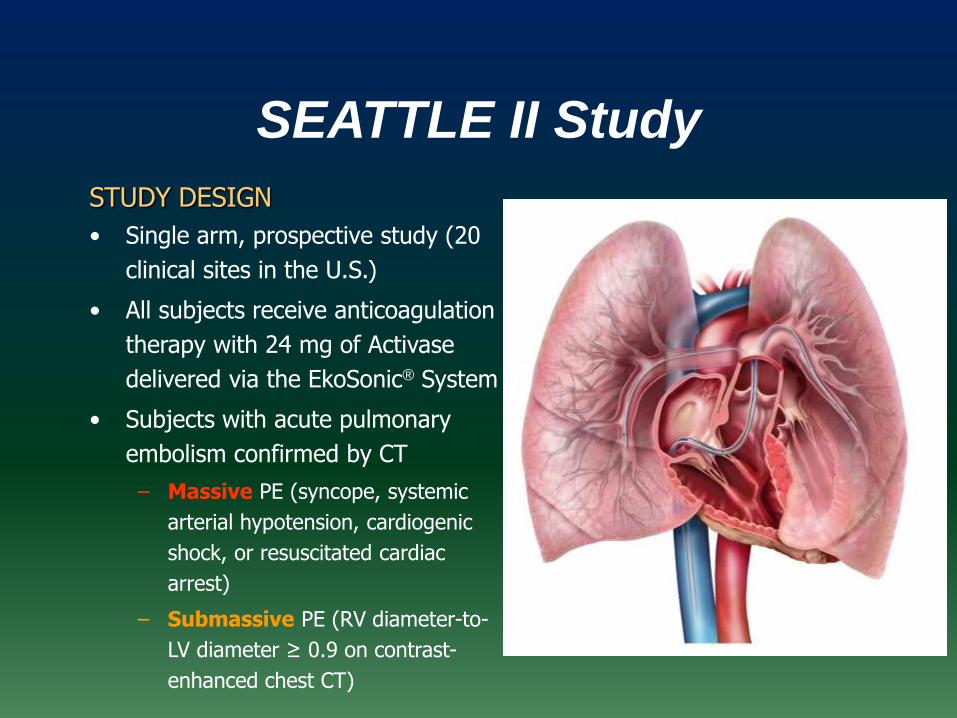
SEATTLE II Study
STUDY DESIGN
• Single arm, prospective study (20
clinical sites in the U.S.)
• All subjects receive anticoagulation
therapy with 24 mg of Activase
delivered via the EkoSonic® System
• Subjects with acute pulmonary
embolism confirmed by CT
– Massive PE (syncope, systemic
arterial hypotension, cardiogenic
shock, or resuscitated cardiac
arrest)
– Submassive PE (RV diameter-to-
LV diameter ≥ 0.9 on contrast-
enhanced chest CT)

EFFICACY
decrease the ratio of RV to LV diameter within 48 ± 6 hours in
patients with massive or submassive PE
SAFETY
Frequency of major bleeding within 72 hours of initiation of
therapy
SEATTLE II Study
EKOS®
?

0
20
40
60
80
100
120
140
Rapid enrollmentPlanned:
150 patients to
enroll in 18 mo.
Actual:
150 patients
enrolled in 9 mo.

DVT
Deep venous thrombosis (DVT) - 500,000-600,000 new cases in US annually1
- 40-60% of pts on anticoagulation will develop PTS
after 1st episode of DVT2
Post thrombotic syndrome (PTS)- clinical complication of DVT can be lifestyle limiting
and debilitating
- Sx: pain, edema, varicosities, skin discoloration,
thickening & ulceration
- 500,000-600,000 venous ulcers yearly3
- Nearly 90% of patients are unable to work due to leg
symptoms 10 years after iliofemoral DVT4
- Suspect MILLIONS suffer from PTS
Estimated socioeconomic burden of $ 3 billion
annually4References
1. US surgeon general’s office; 2008. 2. Kahn SR, Shrier I, Julian JA, et al. Ann Intern Med 2008;149:698–707. 3. Pacific Vascular
Symposium 6. Kona, Hawaii, 2009. 4. Kahn SR, Ginsberg JS. Arch Intern Med 2004; 164:17–265. Lazarusetal. Arch Dermotolgy
1994; 130:489-93.
