
Uintah SD Template Pages - Uintah School District
72
Employee Benefits Guide 2020 2021
Transcript of Uintah SD Template Pages - Uintah School District
EmployeeBenefits Guide
20202021
This communication highlights some of your benefit plans. Your actual rights and benefits are governed by the official plan documents. If any discrepancy exists between this communication and the official plan documents,
the plan documents will prevail. We reserve the right to change any benefit plan without notice. Benefits are not a guarantee of employment.
If you have questions regarding… Call Click
General Benefits InformationKelli Wilson, Benefit Coordinator
(435-781-3100 x 1026
MedicalPEHP
(800) 765-7347(801) 366-7555
www.pehp.org
Health Savings AccountAxisPlus
(877) 872-2125 www.myaxisplus.com
DentalTDA Dental
(800) 880-3536(801) 268-9740
www.tdadental.com
VisionOpticare of Utah
(800) 363-0950(801) 869-2020
www.opticareofutah.com
Life and AD&DLincoln Financial
(800) 423-2765 www.lfg.com
DisabilityLincoln Financial
(800) 423-2765 www.lfg.com
Employee Assistance ProgramLincoln Financial –EmployeeConnect
(888) 682-4824www.guidanceresources.com
Username: LFGsupportPassword: LFGsupport1
Voluntary BenefitsLacey Smith, GBS Benefits, Inc.
(801) 819-7744 [email protected]
2020-2021 Employee Benefits Guide

Table of Contents
What’s InsideThis guide provides information for consideration when newly enrolling, changing your elections, or reenrolling in our benefit programs.
4 Important Information
8 Online EnrollmentInfinityHR
9 MedicalPEHP
25 Health Savings AccountAxisPlus
28 DentalTDA Dental
31 VisionOpticare of Utah
33 Flexible Spending AccountAxisPlus
41 Life and AD&DLincoln Financial
48 DisabilityLincoln Financial
50 VoluntaryAllstate
63 Employee Assistance ProgramEmployeeConnect by Lincoln Financial
66 Premiums
Important InformationUintah School District
4

