UK IBD Audit 3 rd Round
29
Date of presentation Name of presenter UK IBD Audit 3 rd Round Comparison of (Your Site Name) results against the National Results for Clinical Audit of Adult IBD Inpatient Care in the UK
description
UK IBD Audit 3 rd Round. Comparison of (Your Site Name) results against the National Results for Clinical Audit of Adult IBD Inpatient Care in the UK. Participation in round 3:. 198 adults sites across the UK entered clinical audit data England = 161 sites Jersey = 1 site - PowerPoint PPT Presentation
Transcript of UK IBD Audit 3 rd Round

Date of presentation
Name of presenter
UK IBD Audit 3rd Round Comparison of
(Your Site Name) results against the National Results for Clinical Audit of Adult IBD Inpatient
Care in the UK
Participation in round 3:• 198 adults sites across the UK entered clinical
audit data• England = 161 sites• Jersey = 1 site• Northern Ireland = 10 sites• Scotland = 11 sites• Wales = 15 sites
• A ‘site’ typically constitutes a single hospital within a health board/trust. Where a health board/trust has more than one hospital offering independent IBD services they entered data for separate ‘sites’. Some institutions running a coordinated IBD service across two or more hospitals with the same staff took part as one health board/trust-wide site
Publication of results• Data was entered by sites onto a password protected audit web
tool under the direction of a designated site lead, in almost every case a Consultant Gastroenterologist
• Data entered between 1 September 2010 and 31 August 2011
• The results provide contemporary UK-wide data and all participating sites have received site-specific reports which will included local data for comparison against national averages (use this data to populate the ‘your site’ column in all following tables)
• The full National Report was launched on 21 February 2012
Key Results – Ulcerative colitisAdult IBD Care – Ulcerative Colitis. Table (3) of National Report UK Results v Your Site 2010 (page 8)
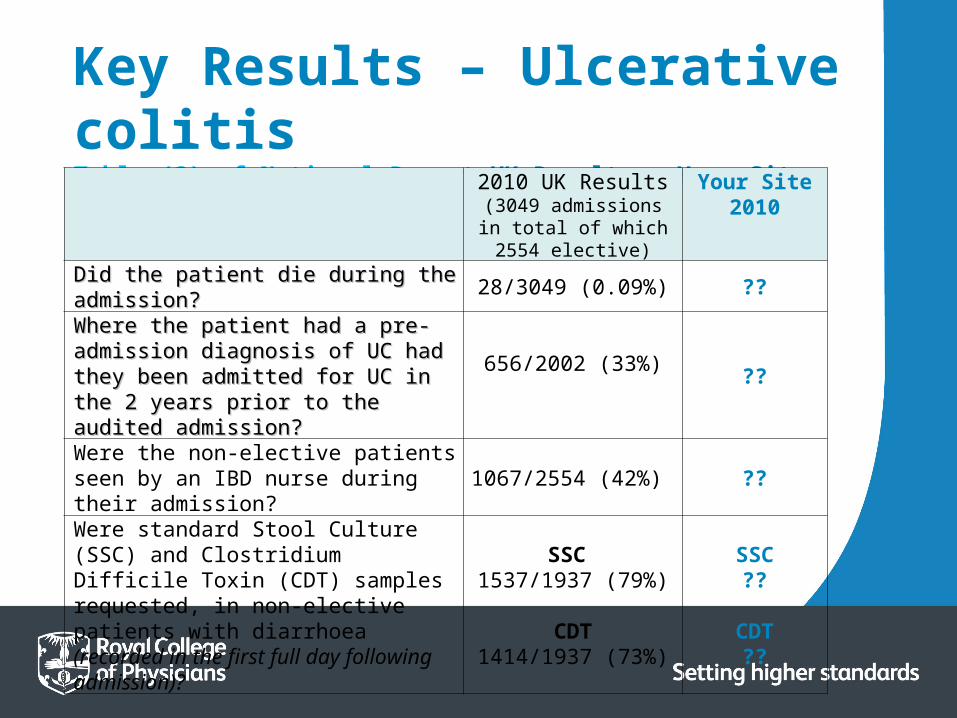
Key Results – Ulcerative colitisTable (3) of National Report UK Results v Your Site 2010
2010 UK Results(3049 admissions in total of which 2554 elective)
Your Site 2010
Did the patient die during the admission?Did the patient die during the admission? 28/3049 (0.09%) ??
