Ultrasonography Evaluation of Scrotal Masses - palmino.orgpalmino.org/files/libri/sommers2014...
17
Ultrasonography Evaluation of Scrotal Masses Daniel Sommers, MD*, Thomas Winter, MD INTRODUCTION This article reviews the anatomy and sonographic findings of scrotal masses. Normal anatomy, gen- eral imaging techniques, and assessment of intra- testicular and extratesticular disorders will be discussed. When a scrotal mass is palpated, the concern is for the presence of a testicular neoplasm. Ultraso- nography (US) is an ideal modality for evaluating the scrotum in this scenario; it is readily available, inexpensive, and without ionizing radiation. US is nearly 100% sensitive for the detection of an intra- scrotal mass. 1 Delineation between intratesticular and extratesticular processes is 98% to 100% accurate. 1–4 NORMAL ANATOMY The normal scrotal wall consists of epidermis, su- perficial dartos muscle and fascia, external sper- matic fascia, cremasteric muscle and fascia, and internal spermatic fascia. The scrotum is a fibro- muscular sac divided by a midline septum into a right and left hemiscrotum. Each hemiscrotum contains a testis, epididymis, spermatic cord, vascular network, and lymphatic network. Separating the testis from the scrotal wall are the 2 layers of the tunica vaginalis; these form an isolated mesothelium-lined sac. 5,6 The parietal layer lines the scrotal wall and is separated from the visceral layer lining the tunica albuginea of the testis and covering the epididymis by a poten- tial space that normally contains a small amount of fluid. The parietal and visceral layers of the tunica vaginalis join where the tunica attaches to the scrotal wall at the posterolateral aspect of the testis. The tunica albuginea covers the testis and epididymis with the exception of a small postero- medial area. 7 The fibrous tunica albuginea covers the testis, protecting it from injury. Posteromedially, the tunica albuginea projects inward into the testes to form the mediastinum testis. Numerous fibrous septa extend from the mediastinum dividing the testis into 250 to 400 lobules. Each lobule consists of 1 to 3 seminiferous tubules that support the Ser- toli cells and spermatocytes. The Leydig cells are adjacent to the tubules within the loose interstitial tissue and are responsible for testosterone secretion. The seminiferous tubules converge to form larger tubuli recti, which open into the dilated Disclosures: None. Department of Radiology, University of Utah School of Medicine, 50 North Medical Drive #1A071, Salt Lake City, UT 84132, USA * Corresponding author. E-mail address: [email protected] KEYWORDS Scrotal ultrasonography Intratesticular scrotal mass Extratesticular scrotal mass KEY POINTS Ultrasonography is the ideal modality for evaluating the scrotum. Normal scrotal anatomy and the sonographic assessment of intratesticular and extratesticular causes that may present as scrotal masses are discussed. Radiol Clin N Am 52 (2014) 1265–1281 http://dx.doi.org/10.1016/j.rcl.2014.07.014 0033-8389/14/$ – see front matter Ó 2014 Elsevier Inc. All rights reserved. radiologic.theclinics.com
Transcript of Ultrasonography Evaluation of Scrotal Masses - palmino.orgpalmino.org/files/libri/sommers2014...

UltrasonographyEvaluation of Scrotal
Masses Daniel Sommers, MD*, Thomas Winter, MDKEYWORDS
� Scrotal ultrasonography � Intratesticular scrotal mass � Extratesticular scrotal mass
KEY POINTS
� Ultrasonography is the ideal modality for evaluating the scrotum.
� Normal scrotal anatomy and the sonographic assessment of intratesticular and extratesticularcauses that may present as scrotal masses are discussed.
INTRODUCTION
This article reviews the anatomy and sonographicfindings of scrotal masses. Normal anatomy, gen-eral imaging techniques, and assessment of intra-testicular and extratesticular disorders will bediscussed.
When a scrotal mass is palpated, the concern isfor the presence of a testicular neoplasm. Ultraso-nography (US) is an ideal modality for evaluatingthe scrotum in this scenario; it is readily available,inexpensive, and without ionizing radiation. US isnearly 100% sensitive for the detection of an intra-scrotal mass.1 Delineation between intratesticularand extratesticular processes is 98% to 100%accurate.1–4
NORMAL ANATOMY
The normal scrotal wall consists of epidermis, su-perficial dartos muscle and fascia, external sper-matic fascia, cremasteric muscle and fascia, andinternal spermatic fascia. The scrotum is a fibro-muscular sac divided by a midline septum into aright and left hemiscrotum. Each hemiscrotumcontains a testis, epididymis, spermatic cord,vascular network, and lymphatic network.
Disclosures: None.Department of Radiology, University of Utah School ofCity, UT 84132, USA* Corresponding author.E-mail address: [email protected]
Radiol Clin N Am 52 (2014) 1265–1281http://dx.doi.org/10.1016/j.rcl.2014.07.0140033-8389/14/$ – see front matter � 2014 Elsevier Inc. All
Separating the testis from the scrotal wall arethe 2 layers of the tunica vaginalis; these form anisolated mesothelium-lined sac.5,6 The parietallayer lines the scrotal wall and is separated fromthe visceral layer lining the tunica albuginea ofthe testis and covering the epididymis by a poten-tial space that normally contains a small amount offluid. The parietal and visceral layers of the tunicavaginalis join where the tunica attaches to thescrotal wall at the posterolateral aspect of thetestis. The tunica albuginea covers the testis andepididymis with the exception of a small postero-medial area.7
The fibrous tunica albuginea covers the testis,protecting it from injury. Posteromedially, thetunica albuginea projects inward into the testesto form the mediastinum testis. Numerous fibroussepta extend from the mediastinum dividing thetestis into 250 to 400 lobules. Each lobule consistsof 1 to 3 seminiferous tubules that support the Ser-toli cells and spermatocytes. The Leydig cells areadjacent to the tubules within the loose interstitialtissue and are responsible for testosteronesecretion.
The seminiferous tubules converge to formlarger tubuli recti, which open into the dilated
Medicine, 50 North Medical Drive #1A071, Salt Lake
rights reserved. radiologic.th
eclinics.com
Sommers & Winter1266
spaces of the rete testis. The rete testis drains intothe epididymal head (globus major) via 15 to 20efferent ductules. The pyramid-shaped head ofthe epididymis is located at the superoposterioraspect of the testis and measures 5 to 12 mm indiameter. The narrow epididymal body (corpus)and tail (globus minor) are formed as the efferentducts converge into a single duct. The curved tailof the epididymis courses inferolaterally and be-comes the vas deferens, which continues superi-orly into the spermatic cord.The appendix testes and appendix epididymis
are embryologic remnants of paramesonephricand mesonephric ducts, respectively, and consistof vascularized connective tissue.Primary vascular supply to the testis is provided
by the testicular artery, which arises from theaorta, just distal to the renal arteries. The testicularartery penetrates the tunica albuginea where itforms the capsular artery. The deferential artery,originating from the superior vesical artery, andthe cremasteric artery, a branch of the inferiorepigastric artery, both supply the epididymis, vasdeferens, and peritesticular tissues.7 Branches ofthe pudendal artery supply the wall of thescrotum. Venous drainage forms the pampiniformplexus around the upper half of the epididymis,which continues as the testicular vein throughthe deep inguinal ring. The spermatic cord con-tains the pampiniform plexus; vas deferens; testic-ular, cremasteric, and deferential arteries;genitofemoral nerve; and lymphatic vessels; andcourses superior toward the superficial and deepinguinal rings.
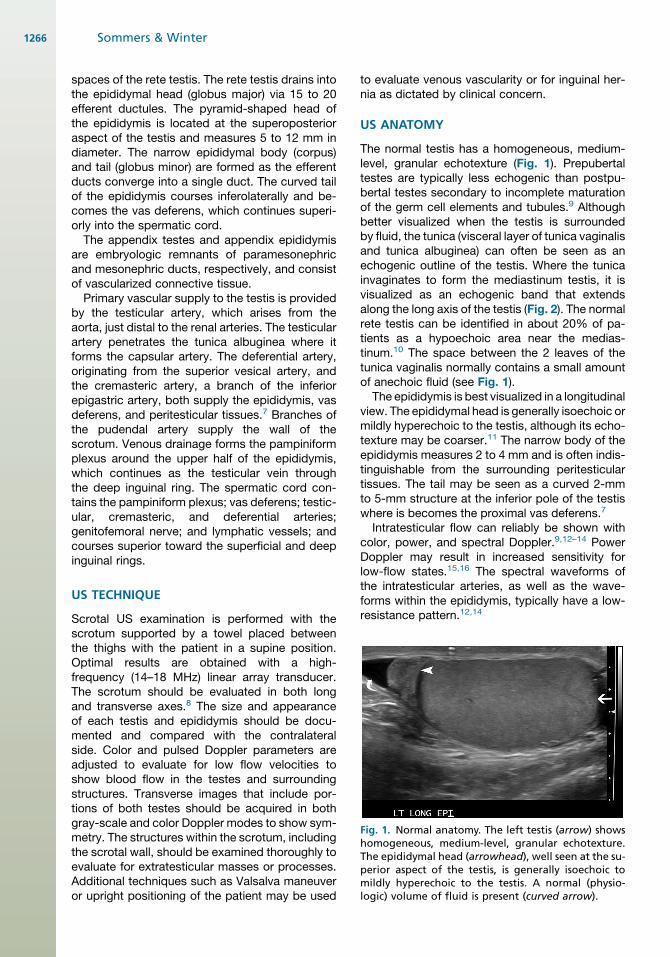
Fig. 1. Normal anatomy. The left testis (arrow) showshomogeneous, medium-level, granular echotexture.The epididymal head (arrowhead), well seen at the su-perior aspect of the testis, is generally isoechoic tomildly hyperechoic to the testis. A normal (physio-logic) volume of fluid is present (curved arrow).
US TECHNIQUE
Scrotal US examination is performed with thescrotum supported by a towel placed betweenthe thighs with the patient in a supine position.Optimal results are obtained with a high-frequency (14–18 MHz) linear array transducer.The scrotum should be evaluated in both longand transverse axes.8 The size and appearanceof each testis and epididymis should be docu-mented and compared with the contralateralside. Color and pulsed Doppler parameters areadjusted to evaluate for low flow velocities toshow blood flow in the testes and surroundingstructures. Transverse images that include por-tions of both testes should be acquired in bothgray-scale and color Doppler modes to show sym-metry. The structures within the scrotum, includingthe scrotal wall, should be examined thoroughly toevaluate for extratesticular masses or processes.Additional techniques such as Valsalva maneuveror upright positioning of the patient may be used
to evaluate venous vascularity or for inguinal her-nia as dictated by clinical concern.