WelcomeWe are committed to providing our employees with quality benefit programs that arecomprehensive, flexible and affordable. Giving our employees the best in benefit plans is one waywe can show you that as an employee, YOU are our most important asset. Eligible employees havemany benefit plans to choose from, so we ask that you read this benefits guide carefully to helpyou make the benefit elections that are the best fit for you and your family.
Know Your BenefitsMaking wise decisions about your benefits requires planning. By selecting benefits that providethe best care and coverage, you can optimize their value and minimize the impact to your budget.The best thing you can do is “shop” for benefits carefully, using the same type of decision-making process you use for other major purchases.
› Take Advantage Of The Tools AvailableThat includes this guide, access to plan information, provider directories, and enrollmentmaterials.
› Be a Smart ShopperIf you were buying a car or purchasing a home, you would do a lot of research beforehand. Youshould do the same for benefits.
› Don’t Miss the Deadline and Keep Record of Your EnrollmentPay attention to the enrollment deadline and be sure to provide us with your benefit electionsin a timely manner. It is important to review your paycheck to ensure the accuracy of payrolldeductions. Notify us immediately if there are any discrepancies. Remember: Once theenrollment period has ended, you may not make or change your benefit elections, unless youexperience a qualified life event.
Summary of Benefits and Coverage (SBC) and Uniform GlossaryIn addition to the plan information in this Benefits Guide, you can also review a Summary ofBenefits and Coverage for each medical plan. This requirement of the ACA standardizes healthplan information so that you can better understand and compare plan features. We willautomatically provide you a copy of the SBC annually during open enrollment.
For the most up-to-date information regarding the ACA, please visit www.healthcare.gov.
Uintah School District’s Benefits and You
5
Enrollment & Eligibility
Who is Eligible?If you are hired as a full-time employee working 30 or more hours per week, coverage will begin onthe first day of the month following the date of qualified employment. You may also enroll youreligible dependents in the same plans you choose for yourself.
Eligible dependents include your legal spouse and your natural, adopted or step-child(ren). Thedependent age limit for children on your medical plan is age 26, but may vary for other benefitsoffered.
When to EnrollYou can enroll for coverage as a new hire, or during our annual open enrollment period. Outside ofthe annual open enrollment period, the only time you can change your coverage is if youexperience a qualifying life event.
How to Make ChangesOnce you enroll in or decline benefits, you will not be able to make any changes to your electionsuntil our next annual open enrollment period, unless you experience a qualified life event.Qualified life events include, but are not limited to:
› Change in your legal marital status› Birth, adoption, placement for adoption or legal guardianship of a child› Death of a dependent› Change in child’s dependent status› You or your dependent(s) become eligible or lose eligibility for Medicaid or the Children’s
Health Insurance Program (CHIP)› Change in your dependent’s employment resulting in loss or gain of eligibility for employer
coverage› A court or administrative order
If your qualified life event is due to loss or gain of Medicaid or CHIP coverage, you have 60 days tocomplete the necessary enrollment forms and return them to us. All other qualified life eventsmust be reported to us within 30 days of the event. It is your responsibility to notify us when youhave a qualified life event and would like to make changes to your benefit elections. Please do notmiss this important deadline!
When Coverage EndsFor most benefits, coverage will end on the last day of the month in which your regular workschedule is reduced to fewer than 30 hours per week, your employment ends, or you stop payingyour share of the coverage. Your dependent(s) coverage ends when your coverage ends, or thelast day of the month in which the dependent is no longer eligible. Certain benefits mayterminate on the date of event.
6
Stretching Your Rx Dollar
GoodRx Comparison ToolStop paying too much for your prescriptions! With the GoodRx Comparison Tool, you cancompare drug prices at over 70,000 pharmacies, and discover free coupons and savings tips.
Isn’t health insurance all I need?Your health insurance provides valuable prescription and other health benefits, but a smartconsumer can save much more, especially for drugs that are not covered by health insurance(weight-loss medications, some antihistamines, etc.), drugs that have limited quantities, drugsthat can be found for less than your copay, or drugs with a lower priced generic.
How can I find these savings?The GoodRx Comparison Tool provides you with instant access to current prices on more than6,000 drugs at virtually every pharmacy in America.
› On the Web: https://www.goodrx.com/Instantly look up current drug prices at CVS, Walgreens, Walmart, Costco, and other localpharmacies.Please Note:
• Prescription drug pricing displayed on the GoodRx Comparison Tool may be more or less thanyour insurance drug card.
• Please be sure to compare all discount pricing options before you purchase.• Check your insurance carrier’s pharmacy benefit before purchasing a 90 day supply.
› On Your PhoneAvailable on the app store or with Android on Google play. Or, just go to m.goodrx.com fromany mobile phone.
Generic Prescriptions$4 30-Day Supply or a $10 90-Day SupplyThese programs may assist you in paying a reduced amount for generic medications, as well as,reducing utilization of the medical prescription benefits.
Did You Know?Even if the generic substitute for one of your prescription drugs is not on one of the $4 lists,generic drugs are often 80% less expensive than brand name drugs, so switching to a generic willhave a large impact on your pocketbook whether you switch pharmacies or not. To see if youwould benefit from a switch to a generic drug, do some comparison shopping. One of the betterplaces to do this is at www.crbestbuydrugs.org, a Consumer Reports site.
Tips• When you receive a prescription from your doctor, ask if a generic equivalent is available.• The member must present the written prescription to the pharmacist and request the $4-
Generic price.• The member should not present the medical ID card. The pharmacy will not submit a claim to
the insurance carrier.
How can I find out if my prescription is on the $4-Generic Drug List?Most of the generic programs offer approximately 150 to 300 generic drugs at a discounted price.The generic drugs offered cover most diseases and most chronic conditions such as arthritis,heart disease, high blood pressure, depression and diabetes.You may search for the generic medication on the pharmacy’s website or contact the pharmacy toinquire if the generic medication the provider prescribed is on the pharmacy’s $4-Generic DrugList.
7
InfinityHREnrolling for benefits online is easy! Follow the steps below to elect or waive coveragefor the current plan year.
Information NeededIf you’re adding a dependent(s), you will need the following:
• Name• Social Security Number• Date of Birth• Home Address (if different from yours)
Step 1: Getting Started• In your web browser type www.infinityhr.com in the address bar.• If you are a first time user or have forgotten your password, click “First time user” or “Reset
ID and Password”• Validate your identity by entering your Date of Birth and SSN then click “Find my Record”.• Enter a new password and make note of it for your records, then click create new password.• Enter your User ID and Password then click log in.
o Your User ID is: [first letter of first name][lastname][last 4 digits of SSN]o For Example: Name: John Doe, SSN: xxx-xx-5555, User ID = jdoe5555
• On the home screen look for Change Events.• Select the event available, which should be “Open Enrollment” , then click “Begin Event”.
o If enrolling outside of Open Enrollment, select the options that are appropriate suchas, New Hire or Marriage.
Step 2: Verify Your Personal and Dependent Information• Verify your Personal Information.• If you need to add or make a change click on “Edit Personal Information” and make updates,
then click “Save Information”.• Once you have verified everything is correct click “Save & Continue”.• If you need to add a dependent click “Add Dependent” or if you need to change a
dependent’s information click “Edit” then add/update the information and click “SaveInformation”.
• Once all of your dependents have been added/updated, click “Save & Continue”.o If your spouse will be enrolled in coverage they are considered a dependent for
insurance purposes.o Please Note: If you plan on enrolling in Spouse Life Insurance or Child Life Insurance,
you need to add your spouse and children as dependents on this screen.
Step 3: Make Your Open Enrollment Elections• Follow the enrollment wizard through each step of the enrollment process and elect or
decline each benefit.o Please Note: As you elect plans, your dependents will appear at the bottom of the
screen. Please remove the check mark from the box if you do not want a dependentcovered on that specific plan.
• Click “Save & Continue” to continue navigating through the system.
Step 4: Confirm Your Elections• After you have made all of your elections you will be at the Review Tab.• Review the benefit elections for yourself and your dependents to ensure accuracy.• Click “Save & Confirm”.• The Enrollment Confirmation Statement will be available on your home screen.8
MedicalPEHP
9
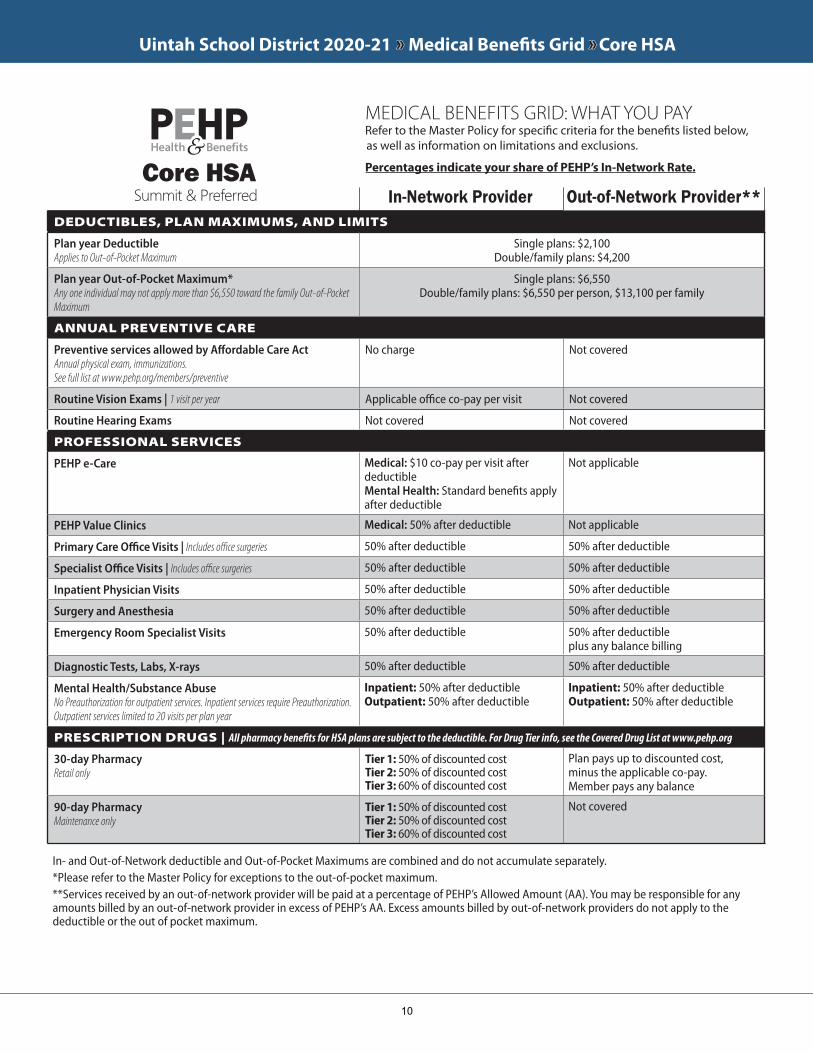
Uintah School District 2020-21 »» Medical Benefits Grid »» Core HSA
DEDUCTIBLES, PLAN MAXIMUMS, AND LIMITS
Plan year Deductible Applies to Out-of-Pocket Maximum
Single plans: $2,100Double/family plans: $4,200
Plan year Out-of-Pocket Maximum* Any one individual may not apply more than $6,550 toward the family Out-of-Pocket Maximum
Single plans: $6,550Double/family plans: $6,550 per person, $13,100 per family
ANNUAL PREVENTIVE CARE
Preventive services allowed by Affordable Care ActAnnual physical exam, immunizations.See full list at www.pehp.org/members/preventive
No charge Not covered
Routine Vision Exams | 1 visit per year Applicable office co-pay per visit Not covered
Routine Hearing Exams Not covered Not covered
PROFESSIONAL SERVICES
PEHP e-Care Medical: $10 co-pay per visit after deductibleMental Health: Standard benefits apply after deductible
Not applicable
PEHP Value Clinics Medical: 50% after deductible Not applicable
Primary Care Office Visits | Includes office surgeries 50% after deductible 50% after deductible
Specialist Office Visits | Includes office surgeries 50% after deductible 50% after deductible
Inpatient Physician Visits 50% after deductible 50% after deductible
Surgery and Anesthesia 50% after deductible 50% after deductible
Emergency Room Specialist Visits 50% after deductible 50% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 50% after deductible 50% after deductible
Mental Health/Substance Abuse No Preauthorization for outpatient services. Inpatient services require Preauthorization.Outpatient services limited to 20 visits per plan year
Inpatient: 50% after deductible Outpatient: 50% after deductible
Inpatient: 50% after deductible Outpatient: 50% after deductible
PRESCRIPTION DRUGS | All pharmacy benefits for HSA plans are subject to the deductible. For Drug Tier info, see the Covered Drug List at www.pehp.org
30-day Pharmacy Retail only
Tier 1: 50% of discounted costTier 2: 50% of discounted costTier 3: 60% of discounted cost
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
90-day Pharmacy Maintenance only
Tier 1: 50% of discounted costTier 2: 50% of discounted costTier 3: 60% of discounted cost
Not covered
Summit & PreferredCore HSA
In-Network Provider Out-of-Network Provider**
In- and Out-of-Network deductible and Out-of-Pocket Maximums are combined and do not accumulate separately.*Please refer to the Master Policy for exceptions to the out-of-pocket maximum.**Services received by an out-of-network provider will be paid at a percentage of PEHP’s Allowed Amount (AA). You may be responsible for any amounts billed by an out-of-network provider in excess of PEHP’s AA. Excess amounts billed by out-of-network providers do not apply to the deductible or the out of pocket maximum.
MEDICAL BENEFITS GRID: WHAT YOU PAY Refer to the Master Policy for specific criteria for the benefits listed below, as well as information on limitations and exclusions.
Percentages indicate your share of PEHP’s In-Network Rate.
10
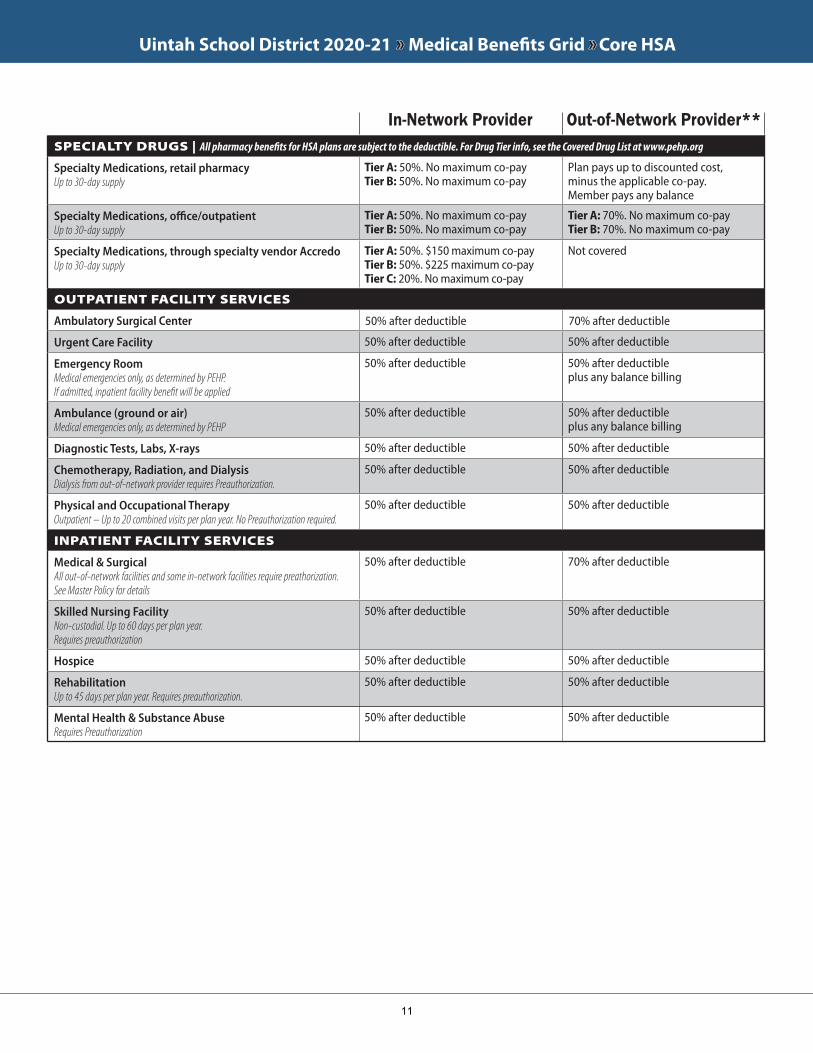
Uintah School District 2020-21 »» Medical Benefits Grid »» Core HSA
SPECIALTY DRUGS | All pharmacy benefits for HSA plans are subject to the deductible. For Drug Tier info, see the Covered Drug List at www.pehp.org
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 50%. No maximum co-payTier B: 50%. No maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 50%. No maximum co-payTier B: 50%. No maximum co-pay
Tier A: 70%. No maximum co-payTier B: 70%. No maximum co-pay
Specialty Medications, through specialty vendor AccredoUp to 30-day supply
Tier A: 50%. $150 maximum co-payTier B: 50%. $225 maximum co-payTier C: 20%. No maximum co-pay
Not covered
OUTPATIENT FACILITY SERVICES
Ambulatory Surgical Center 50% after deductible 70% after deductible
Urgent Care Facility 50% after deductible 50% after deductible
Emergency Room Medical emergencies only, as determined by PEHP.If admitted, inpatient facility benefit will be applied
50% after deductible 50% after deductible plus any balance billing
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
50% after deductible 50% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 50% after deductible 50% after deductible
Chemotherapy, Radiation, and Dialysis Dialysis from out-of-network provider requires Preauthorization.
50% after deductible 50% after deductible
Physical and Occupational Therapy Outpatient – Up to 20 combined visits per plan year. No Preauthorization required.
50% after deductible 50% after deductible
INPATIENT FACILITY SERVICES
Medical & SurgicalAll out-of-network facilities and some in-network facilities require preathorization. See Master Policy for details
50% after deductible 70% after deductible
Skilled Nursing FacilityNon-custodial. Up to 60 days per plan year. Requires preauthorization
50% after deductible 50% after deductible
Hospice 50% after deductible 50% after deductible
RehabilitationUp to 45 days per plan year. Requires preauthorization.
50% after deductible 50% after deductible
Mental Health & Substance AbuseRequires Preauthorization
50% after deductible 50% after deductible
In-Network Provider Out-of-Network Provider**
11
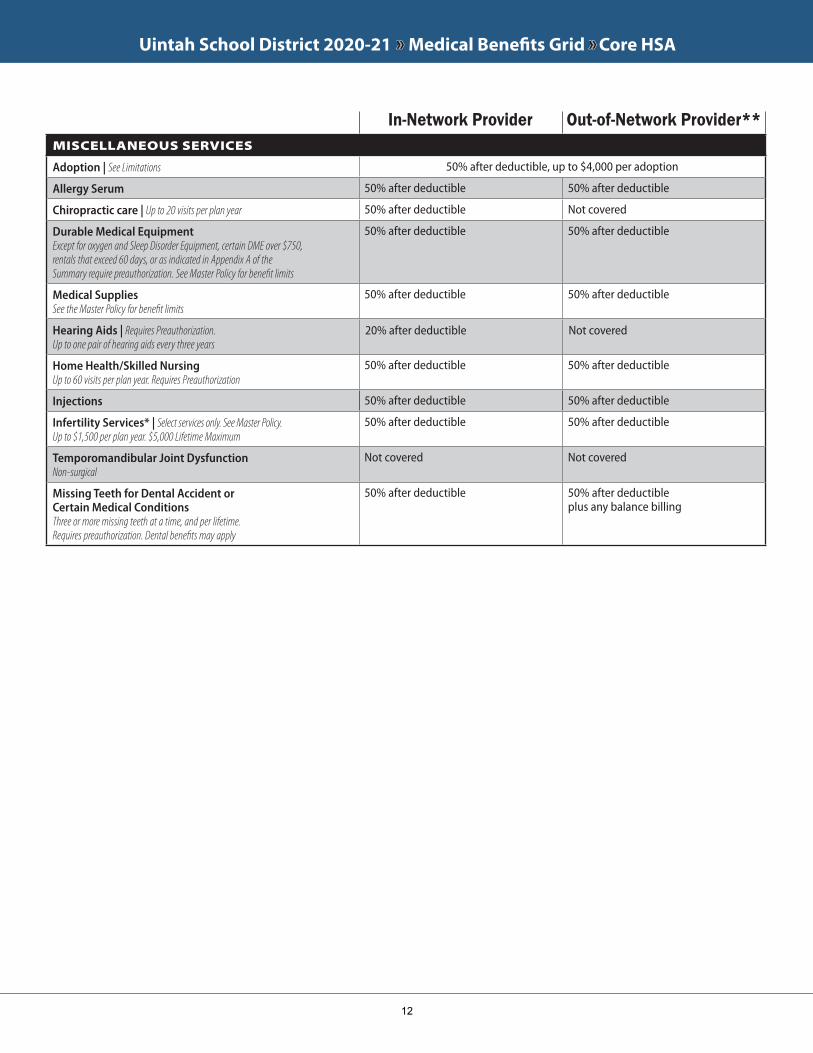
Uintah School District 2020-21 »» Medical Benefits Grid »» Core HSA
MISCELLANEOUS SERVICES
Adoption | See Limitations 50% after deductible, up to $4,000 per adoption
Allergy Serum 50% after deductible 50% after deductible
Chiropractic care | Up to 20 visits per plan year 50% after deductible Not covered
Durable Medical Equipment Except for oxygen and Sleep Disorder Equipment, certain DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Summary require preauthorization. See Master Policy for benefit limits
50% after deductible 50% after deductible
Medical SuppliesSee the Master Policy for benefit limits
50% after deductible 50% after deductible
Hearing Aids | Requires Preauthorization. Up to one pair of hearing aids every three years
20% after deductible Not covered
Home Health/Skilled Nursing Up to 60 visits per plan year. Requires Preauthorization
50% after deductible 50% after deductible
Injections 50% after deductible 50% after deductible
Infertility Services* | Select services only. See Master Policy. Up to $1,500 per plan year. $5,000 Lifetime Maximum
50% after deductible 50% after deductible
Temporomandibular Joint DysfunctionNon-surgical
Not covered Not covered
Missing Teeth for Dental Accident or Certain Medical ConditionsThree or more missing teeth at a time, and per lifetime.Requires preauthorization. Dental benefits may apply
50% after deductible 50% after deductible plus any balance billing
In-Network Provider Out-of-Network Provider**
12
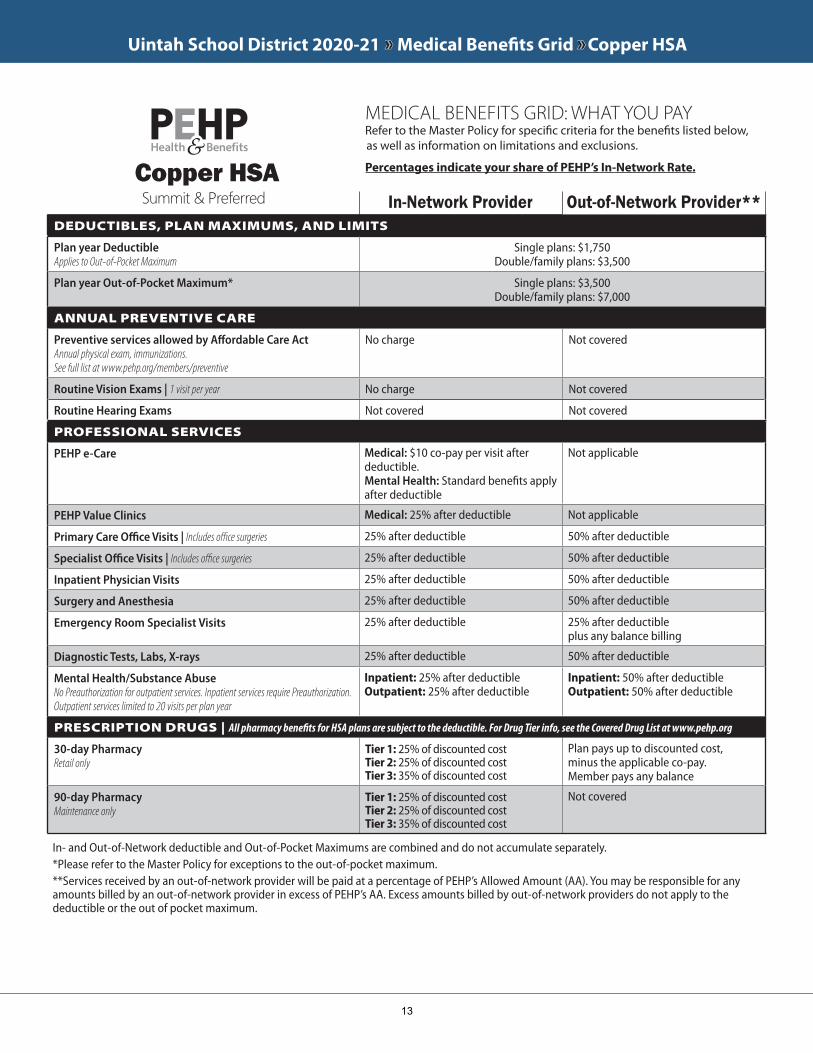
Uintah School District 2020-21 »» Medical Benefits Grid »» Copper HSA
DEDUCTIBLES, PLAN MAXIMUMS, AND LIMITS
Plan year Deductible Applies to Out-of-Pocket Maximum
Single plans: $1,750Double/family plans: $3,500
Plan year Out-of-Pocket Maximum* Single plans: $3,500Double/family plans: $7,000
ANNUAL PREVENTIVE CARE
Preventive services allowed by Affordable Care ActAnnual physical exam, immunizations.See full list at www.pehp.org/members/preventive
No charge Not covered
Routine Vision Exams | 1 visit per year No charge Not covered
Routine Hearing Exams Not covered Not covered
PROFESSIONAL SERVICES
PEHP e-Care Medical: $10 co-pay per visit after deductible.Mental Health: Standard benefits apply after deductible
Not applicable
PEHP Value Clinics Medical: 25% after deductible Not applicable
Primary Care Office Visits | Includes office surgeries 25% after deductible 50% after deductible
Specialist Office Visits | Includes office surgeries 25% after deductible 50% after deductible
Inpatient Physician Visits 25% after deductible 50% after deductible
Surgery and Anesthesia 25% after deductible 50% after deductible
Emergency Room Specialist Visits 25% after deductible 25% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 25% after deductible 50% after deductible
Mental Health/Substance Abuse No Preauthorization for outpatient services. Inpatient services require Preauthorization.Outpatient services limited to 20 visits per plan year
Inpatient: 25% after deductible Outpatient: 25% after deductible
Inpatient: 50% after deductible Outpatient: 50% after deductible
PRESCRIPTION DRUGS | All pharmacy benefits for HSA plans are subject to the deductible. For Drug Tier info, see the Covered Drug List at www.pehp.org
30-day Pharmacy Retail only
Tier 1: 25% of discounted costTier 2: 25% of discounted costTier 3: 35% of discounted cost
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
90-day Pharmacy Maintenance only
Tier 1: 25% of discounted costTier 2: 25% of discounted costTier 3: 35% of discounted cost
Not covered
Summit & PreferredCopper HSA
In-Network Provider Out-of-Network Provider**
In- and Out-of-Network deductible and Out-of-Pocket Maximums are combined and do not accumulate separately.*Please refer to the Master Policy for exceptions to the out-of-pocket maximum.**Services received by an out-of-network provider will be paid at a percentage of PEHP’s Allowed Amount (AA). You may be responsible for any amounts billed by an out-of-network provider in excess of PEHP’s AA. Excess amounts billed by out-of-network providers do not apply to the deductible or the out of pocket maximum.
MEDICAL BENEFITS GRID: WHAT YOU PAY Refer to the Master Policy for specific criteria for the benefits listed below, as well as information on limitations and exclusions.
Percentages indicate your share of PEHP’s In-Network Rate.
13
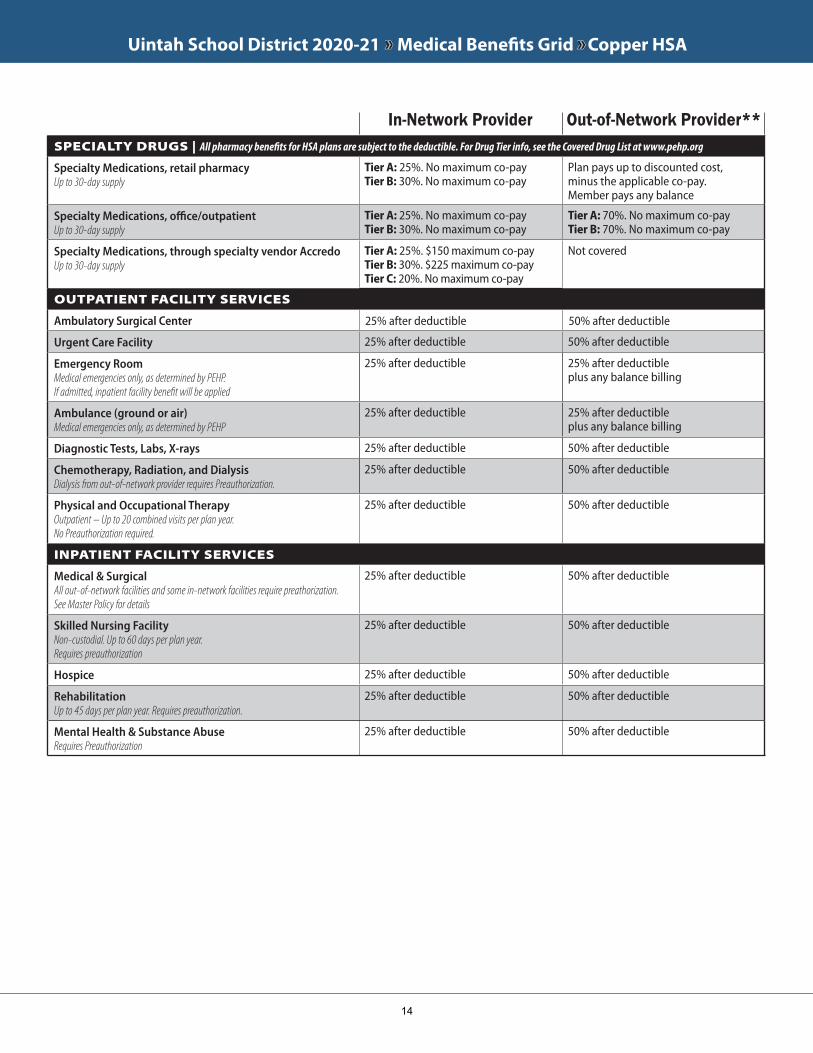
Uintah School District 2020-21 »» Medical Benefits Grid »» Copper HSA
SPECIALTY DRUGS | All pharmacy benefits for HSA plans are subject to the deductible. For Drug Tier info, see the Covered Drug List at www.pehp.org
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 25%. No maximum co-payTier B: 30%. No maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 25%. No maximum co-payTier B: 30%. No maximum co-pay
Tier A: 70%. No maximum co-payTier B: 70%. No maximum co-pay
Specialty Medications, through specialty vendor AccredoUp to 30-day supply
Tier A: 25%. $150 maximum co-payTier B: 30%. $225 maximum co-payTier C: 20%. No maximum co-pay
Not covered
OUTPATIENT FACILITY SERVICES
Ambulatory Surgical Center 25% after deductible 50% after deductible
Urgent Care Facility 25% after deductible 50% after deductible
Emergency Room Medical emergencies only, as determined by PEHP.If admitted, inpatient facility benefit will be applied
25% after deductible 25% after deductible plus any balance billing
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
25% after deductible 25% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 25% after deductible 50% after deductible
Chemotherapy, Radiation, and Dialysis Dialysis from out-of-network provider requires Preauthorization.
25% after deductible 50% after deductible
Physical and Occupational Therapy Outpatient – Up to 20 combined visits per plan year.No Preauthorization required.
25% after deductible 50% after deductible
INPATIENT FACILITY SERVICES
Medical & SurgicalAll out-of-network facilities and some in-network facilities require preathorization. See Master Policy for details
25% after deductible 50% after deductible
Skilled Nursing FacilityNon-custodial. Up to 60 days per plan year. Requires preauthorization
25% after deductible 50% after deductible
Hospice 25% after deductible 50% after deductible
RehabilitationUp to 45 days per plan year. Requires preauthorization.
25% after deductible 50% after deductible
Mental Health & Substance AbuseRequires Preauthorization
25% after deductible 50% after deductible
In-Network Provider Out-of-Network Provider**
14
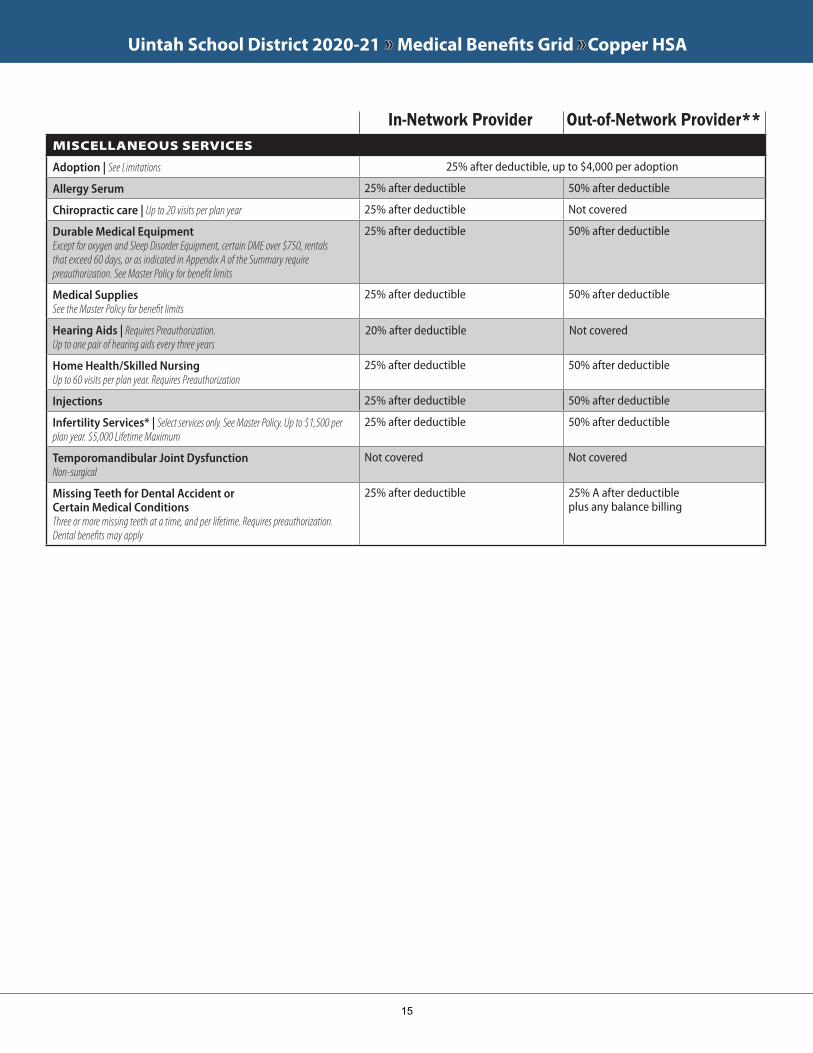
Uintah School District 2020-21 »» Medical Benefits Grid »» Copper HSA
MISCELLANEOUS SERVICES
Adoption | See Limitations 25% after deductible, up to $4,000 per adoption
Allergy Serum 25% after deductible 50% after deductible
Chiropractic care | Up to 20 visits per plan year 25% after deductible Not covered
Durable Medical Equipment Except for oxygen and Sleep Disorder Equipment, certain DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Summary require preauthorization. See Master Policy for benefit limits
25% after deductible 50% after deductible
Medical SuppliesSee the Master Policy for benefit limits
25% after deductible 50% after deductible
Hearing Aids | Requires Preauthorization. Up to one pair of hearing aids every three years
20% after deductible Not covered
Home Health/Skilled Nursing Up to 60 visits per plan year. Requires Preauthorization
25% after deductible 50% after deductible
Injections 25% after deductible 50% after deductible
Infertility Services* | Select services only. See Master Policy. Up to $1,500 per plan year. $5,000 Lifetime Maximum
25% after deductible 50% after deductible
Temporomandibular Joint DysfunctionNon-surgical
Not covered Not covered
Missing Teeth for Dental Accident or Certain Medical ConditionsThree or more missing teeth at a time, and per lifetime. Requires preauthorization. Dental benefits may apply
25% after deductible 25% A after deductible plus any balance billing
In-Network Provider Out-of-Network Provider**
15
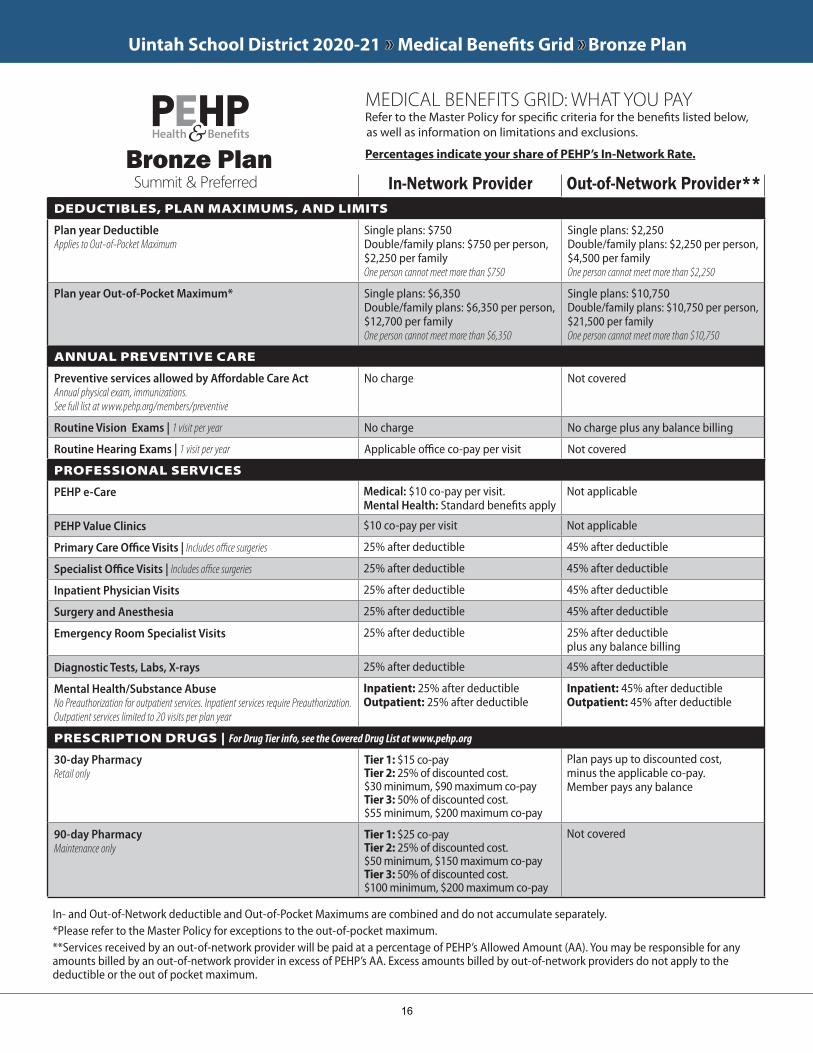
Uintah School District 2020-21 »» Medical Benefits Grid »» Bronze Plan
DEDUCTIBLES, PLAN MAXIMUMS, AND LIMITS
Plan year DeductibleApplies to Out-of-Pocket Maximum
Single plans: $750Double/family plans: $750 per person, $2,250 per familyOne person cannot meet more than $750
Single plans: $2,250Double/family plans: $2,250 per person, $4,500 per familyOne person cannot meet more than $2,250
Plan year Out-of-Pocket Maximum* Single plans: $6,350Double/family plans: $6,350 per person, $12,700 per family One person cannot meet more than $6,350
Single plans: $10,750Double/family plans: $10,750 per person, $21,500 per familyOne person cannot meet more than $10,750
ANNUAL PREVENTIVE CARE
Preventive services allowed by Affordable Care ActAnnual physical exam, immunizations.See full list at www.pehp.org/members/preventive
No charge Not covered
Routine Vision Exams | 1 visit per year No charge No charge plus any balance billing
Routine Hearing Exams | 1 visit per year Applicable office co-pay per visit Not covered
PROFESSIONAL SERVICES
PEHP e-Care Medical: $10 co-pay per visit.Mental Health: Standard benefits apply
Not applicable
PEHP Value Clinics $10 co-pay per visit Not applicable
Primary Care Office Visits | Includes office surgeries 25% after deductible 45% after deductible
Specialist Office Visits | Includes office surgeries 25% after deductible 45% after deductible
Inpatient Physician Visits 25% after deductible 45% after deductible
Surgery and Anesthesia 25% after deductible 45% after deductible
Emergency Room Specialist Visits 25% after deductible 25% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 25% after deductible 45% after deductible
Mental Health/Substance Abuse No Preauthorization for outpatient services. Inpatient services require Preauthorization.Outpatient services limited to 20 visits per plan year
Inpatient: 25% after deductible Outpatient: 25% after deductible
Inpatient: 45% after deductible Outpatient: 45% after deductible
PRESCRIPTION DRUGS | For Drug Tier info, see the Covered Drug List at www.pehp.org
30-day Pharmacy Retail only
Tier 1: $15 co-payTier 2: 25% of discounted cost. $30 minimum, $90 maximum co-payTier 3: 50% of discounted cost. $55 minimum, $200 maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
90-day Pharmacy Maintenance only
Tier 1: $25 co-payTier 2: 25% of discounted cost. $50 minimum, $150 maximum co-pay Tier 3: 50% of discounted cost. $100 minimum, $200 maximum co-pay
Not covered
MEDICAL BENEFITS GRID: WHAT YOU PAY Refer to the Master Policy for specific criteria for the benefits listed below, as well as information on limitations and exclusions.
Percentages indicate your share of PEHP’s In-Network Rate.
Summit & PreferredBronze Plan
In-Network Provider Out-of-Network Provider**
In- and Out-of-Network deductible and Out-of-Pocket Maximums are combined and do not accumulate separately.*Please refer to the Master Policy for exceptions to the out-of-pocket maximum.**Services received by an out-of-network provider will be paid at a percentage of PEHP’s Allowed Amount (AA). You may be responsible for any amounts billed by an out-of-network provider in excess of PEHP’s AA. Excess amounts billed by out-of-network providers do not apply to the deductible or the out of pocket maximum.
16
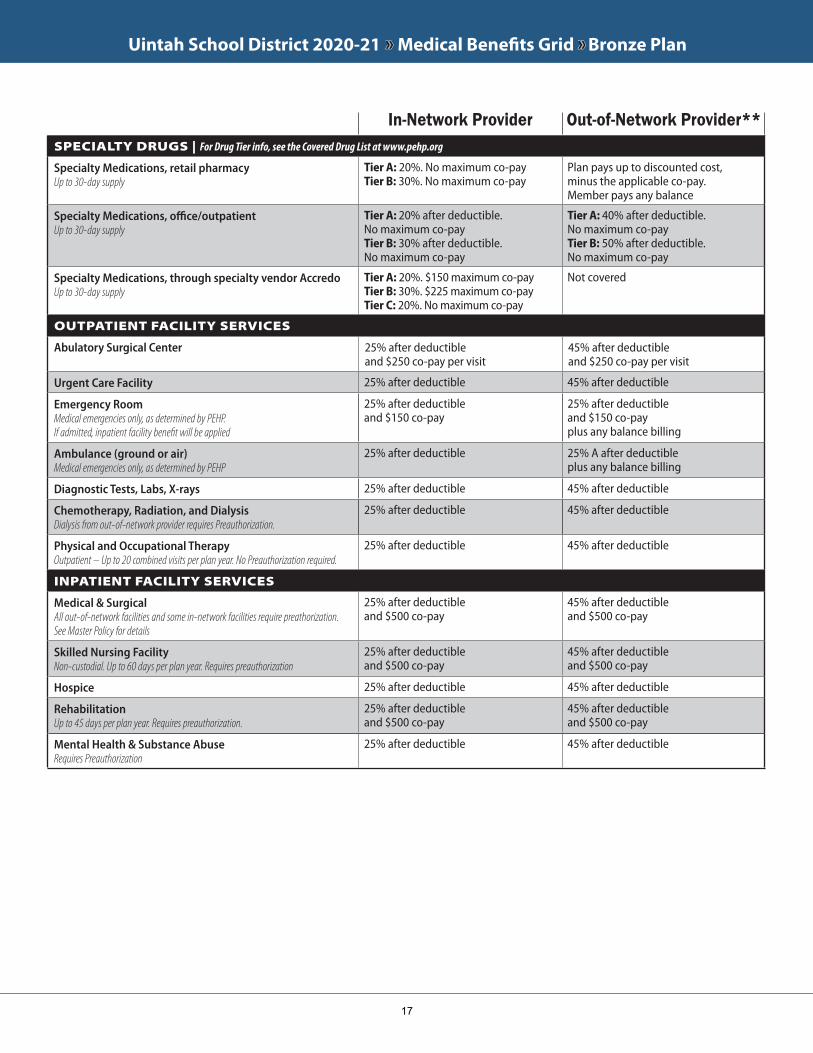
Uintah School District 2020-21 »» Medical Benefits Grid »» Bronze Plan
SPECIALTY DRUGS | For Drug Tier info, see the Covered Drug List at www.pehp.org
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 20%. No maximum co-payTier B: 30%. No maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 20% after deductible. No maximum co-payTier B: 30% after deductible. No maximum co-pay
Tier A: 40% after deductible. No maximum co-payTier B: 50% after deductible. No maximum co-pay
Specialty Medications, through specialty vendor AccredoUp to 30-day supply
Tier A: 20%. $150 maximum co-payTier B: 30%. $225 maximum co-payTier C: 20%. No maximum co-pay
Not covered
OUTPATIENT FACILITY SERVICES
Abulatory Surgical Center 25% after deductible and $250 co-pay per visit
45% after deductible and $250 co-pay per visit
Urgent Care Facility 25% after deductible 45% after deductible
Emergency Room Medical emergencies only, as determined by PEHP.If admitted, inpatient facility benefit will be applied
25% after deductible and $150 co-pay
25% after deductible and $150 co-pay plus any balance billing
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
25% after deductible 25% A after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 25% after deductible 45% after deductible
Chemotherapy, Radiation, and Dialysis Dialysis from out-of-network provider requires Preauthorization.
25% after deductible 45% after deductible
Physical and Occupational Therapy Outpatient – Up to 20 combined visits per plan year. No Preauthorization required.
25% after deductible 45% after deductible
INPATIENT FACILITY SERVICES
Medical & SurgicalAll out-of-network facilities and some in-network facilities require preathorization. See Master Policy for details
25% after deductible and $500 co-pay
45% after deductible and $500 co-pay
Skilled Nursing FacilityNon-custodial. Up to 60 days per plan year. Requires preauthorization
25% after deductible and $500 co-pay
45% after deductible and $500 co-pay
Hospice 25% after deductible 45% after deductible
RehabilitationUp to 45 days per plan year. Requires preauthorization.
25% after deductible and $500 co-pay
45% after deductible and $500 co-pay
Mental Health & Substance AbuseRequires Preauthorization
25% after deductible 45% after deductible
In-Network Provider Out-of-Network Provider**
17