Where the patient had a pre-admission Where the patient had a pre-admission diagnosis of UC had they been admitted for diagnosis of UC had they been admitted for UC in the 2 years prior to the audited UC in the 2 years prior to the audited admission? admission?
656/2002 (33%) ??
Were the non-elective patients seen by an IBD nurse during their admission? 1067/2554 (42%) ??
Were standard Stool Culture (SSC) and Clostridium Difficile Toxin (CDT) samples requested, in non-elective patients with diarrhoea (recorded in the first full day following admission)?
SSC 1537/1937 (79%)
CDT1414/1937 (73%)
SSC??
CDT??
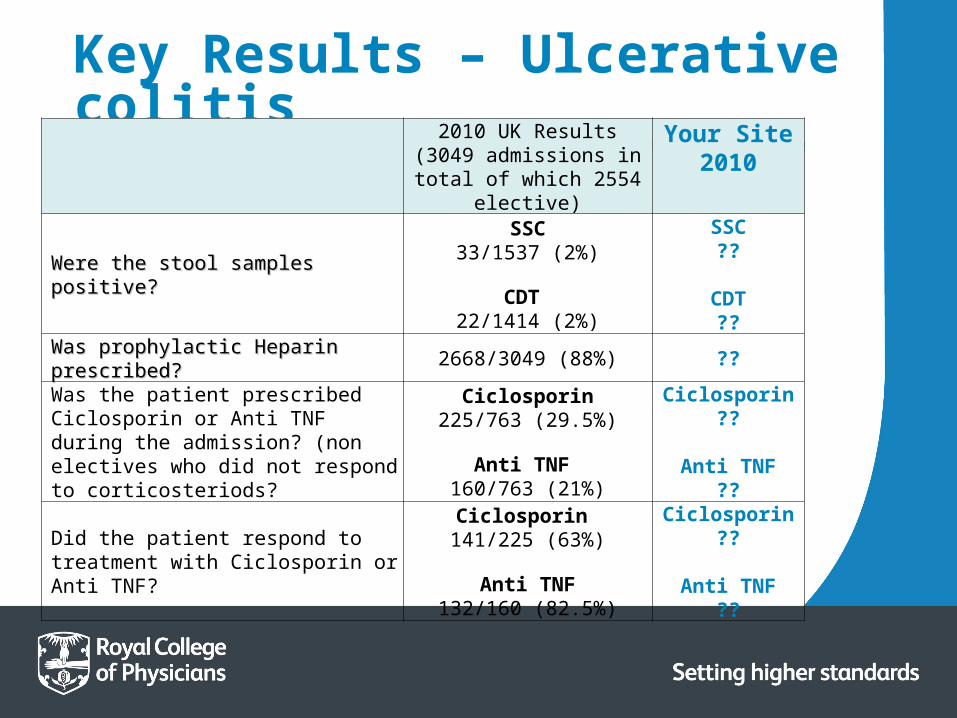
Key Results – Ulcerative colitisTable (3) of National Report UK Results v Your Site 2010
2010 UK Results(3049 admissions in total of
which 2554 elective)
Your Site 2010
Were the stool samples positive? Were the stool samples positive?
SSC33/1537 (2%)
CDT 22/1414 (2%)
SSC??
CDT??
Was prophylactic Heparin prescribed?Was prophylactic Heparin prescribed? 2668/3049 (88%) ??
Was the patient prescribed Ciclosporin or Anti TNF during the admission? (non electives who did not respond to corticosteriods?
Ciclosporin225/763 (29.5%)
Anti TNF 160/763 (21%)
Ciclosporin ??
Anti TNF??
Did the patient respond to treatment with Ciclosporin or Anti TNF?
Ciclosporin 141/225 (63%)
Anti TNF132/160 (82.5%)
Ciclosporin??
Anti TNF??

Key Results – Ulcerative colitisTable (3) of National Report UK Results v Your Site 2010
2010 UK Results(3049 admissions in total of
which 2554 elective)
Your Site 2010
In patients undergoing surgery, In patients undergoing surgery, was this undertaken was this undertaken laparoscopically?laparoscopically?