US ANATOMY
The normal testis has a homogeneous, medium-level, granular echotexture (Fig. 1). Prepubertaltestes are typically less echogenic than postpu-bertal testes secondary to incomplete maturationof the germ cell elements and tubules.9 Althoughbetter visualized when the testis is surroundedby fluid, the tunica (visceral layer of tunica vaginalisand tunica albuginea) can often be seen as anechogenic outline of the testis. Where the tunicainvaginates to form the mediastinum testis, it isvisualized as an echogenic band that extendsalong the long axis of the testis (Fig. 2). The normalrete testis can be identified in about 20% of pa-tients as a hypoechoic area near the medias-tinum.10 The space between the 2 leaves of thetunica vaginalis normally contains a small amountof anechoic fluid (see Fig. 1).The epididymis is best visualized in a longitudinal
view. The epididymal head is generally isoechoic ormildly hyperechoic to the testis, although its echo-texture may be coarser.11 The narrow body of theepididymis measures 2 to 4 mm and is often indis-tinguishable from the surrounding peritesticulartissues. The tail may be seen as a curved 2-mmto 5-mm structure at the inferior pole of the testiswhere is becomes the proximal vas deferens.7
Intratesticular flow can reliably be shown withcolor, power, and spectral Doppler.9,12–14 PowerDoppler may result in increased sensitivity forlow-flow states.15,16 The spectral waveforms ofthe intratesticular arteries, as well as the wave-forms within the epididymis, typically have a low-resistance pattern.12,14
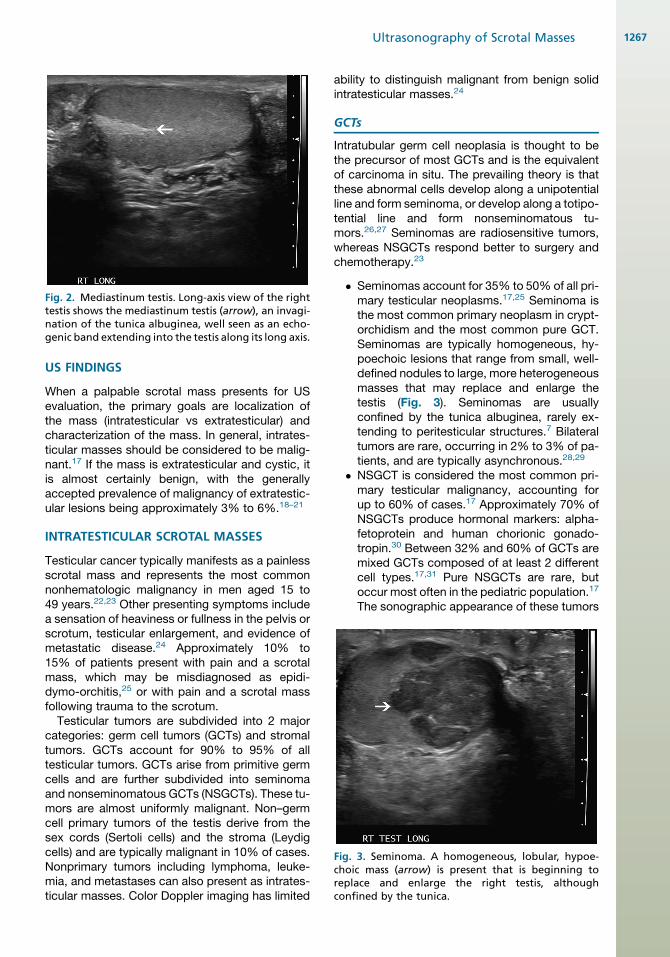
Fig. 2. Mediastinum testis. Long-axis view of the righttestis shows the mediastinum testis (arrow), an invagi-nation of the tunica albuginea, well seen as an echo-genic band extending into the testis along its long axis.
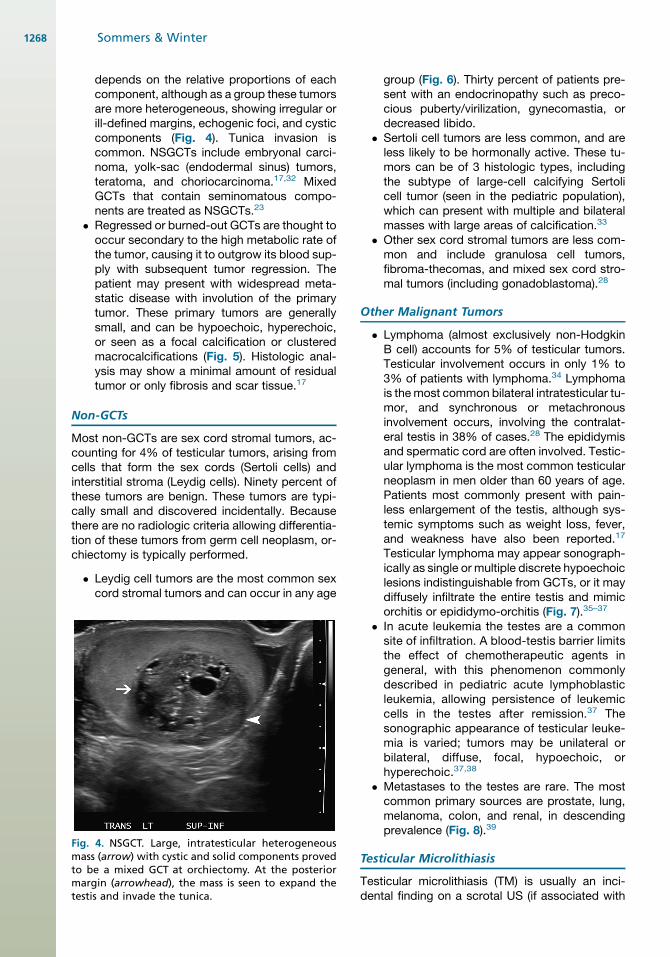
Fig. 3. Seminoma. A homogeneous, lobular, hypoe-choic mass (arrow) is present that is beginning toreplace and enlarge the right testis, althoughconfined by the tunica.
Ultrasonography of Scrotal Masses 1267
US FINDINGS
When a palpable scrotal mass presents for USevaluation, the primary goals are localization ofthe mass (intratesticular vs extratesticular) andcharacterization of the mass. In general, intrates-ticular masses should be considered to be malig-nant.17 If the mass is extratesticular and cystic, itis almost certainly benign, with the generallyaccepted prevalence of malignancy of extratestic-ular lesions being approximately 3% to 6%.18–21
INTRATESTICULAR SCROTAL MASSES
Testicular cancer typically manifests as a painlessscrotal mass and represents the most commonnonhematologic malignancy in men aged 15 to49 years.22,23 Other presenting symptoms includea sensation of heaviness or fullness in the pelvis orscrotum, testicular enlargement, and evidence ofmetastatic disease.24 Approximately 10% to15% of patients present with pain and a scrotalmass, which may be misdiagnosed as epidi-dymo-orchitis,25 or with pain and a scrotal massfollowing trauma to the scrotum.
Testicular tumors are subdivided into 2 majorcategories: germ cell tumors (GCTs) and stromaltumors. GCTs account for 90% to 95% of alltesticular tumors. GCTs arise from primitive germcells and are further subdivided into seminomaand nonseminomatous GCTs (NSGCTs). These tu-mors are almost uniformly malignant. Non–germcell primary tumors of the testis derive from thesex cords (Sertoli cells) and the stroma (Leydigcells) and are typically malignant in 10% of cases.Nonprimary tumors including lymphoma, leuke-mia, and metastases can also present as intrates-ticular masses. Color Doppler imaging has limited
ability to distinguish malignant from benign solidintratesticular masses.24
GCTs
Intratubular germ cell neoplasia is thought to bethe precursor of most GCTs and is the equivalentof carcinoma in situ. The prevailing theory is thatthese abnormal cells develop along a unipotentialline and form seminoma, or develop along a totipo-tential line and form nonseminomatous tu-mors.26,27 Seminomas are radiosensitive tumors,whereas NSGCTs respond better to surgery andchemotherapy.23
� Seminomas account for 35% to 50% of all pri-mary testicular neoplasms.17,25 Seminoma isthe most common primary neoplasm in crypt-orchidism and the most common pure GCT.Seminomas are typically homogeneous, hy-poechoic lesions that range from small, well-defined nodules to large, more heterogeneousmasses that may replace and enlarge thetestis (Fig. 3). Seminomas are usuallyconfined by the tunica albuginea, rarely ex-tending to peritesticular structures.7 Bilateraltumors are rare, occurring in 2% to 3% of pa-tients, and are typically asynchronous.28,29
� NSGCT is considered the most common pri-mary testicular malignancy, accounting forup to 60% of cases.17 Approximately 70% ofNSGCTs produce hormonal markers: alpha-fetoprotein and human chorionic gonado-tropin.30 Between 32% and 60% of GCTs aremixed GCTs composed of at least 2 differentcell types.17,31 Pure NSGCTs are rare, butoccur most often in the pediatric population.17
The sonographic appearance of these tumors
Sommers & Winter1268
depends on the relative proportions of eachcomponent, although as a group these tumorsare more heterogeneous, showing irregular orill-defined margins, echogenic foci, and cysticcomponents (Fig. 4). Tunica invasion iscommon. NSGCTs include embryonal carci-noma, yolk-sac (endodermal sinus) tumors,teratoma, and choriocarcinoma.17,32 MixedGCTs that contain seminomatous compo-nents are treated as NSGCTs.23
� Regressed or burned-out GCTs are thought tooccur secondary to the high metabolic rate ofthe tumor, causing it to outgrow its blood sup-ply with subsequent tumor regression. Thepatient may present with widespread meta-static disease with involution of the primarytumor. These primary tumors are generallysmall, and can be hypoechoic, hyperechoic,or seen as a focal calcification or clusteredmacrocalcifications (Fig. 5). Histologic anal-ysis may show a minimal amount of residualtumor or only fibrosis and scar tissue.17
Non-GCTs
Most non-GCTs are sex cord stromal tumors, ac-counting for 4% of testicular tumors, arising fromcells that form the sex cords (Sertoli cells) andinterstitial stroma (Leydig cells). Ninety percent ofthese tumors are benign. These tumors are typi-cally small and discovered incidentally. Becausethere are no radiologic criteria allowing differentia-tion of these tumors from germ cell neoplasm, or-chiectomy is typically performed.