Uintah School District 2020-21 »» Medical Benefits Grid »» Bronze Plan
MISCELLANEOUS SERVICES
After deductibleoption | See Limitations 25% after deductible, up to $4,000 per after deductibleoption
Allergy Serum 25% after deductible 45% after deductible
Chiropractic care | Up to 20 visits per plan year 25% after deductible Not covered
Durable Medical Equipment Except for oxygen and Sleep Disorder Equipment, certain DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Summary require preauthorization. See Master Policy for benefit limits
25% after deductible 45% after deductible
Medical SuppliesSee the Master Policy for benefit limits
25% after deductible 45% after deductible
Hearing Aids | Requires Preauthorization. Up to one pair of hearing aids every three years
25% after deductible Not covered
Home Health/Skilled Nursing Up to 60 visits per plan year. Requires Preauthorization
25% after deductible 45% after deductible
Injections 25% after deductible 45% after deductible
Infertility Services* | Select services only. See Master Policy. Up to $1,500 per plan year. $5,000 Lifetime Maximum
50% after deductible 50% after deductible
Temporomandibular Joint Dysfunction | Non-surgical Not covered Not covered
Missing Teeth for Dental Accident or Certain Medical ConditionsThree or more missing teeth at a time, and per lifetime. Requires preauthorization. Dental benefits may apply
25% after deductible 25% after deductible plus any balance billing
In-Network Provider Out-of-Network Provider**
18
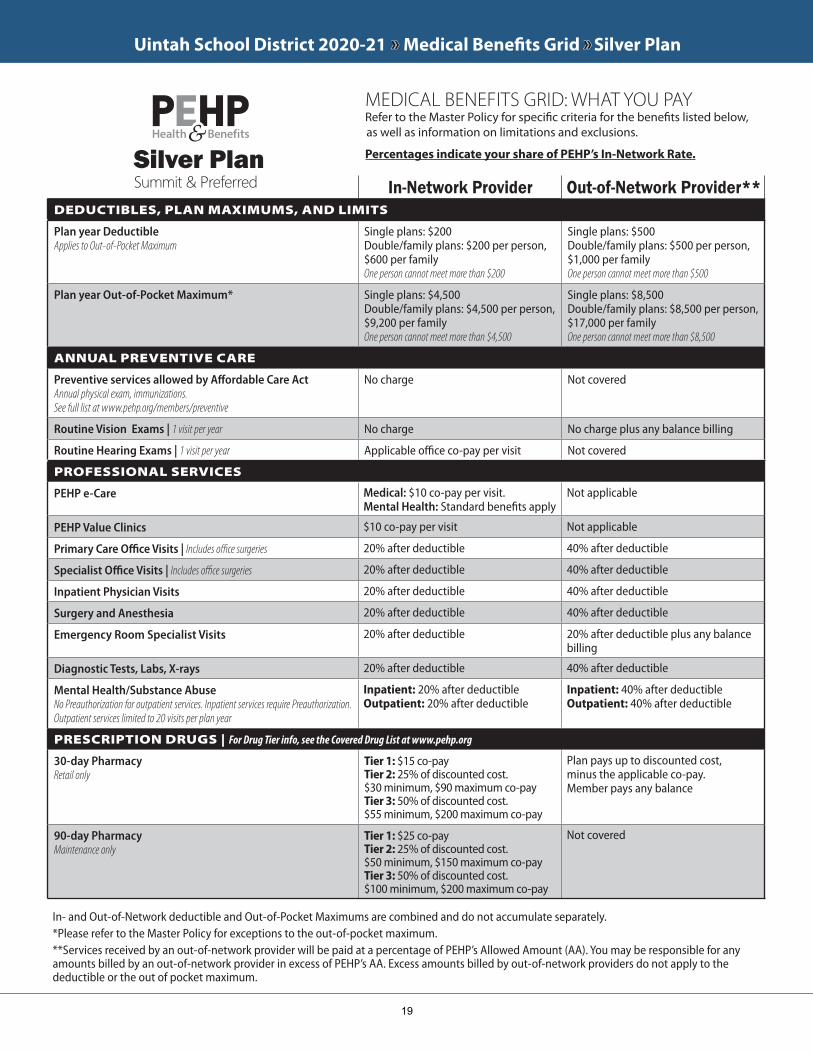
Uintah School District 2020-21 »» Medical Benefits Grid »» Silver Plan
DEDUCTIBLES, PLAN MAXIMUMS, AND LIMITS
Plan year DeductibleApplies to Out-of-Pocket Maximum
Single plans: $200Double/family plans: $200 per person, $600 per familyOne person cannot meet more than $200
Single plans: $500Double/family plans: $500 per person, $1,000 per familyOne person cannot meet more than $500
Plan year Out-of-Pocket Maximum* Single plans: $4,500Double/family plans: $4,500 per person, $9,200 per familyOne person cannot meet more than $4,500
Single plans: $8,500Double/family plans: $8,500 per person, $17,000 per familyOne person cannot meet more than $8,500
ANNUAL PREVENTIVE CARE
Preventive services allowed by Affordable Care ActAnnual physical exam, immunizations.See full list at www.pehp.org/members/preventive
No charge Not covered
Routine Vision Exams | 1 visit per year No charge No charge plus any balance billing
Routine Hearing Exams | 1 visit per year Applicable office co-pay per visit Not covered
PROFESSIONAL SERVICES
PEHP e-Care Medical: $10 co-pay per visit.Mental Health: Standard benefits apply
Not applicable
PEHP Value Clinics $10 co-pay per visit Not applicable
Primary Care Office Visits | Includes office surgeries 20% after deductible 40% after deductible
Specialist Office Visits | Includes office surgeries 20% after deductible 40% after deductible
Inpatient Physician Visits 20% after deductible 40% after deductible
Surgery and Anesthesia 20% after deductible 40% after deductible
Emergency Room Specialist Visits 20% after deductible 20% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 20% after deductible 40% after deductible
Mental Health/Substance Abuse No Preauthorization for outpatient services. Inpatient services require Preauthorization.Outpatient services limited to 20 visits per plan year
Inpatient: 20% after deductible Outpatient: 20% after deductible
Inpatient: 40% after deductible Outpatient: 40% after deductible
PRESCRIPTION DRUGS | For Drug Tier info, see the Covered Drug List at www.pehp.org
30-day Pharmacy Retail only
Tier 1: $15 co-payTier 2: 25% of discounted cost. $30 minimum, $90 maximum co-payTier 3: 50% of discounted cost. $55 minimum, $200 maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
90-day Pharmacy Maintenance only
Tier 1: $25 co-payTier 2: 25% of discounted cost. $50 minimum, $150 maximum co-pay Tier 3: 50% of discounted cost. $100 minimum, $200 maximum co-pay
Not covered
In-Network Provider Out-of-Network Provider**
In- and Out-of-Network deductible and Out-of-Pocket Maximums are combined and do not accumulate separately.*Please refer to the Master Policy for exceptions to the out-of-pocket maximum.**Services received by an out-of-network provider will be paid at a percentage of PEHP’s Allowed Amount (AA). You may be responsible for any amounts billed by an out-of-network provider in excess of PEHP’s AA. Excess amounts billed by out-of-network providers do not apply to the deductible or the out of pocket maximum.
Summit & PreferredSilver Plan
MEDICAL BENEFITS GRID: WHAT YOU PAY Refer to the Master Policy for specific criteria for the benefits listed below, as well as information on limitations and exclusions.
Percentages indicate your share of PEHP’s In-Network Rate.
19
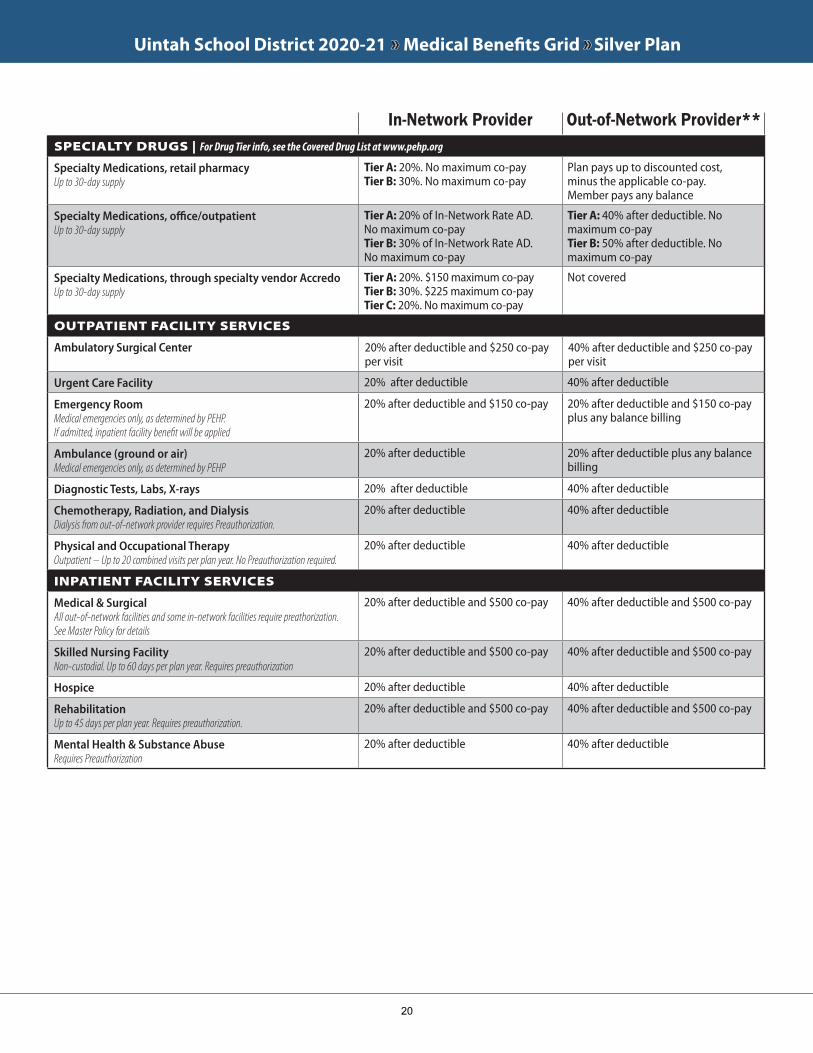
Uintah School District 2020-21 »» Medical Benefits Grid »» Silver Plan
SPECIALTY DRUGS | For Drug Tier info, see the Covered Drug List at www.pehp.org
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 20%. No maximum co-payTier B: 30%. No maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 20% of In-Network Rate AD.No maximum co-payTier B: 30% of In-Network Rate AD.No maximum co-pay
Tier A: 40% after deductible. No maximum co-payTier B: 50% after deductible. No maximum co-pay
Specialty Medications, through specialty vendor AccredoUp to 30-day supply
Tier A: 20%. $150 maximum co-payTier B: 30%. $225 maximum co-payTier C: 20%. No maximum co-pay
Not covered
OUTPATIENT FACILITY SERVICES
Ambulatory Surgical Center 20% after deductible and $250 co-pay per visit
40% after deductible and $250 co-pay per visit
Urgent Care Facility 20% after deductible 40% after deductible
Emergency Room Medical emergencies only, as determined by PEHP.If admitted, inpatient facility benefit will be applied
20% after deductible and $150 co-pay 20% after deductible and $150 co-pay plus any balance billing
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
20% after deductible 20% after deductible plus any balance billing
Diagnostic Tests, Labs, X-rays 20% after deductible 40% after deductible
Chemotherapy, Radiation, and Dialysis Dialysis from out-of-network provider requires Preauthorization.
20% after deductible 40% after deductible
Physical and Occupational Therapy Outpatient – Up to 20 combined visits per plan year. No Preauthorization required.
20% after deductible 40% after deductible
INPATIENT FACILITY SERVICES
Medical & SurgicalAll out-of-network facilities and some in-network facilities require preathorization. See Master Policy for details
20% after deductible and $500 co-pay 40% after deductible and $500 co-pay
Skilled Nursing FacilityNon-custodial. Up to 60 days per plan year. Requires preauthorization
20% after deductible and $500 co-pay 40% after deductible and $500 co-pay
Hospice 20% after deductible 40% after deductible
RehabilitationUp to 45 days per plan year. Requires preauthorization.
20% after deductible and $500 co-pay 40% after deductible and $500 co-pay
Mental Health & Substance AbuseRequires Preauthorization
20% after deductible 40% after deductible
In-Network Provider Out-of-Network Provider**
20
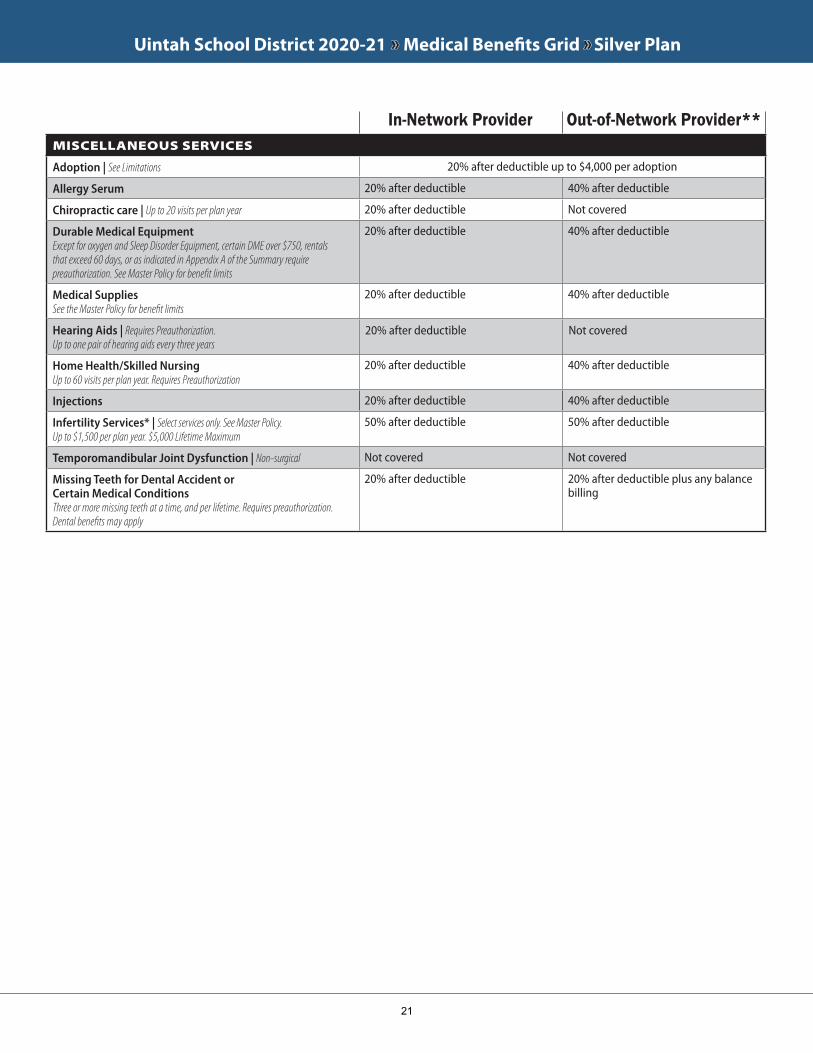
Uintah School District 2020-21 »» Medical Benefits Grid »» Silver Plan
MISCELLANEOUS SERVICES
Adoption | See Limitations 20% after deductible up to $4,000 per adoption
Allergy Serum 20% after deductible 40% after deductible
Chiropractic care | Up to 20 visits per plan year 20% after deductible Not covered
Durable Medical Equipment Except for oxygen and Sleep Disorder Equipment, certain DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Summary require preauthorization. See Master Policy for benefit limits
20% after deductible 40% after deductible
Medical SuppliesSee the Master Policy for benefit limits
20% after deductible 40% after deductible
Hearing Aids | Requires Preauthorization. Up to one pair of hearing aids every three years
20% after deductible Not covered
Home Health/Skilled Nursing Up to 60 visits per plan year. Requires Preauthorization
20% after deductible 40% after deductible
Injections 20% after deductible 40% after deductible
Infertility Services* | Select services only. See Master Policy. Up to $1,500 per plan year. $5,000 Lifetime Maximum
50% after deductible 50% after deductible
Temporomandibular Joint Dysfunction | Non-surgical Not covered Not covered
Missing Teeth for Dental Accident or Certain Medical ConditionsThree or more missing teeth at a time, and per lifetime. Requires preauthorization. Dental benefits may apply
20% after deductible 20% after deductible plus any balance billing
In-Network Provider Out-of-Network Provider**
21
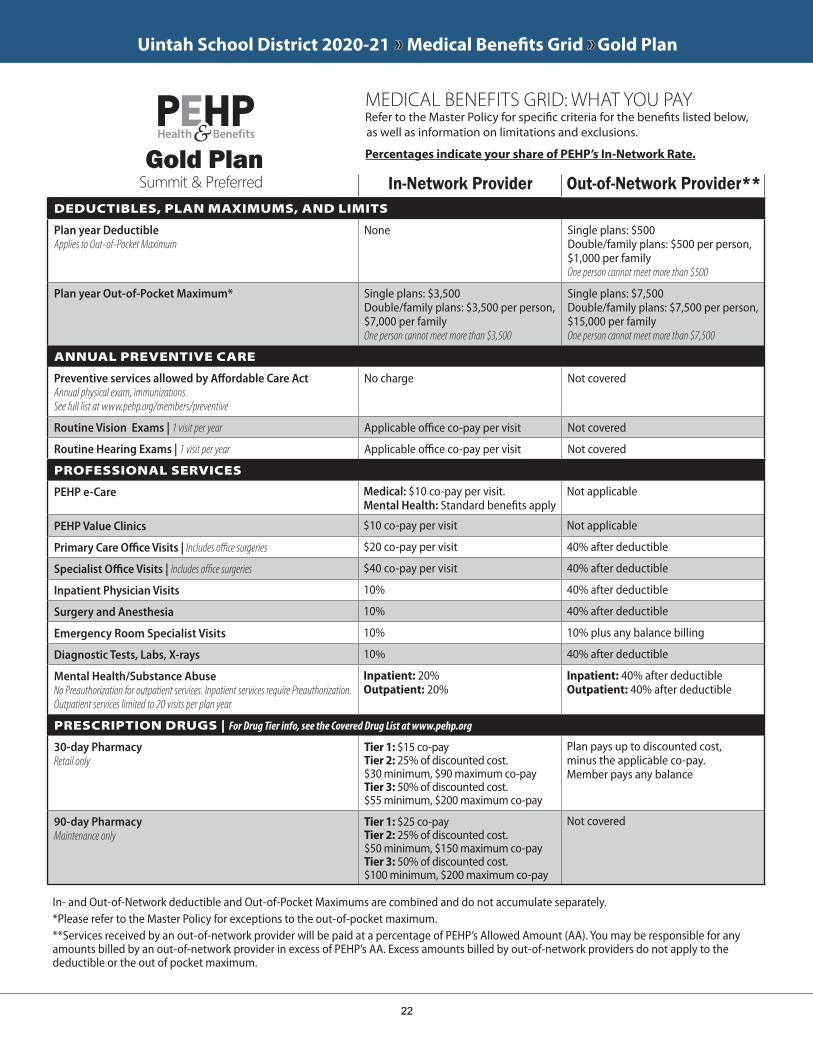
Uintah School District 2020-21 »» Medical Benefits Grid »» Gold Plan
DEDUCTIBLES, PLAN MAXIMUMS, AND LIMITS
Plan year DeductibleApplies to Out-of-Pocket Maximum
None Single plans: $500Double/family plans: $500 per person, $1,000 per familyOne person cannot meet more than $500
Plan year Out-of-Pocket Maximum* Single plans: $3,500Double/family plans: $3,500 per person, $7,000 per familyOne person cannot meet more than $3,500
Single plans: $7,500Double/family plans: $7,500 per person, $15,000 per familyOne person cannot meet more than $7,500
ANNUAL PREVENTIVE CARE
Preventive services allowed by Affordable Care ActAnnual physical exam, immunizations.See full list at www.pehp.org/members/preventive
No charge Not covered
Routine Vision Exams | 1 visit per year Applicable office co-pay per visit Not covered
Routine Hearing Exams | 1 visit per year Applicable office co-pay per visit Not covered
PROFESSIONAL SERVICES
PEHP e-Care Medical: $10 co-pay per visit.Mental Health: Standard benefits apply
Not applicable
PEHP Value Clinics $10 co-pay per visit Not applicable
Primary Care Office Visits | Includes office surgeries $20 co-pay per visit 40% after deductible
Specialist Office Visits | Includes office surgeries $40 co-pay per visit 40% after deductible
Inpatient Physician Visits 10% 40% after deductible
Surgery and Anesthesia 10% 40% after deductible
Emergency Room Specialist Visits 10% 10% plus any balance billing
Diagnostic Tests, Labs, X-rays 10 40% after deductible
Mental Health/Substance Abuse No Preauthorization for outpatient services. Inpatient services require Preauthorization.Outpatient services limited to 20 visits per plan year
Inpatient: 20% Outpatient: 20%
Inpatient: 40% after deductible Outpatient: 40% after deductible
PRESCRIPTION DRUGS | For Drug Tier info, see the Covered Drug List at www.pehp.org
30-day Pharmacy Retail only
Tier 1: $15 co-payTier 2: 25% of discounted cost. $30 minimum, $90 maximum co-payTier 3: 50% of discounted cost. $55 minimum, $200 maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
90-day Pharmacy Maintenance only
Tier 1: $25 co-payTier 2: 25% of discounted cost. $50 minimum, $150 maximum co-pay Tier 3: 50% of discounted cost. $100 minimum, $200 maximum co-pay
Not covered
In- and Out-of-Network deductible and Out-of-Pocket Maximums are combined and do not accumulate separately.*Please refer to the Master Policy for exceptions to the out-of-pocket maximum.**Services received by an out-of-network provider will be paid at a percentage of PEHP’s Allowed Amount (AA). You may be responsible for any amounts billed by an out-of-network provider in excess of PEHP’s AA. Excess amounts billed by out-of-network providers do not apply to the deductible or the out of pocket maximum.
Summit & PreferredGold Plan
In-Network Provider Out-of-Network Provider**
MEDICAL BENEFITS GRID: WHAT YOU PAY Refer to the Master Policy for specific criteria for the benefits listed below, as well as information on limitations and exclusions.
Percentages indicate your share of PEHP’s In-Network Rate.
22
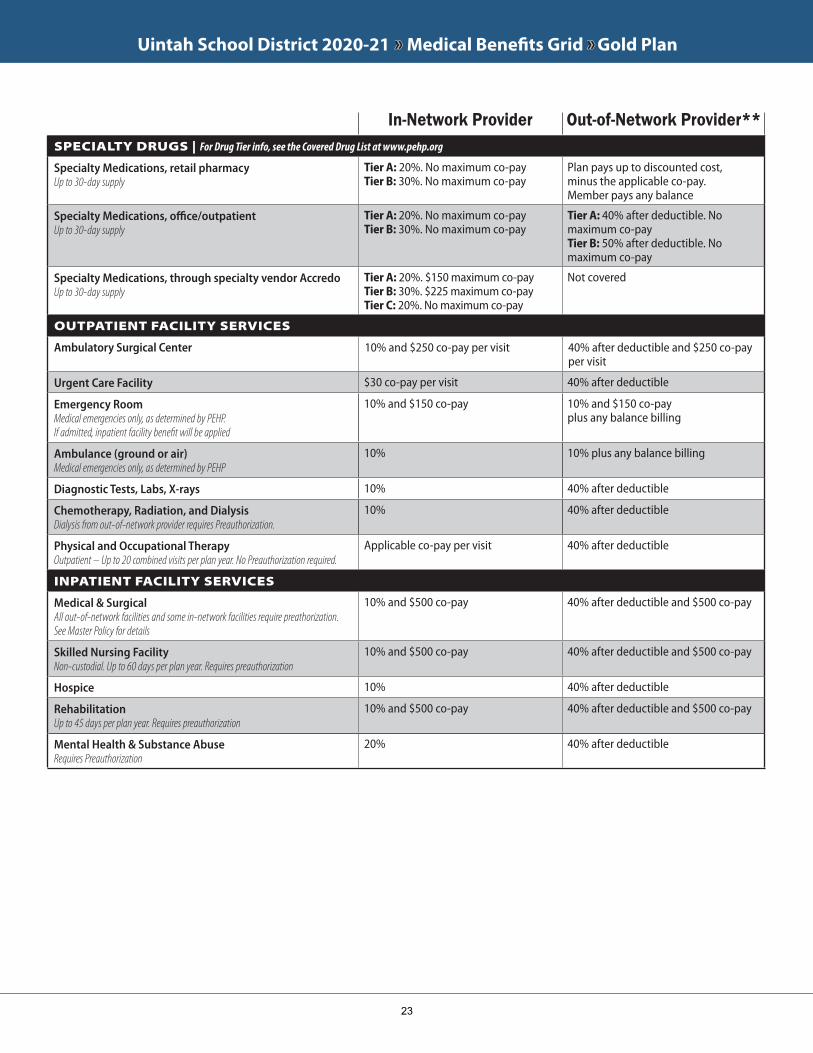
Uintah School District 2020-21 »» Medical Benefits Grid »» Gold Plan
SPECIALTY DRUGS | For Drug Tier info, see the Covered Drug List at www.pehp.org
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 20%. No maximum co-payTier B: 30%. No maximum co-pay
Plan pays up to discounted cost, minus the applicable co-pay. Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 20%. No maximum co-payTier B: 30%. No maximum co-pay
Tier A: 40% after deductible. No maximum co-payTier B: 50% after deductible. No maximum co-pay
Specialty Medications, through specialty vendor AccredoUp to 30-day supply
Tier A: 20%. $150 maximum co-payTier B: 30%. $225 maximum co-payTier C: 20%. No maximum co-pay
Not covered
OUTPATIENT FACILITY SERVICES
Ambulatory Surgical Center 10% and $250 co-pay per visit 40% after deductible and $250 co-pay per visit