Elective 205/490 (42%) Elective ??
Non-Elective 98/317 (31%) Non-Elective ??
If the patient was prescribed If the patient was prescribed steroids on discharge, were they steroids on discharge, were they also prescribed bone protection also prescribed bone protection agents?agents?
1443/2194 (66%) ??

Key Findings – Ulcerative colitisUlcerative Colitis– findings relate to key results indicated in Table(3): Adult IBD Care – Ulcerative Colitis. UK Results v Your Site 2010 (page 10)
1. Mortality rate has halved over the 3 rounds
2. Statistically significant reduction in the number of patients who had been admitted to hospital for UC in the 2 years prior to the audited admission
3. Stool samples are now being sent significantly more frequently for both Standard Stool Cultures (SSC) and Clostridium Difficile Toxin (CDT), for UC patients admitted with diarrhoea
4. Significant reduction in the number of stool samples positive for CDT
5. Prophylactic Heparin is being prescribed more frequently
6. For patients failing to respond to IV steroids, the use of anti-TNF therapy has increased significantly and the use of Ciclosporin has dropped slightly
7. Significant improvement in response rates for anti-TNF therapy across rounds with an improved but non-significant rise in the response rates for Ciclosporin
8. Prescription of bone protection for patients discharged on steroids has increased
Key Findings – Ulcerative colitis:
Key Results – Crohn’s diseaseAdult IBD Care – Crohn’s Disease. Table (4) of National Report UK Results v Your Site 2010 (page 9)

Key Results – Crohn’s diseaseTable (4) of National Report UK Results v Your Site 2010
2010 UK Results(3122 admissions in total of
which 2571 elective)
Your Site 2010
Did the patient die during the admission?Did the patient die during the admission? 21/3122 (0.7%) ??
Was the patient admitted under the care of a Was the patient admitted under the care of a gastroenterology specialist?gastroenterology specialist? 983/2571 (38%) ??
Did the patient see an IBD nurse during their admission? 905/2571 (35%) ??
Was Anti-TNF therapy prescribed during the admission? (only includes non-elective patients indicated as not receiving Anti-TNF on admission)
186/2509 (7.4%) ??
In patient started on Anti TNF during this In patient started on Anti TNF during this admission, did they respond to the treatment?admission, did they respond to the treatment? 163/186 (87.6%) ??
Was prophylactic Heparin prescribed?Was prophylactic Heparin prescribed? 2708/3122 (87%) ??
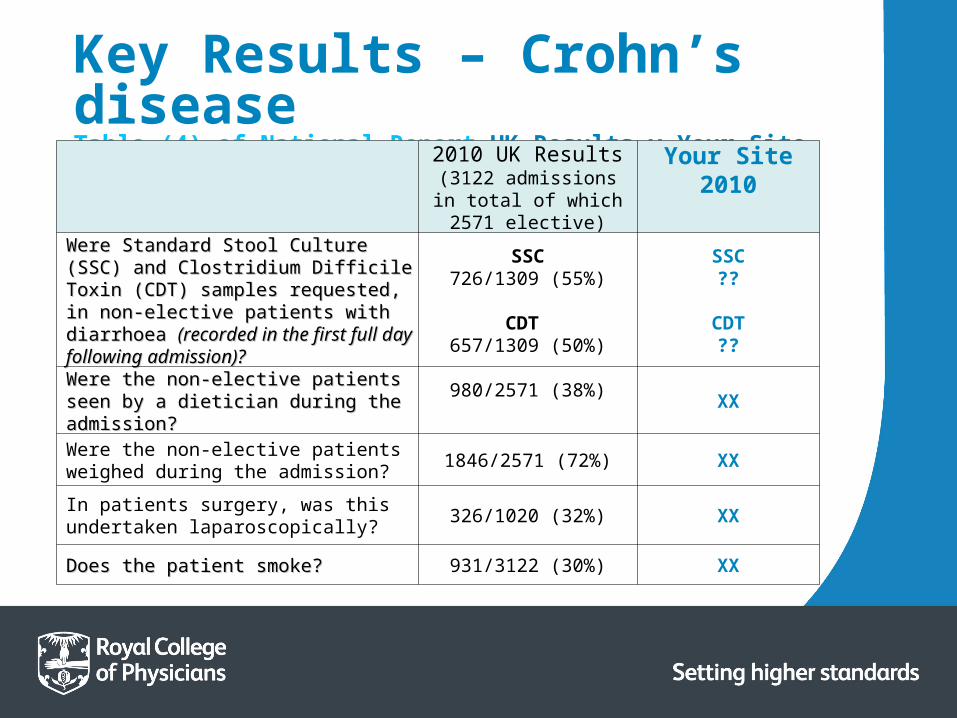
Key Results – Crohn’s diseaseTable (4) of National Report UK Results v Your Site 2010
2010 UK Results(3122 admissions in total of which 2571 elective)
Your Site 2010
Were Standard Stool Culture (SSC) and Were Standard Stool Culture (SSC) and Clostridium Difficile Toxin (CDT) samples Clostridium Difficile Toxin (CDT) samples requested, in non-elective patients with requested, in non-elective patients with diarrhoea diarrhoea (recorded in the first full day (recorded in the first full day following admission)?following admission)?