� Leydig cell tumors are the most common sexcord stromal tumors and can occur in any age
Fig. 4. NSGCT. Large, intratesticular heterogeneousmass (arrow) with cystic and solid components provedto be a mixed GCT at orchiectomy. At the posteriormargin (arrowhead), the mass is seen to expand thetestis and invade the tunica.
group (Fig. 6). Thirty percent of patients pre-sent with an endocrinopathy such as preco-cious puberty/virilization, gynecomastia, ordecreased libido.
� Sertoli cell tumors are less common, and areless likely to be hormonally active. These tu-mors can be of 3 histologic types, includingthe subtype of large-cell calcifying Sertolicell tumor (seen in the pediatric population),which can present with multiple and bilateralmasses with large areas of calcification.33
� Other sex cord stromal tumors are less com-mon and include granulosa cell tumors,fibroma-thecomas, and mixed sex cord stro-mal tumors (including gonadoblastoma).28
Other Malignant Tumors
� Lymphoma (almost exclusively non-HodgkinB cell) accounts for 5% of testicular tumors.Testicular involvement occurs in only 1% to3% of patients with lymphoma.34 Lymphomais themost common bilateral intratesticular tu-mor, and synchronous or metachronousinvolvement occurs, involving the contralat-eral testis in 38% of cases.28 The epididymisand spermatic cord are often involved. Testic-ular lymphoma is the most common testicularneoplasm in men older than 60 years of age.Patients most commonly present with pain-less enlargement of the testis, although sys-temic symptoms such as weight loss, fever,and weakness have also been reported.17
Testicular lymphoma may appear sonograph-ically as single or multiple discrete hypoechoiclesions indistinguishable from GCTs, or it maydiffusely infiltrate the entire testis and mimicorchitis or epididymo-orchitis (Fig. 7).35–37
� In acute leukemia the testes are a commonsite of infiltration. A blood-testis barrier limitsthe effect of chemotherapeutic agents ingeneral, with this phenomenon commonlydescribed in pediatric acute lymphoblasticleukemia, allowing persistence of leukemiccells in the testes after remission.37 Thesonographic appearance of testicular leuke-mia is varied; tumors may be unilateral orbilateral, diffuse, focal, hypoechoic, orhyperechoic.37,38
� Metastases to the testes are rare. The mostcommon primary sources are prostate, lung,melanoma, colon, and renal, in descendingprevalence (Fig. 8).39
Testicular Microlithiasis
Testicular microlithiasis (TM) is usually an inci-dental finding on a scrotal US (if associated with
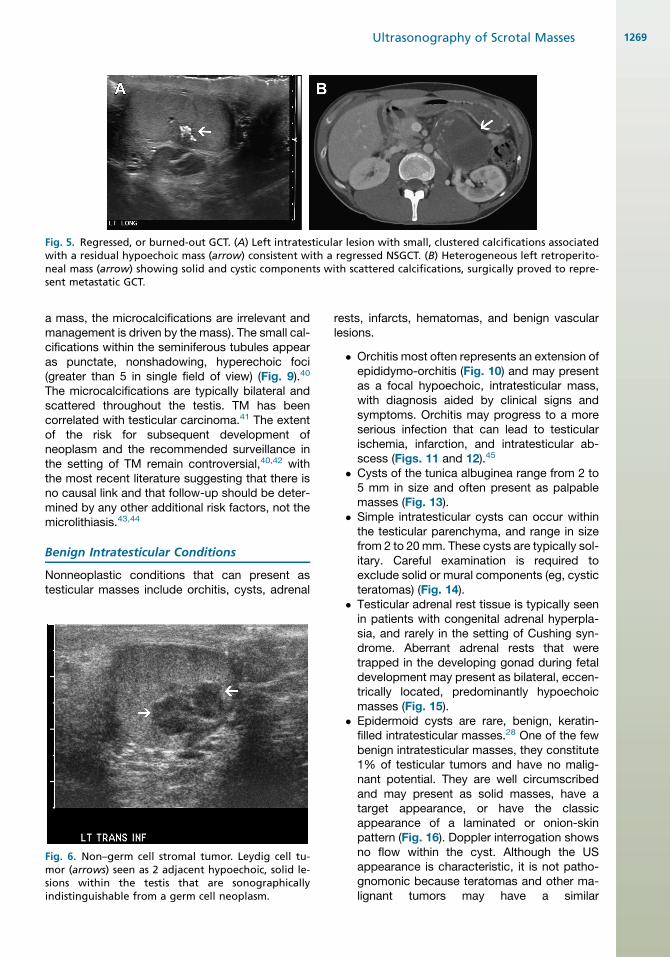
Fig. 5. Regressed, or burned-out GCT. (A) Left intratesticular lesion with small, clustered calcifications associatedwith a residual hypoechoic mass (arrow) consistent with a regressed NSGCT. (B) Heterogeneous left retroperito-neal mass (arrow) showing solid and cystic components with scattered calcifications, surgically proved to repre-sent metastatic GCT.
Ultrasonography of Scrotal Masses 1269
a mass, the microcalcifications are irrelevant andmanagement is driven by the mass). The small cal-cifications within the seminiferous tubules appearas punctate, nonshadowing, hyperechoic foci(greater than 5 in single field of view) (Fig. 9).40
The microcalcifications are typically bilateral andscattered throughout the testis. TM has beencorrelated with testicular carcinoma.41 The extentof the risk for subsequent development ofneoplasm and the recommended surveillance inthe setting of TM remain controversial,40,42 withthe most recent literature suggesting that there isno causal link and that follow-up should be deter-mined by any other additional risk factors, not themicrolithiasis.43,44
Benign Intratesticular Conditions
Nonneoplastic conditions that can present astesticular masses include orchitis, cysts, adrenal
Fig. 6. Non–germ cell stromal tumor. Leydig cell tu-mor (arrows) seen as 2 adjacent hypoechoic, solid le-sions within the testis that are sonographicallyindistinguishable from a germ cell neoplasm.
rests, infarcts, hematomas, and benign vascularlesions.
� Orchitis most often represents an extension ofepididymo-orchitis (Fig. 10) and may presentas a focal hypoechoic, intratesticular mass,with diagnosis aided by clinical signs andsymptoms. Orchitis may progress to a moreserious infection that can lead to testicularischemia, infarction, and intratesticular ab-scess (Figs. 11 and 12).45
� Cysts of the tunica albuginea range from 2 to5 mm in size and often present as palpablemasses (Fig. 13).
� Simple intratesticular cysts can occur withinthe testicular parenchyma, and range in sizefrom 2 to 20 mm. These cysts are typically sol-itary. Careful examination is required toexclude solid or mural components (eg, cysticteratomas) (Fig. 14).
� Testicular adrenal rest tissue is typically seenin patients with congenital adrenal hyperpla-sia, and rarely in the setting of Cushing syn-drome. Aberrant adrenal rests that weretrapped in the developing gonad during fetaldevelopment may present as bilateral, eccen-trically located, predominantly hypoechoicmasses (Fig. 15).
� Epidermoid cysts are rare, benign, keratin-filled intratesticular masses.28 One of the fewbenign intratesticular masses, they constitute1% of testicular tumors and have no malig-nant potential. They are well circumscribedand may present as solid masses, have atarget appearance, or have the classicappearance of a laminated or onion-skinpattern (Fig. 16). Doppler interrogation showsno flow within the cyst. Although the USappearance is characteristic, it is not patho-gnomonic because teratomas and other ma-lignant tumors may have a similar
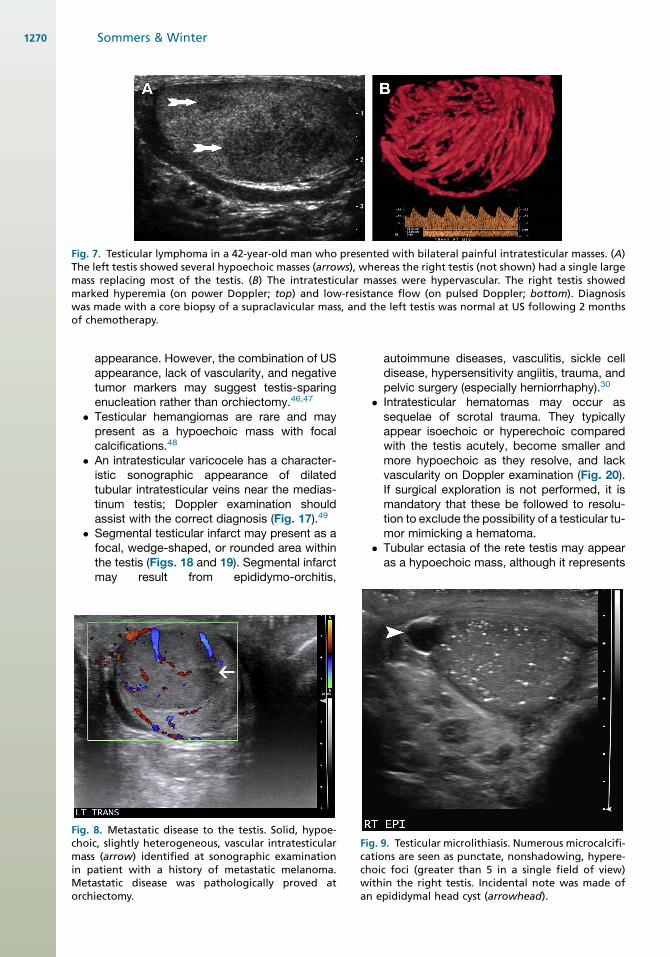
Fig. 7. Testicular lymphoma in a 42-year-old man who presented with bilateral painful intratesticular masses. (A)The left testis showed several hypoechoic masses (arrows), whereas the right testis (not shown) had a single largemass replacing most of the testis. (B) The intratesticular masses were hypervascular. The right testis showedmarked hyperemia (on power Doppler; top) and low-resistance flow (on pulsed Doppler; bottom). Diagnosiswas made with a core biopsy of a supraclavicular mass, and the left testis was normal at US following 2 monthsof chemotherapy.
FichminMor
Sommers & Winter1270
appearance. However, the combination of USappearance, lack of vascularity, and negativetumor markers may suggest testis-sparingenucleation rather than orchiectomy.46,47
� Testicular hemangiomas are rare and maypresent as a hypoechoic mass with focalcalcifications.48
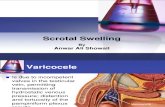
� An intratesticular varicocele has a character-istic sonographic appearance of dilatedtubular intratesticular veins near the medias-tinum testis; Doppler examination shouldassist with the correct diagnosis (Fig. 17).49
� Segmental testicular infarct may present as afocal, wedge-shaped, or rounded area withinthe testis (Figs. 18 and 19). Segmental infarctmay result from epididymo-orchitis,
g. 8. Metastatic disease to the testis. Solid, hypoe-oic, slightly heterogeneous, vascular intratesticularass (arrow) identified at sonographic examinationpatient with a history of metastatic melanoma.
etastatic disease was pathologically proved atchiectomy.