Urgent Care Facility $30 co-pay per visit 40% after deductible
Emergency Room Medical emergencies only, as determined by PEHP.If admitted, inpatient facility benefit will be applied
10% and $150 co-pay 10% and $150 co-pay plus any balance billing
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
10% 10% plus any balance billing
Diagnostic Tests, Labs, X-rays 10% 40% after deductible
Chemotherapy, Radiation, and Dialysis Dialysis from out-of-network provider requires Preauthorization.
10% 40% after deductible
Physical and Occupational Therapy Outpatient – Up to 20 combined visits per plan year. No Preauthorization required.
Applicable co-pay per visit 40% after deductible
INPATIENT FACILITY SERVICES
Medical & SurgicalAll out-of-network facilities and some in-network facilities require preathorization. See Master Policy for details
10% and $500 co-pay 40% after deductible and $500 co-pay
Skilled Nursing FacilityNon-custodial. Up to 60 days per plan year. Requires preauthorization
10% and $500 co-pay 40% after deductible and $500 co-pay
Hospice 10% 40% after deductible
RehabilitationUp to 45 days per plan year. Requires preauthorization
10% and $500 co-pay 40% after deductible and $500 co-pay
Mental Health & Substance AbuseRequires Preauthorization
20% 40% after deductible
In-Network Provider Out-of-Network Provider**
23
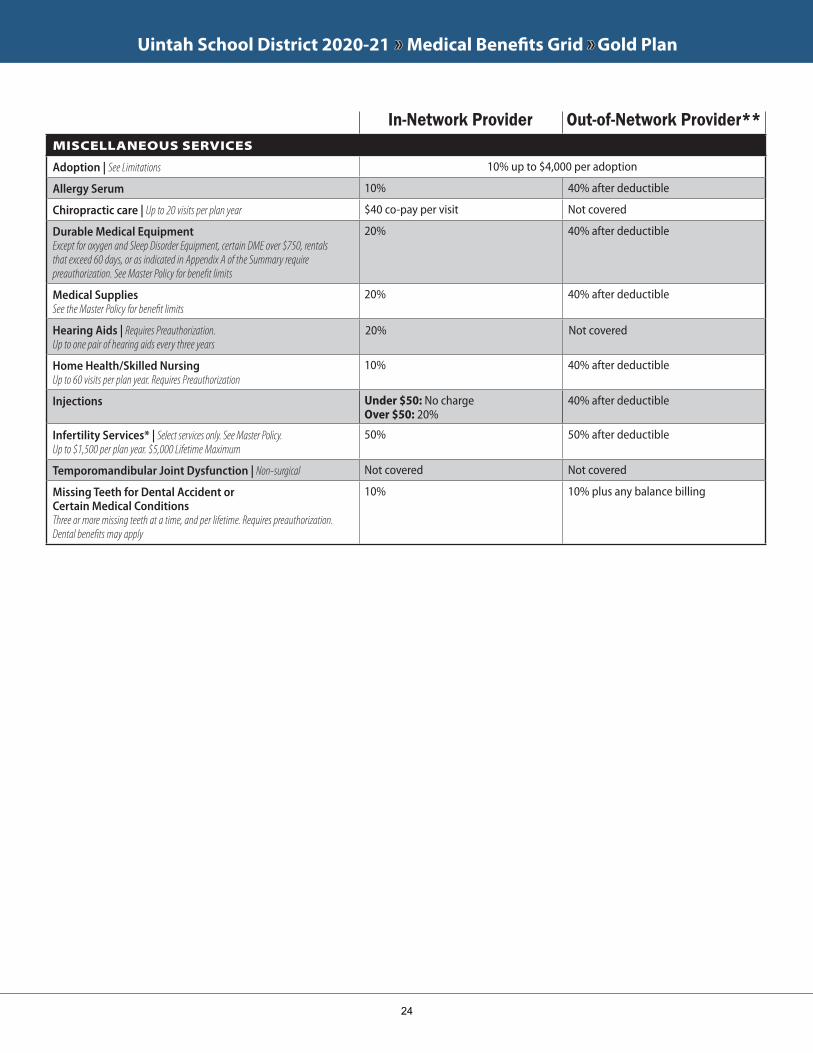
Uintah School District 2020-21 »» Medical Benefits Grid »» Gold Plan
MISCELLANEOUS SERVICES
Adoption | See Limitations 10% up to $4,000 per adoption
Allergy Serum 10% 40% after deductible
Chiropractic care | Up to 20 visits per plan year $40 co-pay per visit Not covered
Durable Medical Equipment Except for oxygen and Sleep Disorder Equipment, certain DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Summary require preauthorization. See Master Policy for benefit limits
20% 40% after deductible
Medical SuppliesSee the Master Policy for benefit limits
20% 40% after deductible
Hearing Aids | Requires Preauthorization. Up to one pair of hearing aids every three years
20% Not covered
Home Health/Skilled Nursing Up to 60 visits per plan year. Requires Preauthorization
10% 40% after deductible
Injections Under $50: No chargeOver $50: 20%
40% after deductible
Infertility Services* | Select services only. See Master Policy. Up to $1,500 per plan year. $5,000 Lifetime Maximum
50% 50% after deductible
Temporomandibular Joint Dysfunction | Non-surgical Not covered Not covered
Missing Teeth for Dental Accident or Certain Medical ConditionsThree or more missing teeth at a time, and per lifetime. Requires preauthorization. Dental benefits may apply
10% 10% plus any balance billing
In-Network Provider Out-of-Network Provider**
24
Health Savings AccountAxisPlus
25
At age 55, an additional $1,000 contribution is allowed annually.
Health Savings AccountAbout Health Savings AccountsA Health Savings Account (HSA) is a tax advantaged savings account that you own and control. HSAs are similar to retirement accounts in that funds rollover year-to-year, it is portable if you move jobs or retire, the balance can be invested in mutual funds, and there are survivor benefits.
The HSA Advantage› It’s a Tax Saver
• Contributions are excluded from federal income tax• Your money grows tax-free• Withdrawals used to pay for qualified health care expenses are also tax-free
› Ownership: The money in your HSA is always yours. Unspent balances simply roll over fromyear to year until spent.
› Flexibility: You decide when and how much to contribute to your account.› Portable: Your money stays put even if you change health plans or employers, or if you retire.
Who is eligible?You must be enrolled in our qualified high deductible health plan (HDHP) and meet the following requirements:
› Have no other health insurance coverage except what’s permitted by the IRS› Not be enrolled in Medicare› Not be claimed as a dependent on someone else’s tax return
How much can I contribute to my HSA?Each year the IRS establishes the maximum contribution limits (see the table below). These limitsare for the total funds contributed, including company contributions, your contributions and anyother contributions. Please keep in mind you can change your HSA allocation at any time duringthe plan year.
Determining Your Annual ContributionYour allowed annual contribution is calculated based on the number of months covered by aqualified HDHP plan and your coverage type (self-only or family). For example, if you have self-only coverage 8 months of the year, your maximum contribution limit is $2,333. Formula: $2,333 =8 x ($3,500 / 12)
Per the last-month rule (IRS Publication 969), if you are eligible on the 1st day of the last month ofyour tax year (usually December 1st), you are considered eligible for the entire year. You maycontribute up to the annual maximum IRS limit, but only if you maintain qualified HDHP coveragefor the entire following year.
Our Banking PartnerWe have partnered with AxisPlus for HSA administration. For newly enrolled employees, yourdemographic data is transmitted to the bank upon electing our qualified HDHP. AxisPlus will mailyou a welcome kit upon activating your account which will contain information about the bank andhow to use the online banking features and your debit card. If you are an existing account holder,you will continue to use your same Health Savings Account which rolls over year after year. Pleaseuse the same debit card you currently have. The bank will automatically send you a new debit cardapproximately one month before your current card expires.
2020Self-Only $3,550Family $7,100
26
Qualified Health Care ExpensesYou can use money in your HSA to pay for any qualified health care expenses you, your legalspouse and your tax dependents incur, even if they are not covered on your plan. Qualified healthcare expenses are designated by the IRS (Publication 502). They include medical, dental, visionand prescription expenses not covered by the insurance carrier.
Qualified expenses include, but are not limited to:• Acupuncture• Alcoholism (rehab)• Ambulance• Amounts not covered under
another health plan• Annual physical
examination• Artificial limbs• Birth control
pills/prescriptioncontraceptives
• Body scans• Post-mastectomy breast
reconstruction surgery
• Chiropractor• Contact lenses• Crutches• Dental treatments• Eyeglasses/eye surgery• Hearing aids• Long-term care expenses• Medicines (prescribed)• Nursing home medical care• Nursing services• Optometrist• Lasik surgery• Orthodontia
• Oxygen• Stop-smoking programs• Surgery, other than
unnecessary cosmeticsurgery
• Telephone equipment forthe hearing-impaired
• Therapy• Transplants• Weight-loss program
(prescribed)• Wheelchairs• Wigs (prescribed)
Non-qualified expenses include any expenses incurred before you establish your HSA. Other non-qualified expenses include, but are not limited to:
• Concierge services• Dancing lessons• Diaper service• Elective cosmetic surgery• Electrolysis or hair removal
• Funeral Expenses• Future medical care• Hair transplants• Health club dues• Insurance premiums*
• Medicines and drugs fromother countries
• Non-prescription drugs(other than insulin)
• Teeth whitening
The following insurance premiums may be reimbursed from your HSA:• COBRA premiums• Health insurance premiums while receiving unemployment benefits• Qualified long-term care premiums• Medicare premiums (Parts A, B, C, etc.)
Documentation is KeyAn HSA can be used for a wide range of health care services within the limits established by law.Be sure you understand what expenses are HSA qualified, and be able to produce receipts forthose items or services that you purchase with your HSA. You must keep records sufficient toshow that:
• The distributions were exclusively to pay or reimburse qualified medical expenses,• The qualified expenses had not been previously paid or reimbursed from another source,
and• The qualified expense had not been taken as an itemized deduction in any year.
Do not send these records with your tax return. Keep them with your tax records.
Health Savings Account
› ImportantAny funds you withdraw for non-qualified expenses will be taxed at your income tax rate plus a20% tax penalty if you're under age 65. After age 65, you pay taxes but no penalty.
27
DentalTDA Dental
28
Provider Network
Class 1 -Preventative Services
-Oral Examinations (2 every 12 months)
-Cleanings (1 every 6 months)
-X-Rays (bitewing 1 every 6 months)
-Pallitave Emergency Treatment
Class 2 -Basic Services
-Restorations (Composite fillings)
-Extractions
-Oral Surgery
Class 3 -Major Dentistry
-Crowns
-Dentures
-Bridges
-Endodontics (root canal therapy)
-Periodontics (treatment of gum tissue)
-Other Prosthetic Services
Class 4 -Orthodontic Services
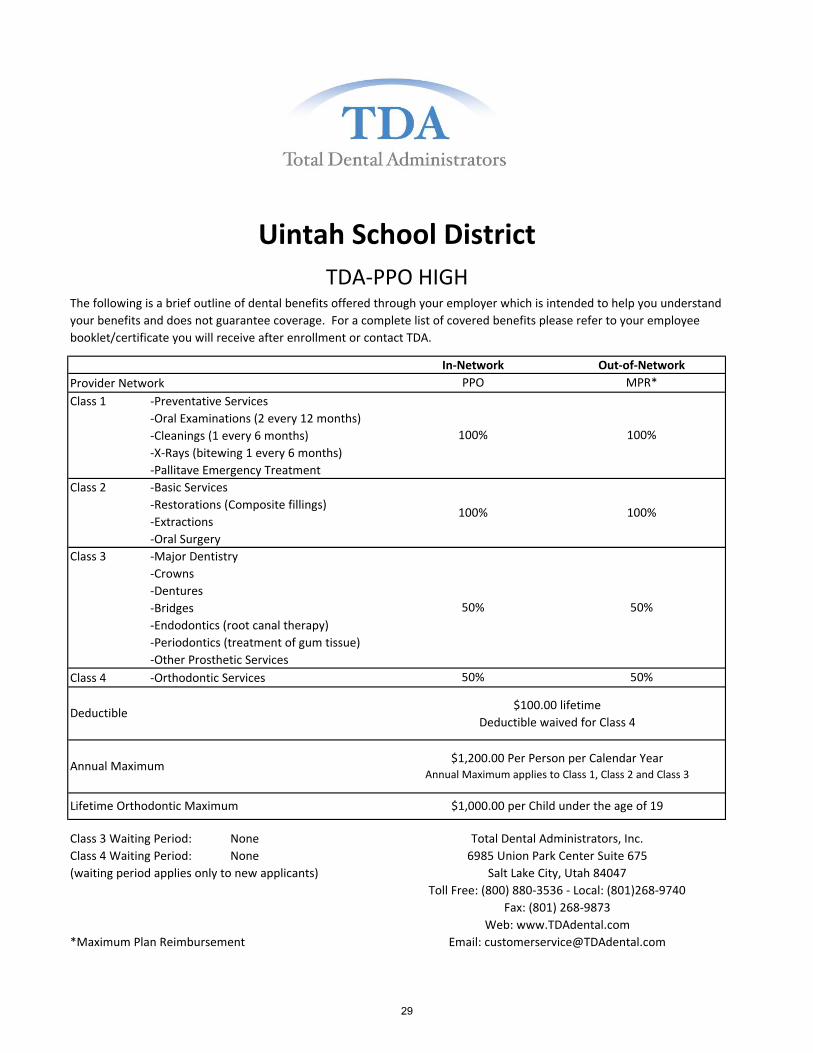
Class 3 Waiting Period: None
Class 4 Waiting Period: None
(waiting period applies only to new applicants)
*Maximum Plan Reimbursement
50%
Deductible$100.00 lifetime
Deductible waived for Class 4
Uintah School District
TDA-PPO HIGHThe following is a brief outline of dental benefits offered through your employer which is intended to help you understand
your benefits and does not guarantee coverage. For a complete list of covered benefits please refer to your employee
booklet/certificate you will receive after enrollment or contact TDA.
In-Network Out-of-Network
Salt Lake City, Utah 84047
Toll Free: (800) 880-3536 - Local: (801)268-9740
Lifetime Orthodontic Maximum $1,000.00 per Child under the age of 19
Annual Maximum$1,200.00 Per Person per Calendar Year
Web: www.TDAdental.com
Email: [email protected]
PPO MPR*
50% 50%
Fax: (801) 268-9873
100% 100%
100% 100%
Annual Maximum applies to Class 1, Class 2 and Class 3
50%
Total Dental Administrators, Inc.
6985 Union Park Center Suite 675
29
Provider Network
Class 1 -Preventative Services
-Oral Examinations (2 every 12 months)
-Cleanings (1 every 6 months)
-X-Rays (bitewing 1 every 6 months)
-Pallitave Emergency Treatment
Class 2 -Basic Services
-Restorations (Composite fillings)
-Extractions
-Oral Surgery
Class 3 -Major Dentistry
-Crowns
-Dentures
-Bridges
-Endodontics (root canal therapy)
-Periodontics (treatment of gum tissue)
-Other Prosthetic Services
Class 4 -Orthodontic Services
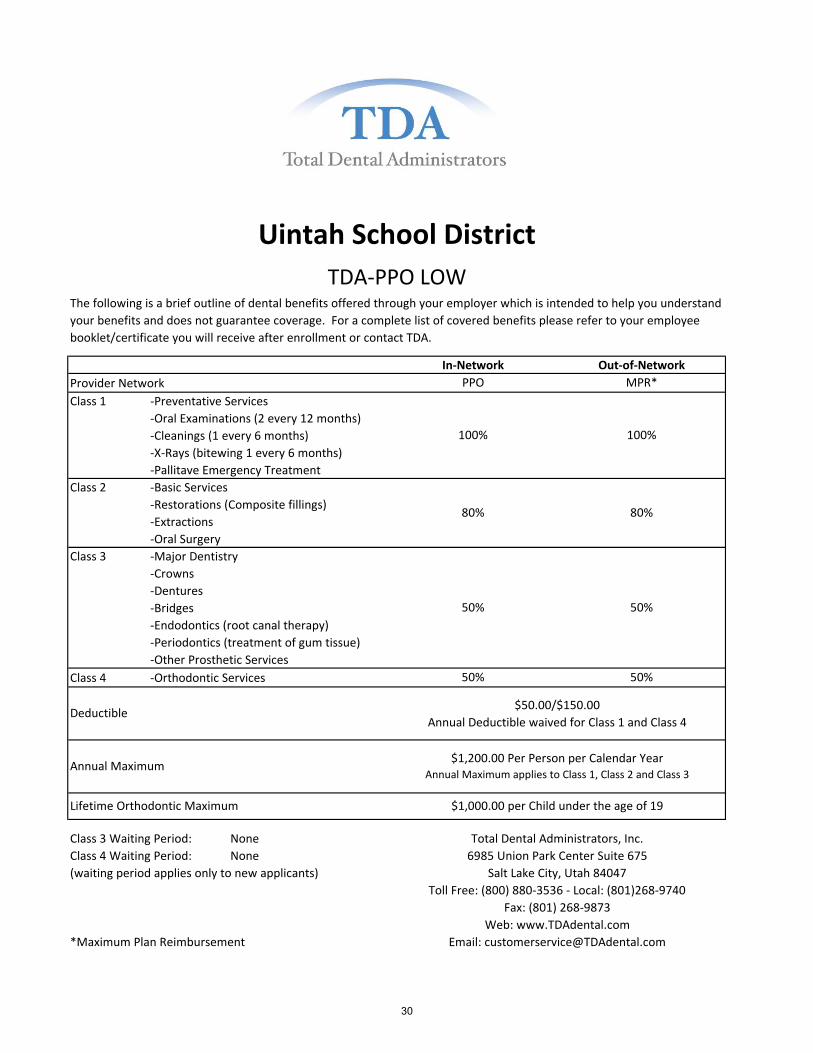
Class 3 Waiting Period: None
Class 4 Waiting Period: None
(waiting period applies only to new applicants)
*Maximum Plan Reimbursement
Web: www.TDAdental.com
Email: [email protected]
PPO MPR*
50% 50%
Fax: (801) 268-9873
100% 100%
80% 80%
Annual Maximum applies to Class 1, Class 2 and Class 3
50%
Total Dental Administrators, Inc.
6985 Union Park Center Suite 675
Salt Lake City, Utah 84047
Toll Free: (800) 880-3536 - Local: (801)268-9740
Lifetime Orthodontic Maximum $1,000.00 per Child under the age of 19
Annual Maximum$1,200.00 Per Person per Calendar Year
50%
Deductible$50.00/$150.00
Annual Deductible waived for Class 1 and Class 4
Uintah School District
TDA-PPO LOWThe following is a brief outline of dental benefits offered through your employer which is intended to help you understand
your benefits and does not guarantee coverage. For a complete list of covered benefits please refer to your employee
booklet/certificate you will receive after enrollment or contact TDA.
In-Network Out-of-Network
30
VisionOpticare of Utah
31
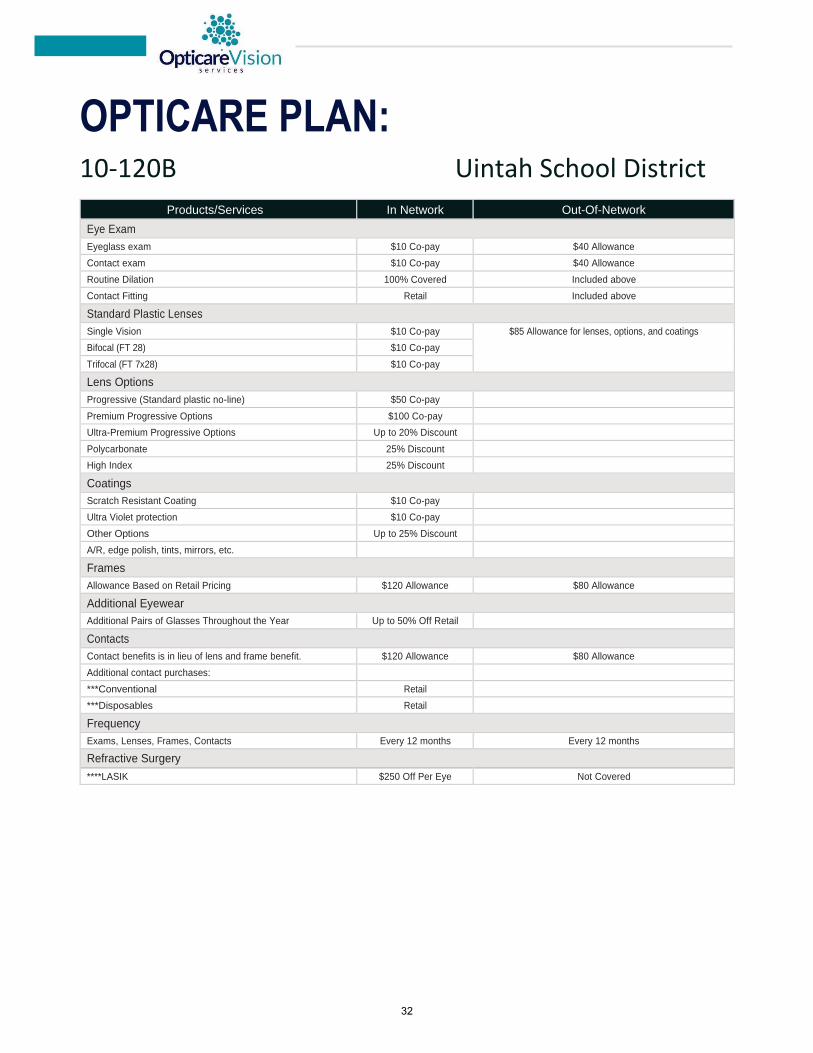
OPTICARE PLAN: 10-120B Uintah School District
Products/Services In Network Out-Of-Network
Eye Exam
Eyeglass exam $10 Co-pay $40 Allowance
Contact exam $10 Co-pay $40 Allowance
Routine Dilation 100% Covered Included above
Contact Fitting Retail Included above
Standard Plastic Lenses
Single Vision $10 Co-pay $85 Allowance for lenses, options, and coatings
Bifocal (FT 28) $10 Co-pay
Trifocal (FT 7x28) $10 Co-pay
Lens Options
Progressive (Standard plastic no-line) $50 Co-pay
Premium Progressive Options $100 Co-pay
Ultra-Premium Progressive Options Up to 20% Discount
Polycarbonate 25% Discount
High Index 25% Discount
Coatings
Scratch Resistant Coating $10 Co-pay
Ultra Violet protection $10 Co-pay
Other Options Up to 25% Discount
A/R, edge polish, tints, mirrors, etc.
Frames
Allowance Based on Retail Pricing $120 Allowance $80 Allowance
Additional Eyewear
Additional Pairs of Glasses Throughout the Year Up to 50% Off Retail
Contacts
Contact benefits is in lieu of lens and frame benefit. $120 Allowance $80 Allowance
Additional contact purchases:
***Conventional Retail
***Disposables Retail
Frequency
Exams, Lenses, Frames, Contacts Every 12 months Every 12 months
Refractive Surgery
****LASIK $250 Off Per Eye Not Covered
32
Flexible Spending Account
AxisPlus
33