SSC726/1309 (55%)
CDT 657/1309 (50%)
SSC??
CDT??
Were the non-elective patients seen by a Were the non-elective patients seen by a dietician during the admission?dietician during the admission?
980/2571 (38%) XX
Were the non-elective patients weighed during the admission? 1846/2571 (72%) XX
In patients surgery, was this undertaken laparoscopically? 326/1020 (32%) XX
Does the patient smoke?Does the patient smoke? 931/3122 (30%) XX
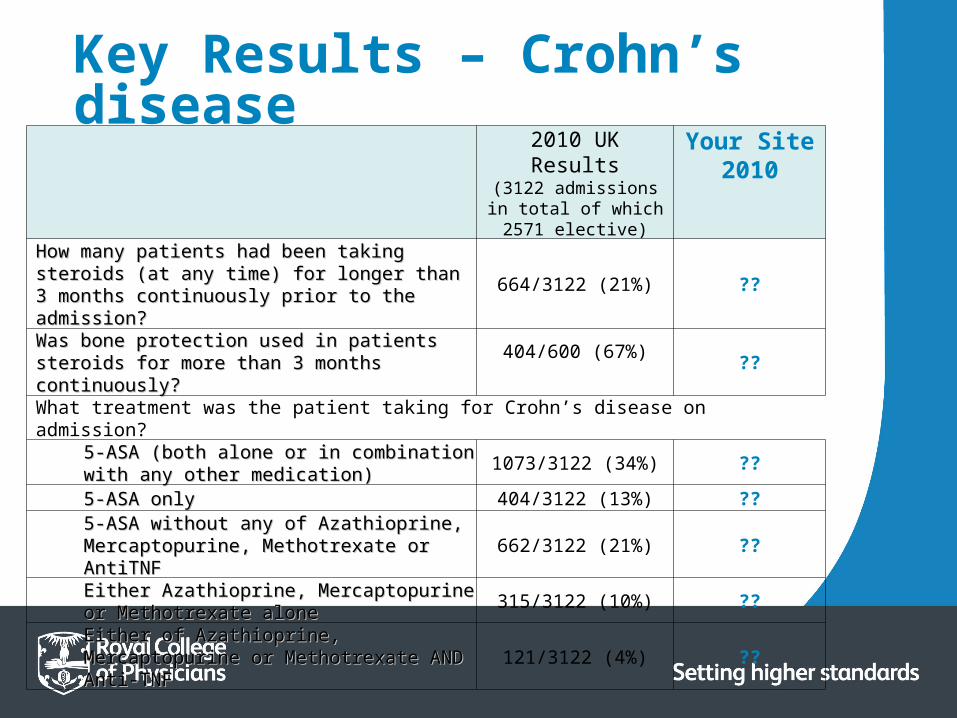
Key Results – Crohn’s diseaseTable (4) of National Report UK Results v Your Site 2010
2010 UK Results(3122 admissions in total of which 2571 elective)
Your Site 2010
How many patients had been taking steroids (at any time) How many patients had been taking steroids (at any time) for longer than 3 months continuously prior to the for longer than 3 months continuously prior to the admission? admission?