Ficachwan
autoimmune diseases, vasculitis, sickle celldisease, hypersensitivity angiitis, trauma, andpelvic surgery (especially herniorrhaphy).30
� Intratesticular hematomas may occur assequelae of scrotal trauma. They typicallyappear isoechoic or hyperechoic comparedwith the testis acutely, become smaller andmore hypoechoic as they resolve, and lackvascularity on Doppler examination (Fig. 20).If surgical exploration is not performed, it ismandatory that these be followed to resolu-tion to exclude the possibility of a testicular tu-mor mimicking a hematoma.
� Tubular ectasia of the rete testis may appearas a hypoechoic mass, although it represents
g. 9. Testicular microlithiasis. Numerous microcalcifi-tions are seen as punctate, nonshadowing, hypere-oic foci (greater than 5 in a single field of view)ithin the right testis. Incidental note was made ofepididymal head cyst (arrowhead).
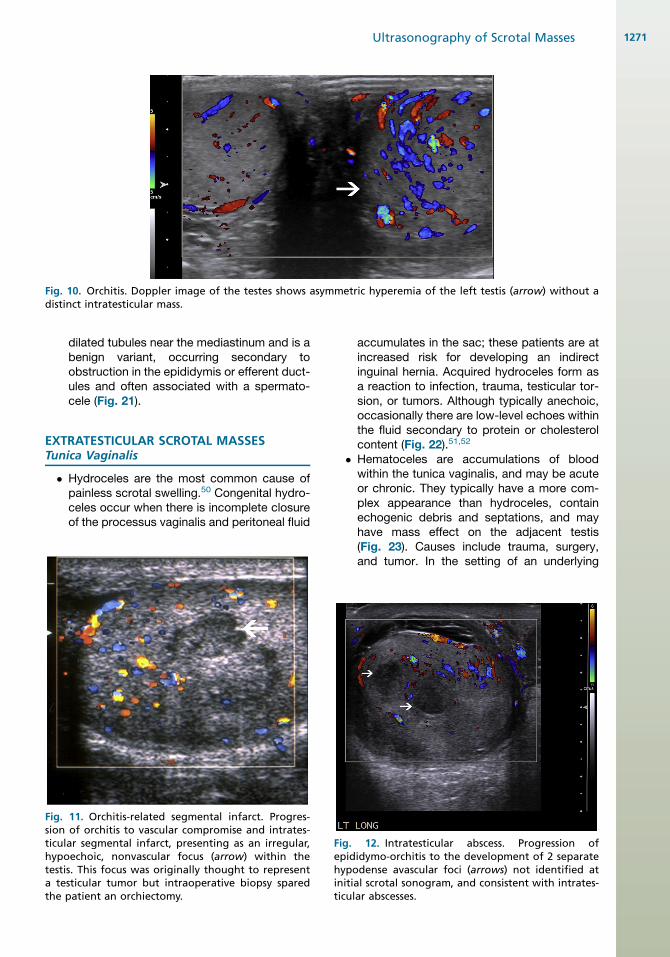
Fig. 10. Orchitis. Doppler image of the testes shows asymmetric hyperemia of the left testis (arrow) without adistinct intratesticular mass.
Fisiotichyteath
Ultrasonography of Scrotal Masses 1271
dilated tubules near the mediastinum and is abenign variant, occurring secondary toobstruction in the epididymis or efferent duct-ules and often associated with a spermato-cele (Fig. 21).
EXTRATESTICULAR SCROTAL MASSESTunica Vaginalis
� Hydroceles are the most common cause ofpainless scrotal swelling.50 Congenital hydro-celes occur when there is incomplete closureof the processus vaginalis and peritoneal fluid
g. 11. Orchitis-related segmental infarct. Progres-n of orchitis to vascular compromise and intrates-ular segmental infarct, presenting as an irregular,poechoic, nonvascular focus (arrow) within thestis. This focus was originally thought to representtesticular tumor but intraoperative biopsy sparede patient an orchiectomy.
Fiephyintic
accumulates in the sac; these patients are atincreased risk for developing an indirectinguinal hernia. Acquired hydroceles form asa reaction to infection, trauma, testicular tor-sion, or tumors. Although typically anechoic,occasionally there are low-level echoes withinthe fluid secondary to protein or cholesterolcontent (Fig. 22).51,52
� Hematoceles are accumulations of bloodwithin the tunica vaginalis, and may be acuteor chronic. They typically have a more com-plex appearance than hydroceles, containechogenic debris and septations, and mayhave mass effect on the adjacent testis(Fig. 23). Causes include trauma, surgery,and tumor. In the setting of an underlying
g. 12. Intratesticular abscess. Progression ofididymo-orchitis to the development of 2 separatepodense avascular foci (arrows) not identified atitial scrotal sonogram, and consistent with intrates-ular abscesses.
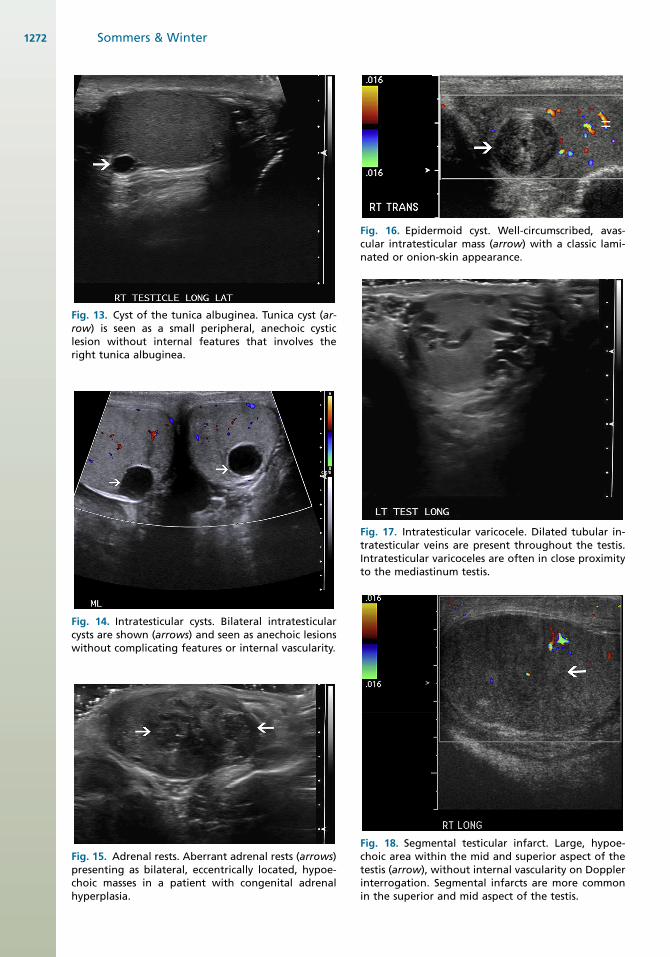
Fig. 13. Cyst of the tunica albuginea. Tunica cyst (ar-row) is seen as a small peripheral, anechoic cysticlesion without internal features that involves theright tunica albuginea.
Fig. 14. Intratesticular cysts. Bilateral intratesticularcysts are shown (arrows) and seen as anechoic lesionswithout complicating features or internal vascularity.
Fig. 15. Adrenal rests. Aberrant adrenal rests (arrows)presenting as bilateral, eccentrically located, hypoe-choic masses in a patient with congenital adrenalhyperplasia.
Fig. 16. Epidermoid cyst. Well-circumscribed, avas-cular intratesticular mass (arrow) with a classic lami-nated or onion-skin appearance.
Fig. 17. Intratesticular varicocele. Dilated tubular in-tratesticular veins are present throughout the testis.Intratesticular varicoceles are often in close proximityto the mediastinum testis.
Fig. 18. Segmental testicular infarct. Large, hypoe-choic area within the mid and superior aspect of thetestis (arrow), without internal vascularity on Dopplerinterrogation. Segmental infarcts are more commonin the superior and mid aspect of the testis.
Sommers & Winter1272
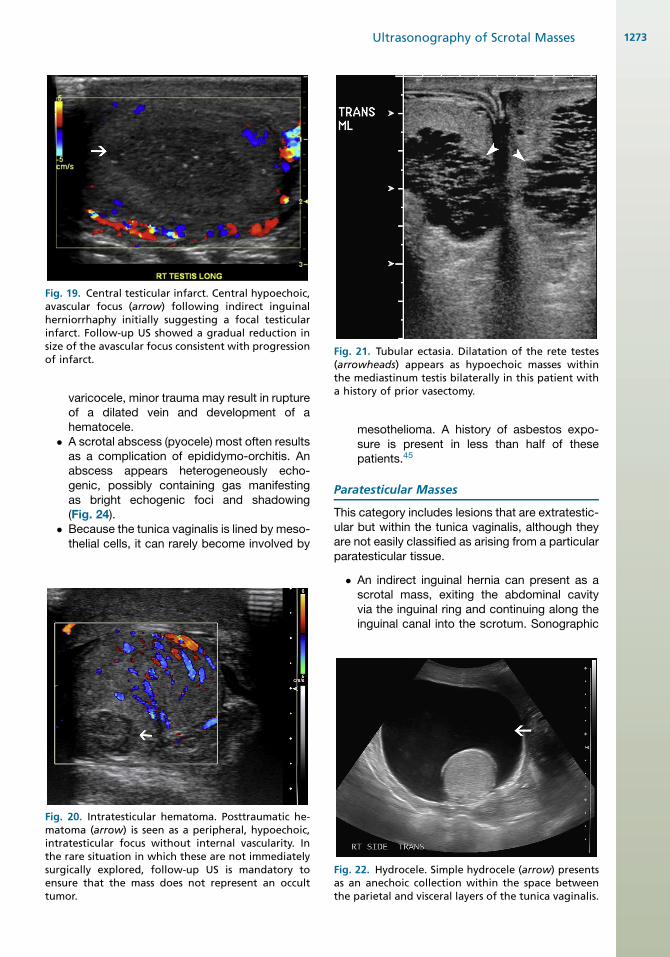
Fig. 19. Central testicular infarct. Central hypoechoic,avascular focus (arrow) following indirect inguinalherniorrhaphy initially suggesting a focal testicularinfarct. Follow-up US showed a gradual reduction insize of the avascular focus consistent with progressionof infarct.
Fiminthsuentu
Fig. 21. Tubular ectasia. Dilatation of the rete testes(arrowheads) appears as hypoechoic masses withinthe mediastinum testis bilaterally in this patient witha history of prior vasectomy.