34
35
36
37
38

39
40
Life and AD&D
Lincoln Financial
41
Uintah School District provides this valuable benefit at no cost to you.
All Full-Time Employees
Safeguard the most important people in your life.
Think about what your loved ones may face after you’re gone. Term life insurance can help them in so many
ways, like covering everyday expenses, paying off debt, and protecting savings. AD&D provides even more
coverage if you die or suffer a covered loss in an accident.
AT A GLANCE:
• A cash benefit of $50,000 to your loved ones in the event of your death, plus a matching cash
benefit if you die in an accident
• A cash benefit to you if you suffer a covered loss in an accident, such as losing a limb or your
eyesight
• LifeKeys® services, which provide access to counseling, financial, and legal support
• TravelConnectSM services, which give you and your family access to emergency medical
assistance when you're on a trip 100+ miles from home
You also have the option to increase your cash benefit by securing additional coverage at affordable group rates. See the enclosed life insurance information for details.
ADDITIONAL DETAILS
Conversion: You can convert your group term life coverage to an individual life insurance policy without
providing evidence of insurability if you lose coverage due to leaving your job or for another reason outlined in
the plan contract. AD&D benefits cannot be converted.
Benefit Reduction: Coverage amounts begin to reduce at age 65 and benefits terminate at retirement. See the
plan certificate for details.
For complete benefit descriptions, limitations, and exclusions, refer to the certificate of coverage. This is not intended as a complete description of the insurance coverage offered. Controlling provisions are provided in the policy, and this summary does not modify those provisions or the insurance in any way. This is not a binding contract. A certificate of coverage will be made available to you that describes the benefits in greater detail. Refer to your certificate for your maximum benefit amounts. Should there be a difference between this summary and the contract, the contract will govern.
LifeKeys® services are provided by ComPsych® Corporation, Chicago, IL. ComPsych®, EstateGuidance® and GuidanceResources® are registered trademarks of ComPsych® Corporation. TravelConnectSM services are provided by On Call International, Salem, NH. ComPsych® and On Call International are not Lincoln Financial Group® companies. Coverage is subject to actual contract language. Each independent company is solely responsible for its own obligations. Insurance products (policy series GL1101) are issued by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicit business in New York, nor is it licensed to do so. Product availability and/or features may vary by state. Limitations and exclusions apply. Lincoln Financial Group is the marketing name for Lincoln National Corporation and its affiliates. Affiliates are separately responsible for their own financial and contractual obligations. Limitations and exclusions apply.
Term Life and AD&D Insurance
42
Term Life Insurance
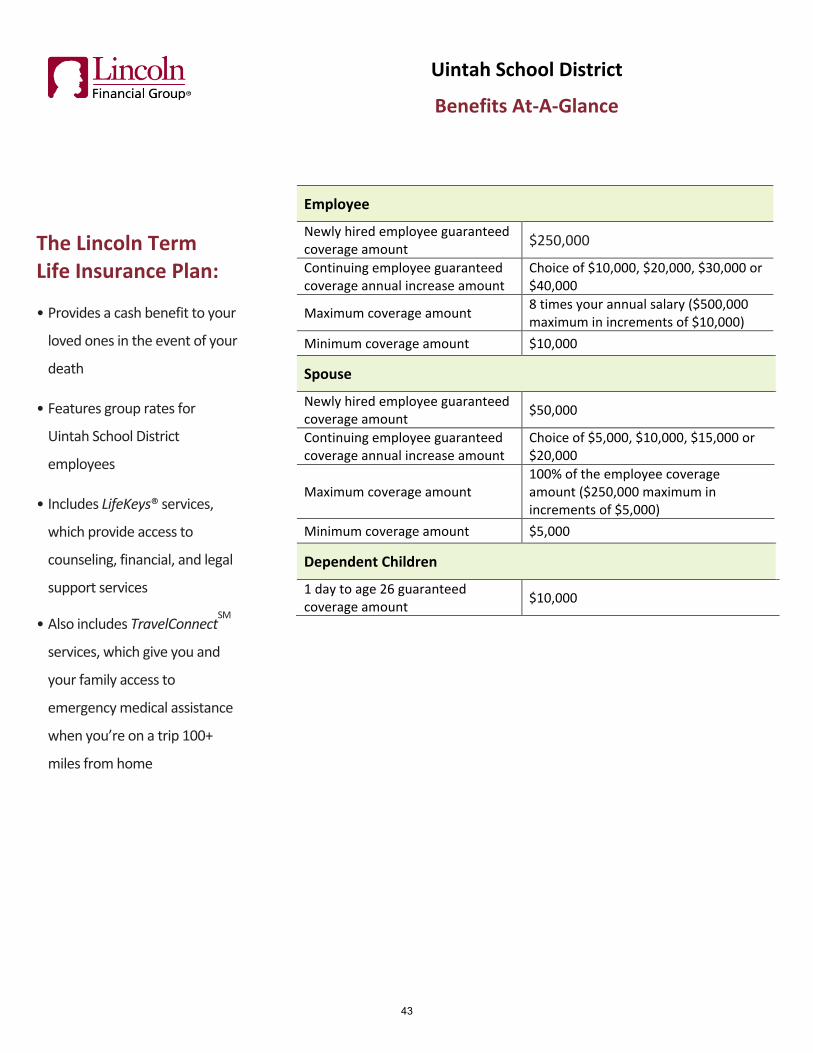
The Lincoln Term Life Insurance Plan:
• Provides a cash benefit to your
loved ones in the event of your
death
• Features group rates for
Uintah School District
employees
• Includes LifeKeys® services,
which provide access to
counseling, financial, and legal
support services
• Also includes TravelConnectSM
services, which give you and
your family access to
emergency medical assistance
when you’re on a trip 100+
miles from home
Uintah School District
Benefits At-A-Glance
Employee
Newly hired employee guaranteed coverage amount
$250,000
Continuing employee guaranteed coverage annual increase amount
Choice of $10,000, $20,000, $30,000 or $40,000
Maximum coverage amount 8 times your annual salary ($500,000 maximum in increments of $10,000)
Minimum coverage amount $10,000
Spouse
Newly hired employee guaranteed coverage amount
$50,000
Continuing employee guaranteed coverage annual increase amount
Choice of $5,000, $10,000, $15,000 or $20,000
Maximum coverage amount 100% of the employee coverage amount ($250,000 maximum in increments of $5,000)
Minimum coverage amount $5,000
Dependent Children
1 day to age 26 guaranteed coverage amount
$10,000
43
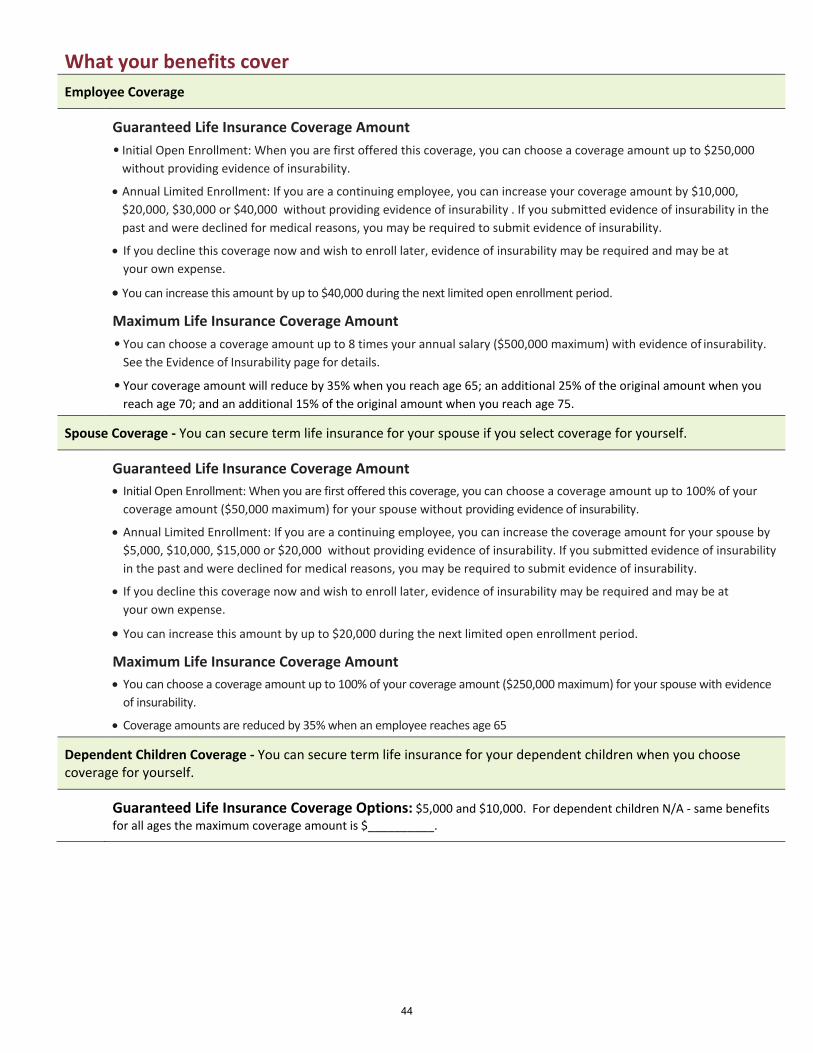
What your benefits cover
Employee Coverage
Guaranteed Life Insurance Coverage Amount
• Initial Open Enrollment: When you are first offered this coverage, you can choose a coverage amount up to $250,000
without providing evidence of insurability.
• Annual Limited Enrollment: If you are a continuing employee, you can increase your coverage amount by $10,000,
$20,000, $30,000 or $40,000 without providing evidence of insurability . If you submitted evidence of insurability in the
past and were declined for medical reasons, you may be required to submit evidence of insurability.
• If you decline this coverage now and wish to enroll later, evidence of insurability may be required and may be at
your own expense.
• You can increase this amount by up to $40,000 during the next limited open enrollment period.
Maximum Life Insurance Coverage Amount
• You can choose a coverage amount up to 8 times your annual salary ($500,000 maximum) with evidence of insurability.
See the Evidence of Insurability page for details.
• Your coverage amount will reduce by 35% when you reach age 65; an additional 25% of the original amount when you
reach age 70; and an additional 15% of the original amount when you reach age 75.
Spouse Coverage - You can secure term life insurance for your spouse if you select coverage for yourself.
Guaranteed Life Insurance Coverage Amount
• Initial Open Enrollment: When you are first offered this coverage, you can choose a coverage amount up to 100% of your
coverage amount ($50,000 maximum) for your spouse without providing evidence of insurability.
• Annual Limited Enrollment: If you are a continuing employee, you can increase the coverage amount for your spouse by
$5,000, $10,000, $15,000 or $20,000 without providing evidence of insurability. If you submitted evidence of insurability
in the past and were declined for medical reasons, you may be required to submit evidence of insurability.
• If you decline this coverage now and wish to enroll later, evidence of insurability may be required and may be at
your own expense.
• You can increase this amount by up to $20,000 during the next limited open enrollment period.
Maximum Life Insurance Coverage Amount
• You can choose a coverage amount up to 100% of your coverage amount ($250,000 maximum) for your spouse with evidence
of insurability.
• Coverage amounts are reduced by 35% when an employee reaches age 65
Dependent Children Coverage - You can secure term life insurance for your dependent children when you choose coverage for yourself.
Guaranteed Life Insurance Coverage Options: $5,000 and $10,000. For dependent children N/A - same benefits
for all ages the maximum coverage amount is $__________.
44

Additional Plan Benefits
Accelerated Death Benefit Included
Premium Waiver Included
Conversion Included
Portability Included
Benefit Exclusions Like any insurance, this term life insurance policy does have exclusions. A suicide exclusion may apply. A complete list of benefit exclusions is included in the policy. State variations apply.
45

Monthly Supplemental Life Insurance Premium Here’s how little you pay with group rates.
Employee Age
Range
Life Premium
Rate
0 - 24 0.0000500
25 - 29 0.0000600
30 - 34 0.0000600
35 - 39 0.0000800
40 - 44 0.0001000
45 - 49 0.0001500
50 - 54 0.0002200
55 - 59 0.0003700
60 - 64 0.0004400
65 - 69 0.0007200
70 - 74 0.0013500
75 - 79 0.0020600
Group Rates for You
if You are not a Tobacco User
The estimated monthly premium for life insurance is determined by multiplying the desired amount of coverage (in increments of $10,000) by the employee age-range premium rate.
$____________ X ___________ = $_______________
coverage amount premium rate monthly premium
Note: Rates are subject to change and can vary over time.
Employee Age
Range
Life Premium
Rate
0 - 24 0.0000900
25 - 29 0.0000900
30 - 34 0.0000900
35 - 39 0.0001200
40 - 44 0.0001500
45 - 49 0.0002400
50 - 54 0.0003300
55 - 59 0.0005600
60 - 64 0.0006600
65 - 69 0.0010800
70 - 74 0.0000000
75 - 79 0.0000000
Group Rates for You
if You are a Tobacco User
The estimated monthly premium for life insurance is determined by multiplying the desired amount of coverage (in increments of $10,000) by the employee age-range premium rate.
$____________ X ___________ = $_______________
coverage amount premium rate monthly premium
Note: Rates are subject to change and can vary over time.
46
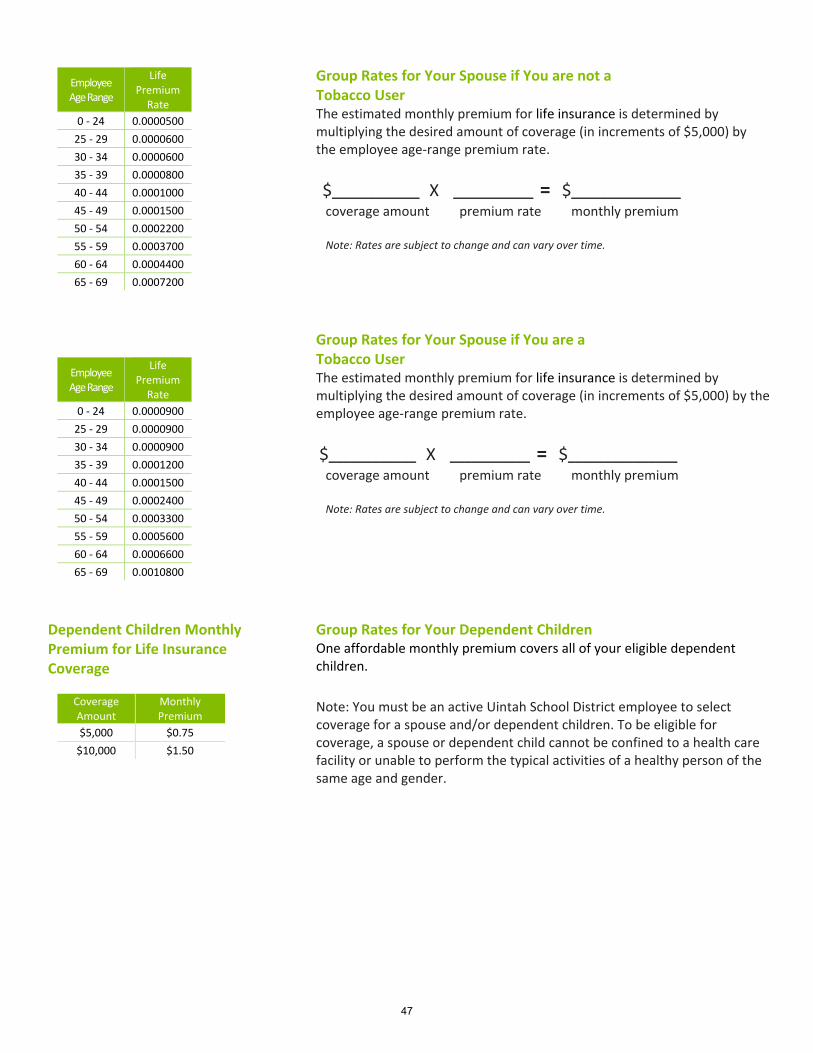
Employee Age Range
Life Premium
Rate
0 - 24 0.0000500
25 - 29 0.0000600
30 - 34 0.0000600
35 - 39 0.0000800
40 - 44 0.0001000
45 - 49 0.0001500
50 - 54 0.0002200
55 - 59 0.0003700
60 - 64 0.0004400
65 - 69 0.0007200
Group Rates for Your Spouse if You are not a Tobacco User
The estimated monthly premium for life insurance is determined by multiplying the desired amount of coverage (in increments of $5,000) by the employee age-range premium rate.
$____________ X ___________ = $_______________
coverage amount premium rate monthly premium
Note: Rates are subject to change and can vary over time.
Employee Age Range
Life Premium
Rate
0 - 24 0.0000900
25 - 29 0.0000900
30 - 34 0.0000900
35 - 39 0.0001200
40 - 44 0.0001500
45 - 49 0.0002400
50 - 54 0.0003300
55 - 59 0.0005600
60 - 64 0.0006600
65 - 69 0.0010800
Group Rates for Your Spouse if You are a Tobacco User The estimated monthly premium for life insurance is determined by multiplying the desired amount of coverage (in increments of $5,000) by the employee age-range premium rate.
$____________ X ___________ = $_______________
coverage amount premium rate monthly premium
Note: Rates are subject to change and can vary over time.
Dependent Children Monthly Premium for Life Insurance Coverage
Coverage Amount
Monthly Premium
$5,000 $0.75
$10,000 $1.50
Group Rates for Your Dependent Children One affordable monthly premium covers all of your eligible dependent children.
Note: You must be an active Uintah School District employee to select coverage for a spouse and/or dependent children. To be eligible for coverage, a spouse or dependent child cannot be confined to a health care facility or unable to perform the typical activities of a healthy person of the same age and gender.
47