664/3122 (21%) ??
Was bone protection used in patients steroids for more Was bone protection used in patients steroids for more than 3 months continuously?than 3 months continuously?
404/600 (67%) ??
What treatment was the patient taking for Crohn’s disease on admission?
5-ASA (both alone or in combination with any other 5-ASA (both alone or in combination with any other medication)medication) 1073/3122 (34%) ??
5-ASA only 5-ASA only 404/3122 (13%) ??
5-ASA without any of Azathioprine, 5-ASA without any of Azathioprine, Mercaptopurine, Methotrexate or AntiTNFMercaptopurine, Methotrexate or AntiTNF 662/3122 (21%) ??
Either Azathioprine, Mercaptopurine or Either Azathioprine, Mercaptopurine or Methotrexate aloneMethotrexate alone 315/3122 (10%) ??
Either of Azathioprine, Mercaptopurine or Either of Azathioprine, Mercaptopurine or Methotrexate AND Anti-TNF Methotrexate AND Anti-TNF 121/3122 (4%) ??

Key Findings – Crohn’s diseaseCrohn’s Disease – findings relate to key results indicated in Table(4): Adult IBD Care – Crohn’s Disease. UK Results v Your Site 2010 (page 10)
Key Findings – Crohn’s disease: 1. Use of Anti-TNF therapy for patients admitted with CD has doubled over 3 rounds but use
remains at a relatively low level overall
2. For CD there has not been the same increase as observed for UC in the rates of stool samples sent for Standard Stool cultures and Clostridium Difficile Toxin in patients admitted with diarrhoea
3. 13% of patients were taking 5-ASA drugs as the sole medication for their CD on admission. A further 21.2% were taking 5-ASA drugs with other medication but not in conjunction with any of Azathioprine, Mercaptopurine, Methotrexate or Anti-TNF therapy
4. 63.3% of patients were not taking any of Azathioprine, Mercaptopurine, Methotrexate or Anti-TNF therapy on admission
5. Significantly more patients were weighed during their admission
6. The number of patients seen by a dietician during their admission has continued to rise across rounds but remains at a low level overall
7. Just under a third of patients with CD admitted to hospital are smokers. This has not changed over the 3 rounds of the IBD audit

Recommendations for Adult IBD Care - IBD Services based on findings collated for Ulcerative Colitis & Crohn’s Disease as detailed in tables (3) & (4) of National Report
(page 11)
Key Recommendations
All IBD patients with diarrhoea should have stools sampled for both SSC and CDT testing
All appropriate IBD patients should be given heparin to reduce the risk of thromboembolism
Clinicians should consider the use of rescue medical therapy for patients that do not respond to IV steroids
Where IBD services have a IBD nurse specialist provision, the nurse should always be made aware of any IBD inpatient that is planned to commence Anti-TNF treatment to ensure appropriate counselling and screening is undertaken prior to the infusion
Bone protection should be prescribed to all patients who receive corticosteroids
Further long term data is needed on the safety, efficacy and appropriateness of use of Anti-TNF drugs. IBD Services are encouraged to participate in the ongoing Biologics audit element of the UK IBD audit
IBD Services are to review the maintenance strategies for CD
Key Recommendations:
Use of immunomodulators and biological therapies, in keeping with the 2011 BSG Guidelines for the management of inflammatory bowel disease in adults, will help to reduce long-term steroid use and the need for admission
A dietician should see all CD inpatients and a multidisciplinary nutrition support team must be available to IBD Services to offer advice on those patients who may require more complex enteral and/or parenteral nutritional support
Smoking cessation is an important factor in maintaining remission and in reducing the risk of relapse in CD. IBD Services should do more to encourage patients with CD to engage with formal smoking cessation services
Key Recommendations continued:
Key Indicator Data• The table in section 5 (page 35) of the report gives named data in
alphabetical order of participating site (divided by health board / SHA)
• These data items were agreed by the UK IBD Audit Steering Group as reflecting the questions of particular importance to IBD patients
• The combined data from all 198 sites are shown for comparison
• These results should be interpreted within the context of the fact that many sites entered a relatively small number of cases to the audit and therefore percentages should be reviewed alongside the actual number of cases submitted

Key Indicators
How many cases were entered to the UK IBD Audit?
