Type I Diabetes by Jinbao Cao Department of Chemistry 03/29/2011.
24
Type I Diabetes by Jinbao Cao Department of Chemistry 03/29/2011
-
Upload
marion-alexandrina-mathews -
Category
Documents
-
view
214 -
download
0
Transcript of Type I Diabetes by Jinbao Cao Department of Chemistry 03/29/2011.

Type I Diabetes by Jinbao Cao Department of Chemistry 03/29/2011

Universal Symbol for Diabetes
Diabetes is a group of diseases marked by high levels of blood glucose resulting from defects in insulin production, insulin action, or both.
Type 1: results from the body's failure to produce insulinType 2: results from insulin resistance, a condition in which cells fail to use insulin properly

Introduction
• Current situationDiabetes affects 25.8 million people, 8.3% of
U.S polulation Diabetes is the leading cause of kidney failure Diabetes is a major cause of heart disease
and stroke Diabetes is the seventh leading cause of
death in the United States
National Diabetes Fact Sheet, 2011
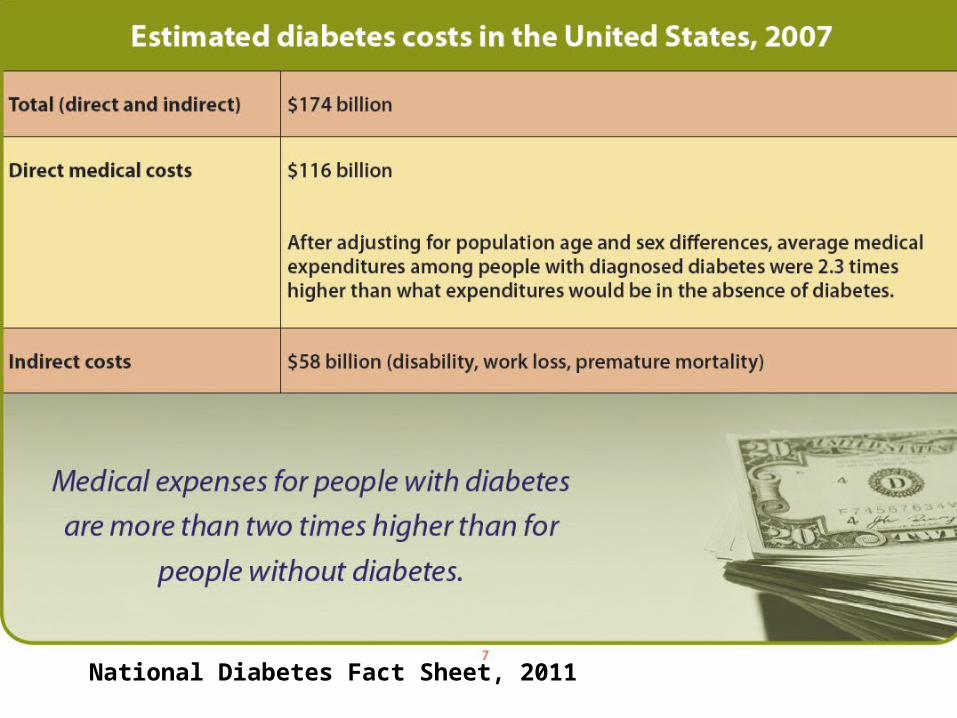
National Diabetes Fact Sheet, 2011

TYPE 1 Signs and Symptoms
• Polydipsia(increased thirst)• Polyphagia(Increased hunger)• Fatigue• Weight loss• Polyuria(frequent urination)

