UCLA Head & Neck Surgery Resident Lecture Series Marc ...
32
UCLA Head & Neck Surgery Resident Lecture Series Marc Cohen, M.D.
Transcript of UCLA Head & Neck Surgery Resident Lecture Series Marc ...

UCLAHead&NeckSurgeryResidentLectureSeriesMarcCohen,M.D.

Alittlehistory…

Videotutorial

Alittlehistory…

Alittlehistory…
By1910,intubationforanesthesiahadbecomeanacceptedpractice
DuringWWI,MagillandMacintoshmadeprofoundimprovements
In1970,high‐volume,lowpressurecuffswereintroduced
Prolongedintubationvs.tracheotomy?
Inthe1960’s,longtermintubationforthemanagementofprematureLBWinfantswasrecommended
Until….Subglotticstenosiswasrecognized

Indicationsforendotrachealintubation
1.Temporaryreliefofupperairwayobstruction
2.Assistedventilationforrespiratoryfailure 3.Pulmonarytoilet

Whatarethepotentialcomplicationsofendotrachealintubation? Edema
Granuloma
Healedfibrousnodule
Interarytenoidadhesion
Posteriorglotticstenosis
Subglotticstenosis
Healedfurrows
Ductalcysts
Hematoma
Laceration
Subluxationofarytenoidcartilage
Lossofmobilityofcricoarytenoidjoint
Vocalcordparalysis
Nasogastrictubesyndrome

Pathogenesis
Pressure‐InducedInjuries
Vulnerablestructures• Medialsurfacesofarytenoids• Vocalprocesses• Cricoarytenoidjoints• Cricoidcartilage• Posteriorglottic/Interarytenoidregion

Pathogenesis
Supraglotticstructuresmaybecomeedematous,butrarelysustainseriousdamage
Trachealinjurieshavealsobecomelesssignificantduetolowpressurecuffs Althoughthereispotentialforinjuryifthecuffisinflatedtoohigh

Pathogenesis
ThemicrocirculationofthemucosaandmucoperichondriumisinterruptedwhenpressurefromtheETTexceedscapillarypressure
IschemiaNecrosisEdema,Hyperemia,Ulceration,andErosion

Factorsforsusceptibility
Extrinsicfactors DiameterofETT Durationofintubation Traumaticormultipleintubations
Patientfactors Poortissueperfusion(i.e.sepsis,organfailure,etc) LPR Abnormallarynx Woundhealing,keloid
Movement Duringventilatoruse Duringsuctioning Duringcoughing Duringtransport
“LaryngealBedsore”
Superficialulcerationcanoccurwithinhoursofintubation Usuallyhealswithoutscarring
AsETTpressurecontinues,migrationofinflammatorycellsensues Ifepithelialerosionsareincomplete,epitheliummaybereplacedbysquamousmetaplasia
Furtherpressurecausesulcerationthroughmucosatocartilage Causesperichondritisanddestructivechondritis Asopposedtosuperficialdamage,deeperulcerationhealsbysecondaryintentionandfibrosis

Edema
3locations1. Reinke’sspace Usuallypersistsafterextubation
2. Ventricularmucosa,seenas“protrusion” Usuallyresolvesafterextubation
3. Subglottis Usuallyresolvesafterextubation

Edema

Granulationtissue
Seenwithin48hours Proliferateatperipheryofulceratedareas

Pathogenesis

Granulationtissue
Flapsofgranulationtissue Canmovewithinspiration/expiration
Inspiratorystridor Notrecommendedtoexcisebothsides
MostcaseswillresolvewithoutanyinterventiononceETTisremoved

Granulationtissue
Incompleteresolutionofgranulationtissuecanyield: Postintubationgranuloma Healedfibrousnodule

Interarytenoidadhesion

Posteriorglotticstenosis
Formswhenscarcontractsafterwideulcerationwithnointactmedianstripofmucosa
Vocalcordsunabletoabduct Glottisremainspartlyclosed Inspiratorystridor Voiceisusuallyunaffected Treatment:deepverticaldivisionwithlaseror11
bladedowntolevelofcricoid Re‐stenosisislikely Costalcartilagegraftmaybenecessary(endoscopicallyoropen)

Posteriorglotticstenosis

Subglotticstenosis
Manycauses Ininfants,mostcommonfactorsrelatedtoacquiredSSareETTsizeandLPRduringlong‐termintubation
Presentationinaninfant: Failedextubation Recurrentoratypicalcroup Slowlyprogressiveairwayobstruction DifficultypassingETT Postanesthesiastridor

Cotton‐MyerGradingSystem
GradeI‐<50%obstruction GradeII–51‐70%obstruction GradeIII–71‐99%obstruction GradeIV–Nodetectablelumen
Ruleofthumb: Subglotticdiameter<4.0mminafull‐terminfantisthelowerlimitofnormal(<3.0mminapreterminfant)