Ultrasonography of Scrotal Masses 1273
varicocele, minor trauma may result in ruptureof a dilated vein and development of ahematocele.
� A scrotal abscess (pyocele) most often resultsas a complication of epididymo-orchitis. Anabscess appears heterogeneously echo-genic, possibly containing gas manifestingas bright echogenic foci and shadowing(Fig. 24).
� Because the tunica vaginalis is lined by meso-thelial cells, it can rarely become involved by
g. 20. Intratesticular hematoma. Posttraumatic he-atoma (arrow) is seen as a peripheral, hypoechoic,tratesticular focus without internal vascularity. Ine rare situation in which these are not immediatelyrgically explored, follow-up US is mandatory tosure that the mass does not represent an occultmor.
mesothelioma. A history of asbestos expo-sure is present in less than half of thesepatients.45
Paratesticular Masses
This category includes lesions that are extratestic-ular but within the tunica vaginalis, although theyare not easily classified as arising from a particularparatesticular tissue.
� An indirect inguinal hernia can present as ascrotal mass, exiting the abdominal cavityvia the inguinal ring and continuing along theinguinal canal into the scrotum. Sonographic
Fig. 22. Hydrocele. Simple hydrocele (arrow) presentsas an anechoic collection within the space betweenthe parietal and visceral layers of the tunica vaginalis.
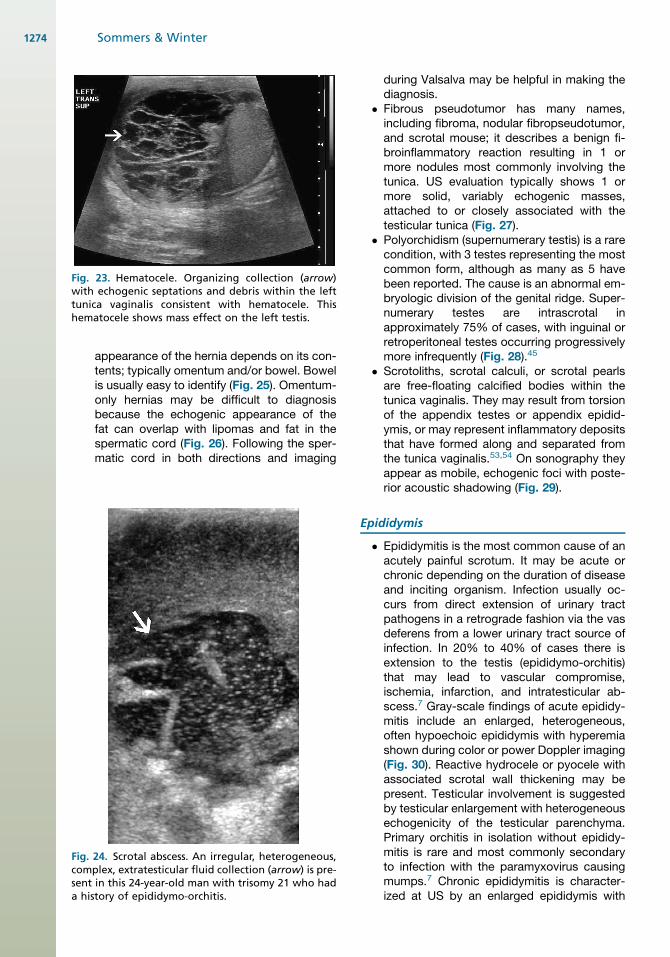
Fig. 23. Hematocele. Organizing collection (arrow)with echogenic septations and debris within the lefttunica vaginalis consistent with hematocele. Thishematocele shows mass effect on the left testis.
Ficosea
Sommers & Winter1274
appearance of the hernia depends on its con-tents; typically omentum and/or bowel. Bowelis usually easy to identify (Fig. 25). Omentum-only hernias may be difficult to diagnosisbecause the echogenic appearance of thefat can overlap with lipomas and fat in thespermatic cord (Fig. 26). Following the sper-matic cord in both directions and imaging
g. 24. Scrotal abscess. An irregular, heterogeneous,mplex, extratesticular fluid collection (arrow) is pre-nt in this 24-year-old man with trisomy 21 who hadhistory of epididymo-orchitis.
during Valsalva may be helpful in making thediagnosis.
� Fibrous pseudotumor has many names,including fibroma, nodular fibropseudotumor,and scrotal mouse; it describes a benign fi-broinflammatory reaction resulting in 1 ormore nodules most commonly involving thetunica. US evaluation typically shows 1 ormore solid, variably echogenic masses,attached to or closely associated with thetesticular tunica (Fig. 27).
� Polyorchidism (supernumerary testis) is a rarecondition, with 3 testes representing the mostcommon form, although as many as 5 havebeen reported. The cause is an abnormal em-bryologic division of the genital ridge. Super-numerary testes are intrascrotal inapproximately 75% of cases, with inguinal orretroperitoneal testes occurring progressivelymore infrequently (Fig. 28).45
� Scrotoliths, scrotal calculi, or scrotal pearlsare free-floating calcified bodies within thetunica vaginalis. They may result from torsionof the appendix testes or appendix epidid-ymis, or may represent inflammatory depositsthat have formed along and separated fromthe tunica vaginalis.53,54 On sonography theyappear as mobile, echogenic foci with poste-rior acoustic shadowing (Fig. 29).
Epididymis
� Epididymitis is the most common cause of anacutely painful scrotum. It may be acute orchronic depending on the duration of diseaseand inciting organism. Infection usually oc-curs from direct extension of urinary tractpathogens in a retrograde fashion via the vasdeferens from a lower urinary tract source ofinfection. In 20% to 40% of cases there isextension to the testis (epididymo-orchitis)that may lead to vascular compromise,ischemia, infarction, and intratesticular ab-scess.7 Gray-scale findings of acute epididy-mitis include an enlarged, heterogeneous,often hypoechoic epididymis with hyperemiashown during color or power Doppler imaging(Fig. 30). Reactive hydrocele or pyocele withassociated scrotal wall thickening may bepresent. Testicular involvement is suggestedby testicular enlargement with heterogeneousechogenicity of the testicular parenchyma.Primary orchitis in isolation without epididy-mitis is rare and most commonly secondaryto infection with the paramyxovirus causingmumps.7 Chronic epididymitis is character-ized at US by an enlarged epididymis with
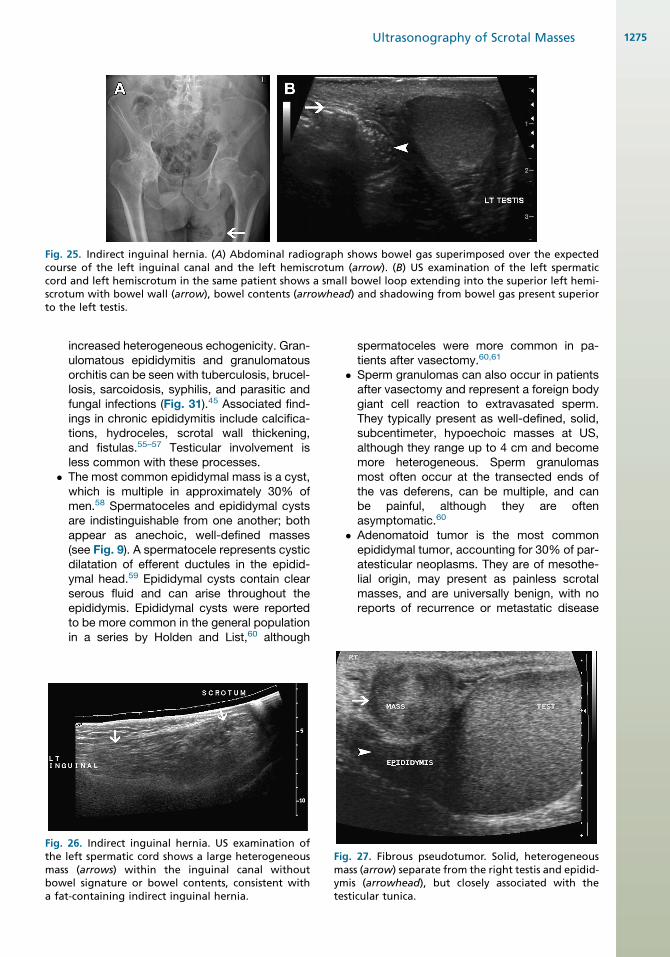
Fig. 25. Indirect inguinal hernia. (A) Abdominal radiograph shows bowel gas superimposed over the expectedcourse of the left inguinal canal and the left hemiscrotum (arrow). (B) US examination of the left spermaticcord and left hemiscrotum in the same patient shows a small bowel loop extending into the superior left hemi-scrotum with bowel wall (arrow), bowel contents (arrowhead) and shadowing from bowel gas present superiorto the left testis.
Fithmboa
Ultrasonography of Scrotal Masses 1275
increased heterogeneous echogenicity. Gran-ulomatous epididymitis and granulomatousorchitis can be seen with tuberculosis, brucel-losis, sarcoidosis, syphilis, and parasitic andfungal infections (Fig. 31).45 Associated find-ings in chronic epididymitis include calcifica-tions, hydroceles, scrotal wall thickening,and fistulas.55–57 Testicular involvement isless common with these processes.
� The most common epididymal mass is a cyst,which is multiple in approximately 30% ofmen.58 Spermatoceles and epididymal cystsare indistinguishable from one another; bothappear as anechoic, well-defined masses(see Fig. 9). A spermatocele represents cysticdilatation of efferent ductules in the epidid-ymal head.59 Epididymal cysts contain clearserous fluid and can arise throughout theepididymis. Epididymal cysts were reportedto be more common in the general populationin a series by Holden and List,60 although
g. 26. Indirect inguinal hernia. US examination ofe left spermatic cord shows a large heterogeneousass (arrows) within the inguinal canal withoutwel signature or bowel contents, consistent withfat-containing indirect inguinal hernia.
Fimymte
spermatoceles were more common in pa-tients after vasectomy.60,61
� Sperm granulomas can also occur in patientsafter vasectomy and represent a foreign bodygiant cell reaction to extravasated sperm.They typically present as well-defined, solid,subcentimeter, hypoechoic masses at US,although they range up to 4 cm and becomemore heterogeneous. Sperm granulomasmost often occur at the transected ends ofthe vas deferens, can be multiple, and canbe painful, although they are oftenasymptomatic.60
� Adenomatoid tumor is the most commonepididymal tumor, accounting for 30% of par-atesticular neoplasms. They are of mesothe-lial origin, may present as painless scrotalmasses, and are universally benign, with noreports of recurrence or metastatic disease
g. 27. Fibrous pseudotumor. Solid, heterogeneousass (arrow) separate from the right testis and epidid-is (arrowhead), but closely associated with thesticular tunica.