Was the patient seen by a gastroenterologist during their admission? (this does not apply to patients who were admitted for either elective surgery or who were under the direct care of a surgeon)
In patient with diarrhoea, was stool sample sent for Standard Stool Culture (SSC)? (SSC is a test to identify bacteria or viruses that may be causing an infection)
Was prophylactic Heparin prescribed? (this medication is used to prevent and treat blood clots)
Ulcerative Colitis
Crohn’s Disease
Ulcerative Colitis
Crohn’s Disease
Ulcerative Colitis
Crohn’s Disease
Ulcerative Colitis
Crohn’s Disease
UK Results 2010
Median = 18
Median = 20
Yes = 2258 (88%)
Yes = 1994 (79%)
Yes = 1537 (79%)
Yes = 726
(55%)
Yes = 2268 (88%)
Yes = 2708 (87%)
Your Site Results ?? ?? ?? ?? ?? ?? ?? ??
Key Indicator Data
Key Indicators
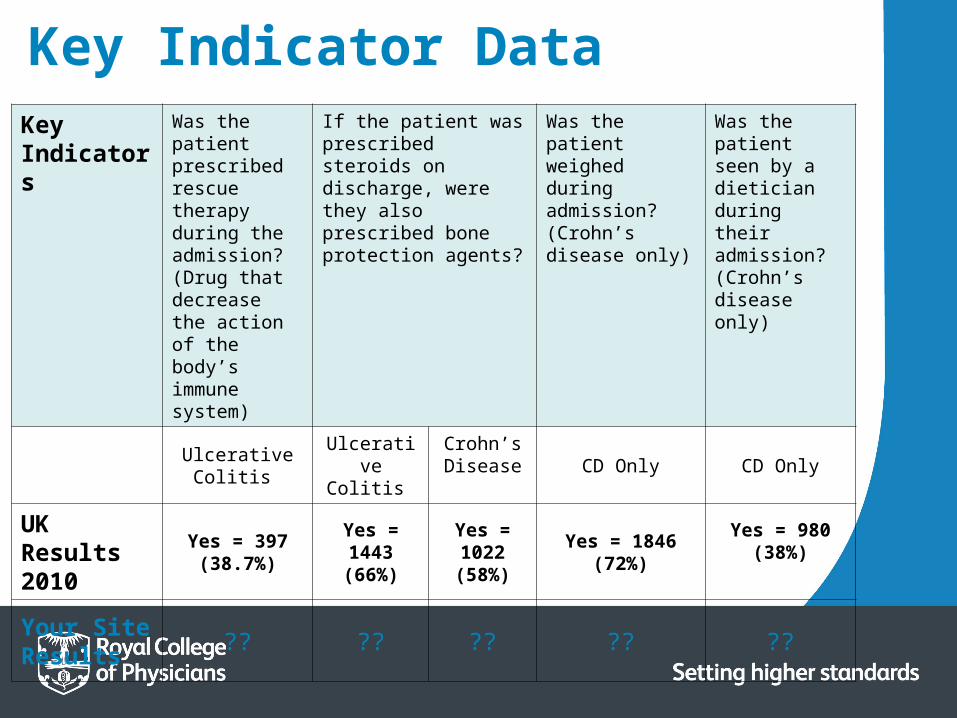
Was the patient prescribed rescue therapy during the admission? (Drug that decrease the action of the body’s immune system)
If the patient was prescribed steroids on discharge, were they also prescribed bone protection agents?
Was the patient weighed during admission? (Crohn’s disease only)
Was the patient seen by a dietician during their admission? (Crohn’s disease only)
Ulcerative Colitis Ulcerative Colitis
Crohn’s Disease CD Only CD Only
UK Results 2010
Yes = 397 (38.7%)
Yes = 1443 (66%)
Yes = 1022 (58%)
Yes = 1846(72%)
Yes = 980 (38%)
Your Site Results ?? ?? ?? ?? ??
