
UA STEMI ACS I - गृहपृष्ठ · 4/22/12 5 badri@gmc Non ST Elevation MI •...
14
4/22/12 1 Dr Badri Paudel GMC Atherothrombosis: Thrombus Superimposed on Atherosclerotic Plaque Adapted with permission from Falk E, et al. Circulation. 1998;92:657-671. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org. 2 badri@gmc Characteristics of Unstable and Stable Plaque Thin fibrous cap Inflammatory cells Few SMCs Eroded endothelium Activated macrophages Thick fibrous cap Lack of inflammatory cells Foam cells Intact endothelium More SMCs Adapted with permission from Libby P. Circulation. 1995;91:2844-2850. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org. Unstable Stable 3 badri@gmc The Stable and Unstable Plaque Reproduced with permission from Yeghiazarians Y, Braunstein JB, Askari A, et al. Unstable angina pectoris. N Engl J Med. 2000;342:101-114.Copyright © 2000, Massachusetts Medical Society. All rights reserved. 4 badri@gmc ACS Pathophysiology Plaque Rupture, Thrombosis, and Microembolization Quiescent plaque Platelet-thrombin micro-emboli Plaque rupture Process Plaque formation Inflammation Multiple factors ? Infection Plaque Rupture ? Macrophages Metalloproteinases Thrombosis Platelet Activation Thrombin Marker Cholesterol LDL C-Reactive Protein Adhesion Molecules Interleukin 6, TNFα, sCD-40 ligand MDA Modified LDL D-dimer, Complement, Fibrinogen, Troponin, CRP, CD40L Vulnerable plaque Macrophages Collagen → platelet activation TF → Clotting Cascade Lipid core Metalloproteinases Inflammation Courtesy of David Kandzari. 5 badri@gmc 6 badri@gmc
Transcript of UA STEMI ACS I - गृहपृष्ठ · 4/22/12 5 badri@gmc Non ST Elevation MI •...
4/22/12
1
Dr Badri Paudel GMC
Atherothrombosis: Thrombus Superimposed on Atherosclerotic Plaque
Adapted with permission from Falk E, et al. Circulation. 1998;92:657-671. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.
2 badri@gmc
Characteristics of Unstable and Stable Plaque
Thin fibrous cap
Inflammatory cells
Few SMCs
Eroded endothelium
Activated macrophages
Thick fibrous cap
Lack of inflammatory cells
Foam cells
Intact endothelium
More SMCs
Adapted with permission from Libby P. Circulation. 1995;91:2844-2850. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.
Unstable Stable
3 badri@gmc
The Stable and Unstable Plaque
Reproduced with permission from Yeghiazarians Y, Braunstein JB, Askari A, et al. Unstable angina pectoris. N Engl J Med. 2000;342:101-114.Copyright © 2000, Massachusetts Medical Society. All rights reserved. 4 badri@gmc
ACS Pathophysiology Plaque Rupture, Thrombosis, and Microembolization
Quiescent plaque
Platelet-thrombin micro-emboli Plaque rupture