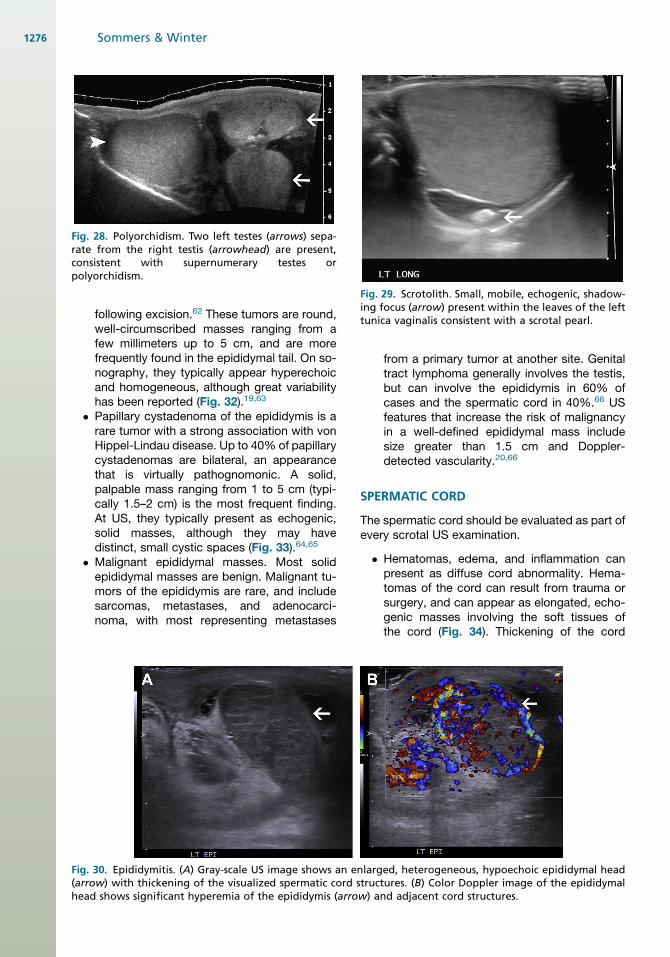
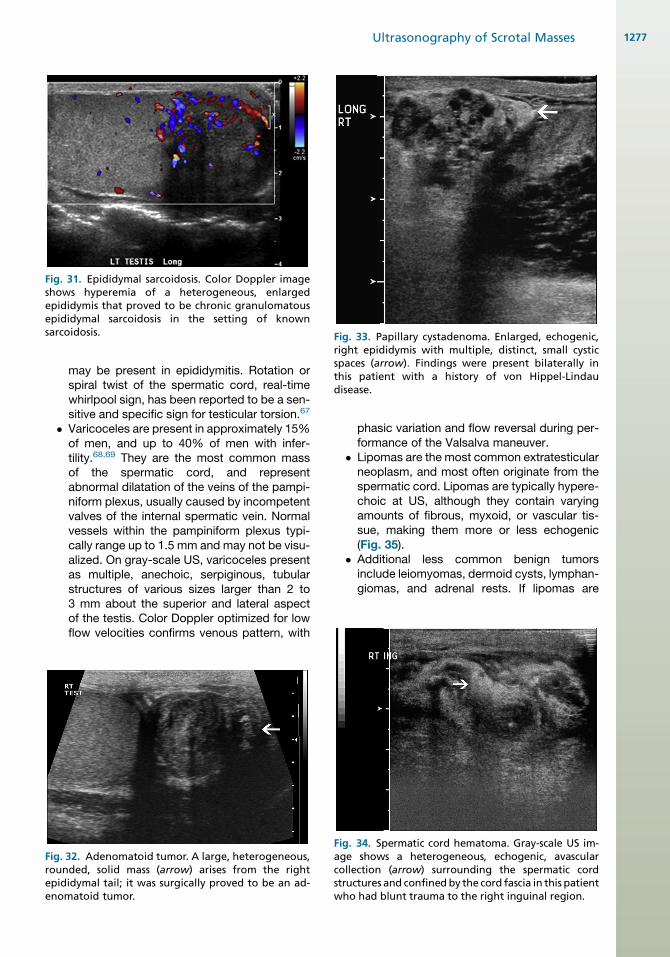
Fig. 28. Polyorchidism. Two left testes (arrows) sepa-rate from the right testis (arrowhead) are present,consistent with supernumerary testes orpolyorchidism.
Fig. 29. Scrotolith. Small, mobile, echogenic, shadow-ing focus (arrow) present within the leaves of the lefttunica vaginalis consistent with a scrotal pearl.
Fi(ahe
Sommers & Winter1276
following excision.62 These tumors are round,well-circumscribed masses ranging from afew millimeters up to 5 cm, and are morefrequently found in the epididymal tail. On so-nography, they typically appear hyperechoicand homogeneous, although great variabilityhas been reported (Fig. 32).19,63
� Papillary cystadenoma of the epididymis is arare tumor with a strong association with vonHippel-Lindau disease. Up to 40% of papillarycystadenomas are bilateral, an appearancethat is virtually pathognomonic. A solid,palpable mass ranging from 1 to 5 cm (typi-cally 1.5–2 cm) is the most frequent finding.At US, they typically present as echogenic,solid masses, although they may havedistinct, small cystic spaces (Fig. 33).64,65
� Malignant epididymal masses. Most solidepididymal masses are benign. Malignant tu-mors of the epididymis are rare, and includesarcomas, metastases, and adenocarci-noma, with most representing metastases
g. 30. Epididymitis. (A) Gray-scale US image shows an enlarrow) with thickening of the visualized spermatic cord strad shows significant hyperemia of the epididymis (arrow)
from a primary tumor at another site. Genitaltract lymphoma generally involves the testis,but can involve the epididymis in 60% ofcases and the spermatic cord in 40%.66 USfeatures that increase the risk of malignancyin a well-defined epididymal mass includesize greater than 1.5 cm and Doppler-detected vascularity.20,66
SPERMATIC CORD
The spermatic cord should be evaluated as part ofevery scrotal US examination.
� Hematomas, edema, and inflammation canpresent as diffuse cord abnormality. Hema-tomas of the cord can result from trauma orsurgery, and can appear as elongated, echo-genic masses involving the soft tissues ofthe cord (Fig. 34). Thickening of the cord
rged, heterogeneous, hypoechoic epididymal heaductures. (B) Color Doppler image of the epididymaland adjacent cord structures.
Firoepen
Fig. 31. Epididymal sarcoidosis. Color Doppler imageshows hyperemia of a heterogeneous, enlargedepididymis that proved to be chronic granulomatousepididymal sarcoidosis in the setting of knownsarcoidosis. Fig. 33. Papillary cystadenoma. Enlarged, echogenic,
right epididymis with multiple, distinct, small cysticspaces (arrow). Findings were present bilaterally inthis patient with a history of von Hippel-Lindaudisease.
Ultrasonography of Scrotal Masses 1277
may be present in epididymitis. Rotation orspiral twist of the spermatic cord, real-timewhirlpool sign, has been reported to be a sen-sitive and specific sign for testicular torsion.67
� Varicoceles are present in approximately 15%of men, and up to 40% of men with infer-tility.68,69 They are the most common massof the spermatic cord, and representabnormal dilatation of the veins of the pampi-niform plexus, usually caused by incompetentvalves of the internal spermatic vein. Normalvessels within the pampiniform plexus typi-cally range up to 1.5 mm and may not be visu-alized. On gray-scale US, varicoceles presentas multiple, anechoic, serpiginous, tubularstructures of various sizes larger than 2 to3 mm about the superior and lateral aspectof the testis. Color Doppler optimized for lowflow velocities confirms venous pattern, with
g. 32. Adenomatoid tumor. A large, heterogeneous,unded, solid mass (arrow) arises from the rightididymal tail; it was surgically proved to be an ad-omatoid tumor.
Fiagcostw
phasic variation and flow reversal during per-formance of the Valsalva maneuver.
� Lipomas are the most common extratesticularneoplasm, and most often originate from thespermatic cord. Lipomas are typically hypere-choic at US, although they contain varyingamounts of fibrous, myxoid, or vascular tis-sue, making them more or less echogenic(Fig. 35).
� Additional less common benign tumorsinclude leiomyomas, dermoid cysts, lymphan-giomas, and adrenal rests. If lipomas are
g. 34. Spermatic cord hematoma. Gray-scale US im-e shows a heterogeneous, echogenic, avascularllection (arrow) surrounding the spermatic cordructures and confinedby the cord fascia in this patientho had blunt trauma to the right inguinal region.
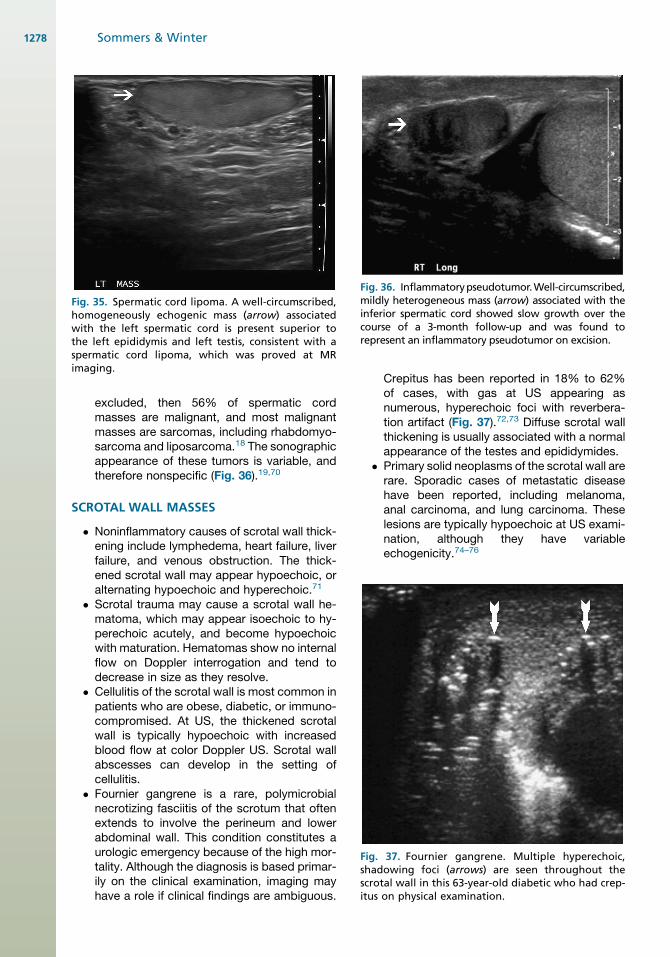
Fig. 35. Spermatic cord lipoma. A well-circumscribed,homogeneously echogenic mass (arrow) associatedwith the left spermatic cord is present superior tothe left epididymis and left testis, consistent with aspermatic cord lipoma, which was proved at MRimaging.