Single-center experience
Retrospective, single center case reviews 106 patients and 122 limbs treated
- 66 M, 40 F- Mean age 57; range 13-96 years old- 17 upper and 105 lower extremities - IVC involvement in 25 (24%)
Documented DVT by USAll patients had symptoms > 1mo DVT defined as chronic by age of sx onset > 1moAll with varying degrees of PTS symptoms:
- Pain & swelling ulcer & gangrene ( > CEAP 3, Villalta > 10)- All c/o QOL & lifestyle limitations
Garcia et al. SIR 2012 Presentation & Press Release

Methods
Case review data was collected including:
- DVT history
- Procedural information
- Immediate technical outcomes
- Symptomatic improvement
- Ultrasound follow-up at 1,3,6, and 12 months, and yearly thereafter
Minimally Invasive endovascular techniques included:
- Initial PTA- ultrasound accelerated thrombolysis (EKOS)- PCBs- Adjunctive therapies (stenting, PMT)- Anticoagulation- ECS
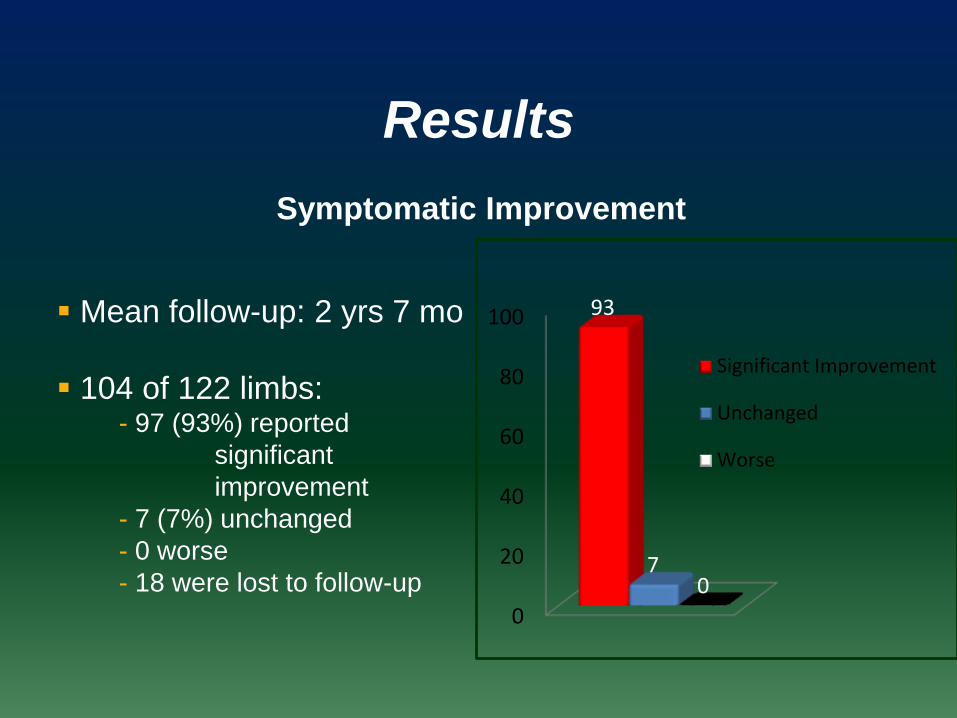
Results
Symptomatic Improvement
Mean follow-up: 2 yrs 7 mo
104 of 122 limbs:- 97 (93%) reported
significant
improvement
- 7 (7%) unchanged
- 0 worse
- 18 were lost to follow-up
0
20
40
60
80
100 93
70
Significant Improvement
Unchanged
Worse
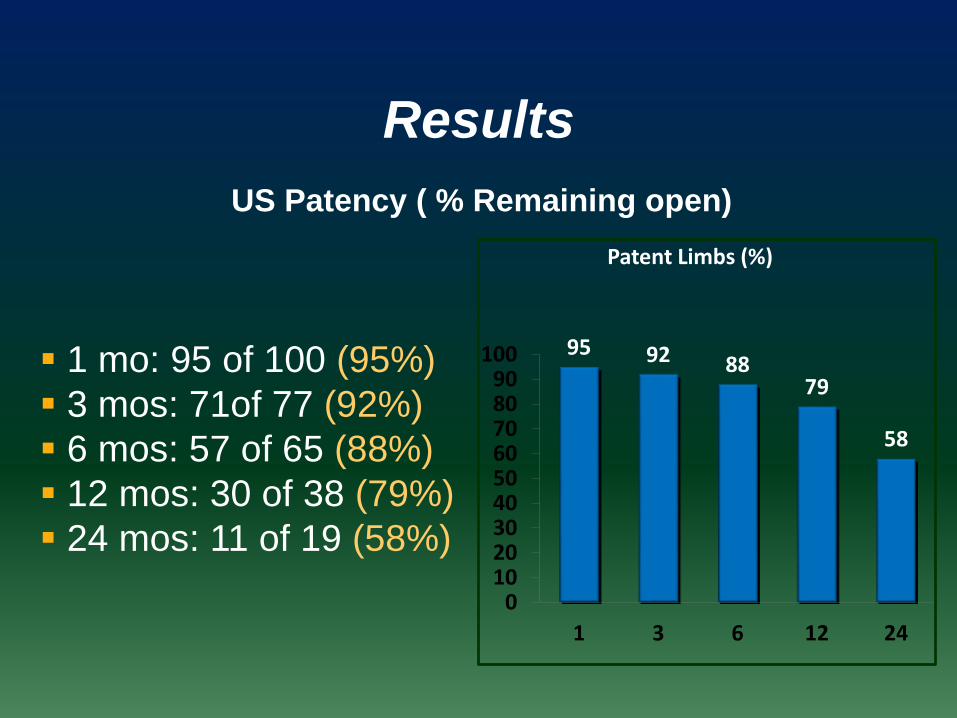
Results
US Patency ( % Remaining open)
1 mo: 95 of 100 (95%)
3 mos: 71of 77 (92%)
6 mos: 57 of 65 (88%)
12 mos: 30 of 38 (79%)
24 mos: 11 of 19 (58%)
95 92 8879
58
0102030405060708090
100
1 3 6 12 24
Patent Limbs (%)
The Key is Removing the Clot
There are two challenges
1. Transport the drug TO the clot (Delivery Catheter)
2. Further transport the drug INTO the Clot(Ultrasound Core)

Time 0
Wait 30 Minutes…
+ Lytic Lytic
+ Ultrasound
In Vitro Thrombus Model(Human Platelet-Poor Plasma Clots)
Control
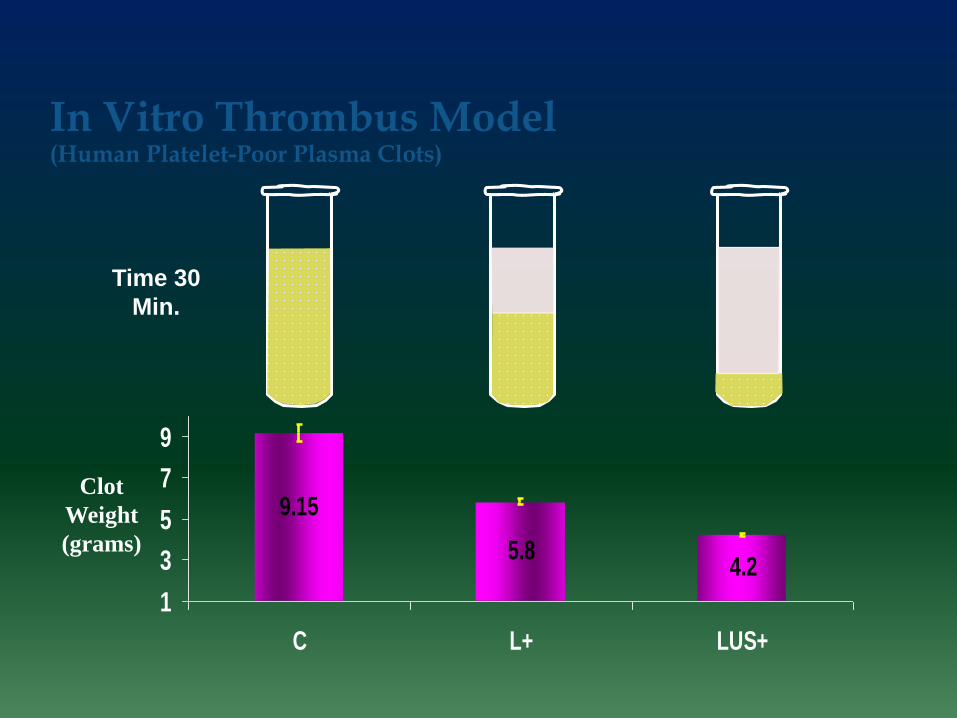
9.15
5.84.2
1
3
5
7
9
C L+ LUS+
Time 30
Min.