Process Plaque formation Inflammation Multiple factors ? Infection Plaque Rupture ? Macrophages Metalloproteinases Thrombosis Platelet Activation Thrombin
Marker Cholesterol LDL C-Reactive Protein Adhesion Molecules Interleukin 6, TNFα, sCD-40 ligand MDA Modified LDL D-dimer, Complement, Fibrinogen, Troponin, CRP, CD40L
Vulnerable plaque
Macrophages Foam Cells
Collagen → platelet activation
TF → Clotting Cascade
Lipid core
Metalloproteinases
Inflammation
Courtesy of David Kandzari.
5 badri@gmc 6 badri@gmc
4/22/12
2
7 badri@gmc 8 badri@gmc
9 badri@gmc badri@gmc
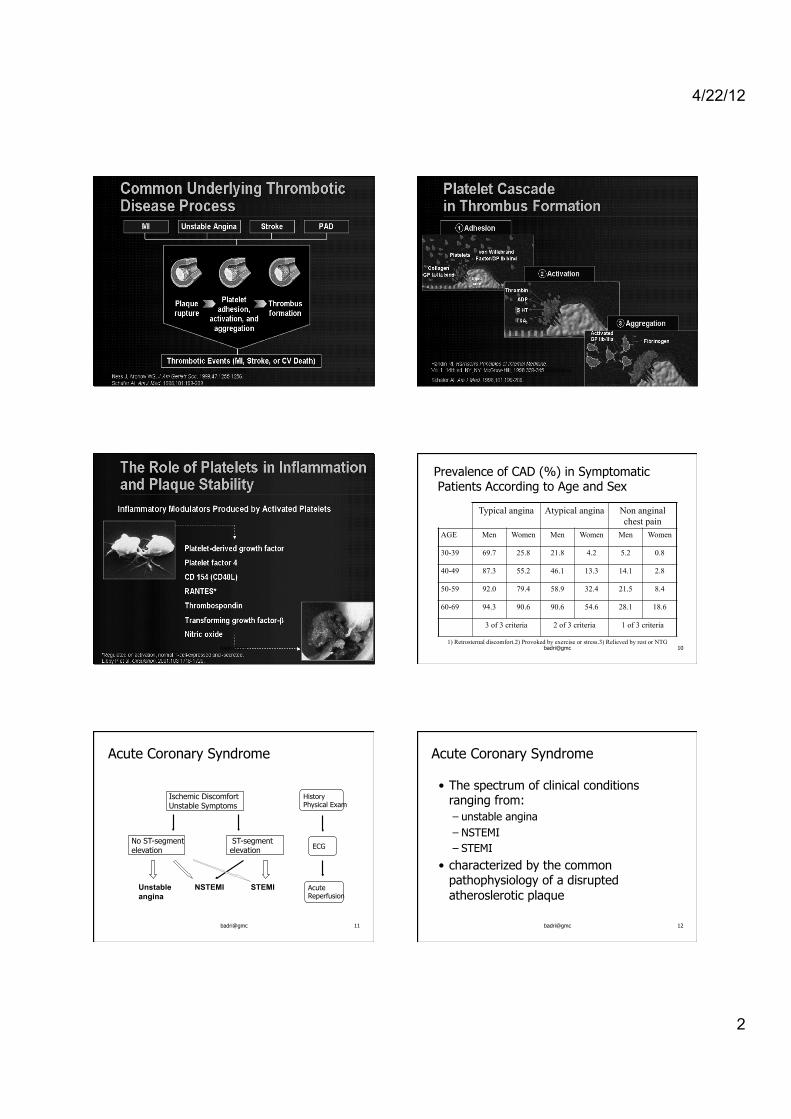
Prevalence of CAD (%) in Symptomatic Patients According to Age and Sex
Typical angina Atypical angina Non anginal chest pain
AGE Men Women Men Women Men Women
30-39 69.7 25.8 21.8 4.2 5.2 0.8
40-49 87.3 55.2 46.1 13.3 14.1 2.8
50-59 92.0 79.4 58.9 32.4 21.5 8.4
60-69 94.3 90.6 90.6 54.6 28.1 18.6
3 of 3 criteria 2 of 3 criteria 1 of 3 criteria
1) Retrosternal discomfort.2) Provoked by exercise or stress.3) Relieved by rest or NTG 10
Acute Coronary Syndrome
Ischemic Discomfort Unstable Symptoms
No ST-segment elevation
ST-segment elevation
Unstable NSTEMI STEMI angina
ECG
Acute Reperfusion
History Physical Exam
11 badri@gmc
Acute Coronary Syndrome
• The spectrum of clinical conditions ranging from: – unstable angina – NSTEMI – STEMI
• characterized by the common pathophysiology of a disrupted atheroslerotic plaque
12 badri@gmc
4/22/12
3
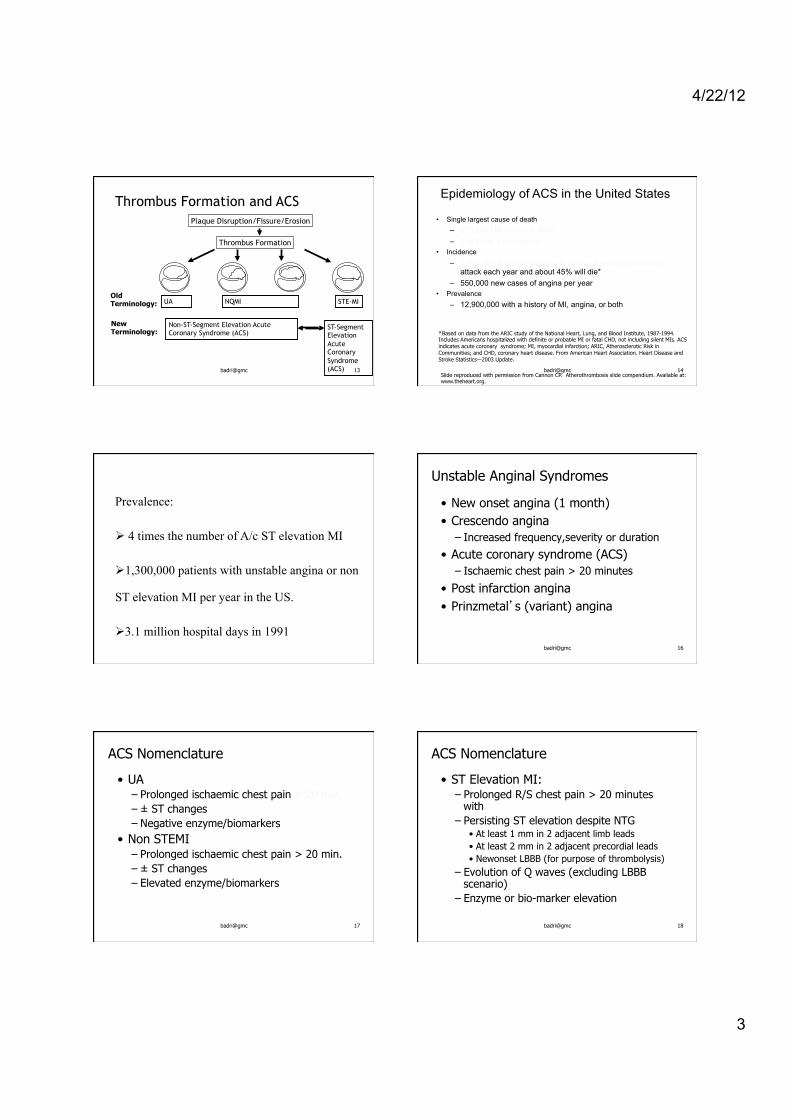
Thrombus Formation and ACS
UA NQMI STE-MI
Plaque Disruption/Fissure/Erosion
Thrombus Formation
Non-ST-Segment Elevation Acute Coronary Syndrome (ACS)
ST-Segment Elevation Acute Coronary Syndrome (ACS)
Old Terminology:
New Terminology:
13 badri@gmc
* Based on data from the ARIC study of the National Heart, Lung, and Blood Institute, 1987-1994. Includes Americans hospitalized with definite or probable MI or fatal CHD, not including silent MIs. ACS indicates acute coronary syndrome; MI, myocardial infarction; ARIC, Atherosclerotic Risk in Communities; and CHD, coronary heart disease. From American Heart Association. Heart Disease and Stroke Statistics—2003 Update.
Epidemiology of ACS in the United States • Single largest cause of death
– 515,204 US deaths in 2000 – 1 in every 5 US deaths
• Incidence – 1,100,000 Americans will have a new or recurrent coronary
attack each year and about 45% will die* – 550,000 new cases of angina per year
• Prevalence – 12,900,000 with a history of MI, angina, or both
Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.
14 badri@gmc
Prevalence:
Ø 4 times the number of A/c ST elevation MI
Ø 1,300,000 patients with unstable angina or non
ST elevation MI per year in the US.
Ø 3.1 million hospital days in 1991 badri@gmc
Unstable Anginal Syndromes
• New onset angina (1 month) • Crescendo angina
– Increased frequency,severity or duration
• Acute coronary syndrome (ACS) – Ischaemic chest pain > 20 minutes
• Post infarction angina • Prinzmetal’s (variant) angina
16
badri@gmc
ACS Nomenclature
• UA – Prolonged ischaemic chest pain > 20 min. – ± ST changes – Negative enzyme/biomarkers
• Non STEMI – Prolonged ischaemic chest pain > 20 min. – ± ST changes – Elevated enzyme/biomarkers
17 badri@gmc
ACS Nomenclature
• ST Elevation MI: – Prolonged R/S chest pain > 20 minutes
with – Persisting ST elevation despite NTG
• At least 1 mm in 2 adjacent limb leads • At least 2 mm in 2 adjacent precordial leads • Newonset LBBB (for purpose of thrombolysis)
– Evolution of Q waves (excluding LBBB scenario)
– Enzyme or bio-marker elevation
18

4/22/12
4
badri@gmc
Categorize the Severity of Angina
CCS Classification Class 0 asymptomatic
Class I on strenuous activity
Class II on moderate activity > 2 blocks or 2 flights of stairs
Class III on mild activity < 2 blocks or 2 flights of stairs
Class IV
rest or minimal activity
19 badri@gmc
Categorize the Severity of Angina
CCS Classification Class IV A
Patient admitted to hospital and becomes relatively asymptomatic with aggressive medical therapy
Class IV B
Patient admitted to hospital and continues to experience angina on maximal medical therapy and cannot be safely discharged home, but does not require IV nitroglycerin.
Class IV C Patient admitted to hospital and maximal medical therapy, including IV nitroglycerin, fails to control symptoms or there is hemodynamic instability.
Class IV D
Cardiogenic Shock
20
CLASSIFICATION OF UNSTABLE ANGINA
SEVERITY;
CLASS 1 – NEW ONSET, SEVERE OR ACCELARATED ANGINA
ANGINA < 2 MOS DURATION, SEVERE OR OCCURING
3 OR MORE TIMES PER DAY,
OR
ANGINA THAT IS DISTINCTLY MORE FRQUENT AND
PPT BY DISTINCTLY LESS EXERTION
NO REST PAIN IN THE LAST 2 MOS
CLASS II;
ANGINA AT REST – SUBACUTE
PATIENTS WITH ONE OR MORE EPISODES OF ANGINA
AT REST DURING THE PRECEDING MONTH
BUT NOT WITHIN THE LAST 48 HOURS
CLASS III
ANGINA AT REST – ACUTE
PATIENTS WITH ONE OR MORE EPISODES AT REST
WITHIN THE PRECEDING 48 HOURS
CLINICAL CIRCUMSTANCES
CLASS A: SECONDARY UNSTABLE ANGINA Anemia, infection, fever, hypotension thyrotoxicosis, hypoxemia secondary to respiratory failure
CLASS B
PRIMARY UNSTABLE ANGINA Develops in the absence of extracardiac condition
CLASS C POST-INFARCTION ANGINA (within two weeks of DOCUMENTED MI). Occurs in 20% of A/c MIs
INTENSITY OF TREATMENT
May be divided in to 3 groups depending on when it occurs
1. ABSENCE OR MINIMAL TREATMENT OF CHRONIC
STABLE ANGINA
2. OCCURING IN PRESENCE OF STANDARD RX FOR
CHRONIC STABLE ANGINA (CONVENTIONAL DOSES OF
BETA BLOSKERS, NITRATES, CCB)
3. OCCURING DESPITE MAXIMALLY TOLERATED DOSES OF
ALL 3 CATEGORIES OF ORAL RX , INCLUDING IV NTG
4/22/12
5
badri@gmc
Non ST Elevation MI
• Definition: – Prolonged ischaemic chest pain – ST-T changes – Positive serum markers
25 badri@gmc
Pathogenesis
ACUTE CORONARY SYNDROME
No ST Elevation ST Elevation
Unstable Angina NQMI QwMI Myocardial Infarction
NSTEMI
UA/NSTEMI 9/00
26
badri@gmc
What Is the Culprit Lesion?
• 58-year-old male with chronic stable angina
• Positive stress test with small reversible ischemic defect on nuclear scintigraphy"
Medication prescribed, but six weeks later…3-day history of unstable angina, including���30 minutes of rest pain
• Medically “cooled off” followed by angiography
Case provided by the McLaren Heart and Vascular Center, Flint, Michigan; used with permission.
27 badri@gmc
Atherosclerosis is a Diffuse Process
28
badri@gmc
Pathogenesis
• Plaque rupture or erosion • Thrombosis with/without occlusion • Necrosis contingent on
– Severity of plaque rupture – Duration of ischaemia – Lability of occlusive thrombus – Adequacy of collaterals – Vasoconstriction – Downstream platelet/fibrin emboli
29 badri@gmc
Unstable Angina: Platelet Plugging of the Capillaries
From: Intramyocardial platelet aggregation in patients with unstable angina suffering sudden ischemic cardiac death Davies MJ, Circulation 1986
“The results support the view that platelet aggregates in the myocardium represent an embolic phenomenon and are a potential cause of unstable angina. The association of myocardial necrosis with such emboli could precipitate sudden death from ventricular fibrillation.”
30

4/22/12
6
badri@gmc
Unstable Angina-Triggers Systemic factors
• Hyper-coagulable state • Increased vascular resistance • Coronary spasm • Increased cortisol & catecholamines • Vasoconstriction • Increased arterial pressure • Circadian variation
31 badri@gmc
Unstable Angina Triggering Situations • Awakening • Excessive physical exertion • Mental stress • Anger • Cigarette smoking • Coffee & alcohol consumption • Sexual activity
32
badri@gmc
Non ST Elevation MI
90% of acute MIs are caused by thrombus formation from rupture of unstable plaques
Ruptured Plaque
33 badri@gmc Extensive subendocardial myocardial infarction (yellow arrows)
Sub-endocardial MI
34
badri@gmc
Occlusive Thrombus
35 badri@gmc
Transmural Infarction
36

4/22/12
7
badri@gmc 37 badri@gmc 38
AntmanAntman et al. et al. JAMAJAMA. 2000;284:835. Available at: . 2000;284:835. Available at: www.www.timitimi.org..org.
TIMI Risk Score for UA/NSTEMITIMI Risk Score for UA/NSTEMI7 Independent Predictors7 Independent Predictors
nn Age Age ≥≥65 years65 yearsnn ≥≥3 CAD risk factors3 CAD risk factors
((↑↑ cholchol, , FHxFHx, HTN, DM, smoking), HTN, DM, smoking)nn Prior CAD (cath stenosis >50%) Prior CAD (cath stenosis >50%) nn ASA in last 7 daysASA in last 7 daysnn ≥≥2 Anginal events 2 Anginal events ≤≤24 hours24 hoursnn ST deviation ST deviation nn Elevated cardiac markers (CKElevated cardiac markers (CK--MB orMB or troponintroponin))
www.timi.org
39 badri@gmc badri@gmc
TIMI Risk Score for UA/NSTEMI
40
Low Risk Intermediate Risk
High Risk Very High Risk
Non ST ↑ ACS 30 Day Death/MI Risk
< 3 % 3-8 % 8-15 % >15%
No higher risk features • Single short duration (<10 min.) rest pain • Crescendo angina/New onset angina (Mod severity) 6 Hour Observation • ECG X 2 normal, unchanged or non-specific ST Δ’s • Negative biomarkers X 2
Rest pain < 20 min. New onset/ Crescendo angina (Low threshold severity) • ECG non-specific abnormalities or normal • Biomarkers normal or borderline ↑ Increased baseline risk • DM • Previous CABG/MI • Recent PCI
Rest pain > 20 min. Prolonged recurrent pains
• ECG ST depression < 2mm • Deep T inversion (e.g. > 5 mm) • T inversion > 2 mm
– Especially in > 5 leads
• Isolated biomarker clearly +ve
• ST depression < 2mm With ↑ CK-MB or Tn • ST depression > 2mm
– Multiple leads – With pain
• Transient ST ↑ > 1 mm
• Hemodynamic instability
– ↓ BP/CHF
Refractory ischaemia with ST shift
D Fitchett, SG Goodman M Gupta, A Langer. Can J Card 2002; 18 (11):1179-1190. 41 badri@gmc
www.timi.org
42 badri@gmc
4/22/12
8
Testing for ACS - Serum Markers
• Creatine Kinase, an intracellular enzyme involved in transferring phosphate grps from ATP to creatine in Cardiac & skeletal muscle and brain
• CK-BB = brain • CK-MM = skeletal • CK-MB = cardiac
4/22/12 43 Badri@GMC
Testing for ACS - Serum Markers
• CK – elevates 4-8 hours after coronary Art. Occlusion – Peaks = 12 to 24 hours – Nml = 3 to 4 days
• CK-MB – Detectable 4-8 hrs – Peak = before 24 hrs – Nml = in 48hrs
• CK-MB normally can be 5% of total CK (Rapid Index)
4/22/12 44 Badri@GMC
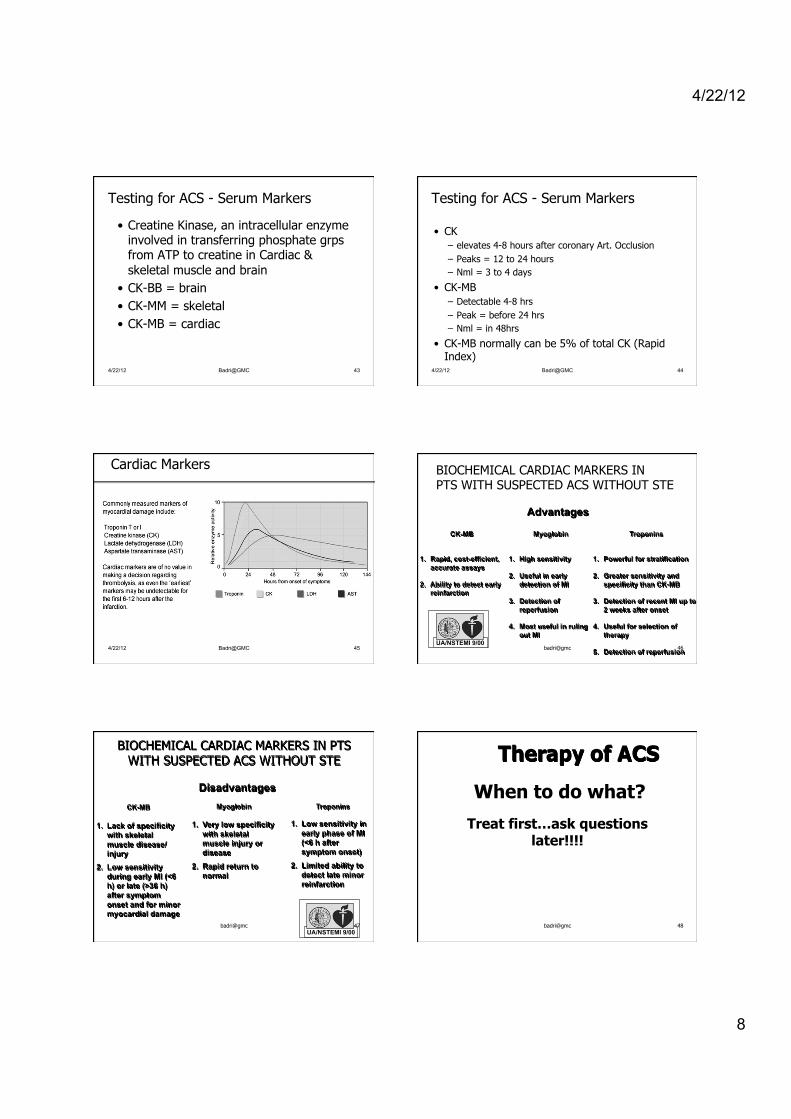
Cardiac Markers
4/22/12 45 Badri@GMC
BIOCHEMICAL CARDIAC MARKERS IN PTS WITH SUSPECTED ACS WITHOUT STE
CK-MB
1. Rapid, cost-efficient,
accurate assays 2. Ability to detect early
reinfarction
Myoglobin
1. High sensitivity 2. Useful in early
detection of MI 3. Detection of
reperfusion 4. Most useful in ruling
out MI
Troponins
1. Powerful for stratification 2. Greater sensitivity and
specificity than CK-MB 3. Detection of recent MI up to
2 weeks after onset 4. Useful for selection of
therapy 5. Detection of reperfusion
Advantages
UA/NSTEMI 9/00 46 badri@gmc
BIOCHEMICAL CARDIAC MARKERS IN PTS WITH SUSPECTED ACS WITHOUT STE
CK-MB 1. Lack of specificity
with skeletal muscle disease/injury
2. Low sensitivity during early MI (<6 h) or late (>36 h) after symptom onset and for minor myocardial damage
Myoglobin
1. Very low specificity with skeletal muscle injury or disease
2. Rapid return to normal
Troponins
1. Low sensitivity in early phase of MI (<6 h after symptom onset)
2. Limited ability to detect late minor reinfarction
Disadvantages
UA/NSTEMI 9/00 47 badri@gmc badri@gmc
When to do what?
Treat first…ask questions later!!!!
Therapy of ACS
48
4/22/12
9
badri@gmc
General Measures
• Rest, oxygen and EKG monitoring • Exclude secondary causes (10-15% ) - Anemia - Arrythmias - Heart Failure - Hypoxemia - Infection - Uncontrolled HTN - Stress - Thyrotoxicosis
49 badri@gmc
Unstable Angina/ACS Therapeutic Goals-1 • Prevent re-thrombosis & prevent
downstream embolization – Anti-platelet therapy
• ASA (65-75% ↓ early events;50%↓ death/MI 2-24 months)
• Clopidogrel 300-600 mg → 75 mg OD • Glycoprotein IIB/IIIA inhibitors
– Anti-coagulant therapy (↓ death MI additional 40%) • UFH or LMWH
50
badri@gmc
Unstable Angina/ACS Therapeutic Goals-1
• Control ischaemia – β-blockers – Nitrates – CCB’s
• Relieve Obstruction – Cardiac cath – PCI – CABG
51
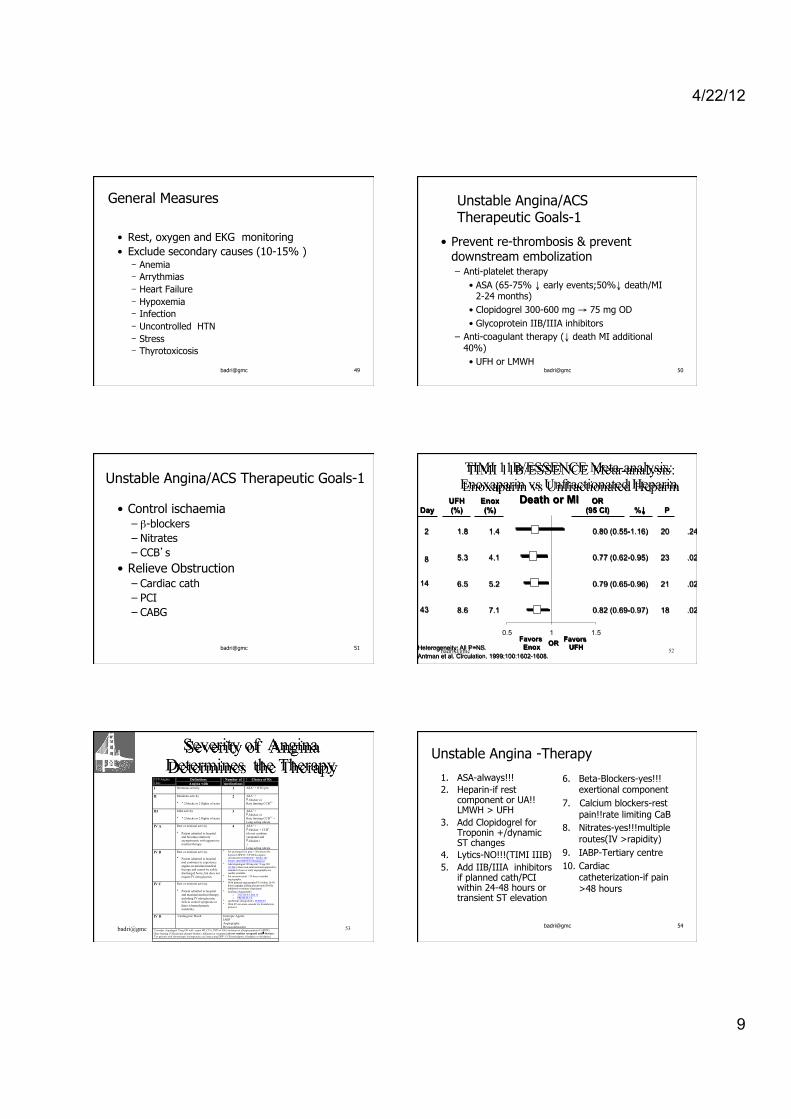
0.5 1 1.5
8.6 7.1 0.82 (0.69-0.97) 18 .02
6.5 5.2 0.79 (0.65-0.96) 21 .02
5.3 4.1 0.77 (0.62-0.95) 23 .02
1.8 1.4 0.80 (0.55-1.16) 20 .24
Day
2
8
14
43
UFH (%)
Enox (%)
OR (95 CI)
Favors Enox
Favors UFH
%↓ P
OR Heterogeneity: All P=NS. Antman et al. Circulation. 1999;100:1602-1608.
Death or MI
TIMI 11B/ESSENCE Meta-analysis: Enoxaparin vs Unfractionated Heparin
52 badri@gmc
badri@gmc
Severity of Angina Determines the Therapy
CCS Angina Class
Definition: Angina with
Number of medications
Choice of Rx
I
Strenuous activity 1 ASA1 + NTG prn
II Moderate activity • > 2 blocks or 2 flights of stairs
2 ASA1 + β-blocker or Rate limiting CCB2,3
III Mild activity • < 2 blocks or 2 flights of stairs
3 ASA1 + β-blocker or Rate limiting CCB2,3 + Long acting nitrate
IV A Rest or minimal activity • Patient admitted to hospital
and becomes relatively asymptomatic with aggressive medical therapy
4 ASA1 + β-blocker + CCB3 (do not combine verapamil and β-blocker) + Long acting nitrate
IV B Rest or minimal activity. • Patient admitted to hospital
and continues to experience angina on maximal medical therapy and cannot be safely discharged home, but does not require IV nitroglycerin.
IV C Rest or minimal activity.
• Patient admitted to hospital
and maximal medical therapy, including IV nitroglycerin, fails to control symptoms or there is hemodynamic instability.
• For prolonged rest pain > 20 minutes Rx heparin LMWH > UFH Enoxaparin (Lovenox®) (ESSENCE / TIMI 11B / TIMI 11B-ESSENCE Metanalysis)
• Add clopidogrel 300 mg stat 75 mg OD (CURE) where non-interventional approach is standard of care or early angiography not readily available.
• For recurrent pain > 24 hours consider angiography
• With planned angiography/PCI within 24-48 hours consider adding glycoprotein IIb/IIIa inhibitor/re-evaluate clopidogrel
• tirofiban (Aggrastat®) o TACTICS-TIMI 18 o PRISM-PLUS
• eptifibitide (Integrilin®) -PURSUIT • With ST elevation consider for thrombolytic
protocol
IV D Cardiogenic Shock Inotropic Agents IABP Angiography Revascularization
1Consider clopidogrel 75mg OD with recent MI, CVA, PVD in ASA intolerant or allergic patients (CAPRIE).
2Rate limiting CCB(calcium channel blocker): diltiazem or verapamil (do not combine verapamil and β-blocker) 3For patients with chronotropic incompetence use long acting DHP- CCB (amlodipine, felodipine or nifedipine)
53 badri@gmc
Unstable Angina -Therapy
1. ASA-always!!! 2. Heparin-if rest
component or UA!! LMWH > UFH
3. Add Clopidogrel for Troponin +/dynamic ST changes
4. Lytics-NO!!!(TIMI IIIB) 5. Add IIB/IIIA inhibitors
if planned cath/PCI within 24-48 hours or transient ST elevation
6. Beta-Blockers-yes!!!exertional component
7. Calcium blockers-rest pain!!rate limiting CaB
8. Nitrates-yes!!!multiple routes(IV >rapidity)
9. IABP-Tertiary centre 10. Cardiac
catheterization-if pain >48 hours
54

4/22/12
10
Management Strategy for ACS/NSTEMI
ACS/NSTEMI
Aggressive Therapy (early cath/intervention)
Conservative Therapy (medical Rx/non-invasive evaluation)
Non-cardiac exacerbation of known CAD • Anemia • Infection • Hyperthyroidism • Other medical causes
Patient preference Stability Normal LV Function Good exercise tolerance Relative C/I to CABG/PCI Brief duration of ischaemia No ST changes Negative biomarkers
Dynamic ST changes Positive Enzymes or Biomarkers
Recurrent ischaemia on medical Rx Prolonged ischaemic pain
PTCA < 6 months Known severe CAD
LV dysfunction • Pre-existing
• new MR • new CHF
Intolerance to medical Rx Recurrent ventricular
arrythmia’s/SCD Early positive non-invasive test
Poor exercise tolerance 55 badri@gmc badri@gmc 56
badri@gmc Reproduced with Permission of CHRC 57 58 badri@gmc
Platelets and Anti-Platelet Therapies
59 badri@gmc
Pathogenesis of Acute Coronary Syndromes: The integral role of platelets
Plaque Fissure or Rupture
Platelet Aggregation
Platelet Activation
Platelet Adhesion
Thrombotic Occlusion
60 badri@gmc

4/22/12
11
Adhesion
The Role of Platelets in Atherothrombosis
Aggregation 3
Reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.
1
Activation 2 61 badri@gmc
ADP
• Ticlopidine • Clopidogrel
• Heparin • LMW Heparin • Direct Thrombin Inhibitors
• Aspirin
Epinephrine Collagen Arachidonic
Acid
Thrombin
IIb/IIIa receptors
fibrin
The Platelet
• GP IIb/IIIa inhibitors
62 badri@gmc
63 badri@gmc 64 badri@gmc
Platelet Inhibition With GP IIb/IIIa Inhibitors
Reproduced with permission from Yeghiazarians Y, Braunstein JB, Askari A, et al. Unstable angina pectoris. N Engl J Med. 2000;342:101-114. Copyright © 2000, Massachusetts Medical Society. All rights reserved.
65 badri@gmc
placebo aspirin heparin ASA+hep 0 2 4 6 8
10 12
% D
evel
opin
g M
I
Treatment
Treatment of Unstable Angina Results of a study from the Montreal Heart Institute
Data from Theroux P, Quimet H, McCans J, et al. Aspirin, heparin, or both to treat acute unstable angina. N Engl J Med. 1988;319:1105-1111. 66 badri@gmc
4/22/12
12
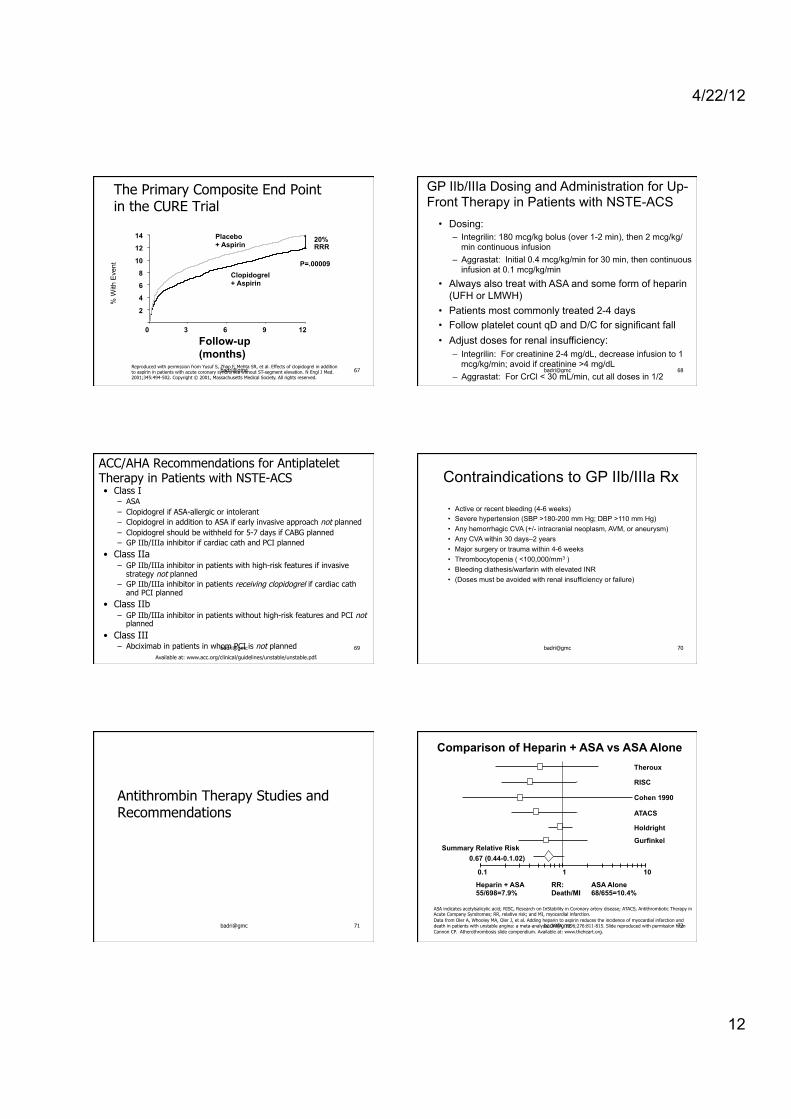
Reproduced with permission from Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494-502. Copyright © 2001, Massachusetts Medical Society. All rights reserved.
2
4
6
8
10
12
14
% W
ith E
vent
Clopidogrel + Aspirin
3 6 9
Placebo + Aspirin
Follow-up (months)
P=.00009
0 12
20% RRR
The Primary Composite End Point in the CURE Trial
67 badri@gmc
GP IIb/IIIa Dosing and Administration for Up-Front Therapy in Patients with NSTE-ACS
• Dosing: – Integrilin: 180 mcg/kg bolus (over 1-2 min), then 2 mcg/kg/
min continuous infusion – Aggrastat: Initial 0.4 mcg/kg/min for 30 min, then continuous
infusion at 0.1 mcg/kg/min
• Always also treat with ASA and some form of heparin (UFH or LMWH)
• Patients most commonly treated 2-4 days • Follow platelet count qD and D/C for significant fall • Adjust doses for renal insufficiency:
– Integrilin: For creatinine 2-4 mg/dL, decrease infusion to 1 mcg/kg/min; avoid if creatinine >4 mg/dL
– Aggrastat: For CrCl < 30 mL/min, cut all doses in 1/2 68 badri@gmc
ACC/AHA Recommendations for Antiplatelet Therapy in Patients with NSTE-ACS • Class I
– ASA – Clopidogrel if ASA-allergic or intolerant – Clopidogrel in addition to ASA if early invasive approach not planned – Clopidogrel should be withheld for 5-7 days if CABG planned – GP IIb/IIIa inhibitor if cardiac cath and PCI planned
• Class IIa – GP IIb/IIIa inhibitor in patients with high-risk features if invasive
strategy not planned – GP IIb/IIIa inhibitor in patients receiving clopidogrel if cardiac cath
and PCI planned
• Class IIb – GP IIb/IIIa inhibitor in patients without high-risk features and PCI not
planned
• Class III – Abciximab in patients in whom PCI is not planned
Available at: www.acc.org/clinical/guidelines/unstable/unstable.pdf.
69 badri@gmc
Contraindications to GP IIb/IIIa Rx
• Active or recent bleeding (4-6 weeks) • Severe hypertension (SBP >180-200 mm Hg; DBP >110 mm Hg) • Any hemorrhagic CVA (+/- intracranial neoplasm, AVM, or aneurysm) • Any CVA within 30 days–2 years • Major surgery or trauma within 4-6 weeks • Thrombocytopenia ( <100,000/mm3 ) • Bleeding diathesis/warfarin with elevated INR • (Doses must be avoided with renal insufficiency or failure)
70 badri@gmc
Antithrombin Therapy Studies and Recommendations
71 badri@gmc
RR: Death/MI
ASA Alone 68/655=10.4%
Heparin + ASA 55/698=7.9%
0.1 1 10
Summary Relative Risk 0.67 (0.44-0.1.02)
Theroux
RISC
Cohen 1990
ATACS
Holdright
Gurfinkel
Comparison of Heparin + ASA vs ASA Alone
ASA indicates acetylsalicylic acid; RISC, Research on InStability in Coronary artery disease; ATACS, Antithrombotic Therapy in Acute Company Syndromes; RR, relative risk; and MI, myocardial infarction. Data from Oler A, Whooley MA, Oler J, et al. Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina: a meta-analysis. JAMA. 1996;276:811-815. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.
72 badri@gmc

4/22/12
13
Dea
th, M
I or
Urg
ent R
evas
cula
rizat
ion
Unfractionated Heparin Enoxaparin (Lovenox)
Days
20
16
12
8
4
2 4 6 8 10 12 14 0
1 6 . 7 %
1 4 . 2 %
p = 0.03 Relative Risk Reduction = 15%
TIMI 11B: Enoxaparin vs. Heparin in NSTE-ACS
Adapted from Antman EM, et al. Circulation. 1999;100:1593-1601. 73 badri@gmc
Guidelines for the Use of Enoxaparin in Patients with NSTE-ACS
• 1 mg/kg SQ q12 hours (actual body weight) – An initial 30 mg IV dose can be considered
• Adjust dosing if CrCl <30 cc/min – 1 mg/kg SQ q24 hours
• Do not follow PTT; do not adjust based on PTT • Stop if platelets ↓ by 50% or below 100,000/mm3 • If patient to undergo PCI:
– 0-8 hours since last SQ dose: no additional antithrombin therapy – 8-12 hours since last SQ dose: 0.3 mg/kg IV immediately prior to
PCI
74 badri@gmc
ACC/AHA Recommendations for Antithrombin Therapy in Patients with NSTE-ACS
• Class I – Anticoagulation with subcutaneous LMWH or intravenous
UFH should be added to antiplatelet therapy – Dose of UFH 60-70 U/kg (max 5000) IV followed by infusion
of 12-15 U/kg/hr (initial max 1000 U/hr) titrated to aPTT 1.5-2.5 times control
– Dose of enoxaparin 1 mg/kg subcutaneously q12 hr; the first dose may be preceded by a 30-mg IV bolus
• Class IIa – Enoxaparin is preferable to UFH as an anticoagulant unless
CABG is planned within 24 hours
Available at: www.acc.org/clinical/guidelines/unstable/unstable.pdf.
75 badri@gmc
Early Invasive Strategy Studies and Recommendations in Patients with NSTE-ACS
76 badri@gmc
Months
4%
20%
16%
12%
8%
TACTICS
1 2 3 4 5 6
15.9%
19.4% Initial Medical Rx
Early Cath + PTCA
Adapted with permission from Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887. Copyright © 2001, Massachusetts Medical Society. All rights reserved.