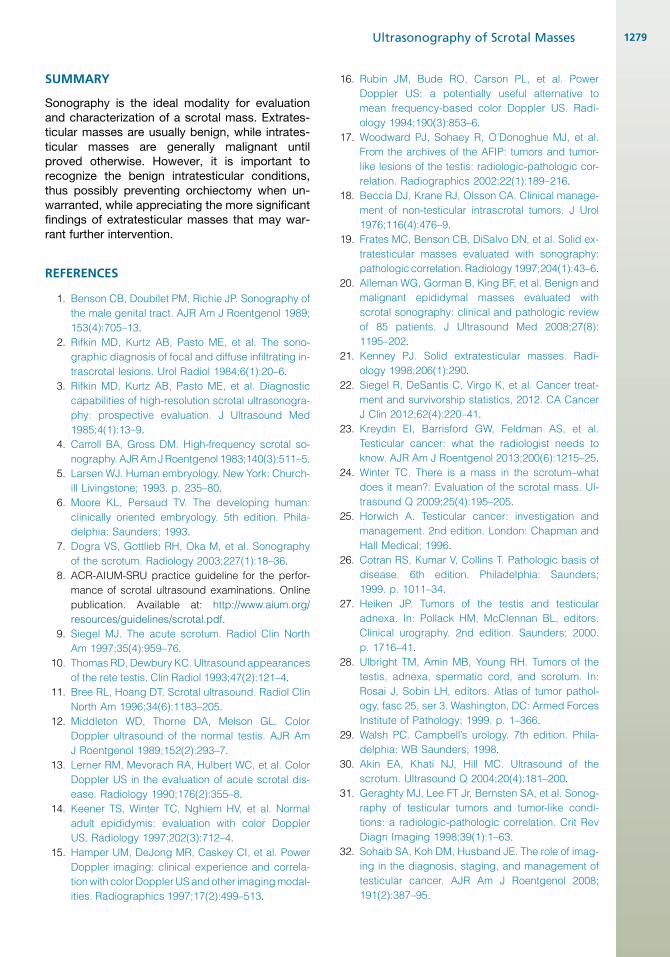
Fig. 36. Inflammatorypseudotumor.Well-circumscribed,mildly heterogeneous mass (arrow) associated with theinferior spermatic cord showed slow growth over thecourse of a 3-month follow-up and was found torepresent an inflammatory pseudotumor on excision.
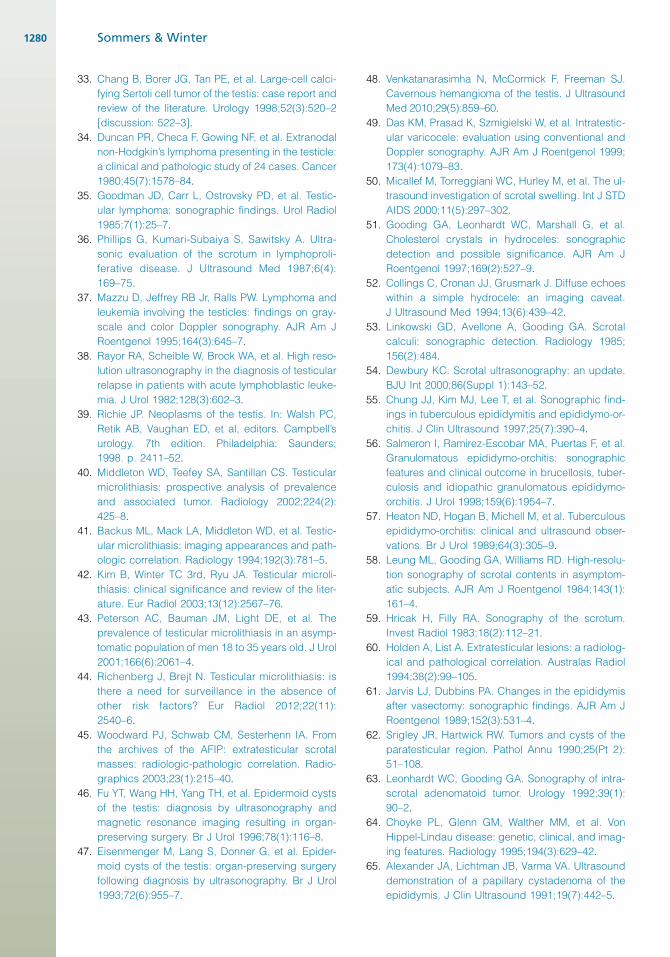
Fig. 37. Fournier gangrene. Multiple hyperechoic,shadowing foci (arrows) are seen throughout thescrotal wall in this 63-year-old diabetic who had crep-itus on physical examination.
Sommers & Winter1278
excluded, then 56% of spermatic cordmasses are malignant, and most malignantmasses are sarcomas, including rhabdomyo-sarcoma and liposarcoma.18 The sonographicappearance of these tumors is variable, andtherefore nonspecific (Fig. 36).19,70
SCROTAL WALL MASSES
� Noninflammatory causes of scrotal wall thick-ening include lymphedema, heart failure, liverfailure, and venous obstruction. The thick-ened scrotal wall may appear hypoechoic, oralternating hypoechoic and hyperechoic.71
� Scrotal trauma may cause a scrotal wall he-matoma, which may appear isoechoic to hy-perechoic acutely, and become hypoechoicwith maturation. Hematomas show no internalflow on Doppler interrogation and tend todecrease in size as they resolve.
� Cellulitis of the scrotal wall is most common inpatients who are obese, diabetic, or immuno-compromised. At US, the thickened scrotalwall is typically hypoechoic with increasedblood flow at color Doppler US. Scrotal wallabscesses can develop in the setting ofcellulitis.
� Fournier gangrene is a rare, polymicrobialnecrotizing fasciitis of the scrotum that oftenextends to involve the perineum and lowerabdominal wall. This condition constitutes aurologic emergency because of the high mor-tality. Although the diagnosis is based primar-ily on the clinical examination, imaging mayhave a role if clinical findings are ambiguous.
Crepitus has been reported in 18% to 62%of cases, with gas at US appearing asnumerous, hyperechoic foci with reverbera-tion artifact (Fig. 37).72,73 Diffuse scrotal wallthickening is usually associated with a normalappearance of the testes and epididymides.
� Primary solid neoplasms of the scrotal wall arerare. Sporadic cases of metastatic diseasehave been reported, including melanoma,anal carcinoma, and lung carcinoma. Theselesions are typically hypoechoic at US exami-nation, although they have variableechogenicity.74–76
Ultrasonography of Scrotal Masses 1279
SUMMARY
Sonography is the ideal modality for evaluationand characterization of a scrotal mass. Extrates-ticular masses are usually benign, while intrates-ticular masses are generally malignant untilproved otherwise. However, it is important torecognize the benign intratesticular conditions,thus possibly preventing orchiectomy when un-warranted, while appreciating the more significantfindings of extratesticular masses that may war-rant further intervention.
REFERENCES
1. Benson CB, Doubilet PM, Richie JP. Sonography of
the male genital tract. AJR Am J Roentgenol 1989;
153(4):705–13.
2. Rifkin MD, Kurtz AB, Pasto ME, et al. The sono-
graphic diagnosis of focal and diffuse infiltrating in-
trascrotal lesions. Urol Radiol 1984;6(1):20–6.
3. Rifkin MD, Kurtz AB, Pasto ME, et al. Diagnostic
capabilities of high-resolution scrotal ultrasonogra-
phy: prospective evaluation. J Ultrasound Med
1985;4(1):13–9.
4. Carroll BA, Gross DM. High-frequency scrotal so-
nography. AJRAmJRoentgenol 1983;140(3):511–5.
5. Larsen WJ. Human embryology. New York: Church-
ill Livingstone; 1993. p. 235–80.
6. Moore KL, Persaud TV. The developing human:
clinically oriented embryology. 5th edition. Phila-
delphia: Saunders; 1993.
7. Dogra VS, Gottlieb RH, Oka M, et al. Sonography
of the scrotum. Radiology 2003;227(1):18–36.
8. ACR-AIUM-SRU practice guideline for the perfor-
mance of scrotal ultrasound examinations. Online
publication. Available at: http://www.aium.org/
resources/guidelines/scrotal.pdf.
9. Siegel MJ. The acute scrotum. Radiol Clin North
Am 1997;35(4):959–76.
10. Thomas RD, Dewbury KC. Ultrasound appearances
of the rete testis. Clin Radiol 1993;47(2):121–4.
11. Bree RL, Hoang DT. Scrotal ultrasound. Radiol Clin
North Am 1996;34(6):1183–205.
12. Middleton WD, Thorne DA, Melson GL. Color
Doppler ultrasound of the normal testis. AJR Am
J Roentgenol 1989;152(2):293–7.
13. Lerner RM, Mevorach RA, Hulbert WC, et al. Color
Doppler US in the evaluation of acute scrotal dis-
ease. Radiology 1990;176(2):355–8.
14. Keener TS, Winter TC, Nghiem HV, et al. Normal
adult epididymis: evaluation with color Doppler
US. Radiology 1997;202(3):712–4.
15. Hamper UM, DeJong MR, Caskey CI, et al. Power
Doppler imaging: clinical experience and correla-
tionwith color Doppler US and other imagingmodal-
ities. Radiographics 1997;17(2):499–513.
16. Rubin JM, Bude RO, Carson PL, et al. Power
Doppler US: a potentially useful alternative to
mean frequency-based color Doppler US. Radi-
ology 1994;190(3):853–6.
17. Woodward PJ, Sohaey R, O’Donoghue MJ, et al.
From the archives of the AFIP: tumors and tumor-
like lesions of the testis: radiologic-pathologic cor-
relation. Radiographics 2002;22(1):189–216.
18. Beccia DJ, Krane RJ, Olsson CA. Clinical manage-
ment of non-testicular intrascrotal tumors. J Urol
1976;116(4):476–9.
19. Frates MC, Benson CB, DiSalvo DN, et al. Solid ex-
tratesticular masses evaluated with sonography:
pathologic correlation. Radiology 1997;204(1):43–6.