Disabil ity
Lincoln Financial
48
Uintah School District provides this valuable benefit at no cost to you.
All Full-Time Employees
Keep getting a check when you’re hurt or sick.
You always have bills to pay, even when you can’t get to work due to injury, illness, or surgery. Long-term
disability insurance helps you make ends meet during this difficult time.
AT A GLANCE:
• A cash benefit of 60% of your monthly salary (up to $6,000) starting 120 days after you are out
of work and continuing up to age 65 or Social Security Normal Retirement Age (SSNRA), whichever
is later
• EmployeeConnectSM services, which give you and your family confidential access to counselors
as well as personal, legal, and financial assistance.
• Program Services include:
- Unlimited, 24/7 access to information and referrals
- In-person help for short-term issues; up to four sessions with a counselor per
person, per issue, per year.
- One free consultation with a network attorney (with subsequent meetings at a
reduced fee)
- Online tools, tutorials, videos and much more
ADDITIONAL DETAILS
Coverage Period for Your Occupation: 24 months. After this initial period, you may be eligible to continue
receiving benefits if your disability prohibits you from performing any employment for which you are
reasonably suited through your training, education, and experience. In this case, your benefits may be
extended through the end of your maximum coverage period (benefit duration).
Pre-existing Condition: If you have a medical condition that begins before your coverage takes effect, and you
receive treatment for this condition within the 3 months leading up to your coverage start date, you may not
be eligible for benefits for that condition until you have been covered by the plan for 12 months.
For complete benefit descriptions, limitations, and exclusions, refer to the certificate of coverage. This is not intended as a complete description of the insurance coverage offered. Controlling provisions are provided in the policy, and this summary does not modify those provisions or the insurance in any way. This is not a binding contract. A certificate of coverage will be made available to you that describes the benefits in greater detail. Refer to your certificate for your maximum benefit amounts. Should there be a difference between this summary and the contract, the contract will govern.
EmployeeConnectSM services are provided by ComPsych® Corporation, Chicago, IL. ComPsych® is a registered trademark of ComPsych® Corporation. ComPsych® is not a Lincoln Financial Group® company. Coverage is subject to actual contract language. Each independent company is solely responsible for its own obligations.
Insurance products (policy series GL3001) are issued by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicit business in New York, nor is it licensed to do so. Product availability and/or features may vary by state. Limitations and exclusions apply. Lincoln Financial Group is the marketing name for Lincoln National Corporation and its affiliates. Affiliates are separately responsible for their own financial and contractual obligations. Limitations and exclusions apply.
Long-term Disability Insurance
49
Voluntary
Allstate
50

Today, active lifestyles in or out of the home may result in bumps, bruises and sometimes breaks. Getting the right treatment can be vital to recovery, but it can also be expensive. And if an accident keeps you away from work during recovery, the financial worries can grow quickly.Most major medical insurance plans only pays a portion of the bills. Our coverage can help pick up where other insurance leaves off and provide cash to help cover the expenses.
With Accident insurance from Allstate Benefits, you can gain the advantage of financial support, thanks to the cash benefits paid directly to you. You also gain the financial empowerment to seek the treatment needed to be on the mend.
Here’s How It WorksOur coverage pays you cash benefits that correspond with hospital and intensive care confinement. Your plan may also include coverage for a variety of occurrences, such as dismemberment, dislocation or fracture, ambulance services, physical therapy and more. The cash benefits can be used to help pay for deductibles, treatment, rent and more.
Meeting Your Needs• Guaranteed Issue, meaning no medical questions to answer• Benefits are paid directly to you unless otherwise assigned• Pays in addition to other insurance coverage• Coverage also available for your dependents• Premiums are affordable and are conveniently payroll deducted• Coverage may be continued; refer to your certificate for more details
With Allstate Benefits, you can protect your finances against life’s slips and falls. Are you in Good Hands? You can be.
Accident Insurance
Protection for accidental off-the-job injuries
*National Safety Council, Injury Facts®, 2014 Edition
DID YOU KNOWThe number of injuries suffered by workers in one year off-the- job includes (in millions):*
?Home
8.3Non-Auto
3.6Auto
2.0
Uintah School District
Offered to the employees of:
51

Daniel’s story of injury and treatment turned into a happy ending, because he had supplemental Accident Insurance to help with expenses.
Daniel was playing a pick-up game of basketball with his friends when he went up for a jump-shot and, on his way back down, twisted his foot and ruptured his Achilles tendon.
Here’s Daniel’s treatment path:
• Taken by ambulance to the emergency room• Examined by a doctor and X-rays were taken• Underwent surgery to reattach the tendon• Was visited by his doctor and released after a
one-day stay in the hospital• Had to immobilize his ankle for 6 weeks• Was seen by the doctor during a follow-up visit
and sent to physical therapy to strengthen his legand improve his mobility
Daniel would go online after each of his treatments to file claims. The cash benefits were direct deposited into his bank account.
Daniel is back playing basketball and enjoying life.
CHOOSE CLAIMUSEDaniel and Sandy choose benefits to help protect their family if they suffer an accidental injury.
Meet Daniel & SandyDaniel and Sandy are like most active couples: they enjoy the outdoors and a great adventure. They have seen their share of bumps, bruises and breaks. Sandy knows an accidental injury could happen to either of them. Most importantly, she worries about how they will pay for it.
Here is what weighs heavily on her mind:• Major medical will only pay a portion
of the expenses associated withinjury treatments
• They have copays they are responsiblefor until they meet their deductible
• If they miss work because of an injury,they must cover the bills, rent/mortgage,groceries and their child’s education
• If they need to seek treatment notavailable locally, they will have topay for it
Daniel’s Accident claim paid cash benefits for the following:
Ground AmbulanceMedicineEmergency Room ServicesX-raysHospitalization ConfinementDaily Hospitalization ConfinementAccident Physician’s TreatmentTendon SurgeryGeneral AnesthesiaAccident Follow-Up TreatmentPhysical Therapy (3 days/week)
For a listing of benefits and benefit amounts, see your company’s rate insert.
52
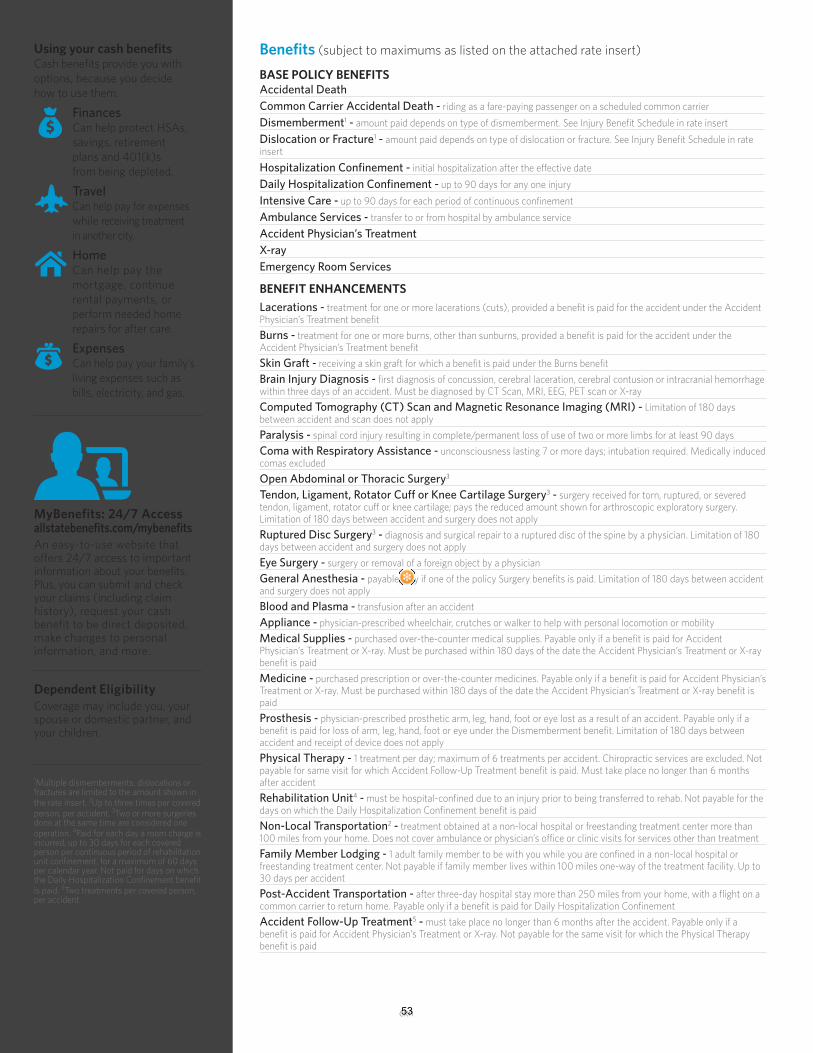
Benefits (subject to maximums as listed on the attached rate insert) Using your cash benefitsCash benefits provide you with options, because you decide how to use them.
FinancesCan help protect HSAs, savings, retirement plans and 401(k)s from being depleted.
TravelCan help pay for expenses
while receiving treatment in another city.
HomeCan help pay the mortgage, continue rental payments, or perform needed home repairs for after care.
ExpensesCan help pay your family’s living expenses such as bills, electricity, and gas.
An easy-to-use website that offers 24/7 access to important information about your benefits. Plus, you can submit and check your claims (including claim history), request your cash benefit to be direct deposited, make changes to personal information, and more.
MyBenefits: 24/7 Accessallstatebenefits.com/mybenefits
BASE POLICY BENEFITSAccidental DeathCommon Carrier Accidental Death -^ riding as a fare-paying passenger on a scheduled common carrierDismemberment1 -^ amount paid depends on type of dismemberment. See Injury Benefit Schedule in rate insertDislocation or Fracture1 -^ amount paid depends on type of dislocation or fracture. See Injury Benefit Schedule in rate insertHospitalization Confinement -^ initial hospitalization after the effective date Daily Hospitalization Confinement -^ up to 90 days for any one injury Intensive Care -^ up to 90 days for each period of continuous confinementAmbulance Services -^ transfer to or from hospital by ambulance serviceAccident Physician’s TreatmentX-rayEmergency Room Services
BENEFIT ENHANCEMENTSLacerations -^ treatment for one or more lacerations (cuts), provided a benefit is paid for the accident under the Accident Physician’s Treatment benefitBurns -^ treatment for one or more burns, other than sunburns, provided a benefit is paid for the accident under the Accident Physician’s Treatment benefitSkin Graft -^ receiving a skin graft for which a benefit is paid under the Burns benefitBrain Injury Diagnosis -^ first diagnosis of concussion, cerebral laceration, cerebral contusion or intracranial hemorrhage within three days of an accident. Must be diagnosed by CT Scan, MRI, EEG, PET scan or X-rayComputed Tomography (CT) Scan and Magnetic Resonance Imaging (MRI) -^ Limitation of 180 days between accident and scan does not applyParalysis -^ spinal cord injury resulting in complete/permanent loss of use of two or more limbs for at least 90 daysComa with Respiratory Assistance -^ unconsciousness lasting 7 or more days; intubation required. Medically induced comas excludedOpen Abdominal or Thoracic Surgery3
Tendon, Ligament, Rotator Cuff or Knee Cartilage Surgery3 -^ surgery received for torn, ruptured, or severed tendon, ligament, rotator cuff or knee cartilage; pays the reduced amount shown for arthroscopic exploratory surgery. Limitation of 180 days between accident and surgery does not applyRuptured Disc Surgery3 -^ diagnosis and surgical repair to a ruptured disc of the spine by a physician. Limitation of 180 days between accident and surgery does not applyEye Surgery -^ surgery or removal of a foreign object by a physicianGeneral Anesthesia -^ payable only if one of the policy Surgery benefits is paid. Limitation of 180 days between accident and surgery does not applyBlood and Plasma -^ transfusion after an accidentAppliance -^ physician-prescribed wheelchair, crutches or walker to help with personal locomotion or mobilityMedical Supplies -^ purchased over-the-counter medical supplies. Payable only if a benefit is paid for Accident Physician’s Treatment or X-ray. Must be purchased within 180 days of the date the Accident Physician’s Treatment or X-ray benefit is paidMedicine -^ purchased prescription or over-the-counter medicines. Payable only if a benefit is paid for Accident Physician’s Treatment or X-ray. Must be purchased within 180 days of the date the Accident Physician’s Treatment or X-ray benefit is paidProsthesis -^ physician-prescribed prosthetic arm, leg, hand, foot or eye lost as a result of an accident. Payable only if a benefit is paid for loss of arm, leg, hand, foot or eye under the Dismemberment benefit. Limitation of 180 days between accident and receipt of device does not applyPhysical Therapy -^ 1 treatment per day; maximum of 6 treatments per accident. Chiropractic services are excluded. Not payable for same visit for which Accident Follow-Up Treatment benefit is paid. Must take place no longer than 6 months after accidentRehabilitation Unit4 -^ must be hospital-confined due to an injury prior to being transferred to rehab. Not payable for the days on which the Daily Hospitalization Confinement benefit is paidNon-Local Transportation2 -^ treatment obtained at a non-local hospital or freestanding treatment center more than 100 miles from your home. Does not cover ambulance or physician’s office or clinic visits for services other than treatmentFamily Member Lodging -^ 1 adult family member to be with you while you are confined in a non-local hospital or freestanding treatment center. Not payable if family member lives within 100 miles one-way of the treatment facility. Up to 30 days per accidentPost-Accident Transportation -^ after three-day hospital stay more than 250 miles from your home, with a flight on a common carrier to return home. Payable only if a benefit is paid for Daily Hospitalization ConfinementAccident Follow-Up Treatment5 -^ must take place no longer than 6 months after the accident. Payable only if a benefit is paid for Accident Physician’s Treatment or X-ray. Not payable for the same visit for which the Physical Therapy benefit is paid
ckn
Dependent EligibilityCoverage may include you, your spouse or domestic partner, and your children.
1Multiple dismemberments, dislocations or fractures are limited to the amount shown in the rate insert. 2Up to three times per covered person, per accident. 3Two or more surgeries done at the same time are considered one operation. 4Paid for each day a room charge is incurred, up to 30 days for each covered person per continuous period of rehabilitation unit confinement, for a maximum of 60 days per calendar year. Not paid for days on which the Daily Hospitalization Confinement benefit is paid. 5Two treatments per covered person, per accident.
53

This brochure is for use in UT and is incomplete without the accompanying rate insert.This material is valid as long as information remains current, but in no event later than June 26, 2021.
Group Accident benefits are provided by policy form GVAP2, or state variations thereof. Outpatient Physician’s Benefit Rider provided by rider form GOPBR, or state variations thereof.Coverage is provided by Limited Benefit Supplemental Accident Insurance. The policy is not a Medicare Supplement Policy. If eligible for Medicare, review Medicare Supplement Buyer’s Guide available from Allstate Benefits. This information highlights some features of the policy but is not the insurance contract. For complete details, contact your Allstate Benefits Agent. This is a brief overview of the benefits available under the Group Voluntary Policy underwritten by American Heritage Life Insurance Company (Home Office, Jacksonville, FL). Details of the insurance, including exclusions, restrictions and other provisions are included in the certificates issued.The coverage does not constitute comprehensive health insurance coverage (often referred to as “major medical coverage”) and does not satisfy the requirement of minimum essential coverage under the Affordable Care Act.
Allstate Benefits is the marketing name used by American Heritage Life Insurance Company, a subsidiary of The Allstate Corporation. ©2018 Allstate Insurance Company. www.allstate.com or allstatebenefits.com
CERTIFICATE SPECIFICATIONSConditions and Limits ^When an injury results in a covered loss within 180 days (unless otherwise stated on the Benefits page) from the date of an accident and is diagnosed by a physician, Allstate Benefits will pay benefits as stated. Treatment must be received in the United States or its territories.
Eligibility ^Your employer decides who is eligible for your group (such as length of service and hours worked each week).
Dependent Eligibility/Termination ^Coverage may include you, your spouse or domestic partner, and your children. Coverage for children ends when the child reaches age 26, unless he or she continues to meet the requirements of an eligible dependent. Spouse coverage ends upon valid decree of divorce or your death. Domestic partner coverage ends upon termination of the domestic partnership or your death.
When Coverage Ends ^Coverage under the policy and riders (if included) ends on the earliest of: the date the policy or certificate is canceled; the last day of the period for which you made any required contributions; the last day you are in active employment, except as provided under the Temporary Layoff, Leave of Absence, or Family and Medical Leave of Absence provision; the date you are no longer in an eligible class; the date your class is no longer eligible; or discovery of fraud or material misrepresentation when filing a claim.
Continuing Your Coverage ^You may be eligible to continue your coverage when coverage under the policy ends. Refer to your Certificate of Insurance for details.
EXCLUSIONS AND LIMITATIONSExclusions and Limitations for the Base Policy:^ Benefits are not paid for: injury incurred before the effective date; injury as a result of an on-the-job accident; act of war or voluntary participation in a riot, insurrection or rebellion; suicide or attempt at suicide; intentionally self-inflicted injury or action; injury while under the influence of alcohol or any narcotic, unless taken upon the advice of a physician, if the use of alcohol or any narcotic substantially contributes to or causes the accident or is over the legal limit; any bacterial infection (except pyogenic infections from an accidental cut or wound); participation in aeronautics unless a fare-paying passenger on a licensed common-carrier aircraft; engaging in an illegal occupation or committing or attempting an assault or felony; driving in any race or speed test or testing any vehicle on any racetrack or speedway; hernia, including complications; serving as an active member of the Military, Naval, or Air Forces of any country or combination of countries.
Exclusions and Limitations for Outpatient Physician’s Benefit Rider ^Benefits are not paid for: a loss incurred before the effective date; a loss occurring from an on-the-job accident; act of war or voluntary participation in a riot, insurrection or rebellion; suicide or attempt at suicide; intentionally self-inflicted injury or action; any loss while under the influence of alcohol or any narcotic, unless taken upon the advice of a physician, if the use of alcohol or any narcotic substantially contributes to or causes the accident or is over the legal limit; participation in aeronautics unless a fare-paying passenger on a licensed common-carrier aircraft; engaging in an illegal occupation or committing or attempting an assault or felony; driving in any race or speed test or testing an automobile or any vehicle on any racetrack or speedway; serving as an active member of the Military, Naval, or Air Forces of any country or combination of countries.
54