77 badri@gmc
The Primary Composite Ischemic End Point in RITA-3
Reproduced with permission from Fox KA, Poole-Wilson PA, Henderson RA, et al. Interventional versus conservative treatment for patients with unstable angina or non-ST-elevation myocardial infarction: the British Heart Foundation RITA 3 randomised trial. Randomised Intervention Trial of Unstable Angina. Lancet. 2002;360:743-751.
78 badri@gmc
4/22/12
14
ACC/AHA Class I Recommendations for Invasive and Medical Strategies in Patients with NSTE-ACS
• Class I – An early invasive strategy in patients with any high-risk
indicators: • Recurrent angina/ischemia at rest or with low-level activities • Elevated troponin • New or presumed new ST-segment depression • Recurrent angina/ischemia with CHF Sx and S3 gallop,
pulmonary edema, worsening rales, or new or worsening MR • High-risk findings on noninvasive stress testing • Depressed LVEF (<40%) • Hemodynamic instability • Sustained ventricular tachycardia • PCI with 6 months or prior CABG
– In the absence of any of the above high-risk indicators, either an early conservative or an early invasive strategy
Available at www.acc.org/clinical/guidelines/unstable/unstable.pdf.
79 badri@gmc
Peri- and Post-Discharge Therapies and Risk Modification
80 badri@gmc
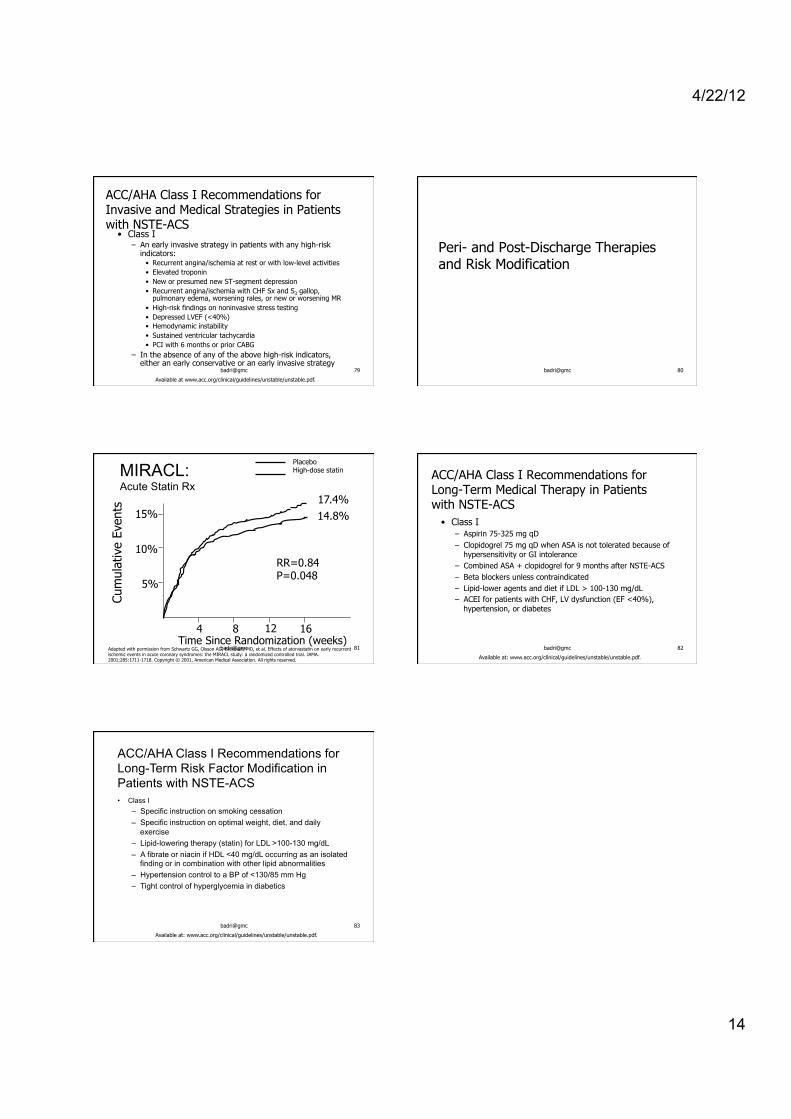
MIRACL: Acute Statin Rx
Cum
ulat
ive
Even
ts
5%
10%
15%
Time Since Randomization (weeks) 4 8 12 16
RR=0.84 P=0.048
17.4% 14.8%
Placebo High-dose statin
Adapted with permission from Schwartz GG, Olsson AG, Ezekowitz MD, et al. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA. 2001;285:1711-1718. Copyright © 2001, American Medical Association. All rights reserved.
81 badri@gmc
ACC/AHA Class I Recommendations for Long-Term Medical Therapy in Patients with NSTE-ACS
• Class I – Aspirin 75-325 mg qD – Clopidogrel 75 mg qD when ASA is not tolerated because of
hypersensitivity or GI intolerance – Combined ASA + clopidogrel for 9 months after NSTE-ACS – Beta blockers unless contraindicated – Lipid-lower agents and diet if LDL > 100-130 mg/dL – ACEI for patients with CHF, LV dysfunction (EF <40%),
hypertension, or diabetes
Available at: www.acc.org/clinical/guidelines/unstable/unstable.pdf.
82 badri@gmc
ACC/AHA Class I Recommendations for Long-Term Risk Factor Modification in Patients with NSTE-ACS • Class I
– Specific instruction on smoking cessation – Specific instruction on optimal weight, diet, and daily
exercise – Lipid-lowering therapy (statin) for LDL >100-130 mg/dL – A fibrate or niacin if HDL <40 mg/dL occurring as an isolated
finding or in combination with other lipid abnormalities – Hypertension control to a BP of <130/85 mm Hg – Tight control of hyperglycemia in diabetics
Available at: www.acc.org/clinical/guidelines/unstable/unstable.pdf.
83 badri@gmc







![Abstract arXiv:1804.00298v2 [cs.CV] 3 Apr 2018 · Badri Patro, Vinay P. Namboodiri IIT Kanpur { badri,vinaypn }@iitk.ac.in Abstract In this paper we aim to answer questions based](https://static.fdocuments.in/doc/165x107/5f2edba9794bcd20b26cb7fa/abstract-arxiv180400298v2-cscv-3-apr-2018-badri-patro-vinay-p-namboodiri.jpg)