20. Alleman WG, Gorman B, King BF, et al. Benign and
malignant epididymal masses evaluated with
scrotal sonography: clinical and pathologic review
of 85 patients. J Ultrasound Med 2008;27(8):
1195–202.
21. Kenney PJ. Solid extratesticular masses. Radi-
ology 1998;206(1):290.
22. Siegel R, DeSantis C, Virgo K, et al. Cancer treat-
ment and survivorship statistics, 2012. CA Cancer
J Clin 2012;62(4):220–41.
23. Kreydin EI, Barrisford GW, Feldman AS, et al.
Testicular cancer: what the radiologist needs to
know. AJR Am J Roentgenol 2013;200(6):1215–25.
24. Winter TC. There is a mass in the scrotum–what
does it mean?: Evaluation of the scrotal mass. Ul-
trasound Q 2009;25(4):195–205.
25. Horwich A. Testicular cancer: investigation and
management. 2nd edition. London: Chapman and
Hall Medical; 1996.
26. Cotran RS, Kumar V, Collins T. Pathologic basis of
disease. 6th edition. Philadelphia: Saunders;
1999. p. 1011–34.
27. Heiken JP. Tumors of the testis and testicular
adnexa. In: Pollack HM, McClennan BL, editors.
Clinical urography. 2nd edition. Saunders; 2000.
p. 1716–41.
28. Ulbright TM, Amin MB, Young RH. Tumors of the
testis, adnexa, spermatic cord, and scrotum. In:
Rosai J, Sobin LH, editors. Atlas of tumor pathol-
ogy, fasc 25, ser 3. Washington, DC: Armed Forces
Institute of Pathology; 1999. p. 1–366.
29. Walsh PC. Campbell’s urology. 7th edition. Phila-
delphia: WB Saunders; 1998.
30. Akin EA, Khati NJ, Hill MC. Ultrasound of the
scrotum. Ultrasound Q 2004;20(4):181–200.
31. Geraghty MJ, Lee FT Jr, Bernsten SA, et al. Sonog-
raphy of testicular tumors and tumor-like condi-
tions: a radiologic-pathologic correlation. Crit Rev
Diagn Imaging 1998;39(1):1–63.
32. Sohaib SA, Koh DM, Husband JE. The role of imag-
ing in the diagnosis, staging, and management of
testicular cancer. AJR Am J Roentgenol 2008;
191(2):387–95.
Sommers & Winter1280
33. Chang B, Borer JG, Tan PE, et al. Large-cell calci-
fying Sertoli cell tumor of the testis: case report and
review of the literature. Urology 1998;52(3):520–2
[discussion: 522–3].
34. Duncan PR, Checa F, Gowing NF, et al. Extranodal
non-Hodgkin’s lymphoma presenting in the testicle:
a clinical and pathologic study of 24 cases. Cancer
1980;45(7):1578–84.
35. Goodman JD, Carr L, Ostrovsky PD, et al. Testic-
ular lymphoma: sonographic findings. Urol Radiol
1985;7(1):25–7.
36. Phillips G, Kumari-Subaiya S, Sawitsky A. Ultra-
sonic evaluation of the scrotum in lymphoproli-
ferative disease. J Ultrasound Med 1987;6(4):
169–75.
37. Mazzu D, Jeffrey RB Jr, Ralls PW. Lymphoma and
leukemia involving the testicles: findings on gray-
scale and color Doppler sonography. AJR Am J
Roentgenol 1995;164(3):645–7.
38. Rayor RA, Scheible W, Brock WA, et al. High reso-
lution ultrasonography in the diagnosis of testicular
relapse in patients with acute lymphoblastic leuke-
mia. J Urol 1982;128(3):602–3.
39. Richie JP. Neoplasms of the testis. In: Walsh PC,
Retik AB, Vaughan ED, et al, editors. Campbell’s
urology. 7th edition. Philadelphia: Saunders;
1998. p. 2411–52.
40. Middleton WD, Teefey SA, Santillan CS. Testicular
microlithiasis: prospective analysis of prevalence
and associated tumor. Radiology 2002;224(2):
425–8.
41. Backus ML, Mack LA, Middleton WD, et al. Testic-
ular microlithiasis: imaging appearances and path-
ologic correlation. Radiology 1994;192(3):781–5.
42. Kim B, Winter TC 3rd, Ryu JA. Testicular microli-
thiasis: clinical significance and review of the liter-
ature. Eur Radiol 2003;13(12):2567–76.
43. Peterson AC, Bauman JM, Light DE, et al. The
prevalence of testicular microlithiasis in an asymp-
tomatic population of men 18 to 35 years old. J Urol
2001;166(6):2061–4.
44. Richenberg J, Brejt N. Testicular microlithiasis: is
there a need for surveillance in the absence of
other risk factors? Eur Radiol 2012;22(11):
2540–6.
45. Woodward PJ, Schwab CM, Sesterhenn IA. From
the archives of the AFIP: extratesticular scrotal
masses: radiologic-pathologic correlation. Radio-
graphics 2003;23(1):215–40.
46. Fu YT, Wang HH, Yang TH, et al. Epidermoid cysts
of the testis: diagnosis by ultrasonography and
magnetic resonance imaging resulting in organ-
preserving surgery. Br J Urol 1996;78(1):116–8.
47. Eisenmenger M, Lang S, Donner G, et al. Epider-
moid cysts of the testis: organ-preserving surgery
following diagnosis by ultrasonography. Br J Urol
1993;72(6):955–7.
48. Venkatanarasimha N, McCormick F, Freeman SJ.
Cavernous hemangioma of the testis. J Ultrasound
Med 2010;29(5):859–60.
49. Das KM, Prasad K, Szmigielski W, et al. Intratestic-
ular varicocele: evaluation using conventional and
Doppler sonography. AJR Am J Roentgenol 1999;
173(4):1079–83.
50. Micallef M, Torreggiani WC, Hurley M, et al. The ul-
trasound investigation of scrotal swelling. Int J STD
AIDS 2000;11(5):297–302.
51. Gooding GA, Leonhardt WC, Marshall G, et al.
Cholesterol crystals in hydroceles: sonographic
detection and possible significance. AJR Am J
Roentgenol 1997;169(2):527–9.
52. Collings C, Cronan JJ, Grusmark J. Diffuse echoes
within a simple hydrocele: an imaging caveat.
J Ultrasound Med 1994;13(6):439–42.
53. Linkowski GD, Avellone A, Gooding GA. Scrotal
calculi: sonographic detection. Radiology 1985;
156(2):484.
54. Dewbury KC. Scrotal ultrasonography: an update.
BJU Int 2000;86(Suppl 1):143–52.
55. Chung JJ, Kim MJ, Lee T, et al. Sonographic find-
ings in tuberculous epididymitis and epididymo-or-
chitis. J Clin Ultrasound 1997;25(7):390–4.
56. Salmeron I, Ramirez-Escobar MA, Puertas F, et al.
Granulomatous epididymo-orchitis: sonographic
features and clinical outcome in brucellosis, tuber-
culosis and idiopathic granulomatous epididymo-
orchitis. J Urol 1998;159(6):1954–7.
57. Heaton ND, Hogan B, Michell M, et al. Tuberculous
epididymo-orchitis: clinical and ultrasound obser-
vations. Br J Urol 1989;64(3):305–9.
58. Leung ML, Gooding GA, Williams RD. High-resolu-
tion sonography of scrotal contents in asymptom-
atic subjects. AJR Am J Roentgenol 1984;143(1):
161–4.
59. Hricak H, Filly RA. Sonography of the scrotum.
Invest Radiol 1983;18(2):112–21.
60. Holden A, List A. Extratesticular lesions: a radiolog-
ical and pathological correlation. Australas Radiol
1994;38(2):99–105.
61. Jarvis LJ, Dubbins PA. Changes in the epididymis
after vasectomy: sonographic findings. AJR Am J
Roentgenol 1989;152(3):531–4.
62. Srigley JR, Hartwick RW. Tumors and cysts of the
paratesticular region. Pathol Annu 1990;25(Pt 2):
51–108.
63. Leonhardt WC, Gooding GA. Sonography of intra-
scrotal adenomatoid tumor. Urology 1992;39(1):
90–2.
64. Choyke PL, Glenn GM, Walther MM, et al. Von
Hippel-Lindau disease: genetic, clinical, and imag-
ing features. Radiology 1995;194(3):629–42.
65. Alexander JA, Lichtman JB, Varma VA. Ultrasound
demonstration of a papillary cystadenoma of the
epididymis. J Clin Ultrasound 1991;19(7):442–5.
Ultrasonography of Scrotal Masses 1281
66. Bostwick D. Spermatic cord and testicular adnexa.
In: Bostwick D, Eble JN, editors. Urologic surgical
pathology. St Louis (MO): Mosby; 1997. p. 647–74.
67. Vijayaraghavan SB. Sonographic differential diag-
nosis of acute scrotum: real-time whirlpool sign, a
key sign of torsion. J Ultrasound Med 2006;25(5):
563–74.
68. Meacham RB, Townsend RR, Rademacher D, et al.
The incidence of varicoceles in the general popula-
tion when evaluated by physical examination, gray
scale sonography and color Doppler sonography.
J Urol 1994;151(6):1535–8.
69. Kim ED, Lipshultz LI. Role of ultrasound in the
assessment of male infertility. J Clin Ultrasound
1996;24(8):437–53.
70. Haller J, Tscholakoff D, Gundry C, et al. Sonogra-
phy of unusual extratesticular lesions. Urol Radiol
1989;11(3):190–3.
71. Grainger AJ, Hide IG, Elliott ST. The ultrasound ap-
pearances of scrotal oedema. Eur J Ultrasound
1998;8(1):33–7.
72. Rajan DK, Scharer KA. Radiology of Fournier’s
gangrene.AJRAmJRoentgenol 1998;170(1):163–8.
73. Dogra VS, Smeltzer JS, Poblette J. Sonographic
diagnosis of Fournier’s gangrene. J Clin Ultrasound
1994;22(9):571–2.
74. Ferguson MA, White BA, Johnson DE, et al. Carci-
noma en cuirasse of the scrotum: an unusual pre-
sentation of lung carcinoma metastatic to the
scrotum. J Urol 1998;160(6 Pt 1):2154–5.
75. Nazzari G, Drago F, Malatto M, et al. Epidermoid
anal canal carcinoma metastatic to the skin. A clin-
ical mimic of prostate adenocarcinoma metasta-
ses. J Dermatol Surg Oncol 1994;20(11):765–6.
76. SiegalGP,GaffeyTA.Solitary leiomyomasarising from
the tunica dartos scroti. J Urol 1976;116(1):69–71.