BE
NE
FIT
EN
HA
NC
EM
EN
TS
PL
AN
1P
LA
N 2
La
ce
rati
on
s (P
ay
s o
nc
e/
ye
ar)
$5
0$
50
Bu
rns
(oth
er
tha
n s
un
bu
rns)
<
15
% b
od
y s
urf
ac
e$
100
$10
0
Off
ere
d t
o t
he
em
plo
ye
es
of:
> 1
5%
or
mo
re$
50
0$
50
0
Sk
in G
raft
(%
of
Bu
rns
Be
ne
fit)
50
%
50
%
Bra
in I
nju
ry D
iag
no
sis
(Pa
ys
on
ce
)$
150
$15
0
Pa
raly
sis
(Pa
ys
on
ce
)P
ara
ple
gia
$7
,50
0$
7,5
00
Qu
ad
rip
leg
ia$
15,0
00
$15
,00
0
PL
AN
1P
LA
N 2
Co
ma
wit
h R
esp
ira
tory
Ass
ista
nc
e (
Pa
ys
on
ce
)$
10,0
00
$10
,00
0
Emp
loye
e$
40
,00
0$
60
,00
0O
pe
n A
bd
om
ina
l o
r T
ho
rac
ic S
urg
ery
$1,
00
0$
1,0
00
Spo
use
$2
0,0
00
$3
0,0
00
Te
nd
on
, Lig
am
en
t, R
ota
tor
Cu
ffS
urg
ery
$5
00
$5
00
Ch
ildre
n$
10,0
00
$15
,00
0o
r K
ne
e C
art
ila
ge
Su
rge
ryE
xp
lora
tory
$15
0$
150
Emp
loye
e$
20
0,0
00
$3
00
,00
0R
up
ture
d S
pin
al
Dis
c S
urg
ery
$5
00
$5
00
(far
e-p
ayin
g p
asse
nge
r)Sp
ou
se$
100
,00
0$
150
,00
0E
ye
Su
rge
ry$
100
$10
0
Ch
ildre
n$
50
,00
0$
75
,00
0G
en
era
l A
ne
sth
esi
a$
100
$10
0
Emp
loye
e$
40
,00
0
$6
0,0
00
B
loo
d a
nd
Pla
sma
$
30
0$
30
0
Spo
use
$2
0,0
00
$
30
,00
0
Ap
pli
an
ce
$12
5$
125
Ch
ildre
n$
10,0
00
$
15,0
00
M
ed
ica
l S
up
pli
es
$5
$5
Emp
loye
e$
4,0
00
$
6,0
00
M
ed
icin
e$
5$
5
Spo
use
$2
,00
0
$3
,00
0
Pro
sth
esi
s 1
de
vic
e$
50
0$
50
0
Ch
ildre
n$
1,0
00
$
1,5
00
2
or
mo
re d
ev
ice
s$
1,0
00
$1,
00
0
$1,
00
0$
1,5
00
Ph
ysi
ca
l T
he
rap
y (
Pa
ys
da
ily
; ma
x. 6
da
ys/
ac
cid
en
t)$
30
$3
0
$2
00
$3
00
Re
ha
bil
ita
tio
n U
nit
(P
ay
s d
ail
y)
$10
0$
100
$4
00
$6
00
No
n-L
oc
al
Tra
nsp
ort
ati
on
$4
00
$4
00
Gro
un
d$
20
0$
30
0F
am
ily
Me
mb
er
Lo
dg
ing
$10
0$
100
Air
$6
00
$9
00
Po
st-A
cc
ide
nt
Tra
nsp
ort
ati
on
(P
ay
s o
nc
e/
ye
ar)
$2
00
$2
00
Acc
iden
t P
hys
icia
n’s
Tre
atm
ent
$10
0$
150
Ac
cid
en
t F
oll
ow
-Up
Tre
atm
en
t$
50
$5
0
$2
00
$3
00
AD
DIT
ION
AL
RID
ER
BE
NE
FIT
PL
AN
1P
LA
N 2
Emer
gen
cy R
oo
m S
ervi
ces
$2
00
$3
00
Ou
tpa
tie
nt
Ph
ysi
cia
n’s
Be
ne
fit
$5
0$
100
Gro
up
Vo
lun
tary
Ac
cid
en
t (G
VA
P2
)
¹Up
to
am
ou
nt
sho
wn
; act
ual
am
ou
nt
pai
d d
epen
ds
on
inju
ry a
nd
is b
ased
on
Sch
edu
le o
f
Ben
efit
s an
d F
acto
rs in
yo
ur
cert
ific
ate
of
cove
rage
. M
ult
iple
loss
es f
rom
sam
e in
jury
pay
on
ly u
p t
o a
mo
un
t sh
ow
n a
bo
ve.
X-R
ay
Co
mp
ute
d T
om
og
rap
hy
(C
T)
Sc
an
an
d M
ag
ne
tic
Re
son
an
ce
Im
ag
ing
(M
RI)
$5
0
Off
-th
e-J
ob
Ac
cid
en
t In
su
ran
ce
fro
m A
llst
ate
Be
ne
fits
Se
e a
tta
ch
ed
Im
po
rta
nt
info
rma
tio
n A
bo
ut
Co
ve
rag
e.
Uin
tah
Scho
ol D
istr
ict
BE
NE
FIT
AM
OU
NT
S
Be
ne
fits
are
pa
id o
nc
e p
er
ac
cid
en
t u
nle
ss o
the
rwis
e n
ote
d h
ere
or
in t
he
Im
po
rta
nt
Info
rma
tio
n A
bo
ut
Co
ve
rag
e.
Acc
iden
tal D
eath
$5
0
Co
mm
on
Car
rier
Acc
iden
tal D
eath
Dis
mem
ber
men
t¹
Dis
loca
tio
n o
r Fr
actu
re¹
BA
SE
AC
CID
EN
T B
EN
EF
ITS
Am
bu
lan
ce
Inte
nsi
ve C
are
(Pay
s d
aily
)
Ho
spit
al C
on
fin
emen
t (P
ays
on
ce/y
ear)
Dai
ly H
osp
ital
Co
nfi
nem
ent
(Pay
s d
aily
)
55
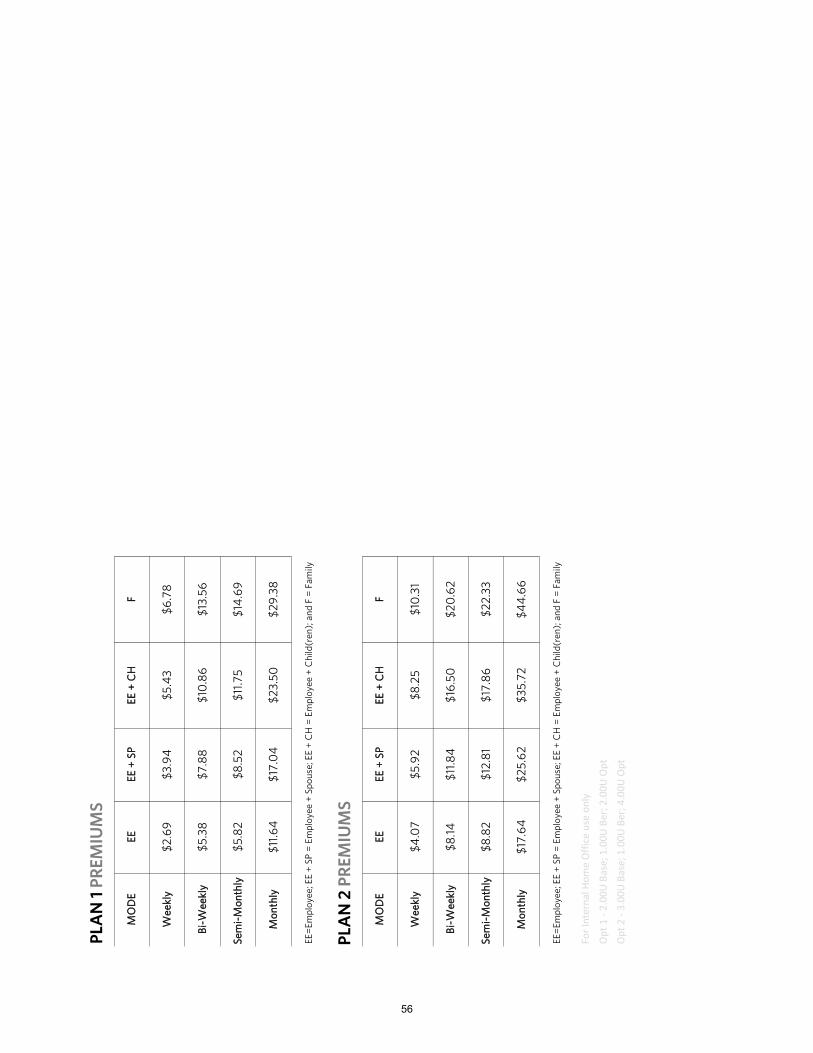
For
Inte
rnal
Ho
me
Off
ice
use
on
ly
Op
t 1
- 2
.00
U B
ase;
1.0
0U
Ber
; 2.0
0U
Op
t
Op
t 2
- 3
.00
U B
ase;
1.0
0U
Ber
; 4.0
0U
Op
t
Mo
nth
ly$
11.6
4$
17.0
4$
23
.50
$2
9.3
8
EE
=E
mp
loy
ee
; E
E +
SP
= E
mp
loy
ee
+ S
po
use
; E
E +
CH
= E
mp
loy
ee
+ C
hil
d(r
en
); a
nd
F =
Fa
mil
y
F
$13
.56
Se
mi-
Mo
nth
ly
$5
.82
EE
MO
DE
$14
.69
$10
.86
$6
.78
$8
.52
$11
.75
$7
.88
EE
+ C
HE
E +
SP
PL
AN
1 P
RE
MIU
MS
$5
.38
Bi-
We
ek
ly
$5
.43
$3
.94
$2
.69
We
ek
ly
PL
AN
2 P
RE
MIU
MS
MO
DE
EE
EE
+ S
PE
E +
CH
F
We
ek
ly$
4.0
7$
5.9
2$
8.2
5$
10.3
1
Mo
nth
ly$
17.6
4$
25
.62
$3
5.7
2$
44
.66
EE
=E
mp
loy
ee
; E
E +
SP
= E
mp
loy
ee
+ S
po
use
; E
E +
CH
= E
mp
loy
ee
+ C
hil
d(r
en
); a
nd
F =
Fa
mil
y
Bi-
We
ek
ly$
8.1
4$
11.8
4$
16.5
0$
20
.62
Se
mi-
Mo
nth
ly
$8
.82
$12
.81
$17
.86
$2
2.3
3
56
No one is ever really prepared for a life-altering critical illness diagnosis. The whirlwind of appointments, tests, treatments and medications can add to your stress levels.The treatment to recovery is vital, but it can also be expensive. Your medical coverage may only cover some of the costs associated with treatment. You’re still responsible for deductibles and coinsurance. If treatment keeps you out of work, the financial worries can grow quickly and stress levels may rise.
Critical Illness coverage helps provide financial support if you are diagnosed with a covered critical illness. With the expense of treatment often high, seeking the treatment you need could seem like a financial burden. When a diagnosis occurs, you need to be focused on getting better and taking control of your health, not stressing over financial worries.
Here’s How It WorksYou choose benefits to protect yourself and any family members if diagnosed with a critical illness. Then, if diagnosed with a covered critical illness, you will receive a cash benefit based on the percentage payable for the condition.
Meeting Your Needs• Guaranteed Issue, meaning no medical questions to answer at initial enrollment• Coverage available for dependents• Covered dependents receive 50% of your Basic-Benefit Amount• Benefits paid regardless of any other medical or disability plan coverage• Premiums are affordable and conveniently payroll deducted• Coverage may be continued; refer to your certificate for more details
With Allstate Benefits, you can make treatment decisions without putting your finances at risk. Are you in Good Hands? You can be.
1https://www.cdc.gov/heartdisease/heart_attack.htm2https://www.cdc.gov/stroke/facts.htm
Critical Illness Insurance
Protection when faced with a critical illness diagnosis and you need treatment
DID YOU KNOW ?
Every 40 seconds,an American will suffera heart attack1
Every 40 seconds,someone in the U.S. has a stroke2
Uintah School District
Offered to the employees of:
57
Ashley’s story of diagnosis and treatment turned into a happy ending, because she had supplemental Critical Illness Insurance to help with expenses.
During Ashley’s annual wellness exam, her doctor noticed an irregular heartbeat. She underwent an electrocardiogram (EKG) test and stress test, which confirmed she had a blockage in one of her coronary arteries.
Here’s Ashley’s treatment path:• Ashley has her annual wellness exam• Her doctor notices an abnormality in her
heartbeat; tests are performed and she isdiagnosed with coronary artery disease
• After visits with doctors, surgeons and ananesthesiologist, Ashley undergoes surgery
• Surgery is performed to remove the blockagewith a bypass graft. She is visited by her doctorduring a 4-day hospital stay and released
• Ashley followed her doctor required treatment during a 2-month recovery period, and had regular doctor office visits
Ashley is doing well and is on the road to recovery.
CHOOSE CLAIMUSEAshley chooses Critical Illness benefits and rider benefits to helpprotect her and her children, if they are diagnosed with a critical illness.
Meet AshleyAshley is like any single parent who has been diagnosed with a critical illness. She’s worried about her future, her children and how they will cope with her treatments. Most importantly, she worries about how she will pay for it all.Here is what weighs heavily on her mind:• Major medical only pays a portion of the
expenses associated with my treatment• I have copays I am responsible for
until I meet my deductible• If I am not working due to my
treatments, I must cover my bills, rent/mortgage, groceries and my children’s education
• If the right treatment is not availablelocally, I will have to travel to get the treatment I need
Ashley’s Critical Illness claim paid her cash benefits for the following:
Wellness
Coronary Artery Bypass Surgery
The cash benefits were direct deposited into her bank account.
For a listing of benefits and benefit amounts, see your company’s rate insert.
58

Using your cash benefitsCash benefits provide you with options, because you decide how to use them.
FinancesCan help protect HSAs, savings, retirement plans and 401(k)s from being depleted.
TravelCan help pay for expenses
while receiving treatment in another city.
HomeCan help pay the mortgage, continue rental payments, or perform needed home repairs for after care.
ExpensesCan help pay your family’s living expenses such as bills, electricity, and gas.
An easy-to-use website that offers 24/7 access to important information about your benefits. Plus, you can submit and check your claims (including claim history), request your cash benefit to be direct deposited, make changes to personal information, and more.
MyBenefits: 24/7 Accessallstatebenefits.com/mybenefits
Benefits (subject to maximums as listed on the attached rate insert)
Benefit paid upon diagnosis of one of the following conditionsINITIAL CRITICAL ILLNESS BENEFITS*Heart Attack -^ the death of a portion of the heart muscle due to inadequate blood supply. Established (old) myocardial infarction and cardiac arrest are not coveredStroke -^ the death of a portion of the brain producing neurological sequelae including infarction of brain tissue, hemorrhage and embolization from an extra-cranial source. Transient ischemic attacks (TIAs), head injury, chronic cerebrovascular insufficiency and reversible ischemic neurological deficits are not coveredMajor Organ Transplant -^ transplant of heart, lung, liver, pancreas or kidneys. Transplanted organ must come from a human donorEnd Stage Renal Failure -^ irreversible failure of both kidneys, resulting in peritoneal dialysis or hemodialysis. Renal failure caused by traumatic events, including surgical trauma, are not coveredCoronary Artery Bypass Surgery -^ to correct narrowing or blockage of one or more coronary arteries with bypass graft. Abdominal aortic bypass, balloon angioplasty, laser embolectomy, atherectomy, stent placement and non-surgical procedures are not coveredWaiver of Premium (Employee only) -^ premiums waived if disabled for 90 consecutive days due to a critical illness
CANCER CRITICAL ILLNESS BENEFITS*Invasive Cancer -^ malignant tumor with uncontrolled growth, including Leukemia and Lymphoma. Carcinoma in situ, non-invasive or metastasized skin cancer and early prostate cancer are not coveredCarcinoma In Situ -^ non-invasive cancer, including early prostate cancer (stages A, I, II) and melanoma that has not invaded the dermis. Other skin malignancies, pre-malignant lesions (such as intraepithelial neoplasia), benign tumors and polyps are not covered
SECOND EVENT BENEFIT*Second Event Initial Critical Illness -^ second diagnosis more than 12 months after the first date of diagnosis for which an Initial Critical Illness benefit was paid
OPTIONAL/ADDITIONAL BENEFITWellness -^ 23 exams. Once per person, per calendar year; see left for list of wellness services and tests
*Benefits paid once per covered person. When all benefits have been used, the coverage terminates.
Wellness -^ Biopsy for skin cancer; Bone Marrow Testing; Blood tests for triglycerides, CA15-3 (breast cancer), CA125 (ovarian cancer), CEA (colon cancer), PSA (prostate cancer); Chest X-ray; Colonoscopy; Doppler screening for carotids or peripheral vascular disease; Echocardiogram; EKG; Flexible sigmoidoscopy; Hemoccult stool analysis; HPV (Human Papillomavirus) Vaccination; Lipid panel (total cholesterol count); Mammography, including Breast Ultrasound; Pap Smear, including ThinPrep Pap Test; Serum Protein Electrophoresis (test for myeloma); Stress test on bike or treadmill; Thermography; Ultrasound screening for abdominal aortic aneurysms.
59
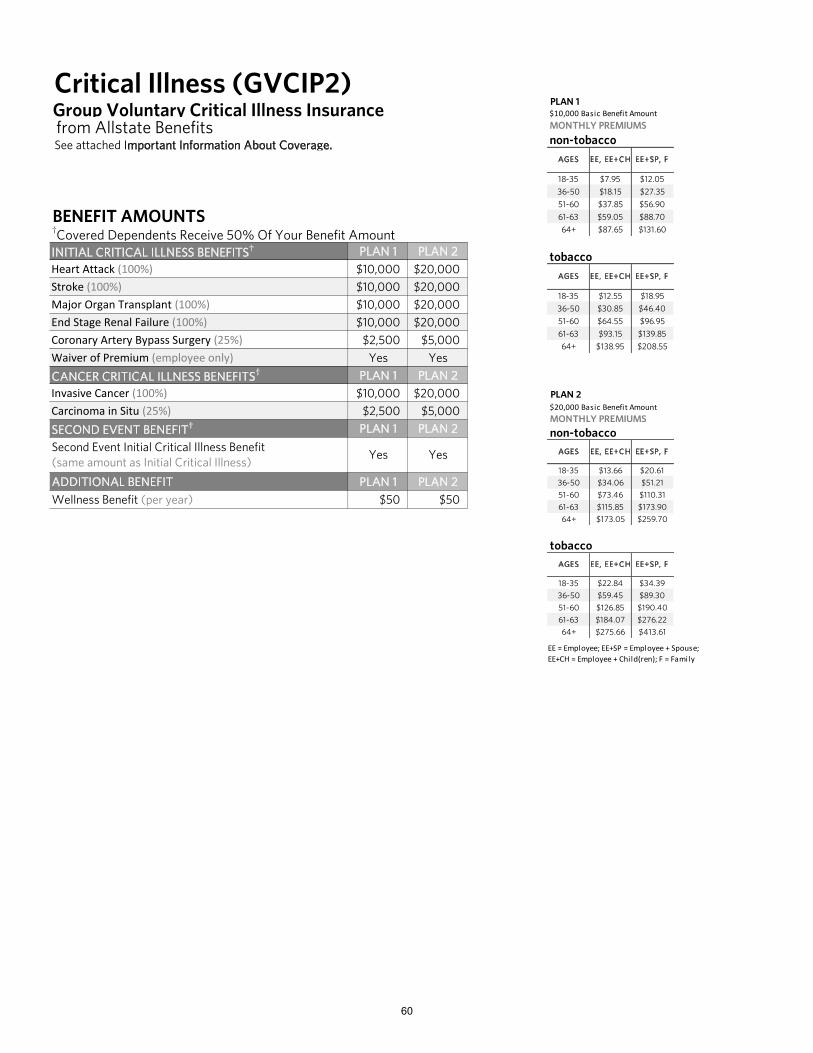
Group Voluntary Critical Illness Insurance from Allstate Benefits See attached Important Information About Coverage.
BENEFIT AMOUNTS†Covered Dependents Receive 50% Of Your Benefit AmountINITIAL CRITICAL ILLNESS BENEFITS† PLAN 1 PLAN 2Heart Attack (100%) $10,000 $20,000Stroke (100%) $10,000 $20,000Major Organ Transplant (100%) $10,000 $20,000End Stage Renal Failure (100%) $10,000 $20,000Coronary Artery Bypass Surgery (25%) $2,500 $5,000Waiver of Premium (employee only) Yes Yes
CANCER CRITICAL ILLNESS BENEFITS† PLAN 1 PLAN 2Invasive Cancer (100%) $10,000 $20,000Carcinoma in Situ (25%) $2,500 $5,000
SECOND EVENT BENEFIT† PLAN 1 PLAN 2
ADDITIONAL BENEFIT PLAN 1 PLAN 2
Wellness Benefit (per year) $50 $50
Critical Illness (GVCIP2)
Second Event Initial Critical Illness Benefit(same amount as Initial Critical Illness)
Yes Yes
PLAN 2 $20,000 Basic Benefit AmountMONTHLY PREMIUMS
non-tobacco
18-35 $13.66 $20.61
36-50 $34.06 $51.21
51-60 $73.46 $110.31
61-63 $115.85 $173.90
64+ $173.05 $259.70
tobacco
18-35 $22.84 $34.39
36-50 $59.45 $89.30
51-60 $126.85 $190.40
61-63 $184.07 $276.22
64+ $275.66 $413.61
EE = Employee; EE+SP = Employee + Spouse;EE+CH = Employee + Child(ren); F = Family
EE, EE+CH EE+SP, F
EE+SP, FAGES EE, EE+CH
AGES
PLAN 1 $10,000 Basic Benefit AmountMONTHLY PREMIUMS
non-tobacco
18-35 $7.95 $12.05
36-50 $18.15 $27.35
51-60 $37.85 $56.90
61-63 $59.05 $88.70
64+ $87.65 $131.60
tobacco
18-35 $12.55 $18.95
36-50 $30.85 $46.40
51-60 $64.55 $96.95
61-63 $93.15 $139.85
64+ $138.95 $208.55
EE+SP, FAGES EE, EE+CH
AGES EE, EE+CH EE+SP, F
60
Protect your family’s privacy, identity, and finances with PrivacyArmor® Plus
For more information:
Comprehensive identity monitoringOur proprietary monitoring platform detects high-risk activity to alert you at the first sign of fraud. We scour the dark web for compromised credentials and monitor financial transactions, all while keeping tabs on your credit reports.
Fraud remediation and restorationShould identity theft or fraud occur, you have a dedicated Privacy Advocate® to fully manage your recovery and restore your identity. And since fraud doesn’t take a holiday, our Privacy Advocates are available 24/7.
Identity theft reimbursementYou never have to worry about covering the costs of identity theft. PrivacyArmor Plus’ $1 million identity theft insurance policy† covers any out-of-pocket expenses, lost wages, or legal fees. Plus, we’ll reimburse funds stolen from your bank, HSA, or 401(k) accounts.
14.4 million Americans experienced identity fraud in 20181
MyPrivacyArmor.com
Questions? 1.800.789.2720
Plans and pricing$9.95 per person / month$17.95 per family / month
61

Enroll Access to your full PrivacyArmor Plus capabilities begins on your effective date.
We monitorOur advanced technology looks for suspicious activity associated with your personal profile.
We alert We alert you to any activity associated with your account.
We restore In the event of identity theft, we fully manage the process of recovering your identity, credit, and sense of security so the impact to your life is minimal.
We reimburse Our $1 million identity theft insurance policy covers the costs associated with reinstating your identity.†
1 4
52
3
How it works
The most extensive identity protection plan available
Identity and credit monitoring
Tri-bureau credit alerts
Unlimited credit reports from TransUnion
Dark web monitoring
Financial transaction monitoring
Social media reputation monitoring
Accounts secured with two-factor authentication
24/7 Privacy Advocate remediation
$1 million identity theft insurance policy
401(k) and HSA stolen fund reimbursement
Tax fraud refund advances
For More Information:
Starting on your PrivacyArmor Plus effective date, you will automatically be covered with:
Identity monitoring and alerts
24/7 Privacy Advocate® support
$1 million identity theft insurance policy†
MyPrivacyArmor.com
Questions? 1.800.789.2720
Plans and pricing$9.95 per person / month$17.95 per family / month
62
Employee AssistanceProgram
EmployeeConnect through Lincoln Financial
63
Employee Assistance Program Services
Confidential help 24 hours a day, 7 days a week for employees and family members
Visit www.Lincoln4Benefits.com or www.GuidanceResources.com (user name = LFGsupport; password = LFGsupport1). Or talk with a specialist at 888-628-4824.
EmployeeConnect SM
Family
Parenting
Addictions
Emotional
Legal
Financial
Relationships
Stress
Employee Assistance Program Services
Confidential help 24 hours a day, 7 days a week for employees and family members
Visit www.Lincoln4Benefits.com or www.GuidanceResources.com (user name = LFGsupport; password = LFGsupport1). Or talk with a specialist at 888-628-4824.
EmployeeConnect SM
Family
Parenting
Addictions
Emotional
Legal
Financial
Relationships
Stress
Life has its share of ups and downs — and sometimes you may need a little guidance through the “downs.” EmployeeConnectSM services included with your long-term disability insurance offer an array of confidential services to help you and your loved ones meet the challenges that life, work, and relationships can bring.
Your EmployeeConnectSM benefitsUnlimited 24/7 assistance You can access the following services anytime, online or with a toll-free call:• Information, resources, and referrals on family matters, such as child and elder care; kennels and pet care; event and
vacation planning; moving and relocation; car buying; college planning; and more• Legal information and referrals for situations requiring expertise in family law, estate planning, landlord/tenant relations,
consumer and civil law, and more• Guidance with financial matters, including household budgeting, and short- and long-term planning
In-person guidance Some matters are best resolved by meeting with a professional in person. With EmployeeConnect, you get:• In-person help for short-term issues (up to four* sessions with a counselor per person, per issue, per year)• In-person consultations with network lawyers, including one free 30-minute in-person consultation per legal issue, and
subsequent meetings at a reduced fee
Online resources EmployeeConnect offers a wide range of information and resources that you can research and access on your own just by visiting GuidanceResources.com. You’ll find:• Articles and tutorials• Streaming videos• Interactive tools — including financial calculators, budgeting spreadsheets, and a language translator
The resources you need to meet life’s challenges.
!
This card is your connection to real support for real-life issues.Cut out and keep it with you at all times.
*In California, up to three sessions in six months, starting with initial contact by employee.
64

EmployeeConnectSM is marketed by Lincoln Financial Group. Services are provided by ComPsych® Corporation, Chicago, IL.
EmployeeConnectSM is marketed by Lincoln Financial Group. Services are provided by ComPsych® Corporation, Chicago, IL.
EmployeeConnectSM counselors are experienced and credentialedWhen you call our toll-free line, you’ll talk to an experienced professional who will provide counseling, work-life advice, and referrals. All counselors hold master’s degrees, with broad-based clinical skills and at least three years of experience in counseling on a variety of issues. For face-to-face meetings, you will be referred to a fully credentialed, state-licensed clinician.
You’ll receive a customized information packet for each of the work-life services you use.
To take advantage of the EmployeeConnectSM program, or for more information:
Visit www.GuidanceResources.com or call 888-628-4824.
EmployeeConnectSM services are provided by ComPsych® Corporation, Chicago, IL. ComPsych® and GuidanceResources® are registered trademarks of ComPsych® Corporation. ComPsych® is not a Lincoln Financial Group® company. Coverage is subject to actual contract language. Each independent company is solely responsible for its own obligations.
Insurance products (policy series GL3001) are issued by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicit business in New York, nor is it licensed to do so. In New York, insurance products (policy series GL3001) are issued by Lincoln Life & Annuity Company of New York (Syracuse, NY). Both are Lincoln Financial Group® companies. Product availability and/or features may vary by state. Limitations and exclusions apply.
65
Premiums
66
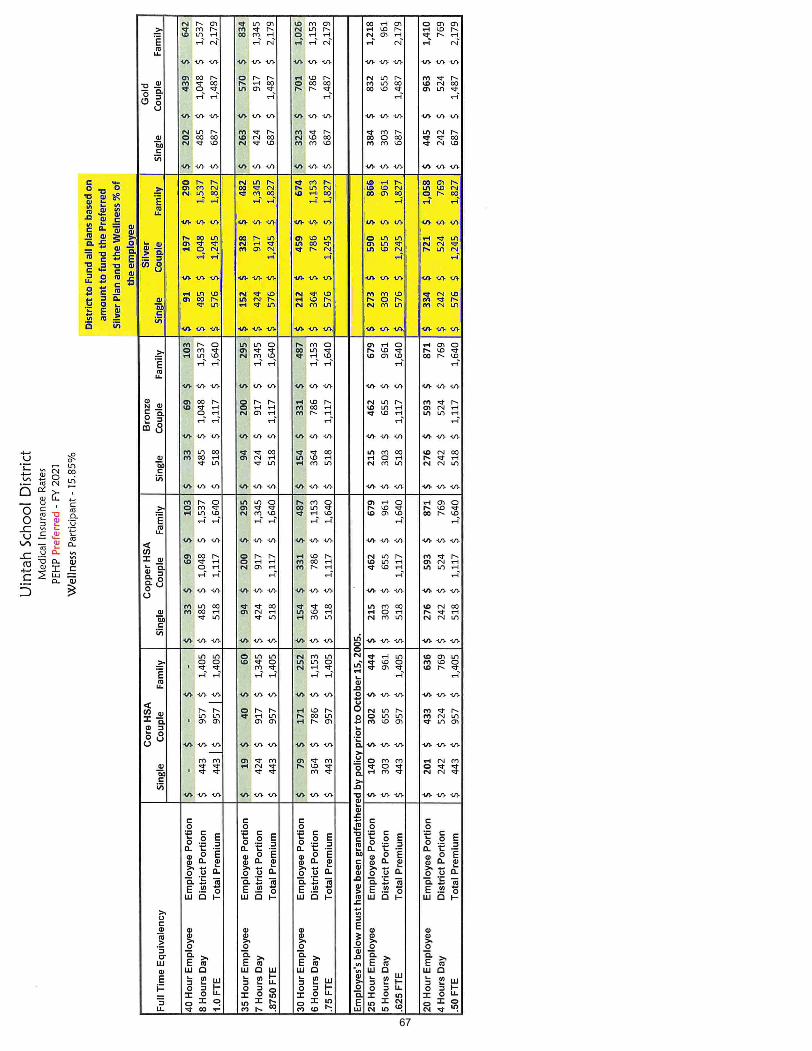
67
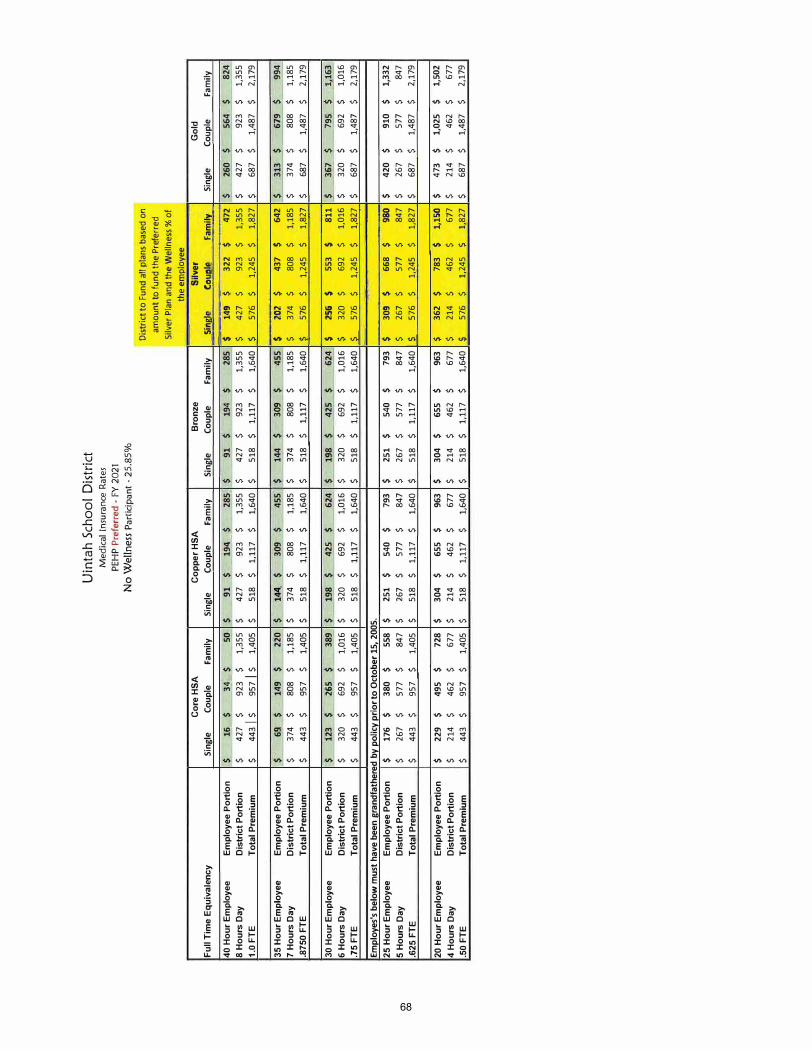
Cor
e H
SA
Full
Tim
e Eq
uiva
lenc
y Si
ngle
Co
uple
Fa
mily
40 H
our
Empl
oyee
Em
ploy
ee P
ortio
n ,$
16
_$
34_
.. $
so
$ 8
Hou
rs D
ay
Dis
tric
t Port
ion
$
427
$
923
$
1,35
5 $
1.0
FTE
Tota
l Pre
miu
m
$
443
Is
957
Is
1,40
5 $
35 H
our E
mpl
oyee
E
mpl
oyee
Por
tion
$ 69
_$
.149
$
220
$ 7
Hou
rs D
ay
Dis
tric
t Port
ion
$ 37
4 $
808
$ 1,
185
$ .8
750
FTE
Tota
l Pre
miu
m
$ 44
3 $
957
$ 1,
405
$
30 H
our
Empl
oyee
E
mpl
oyee
Por
tion
$ 12
3 $
265
$ 38
9 $
6 H
ours
Day
D
istr
ict P
ortio
n $
320
$ 69
2 $
1,01
6 $
.75
FTE
Tota
l Pre
miu
m
$
443
$ 95
7 $
1,40
5 $
Empl
oyes
's b
elow
mus
t ha
ve b
een
gran
dfat
here
d by
pol
icy
prio
r to
Oct
ober
15,
200
5.
25 H
our
Em
ploy
ee
Em
ploy
ee P
ortio
n $
176
$ 38
0 $
558
$
5 H
ours
Day
D
istr
ict P
ortio
n $
267
$ 57
7 $
847
$ .6
25F
TE
Tota
l Pre
miu
m
$ 44
3 $
957
$ 1,
405
$
20 H
our
Em
ploy
ee
Em
ploy
ee P
ortio
n $
229
$ 49
5 $
728
$ 4
Hou
rs D
ay
Dis
tric
t Port
ion
$ 21
4 $
462
$ 67
7 $
.50
FTE
Tota
l Pre
miu
m
$ 44
3 $
957
$ 1,
405
$
Sing
le
Uin
tah
Sch
oo
l D
istr
ict
Med
ical
Insu
ran
ce R
ates
PE
HP
Pref
erre
d -
FY 2
021
No
Wel
lnes
s Pa
rtic
ipan
t -2
5.85
%
Cop
per
HSA
Co
uple
Fa
mily
Si
ngle
91
$ 19
4_$
285,
$
91
$ 42
7 $
923
$ 1,
355
$ 42
7 $
518
$ 1,
117
$ 1,
640
$
518
$
144.
$
309
$
455
. $
144
$ 37
4 $
808
$ 1,
185
$
374
$ 51
8 $
1,11
7 $
1,64
0 $
518
$
198
$ 42
5 $
624
$ 19
8 $
320
$ 69
2 $
1,01
6 $
320
$ 51
8 $
1,11
7 $
1,64
0 $
518
$
251
$ 54
0 $
793
$ 25
1 $
267
$ 57
7 $
847
$ 26
7 $
518
$ 1,
117
$ 1,
640
$ 51
8 $
304
$65
5 $
963
$ 30
4 $
214
$ 46
2 $
677
$ 21
4 $
518
$
1,11
7 $
1,64
0 $
518
$
Bro
nze
Coup
le
Fam
ily
194
$ 28
5 92
3 $
1,35
5 1,
117
$
1,64
0
309
$ 45
5 80
8 $
1,18
5 1,
117
$ 1,
640
425
$ 62
4 69
2 $
1,01
6 1,
117
$ 1,
640
540
$ 79
3 57
7 $
847
1,11
7 $
1,64
0
655
$ 96
3 46
2 $
677
1,11
7 $
1,64
0
Dist
rict t
o F
und
all p
lans
bas
ed o
n am
ount
to fu
nd th
e Pr
efer
red
Silv
er P
lan
and
the
Wel
lnes
s% o
f th
e em
ploy
ee
Silv
er
Sin�
C_
ou�
.
Fam
ily
$ 14
9 $,
32
2 $
472
$ $
427
$
923
$ 1,
355
$
$ 57
6 $
1,24
5 $
1,82
7 $
$
202
$
437
$64
2 $
$ 37
4 $
808
$ 1,
185
$ l
576
$ 1,
245
$ 1,
827
$
$
25
6
$
553
$
811
$ $
320
$ 69
2 $
1,01
6 $
2-.__
576
$
1,24
5 $
1,82
7 $
$
309
$
668
$ 980
$ $
267
$
577
$
847
$
2-57
6 $
1,24
5 $
1,82
7$
$
362
$ 78
3 $
1,15
0 $
$ 21
4 $
462
$ 67
7 $
s
576
$
1,24
5 $
1,82
7 $
Gol
d Si
ngle
Co
uple
Fa
mily
260
$56
4 $
824
427
$ 92
3 $
1,35
5 68
7 $
1,48
7 $
2,17
9
313
$ 67
9 $
994
374
$ 80
8 $
1,18
5 68
7 $
1,48
7 $
2,17
9
367
$
795
$
1,16
3 32
0 $
692
$
1,01
6 68
7 $
1,48
7 $
2,17
9
420
$ 91
0 $
1,33
2 26
7 $
577
$
847
687
$ 1,
487
$ 2,
179
473
$ 1,
025
$ 1,
502
214
$ 46
2 $
677
687
$ 1,
487
$
2,17
9
68
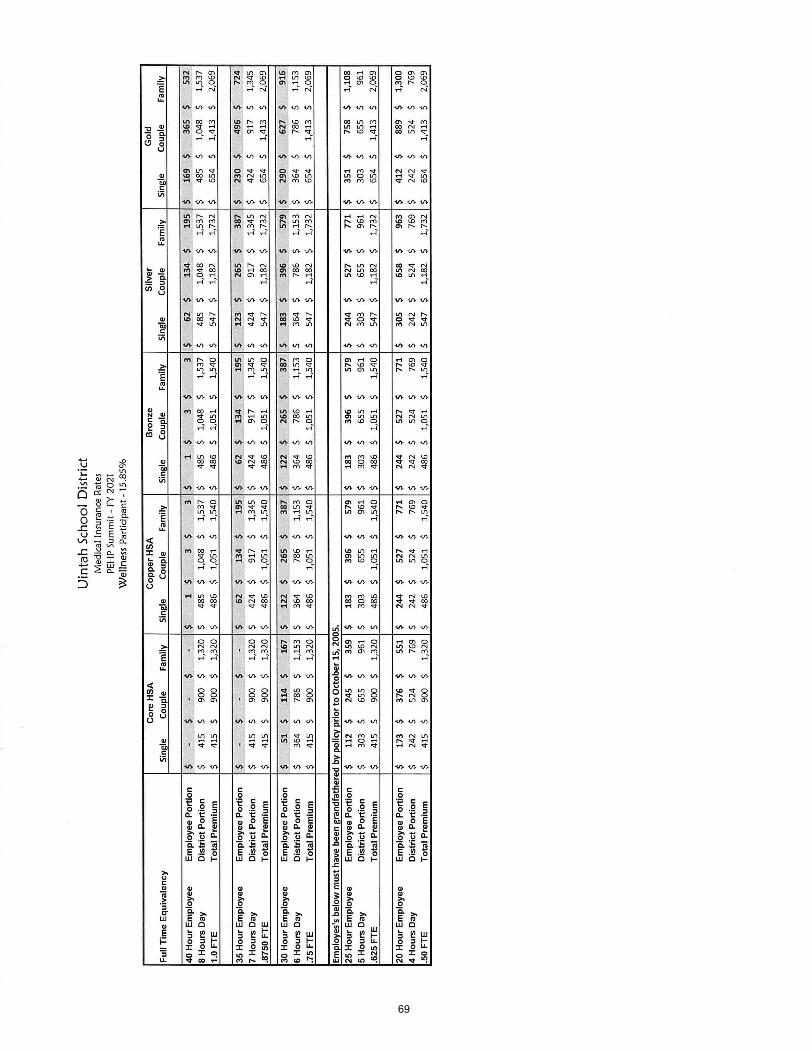
69
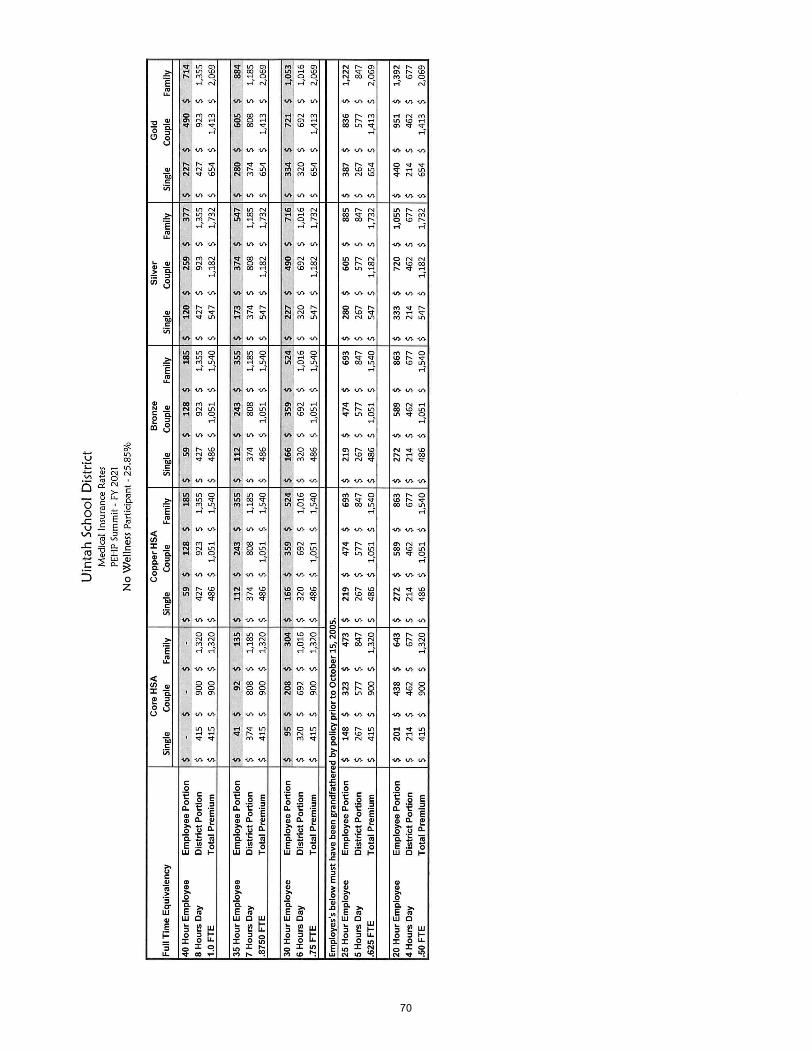
70
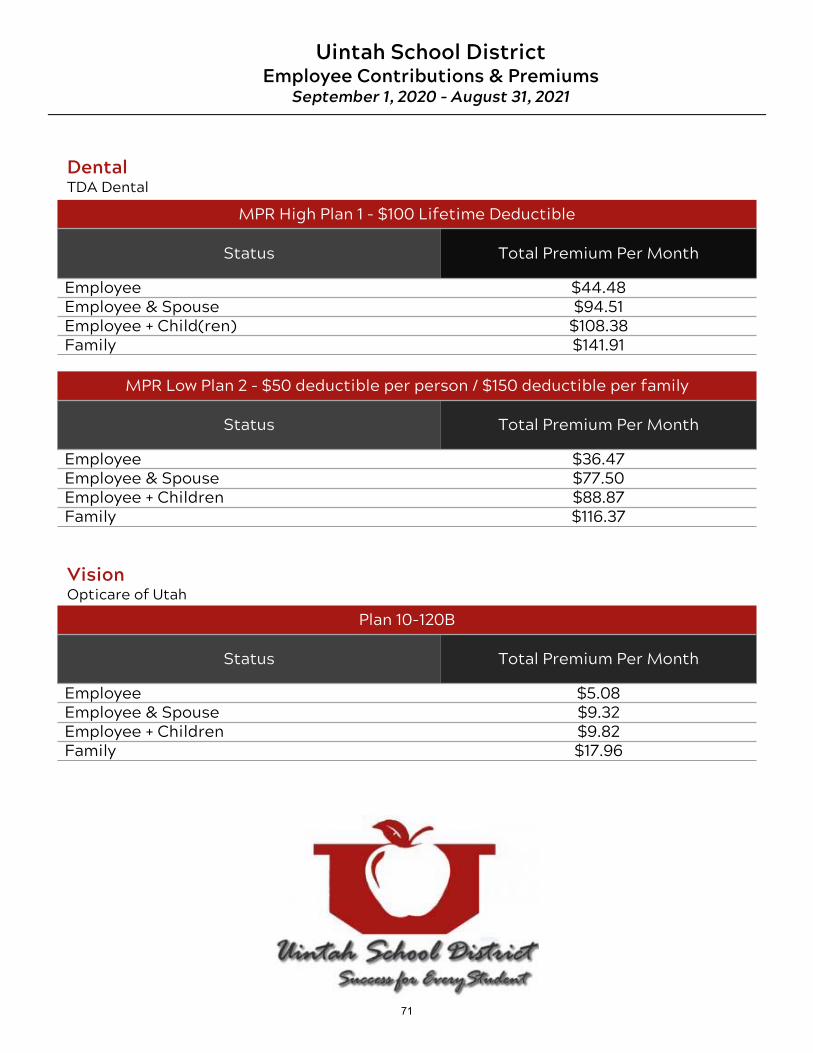
MPR High Plan 1 - $100 Lifetime Deductible
Status Total Premium Per Month
Employee $44.48Employee & Spouse $94.51Employee + Child(ren) $108.38Family $141.91
DentalTDA Dental
Uintah School DistrictEmployee Contributions & Premiums
September 1, 2020 – August 31, 2021
MPR Low Plan 2 - $50 deductible per person / $150 deductible per family
Status Total Premium Per Month
Employee $36.47Employee & Spouse $77.50Employee + Children $88.87Family $116.37
VisionOpticare of Utah
Plan 10-120B
Status Total Premium Per Month
Employee $5.08Employee & Spouse $9.32Employee + Children $9.82Family $17.96
71



