Subglotticstenosis
Whenrepeatedattemptsatextubationfail: ReintubatewithsmallerETT Racemicepinepherine Dexamethasone Ifthesemaneuversfail: Cricoidsplitwith/withoutcartilagegraft Tracheostomy

DuctalCysts
Resultfromretentionofmucusinobstructed,dilatedductsofsubmucosalmucousglands
Mostaresmallandrequirenotreatment Whenlargeandcauseobstruction,endoscopicremovalisrequired
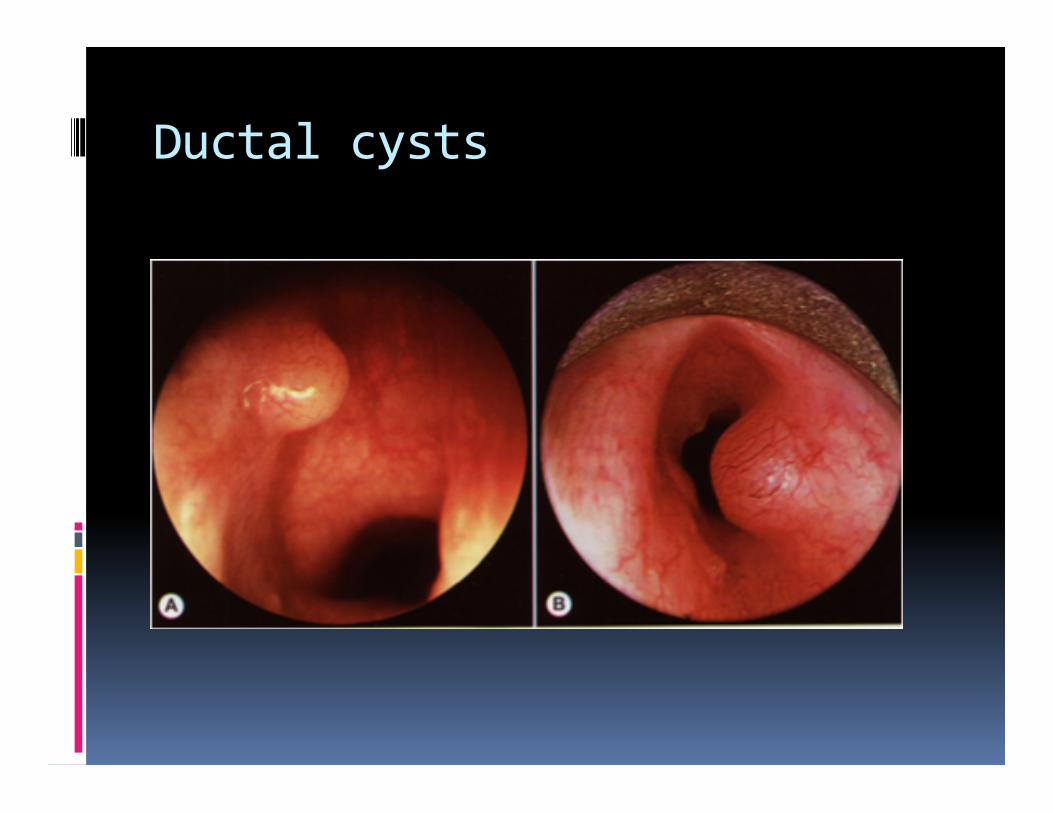
Ductalcysts

Arytenoiddislocation
MayoccurduringpassageofanETT Leftarytenoidisusuallyaffectedsinceintubationoccursfromrightsideofmouth
Patientwillcomplainofhoarseness,throatdiscomfort,odynophagia,andcough
Microlaryngoscopyandclosedreductionshouldbeperformedearly

Arytenoiddislocation

Nasogastrictubesyndrome
OccurswhenNGTrestscentrally,ratherthanlaterally
Anteriorwallofhypopharynx/posteriorwallofcricoidbecomesulcerated
Resultsinperichondritis,chondritis,necrosis
Canprogresstosudden,life‐threateningbilateralvocalcordparalysisduetomyositisofPCAmuscles
Diabeticsandrenaltransplantswhoareinrenalfailureareespeciallyvulnerable
Warningsigns:hoarseness,otalgia,andodynophagia
Treatment:removeNGT,abx,G‐tube,andpossibletracheostomy

Timelineofpostextubationobstruction Immediate:flapsofgranulationtissue,laryngealspasm
Minutestohours:flapsofgranulationtissue,subglotticedema,granulationtissue,LPR
Daystoweeks:persistentedemaorgranulationtissue,granuloma
Months:posteriorglotticstenosis,subglotticstenosis

Totrachornottotrach?
Oneschoolofthoughtisthatanyonewhoisintubatedlongerthan7daysshouldundergotracheotomy
NewerrecommendationsareforDLafter7days–ifnoevidenceofsignificantlaryngealpathology,keepthepatientintubatedunlessplanforlong‐termtracheostomy