In Vitro Thrombus Model(Human Platelet-Poor Plasma Clots)
Clot
Weight
(grams)

Ultrasound enhances lytic agents
equally
0
20
40
60
80
100
UK rtPA reteplase
25 0.002 0.0009
Drug Type and Conc. in [mg/ml plasma]
Lysis
En
ha
nce
me
nt F
acto
r
[%]

1. Clot is made up of tight fibrin strands.• The strands protect the clot
2. Plasminogen is present in the clot• When Activated: Plasminogen converts to Plasmin
• Plasmin eats fibrin
3. tPA activates plasminogen• Creating more plasmin to digest fibrin
4. The speed of lysis depends on ability of lytic to access plasminogen receptors sites.*
What we know about the Clot?
* Francis, Charles W. et al. “Ultrasound Accelerates Transport of Recombinant Tissue Plasminogen Activator into Clots.”
Ultrasound in Medicine and Biology 21.3 (1995):419-424.
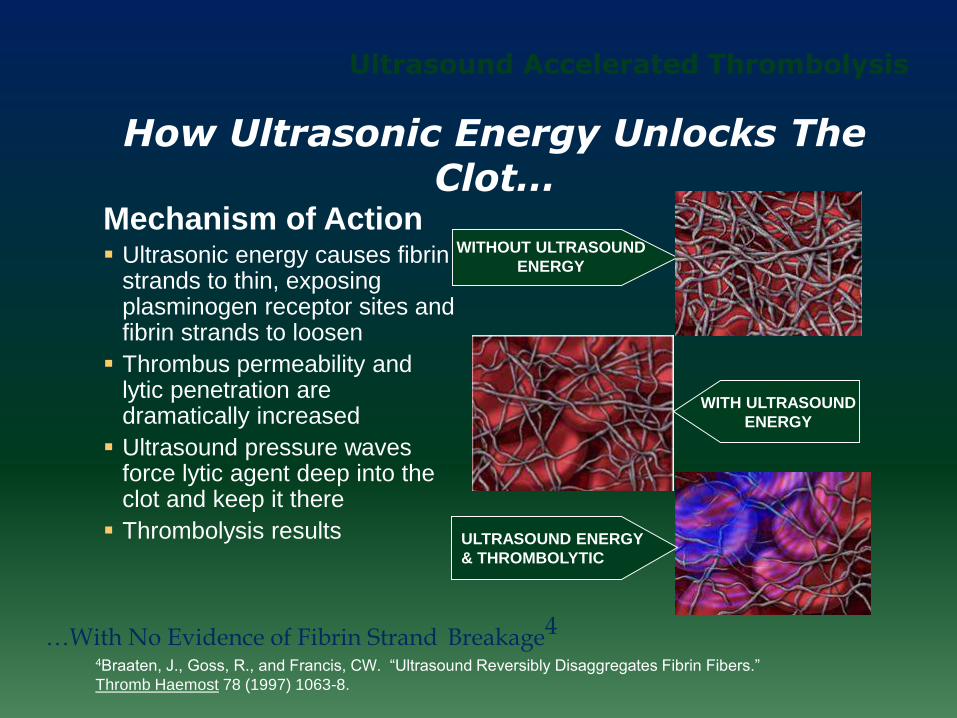
WITH ULTRASOUND
ENERGY
WITHOUT ULTRASOUND
ENERGY
How Ultrasonic Energy Unlocks The Clot…
Mechanism of Action Ultrasonic energy causes fibrin
strands to thin, exposing plasminogen receptor sites and fibrin strands to loosen
Thrombus permeability and lytic penetration are dramatically increased
Ultrasound pressure waves force lytic agent deep into the clot and keep it there
Thrombolysis results
…With No Evidence of Fibrin Strand Breakage4
ULTRASOUND ENERGY
& THROMBOLYTIC
Ultrasound Accelerated Thrombolysis
4Braaten, J., Goss, R., and Francis, CW. “Ultrasound Reversibly Disaggregates Fibrin Fibers.”
Thromb Haemost 78 (1997) 1063-8.
µSonic pressure waves
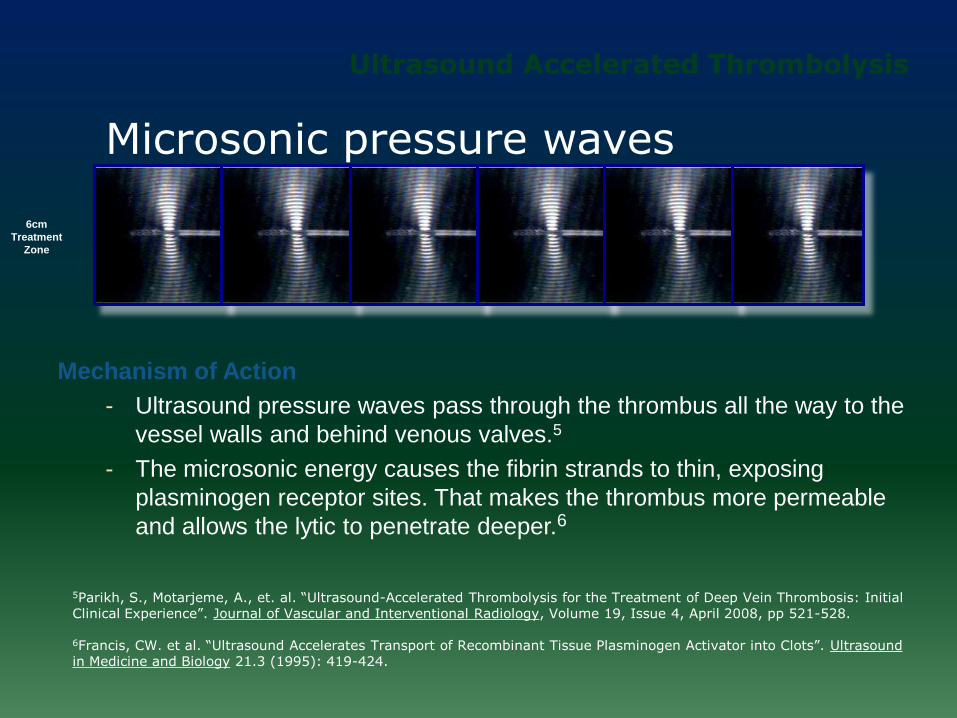
Mechanism of Action
- Ultrasound pressure waves pass through the thrombus all the way to the
vessel walls and behind venous valves.5
- The microsonic energy causes the fibrin strands to thin, exposing
plasminogen receptor sites. That makes the thrombus more permeable
and allows the lytic to penetrate deeper.6
5Parikh, S., Motarjeme, A., et. al. “Ultrasound-Accelerated Thrombolysis for the Treatment of Deep Vein Thrombosis: Initial Clinical Experience”. Journal of Vascular and Interventional Radiology, Volume 19, Issue 4, April 2008, pp 521-528.
6Francis, CW. et al. “Ultrasound Accelerates Transport of Recombinant Tissue Plasminogen Activator into Clots”. Ultrasound in Medicine and Biology 21.3 (1995): 419-424.
Microsonic pressure waves
Ultrasound Accelerated Thrombolysis
6cm
Treatment
Zone
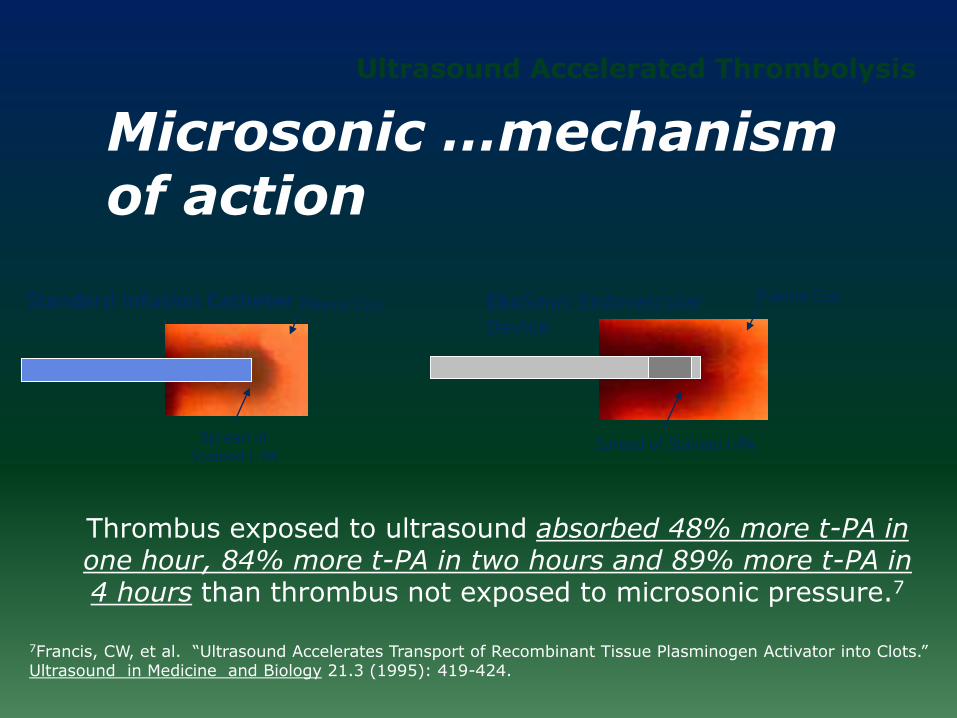
Microsonic …mechanism of action
Standard Infusion Catheter
Spread of
Stained t-PA
Plasma ClotPlasma Clot
Spread of Stained t-PA
EkoSonic Endovascular
Device
Thrombus exposed to ultrasound absorbed 48% more t-PA in one hour, 84% more t-PA in two hours and 89% more t-PA in 4 hours than thrombus not exposed to microsonic pressure.7
Ultrasound Accelerated Thrombolysis
7Francis, CW, et al. “Ultrasound Accelerates Transport of Recombinant Tissue Plasminogen Activator into Clots.” Ultrasound in Medicine and Biology 21.3 (1995): 419-424.
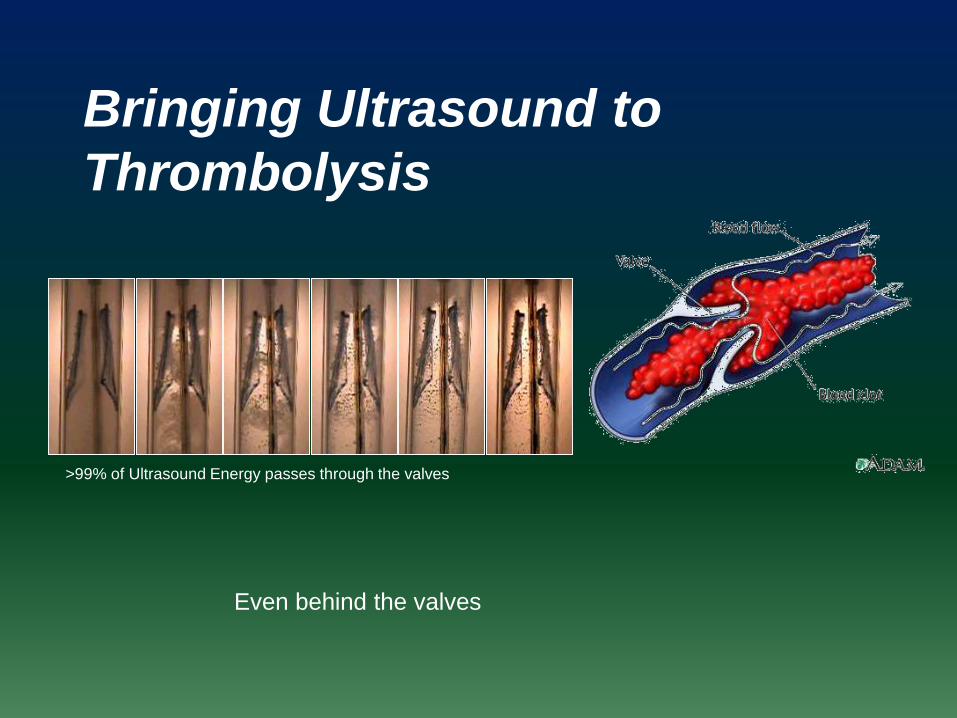
>99% of Ultrasound Energy passes through the valves
Bringing Ultrasound to
Thrombolysis
Even behind the valves

Turkish Experience
August 2010 – October 2013
284 PE
761 DVT
No reliable follow-up
11.7% stenting
Reported major complications
- 1 dead during PE treatment
- 2 major bleeding

THANKS















![diagnosis and management of VTE.ppt [Read-Only]€¦ · Diagnosis and Management of VTE Disclosures I have nothing to disclose. 2 TOPICS ... Date of download: 8/12/2014 Thrombolysis](https://static.fdocuments.in/doc/165x107/5ac464297f8b9a333d8d432e/diagnosis-and-management-of-vteppt-read-only-diagnosis-and-management-of-vte.jpg)