Key Indicator Data
Summary of National ResultsThese results highlight:
• Clear evidence of sustained improvements in quality of care for IBD patients • Substantial continued improvement seen particularly for patients admitted with UC –
mortality rates halved over 3 rounds of the audit • Readmission rates lowered • Percentage of patients seen by an IBD nurse specialist during admission doubled since first
round • Collection of stool samples for SSC and CDT continued to improve – halving of positive CDT
samples noted • Prescription of prophylactic Heparin continued to rise• Numerical but not statistically significant reduction in mortality for patients admitted with
CD• Rate of operations undertaken laparoscopically increased significantly across rounds • Use of anti-TNF therapy for patients admitted with CD doubled since first round • 60% of patients with CD still not seen by a dietician during admission • Rates of collection of stool samples for SSC and CDT increased across rounds one and two
but fallen back in this round
UK IBD Audit continues to demonstrate significant changes in the delivery of IBD care over a relatively short time period but there remains more to be done.

Action Plan National Recommendation
Action Required Staff Responsible
Progress at Your Site
1. Sites should aim to continue to deliver high quality care for patients with UC and CD, including collecting stool specimens and giving Prophylactic Heparin to all appropriate inpatients
a) Submission of all relevant local cases to the UK IBD Audit
b) All IBD patients with diarrhoea should be considered for stool sample collection for SSC and CDT
c) All IBD patients should be prescribed Heparin, unless contraindicated
UK IBD Audit Clinical Lead
Consultant Gastroenterologists
Consultant Gastroenterologists
2. Sites should consider the value of rescue therapy for patients hat do not respond to intravenous steroids.
d) In patients with no/poor response to steroid treatment, Ciclosporin/Anti-TNF should be considered
Consultant Gastroenterologists

Action Plan National Recommendation
Action Required Staff Responsible
Progress at Your Site
3. Bone protection should be prescribed to all patients who receive corticosteroids
e) Local policy should dictate that bone protection agents are prescribed to all IBD patients started on steroid treatment
Consultant Gastroenterologists/Hospital Policy Managers
4. Sites should continue to ensure appropriate use of specialist ward areas
f) All IBD patients should be admitted directly to specialist gastroenterology wards
Bed Managers/Ward Staff
5. Further audit is needed on the use of Anti-TNF drugs and sites are encouraged to participate in the ongoing UK IBD Biologics Audit
g) Any site providing biological treatment (Infliximab or Adalimumab) to IBD patients, should be registered to participate in the UK IBD Biologics Audit (or a relevant alternative)
UK IBD Clinical Lead
Action Plan National Recommendation
Action Required Staff Responsible
Progress at Your Site
6. Sites are strongly encouraged to review the therapy received by all IBD patients. 5-ASA drugs may be stopped in many CD cases and the use of immunomodulators and biologics in keeping with national clinical guidance will help to reduce long-term steroid use and the need for admission
h) Local review of existing evidence should be undertaken to inform any continued use of 5-ASA drugs in CD patients
i) Any patient on long-term steroids (>3 months) should be under regular review
Consultant Gastroenterologists
Consultant Gastroenterologists

Action Plan
National Recommendation
Action Required Staff Responsible
Progress at Your Site
7. Sites should continue to focus on the nutritional needs of patients with CD ensuring they have appropriate dietetic support
j) All CD inpatients should have their weight regularly monitored (weekly/daily?)
k) Business cases should put forward to promote the need for further dietetic support for IBD patients
Nursing Staff/Healthcare Assistants
Consultant Gastroenterologists
8. Patients with CD who smoke should be encouraged to engage with formal smoking cessation services
l) Leaflets promoting local smoking cessation services should be handed to all CD inpatients that smoke
All members of the IBD Team
Your 3 key areas for local change:
Local key area identified
What action needs to occur to facilitate this change?
Who will be responsible?
How and when will you review this action?
1.
2.
3.

The Future: • Data entry for the biologics audit element of the round 3 UK
IBD Audit continues. An interim report will be published in June 2012
• Enter data for your IBD patients receiving biological therapy at: www.ibdbiologicsaudit.org
• Sites are encouraged to access and contribute towards the Shared Document Store on the IBD Quality Improvement Project (IBDQIP) website: www.ibdqip.co.uk which provides tools that sites can use to implement change within their own IBD Service.

Acknowledgements
• Most importantly thank you to all of the people who worked within ‘Your Site’ towards collating and entering the data
• All members of the UK IBD Audit Steering Group
For further information contact: