
Uganda experience by Dr Patrick Kerchan, UPMB
19
ACHAP Pre-conference Workshop DR PATRICK KERCHAN February 25, 2015 HEAD OF PROGRAMMS Three project experiences from Uganda Protestant Medical Bureau FBO contributions to improved MCH at country level.
-
Upload
achapkenya -
Category
Documents
-
view
82 -
download
0
Transcript of Uganda experience by Dr Patrick Kerchan, UPMB

ACHAP Pre-conference Workshop DR PATRICK KERCHAN
February 25, 2015 HEAD OF PROGRAMMS
Three project experiences from Uganda Protestant Medical Bureau
FBO contributions to improved
MCH at country level.
– UPMB runs a network of
278 Health facilities, 35%
of the private, not-for-
profit sector in Uganda
– 90% of UPMB facilities
serve rural populations
– Began focused
investment in
strengthening FP in 2013
UPMB Background
Private, not-for-profit facilities across Uganda
Maternal and Child Health in Uganda
MCH cluster is composed of five elements;
• Sexual and Reproductive Health (SRH),
• Newborn care,
• Common childhood illnesses,
• Immunization
• Nutrition.
This emphasizes the link between maternal and child health and the cumulative nature of health problems through the entire lifecycle.
Sexual and Reproductive Health and Rights
Core HSSIP Indicators
• Maternal Mortality Ratio 438/100,000 – UDHS 2011
• % pregnant women attending 4 ANC sessions.
• % deliveries in health facilities.
• % pregnant women who have completed IPT2
• Contraceptive Prevalence Rate. Achieved 30% 2011/12 UDHS findings.
• Half of Uganda’s population is under 18 years and 57% of
women have given birth or are pregnant by age 19
• High fertility (7 children per woman) and low CPR (30%)
• 34 % unmet need for FP, particularly high in rural areas
• 25% of births occur with suboptimal spacing (<2
years after previous birth)
Top reasons for non-use of FP:
– Fear of side effects or health concerns (32%)
– Belief that they can’t get pregnant (correct
or incorrect assessment of risk) (17%)
– Woman or husband opposed (15%)
– Infrequent sex (7%)
FP in Uganda
Source: Uganda DHS 2011

Reproductive Health at UPMB UPMB
YEAR PROJECT/ FUNDER
# FACILITI
ES FOCUS
2002-04
Family Health International (FHI)
10 Facility-based strengthening local networks in integrated maternal health and SRH Services in rural communities
2006-09 Big Lottery
10 Facility-based strengthening of SRH information, particularly targeting adolescent girls
2009-13
Big Lottery
31
Voucher program for antenatal services, support to facility based maternal and neonatal health services, community outreaches, ambulances
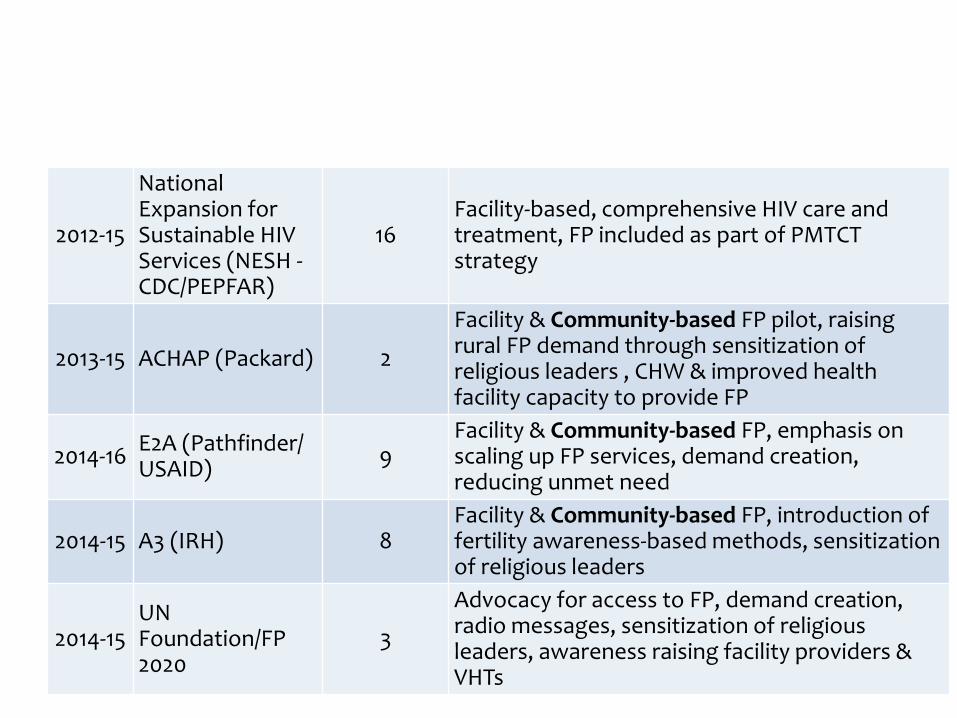
2012-15
National Expansion for Sustainable HIV Services (NESH - CDC/PEPFAR)
16 Facility-based, comprehensive HIV care and treatment, FP included as part of PMTCT strategy
2013-15 ACHAP (Packard) 2
Facility & Community-based FP pilot, raising rural FP demand through sensitization of religious leaders , CHW & improved health facility capacity to provide FP
2014-16 E2A (Pathfinder/ USAID)
9 Facility & Community-based FP, emphasis on scaling up FP services, demand creation, reducing unmet need
2014-15 A3 (IRH) 8 Facility & Community-based FP, introduction of fertility awareness-based methods, sensitization of religious leaders
2014-15 UN Foundation/FP 2020
3
Advocacy for access to FP, demand creation, radio messages, sensitization of religious leaders, awareness raising facility providers & VHTs
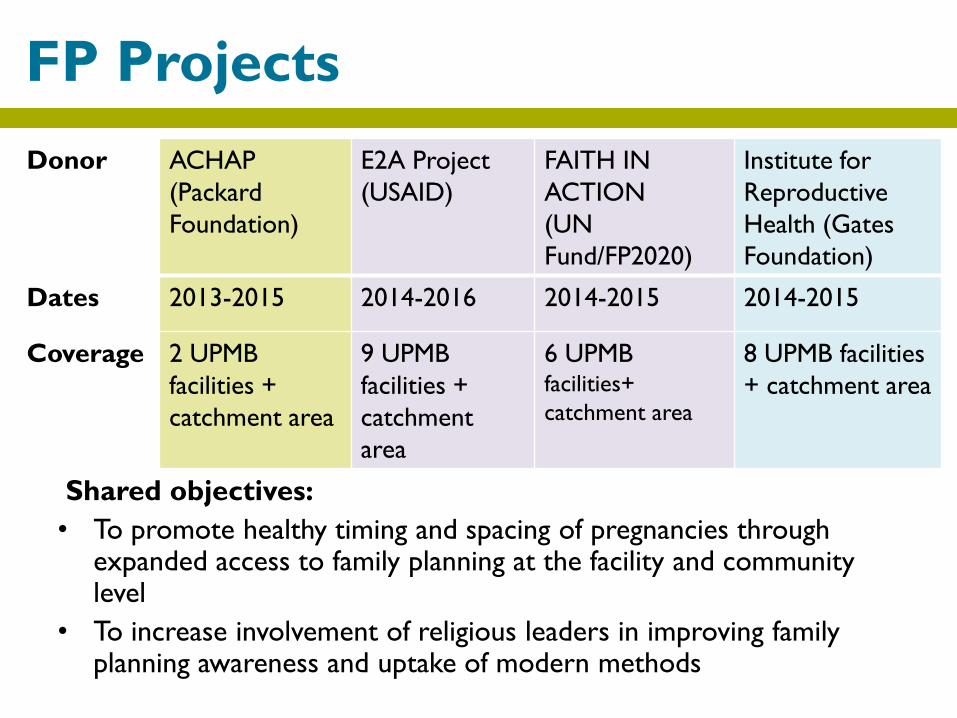
Shared objectives:
• To promote healthy timing and spacing of pregnancies through expanded access to family planning at the facility and community level
• To increase involvement of religious leaders in improving family planning awareness and uptake of modern methods
FP Projects
Donor ACHAP
(Packard
Foundation)
E2A Project
(USAID)
FAITH IN
ACTION
(UN
Fund/FP2020)
Institute for
Reproductive
Health (Gates
Foundation)
Dates 2013-2015 2014-2016 2014-2015 2014-2015
Coverage 2 UPMB
facilities +
catchment area
9 UPMB
facilities +
catchment
area
6 UPMB facilities+
catchment area
8 UPMB facilities
+ catchment area
• 185 religious leaders(30-ACHAP/UPMB,80 FAM PROJECT,45-E2A and
30-FAITH IN ACTION PROJECT) were equipped with skills to deliver accurate FP messages .
• Refer clients to health centers and CHWs for provision of FP methods
Role
• Work with CHWs and Health workers
• Make referrals to the facilities.
• Engage in community sensitizations
• Create platforms for health workers to deliver messages on
RH.
• Routine updates on work data through reports
Progress to date
• When Religious Leaders are involved in RH programs such as
family planning, they serve as ambassadors and agents of
change to level the ground for the ‘conservative’ attitudes in
Family Planning usually associated with traditional religious
beliefs.
• The number of referrals for family planning services in the
two health facilities has increased three-fold (ACHAP/UPMB
FP PROJECT
Results
Voices from the –Religious leaders
“I can now confidently talk to anyone about family
planning. I wish the government would also use us
when reaching out to the communities. If I pass on a
messages to a congregation of 120 worshippers,
everyone will believe me without doubt.” - Imam
Voices from the Religious leaders
Some of my followers at
church ask: “How come
the message is now
different?”
This issue(FP) needs
action and not mere
prayers, I keep
explaining.”
Initially, I preached messages against use of modern family planning methods, But this has changed with the ACHAP family planning project training for religious leaders, Pastor
• Routine support supervision to member units
• Strengthen collaborations with public sector (District and
national level)
• Scholarship programs supporting health workers
• Extension of donor support to the rural
• Improved health information management systems.
Reaching the hard to reach
• Some myths and misconceptions have been cleared through trainings and routine interactions with health workers.
• Personal testimonies by religious leaders from permanent method users (tubal ligation and vasectomy)
• Religious leaders create platforms for sensitizations on FP/RH for health workers in their houses of worship.
• Peer education among religious leaders
Lessons Learned: Successes
• This was an opportunities to
work with other faiths
(Catholic, Protestant,
Muslim)--FAM options
create entry point for
discussion of challenging
interfaith issues
• Some religious leaders still hold some myths and misconceptions.
• Religious leaders have high expectations in terms of monthly facilitation and allowances which makes sustainability hard.
• Need for routine refresher trainings for religious leaders to keep abreast of new developments in RH
• Strong supportive supervision is needed for accurate data collection and reporting at all levels
Lessons Learned: Challenges
• Routine reviews and mentorships for religious leaders by
family planning focal persons at facility level
• Refresher trainings for religious leaders
• Strengthen collaborations with public sector (District and
national level)
• Continue engaging religious leaders as champions in FP
• Advocate for a standardized training curriculum for religious
leaders
Interventions ahead
Discussion Guide for Religious
Leaders
Useful information
For additional information, please contact:
UGANDA PROTESTANT MEDICAL BUREAU
Thank you!


