Cause of Type 1 Dibetes
Genetic: many different genes contribute to it
Enviromental
Diet: Wheat, Cow’s milk, Vitamin D, Brest milk etc.
Chemicals and Drugs: Vacor, Zanosasr
Virus
Vacor
Zanosar
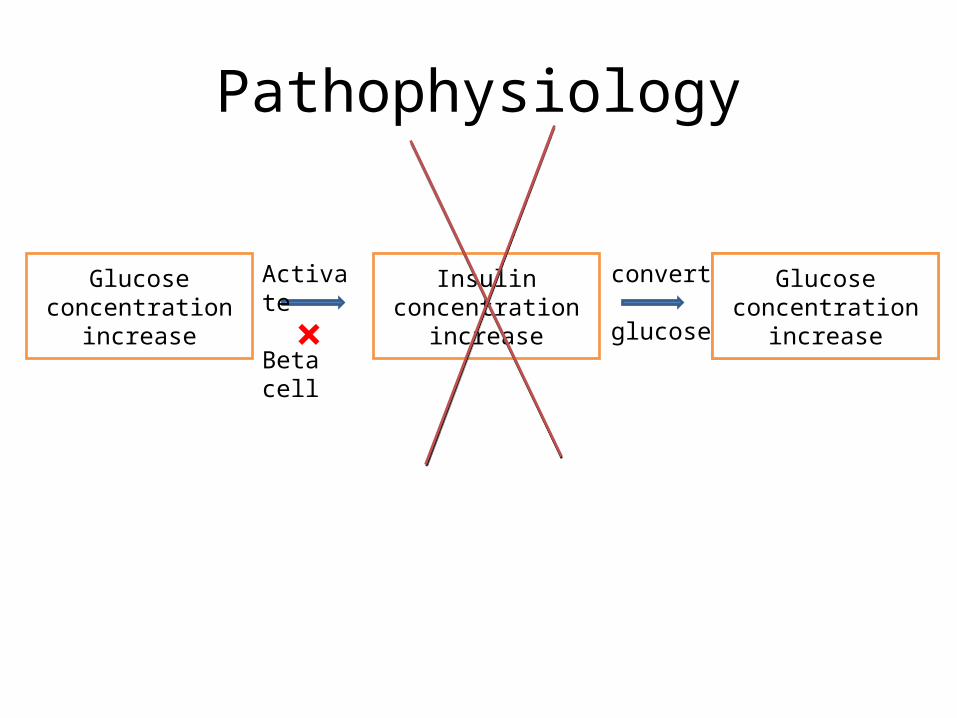
Pathophysiology
Glucose concentration
increase
Glucose concentration
decrease
Insulin concentration increase
Activate
Beta cell
convert
glucose×Glucose
concentration increase

Diagnose
Fasting plasma glucose level at or above 7.0mmol/L (126mg/dL) Plasma glucose at or above 11.1 mmol/L (200mg/dL) two hours after a 75 g oral glucoes load as in a glucose tolerance test

Treatment
• Daily injection of insulin - Under skin - Before meal - Several times - Can’t be swallowed
• Insulin pump• Oral meditation: Pramlintide (Symlin)• Health diet: fruits, vegetables, whole wheat• Excise: consume glucose

New Methods
• Polymeric materials used as drug delivery• Drugs can be bind to biodegradable polymer
pedant groups, when polymer breaks down, drug will be released continuously
• Stimuli responsive polymers. Temperature, pH, glucose etc.

Insulin
• A hormone regulating carbohydrate and fat metabolism in the body.
• Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle.
• When insulin is absent, body begins to use fat as energy source. Lose weight, high blood glucose concentration

Insulin history
• 1921 Frederick Banting and John Macleod first isolated insulin and successfully used to treat diabetes
• 1923 - MacLeod and Banting received Nobel Prize in Physiology and Medicine for insulin discovery
• 1955 Frederick Sanger won Nobel Prize in Chemistry for determining first order structure of insulin
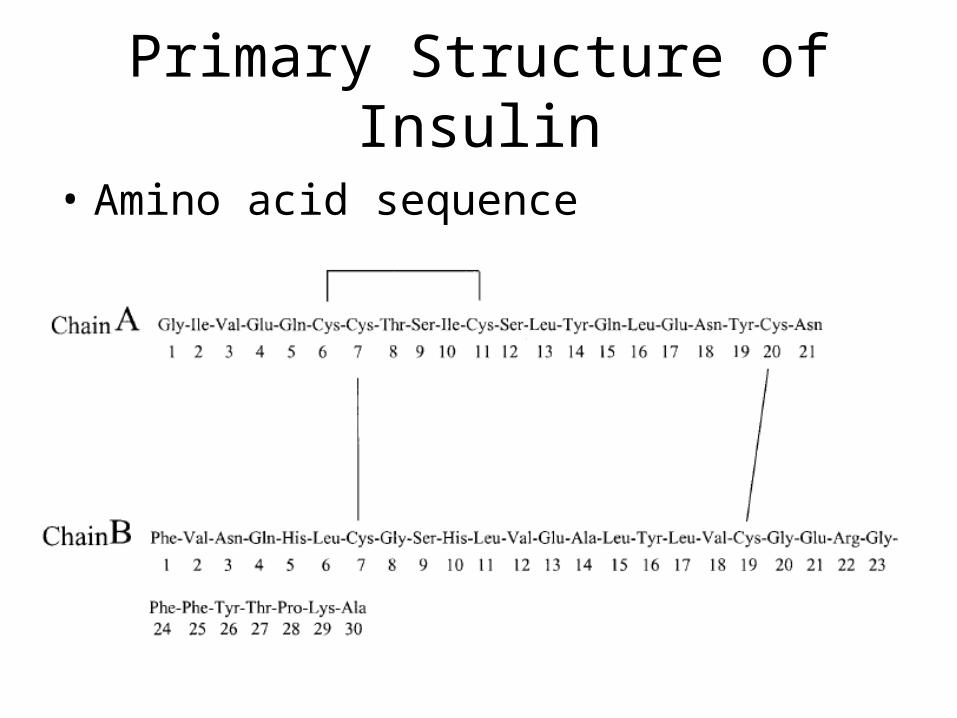
Primary Structure of Insulin
• Amino acid sequence

Secondary Structure of Insulin
• Hydrogen bonding stabilizes insulin
Blue: chain ARed: chain B

Tertiary Structure of Insulin
• Disulfide bond(yellow) -SH+-SH S-S• Disulfide bond formed Between 6 CYS residues• Two disulfide bond between Chain A and
Chain B, one between Chain A• In addition salt bridge and Van de Waals force also exist

Quaternary structure of Insulin
• Hydrophobic interaction between molecules• General form in beta cell and blood• Dimers also formed• Active form is single molecular

Synthesis of Insulin
• In vivo, produced within pancreas by cells. Pig insulin and cattle insulin are very similar to
human insulin• Chinese scientists firstly synthesized insulin
1965• Today, insulin is mostly made biosynthetically
by recombinant DNA technology or 'genetic engineering'.
Release of Insulin• First phase: triggered by increase blood GLU -Glucose enters the β-cells through the glucose transporter GLUT2 -Glucose goes into glycolysis and the respiratory cycle, where multiple high-energy ATP molecules are produced by oxidation -Dependent on the ATP:ADP ratio, and hence blood glucose levels, the ATP- dependent potassium channels (K+) close and the cell membrane depolarizes -On depolarization, voltage controlled calcium channels (Ca2+) open and calcium flows into the cells -An increased calcium level causes activation of phospholipase C, which cleaves the membrane phospholipid phosphatidyl inositol 4,5-bisphosphate into inositol 1,4,5-triphosphate and diacylglycerol. -Inositol 1,4,5-triphosphate (IP3) binds to receptor proteins in the membrane of endoplasmic reticulum (ER). This allows the release of Ca2+ from the ER via IP3 gated channels, and further raises the cell concentration of calcium. -Significantly increased amounts of calcium in the cells causes release of previously synthesized insulin, which has been stored in secretory vesicles
• Second phase: slowly release of newly formed insulin

Oscillations
• Insulin release from pancreas is not continuous• Oscillates within a period of 3-6min• Concentration from 100pmol/L—800pmol/L (A picomole is one-trillionth of a mole)• Guidance for injection of insulin
Degradation of Insulin
• Degraded one hour after release
• After work, either release back into extracellular environment or degraded by the cell
• Usually happens in liver or kindney

Questions
• What are the difference between type 1 and type 2 diabetes? To the level of the causes of two types.
• What are signs of type I diabetes?• What is major force for the secondary
structure of insulin?

Assigned reading
• Goodman and Gillman, Chapter 43, pp. 1237-1254 (large type only).
• Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia
(This a report of a WHO/IDF consultation, which introduces diabetes mellitus. You can read this report if you are interested. The precious questions are not based on this paper.)

Reference http://en.wikipedia.org/wiki/Diabetes_mellitus_type_1 http://en.wikipedia.org/wiki/Insulin National Diabetes Fact Sheet, 2011 Jeffrey A. Bluestone1, Vol 464(29) April 2010, Nature Bart O. Roep, Diabetologia (2003) 46:305–321 Definition and diagnosis of diabetes mellitus and intermediate
hyperglycemia