![CFRP [Wet-preg]](https://static.fdocuments.in/doc/165x107/546e6828b4af9faa268b4674/cfrp-wet-preg.jpg)
Two mifepristone doses and two intervals of misoprostol administration for termination of early preg
9
Two mifepristone doses and two intervals of misoprostol administration for termination of early pregnancy: a randomised factorial controlled equivalence trial* H von Hertzen, G Piaggio, D Wojdyla, L Marions, NT My Huong, OS Tang, AH Fang, SC Wu, L Kalmar, S Mittal, R Erdenetungalag, M Horga, A Pretnar-Darovec, A Kapamadzija, K Dickson, ND Anh, NV Tai, HTD Tuyet, A Peregoudov for the WHO Research Group on Post-ovulatory Methods of Fertility Regulation See Supporting Information for the full list of author affiliations Correspondence: Dr H von Hertzen, UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, Department of Reproductive Health and Research, WHO, 1211 Geneva 27, Switzerland. Email [email protected] Accepted 5 October 2008. Objective To compare the efficacy of 100 mg and 200 mg of mifepristone and 24- and 48-hour intervals to administration of 800mg vaginal misoprostol for termination of early pregnancy. Design Placebo-controlled, randomized, equivalence trial, stratified by centre. Setting 13 departments of obstetrics and gynecology in nine countries. Population 2181 women with 63 days or less gestation requesting medical abortion. Methods Two-sided 95% CI for the risk differences of failure to complete abortion were calculated and compared with 5% equivalence margin between two doses of mifepristone and two intervals to misoprostol administration. Proportions of women with adverse effects were compared between the regimens using standard testes for proportions. Outcome measures Rates of complete abortion without surgical intervention and adverse effects associated with the regimens. Results Efficacy outcome was analysed for 2126 women (97.5%) excluding 55 lost to follow up. Both mifepristone doses were found to be similar in efficacy. The rate of complete abortion was 92.0% for women assigned 100 mg of mifepristone and 93.2% for women assigned 200 mg of mifepristone (difference 1.2%, 95% CI: –1.0 to 3.5). Equivalence was also evident for the two intervals of administration: the rate of complete abortion was 93.5% for 24- hour interval and 91.7% for the 48-hour interval (difference –1.8%, 95% CI: –4.0 to 0.5). Interaction between doses and interval to misoprostol administration was not significant (P = 0.92). Adverse effects related to treatments did not differ between the groups. Conclusions Both the 100 and 200 mg doses of mifepristone and the 24- and 48-hour intervals have a similar efficacy to achieve complete abortion in early pregnancy when mifepristone is followed by 800 micrograms of vaginally administered misoprostol. Keywords Medical abortion, mifepristone dose, mifepristone- misoprostol interval. Please cite this paper as: von Hertzen H, Piaggio G, Wojdyla D, Marions L, My Huong N, Tang O, Fang A, Wu S, Kalmar L, Mittal S, Erdenetungalag R, Horga M, Pretnar-Darovec A, Kapamadzija A, Dickson K, Anh N, Tai N, Tuyet H, Peregoudov A, for the WHO Research Group on Post-ovulatory Methods of Fertility Regulation. Two mifepristone doses and two intervals of misoprostol administration for termination of early pregnancy: a randomised factorial controlled equivalence trial. BJOG 2009;116:381–389. Introduction The antiprogestin mifepristone followed by a suitable prosta- glandin analogue is registered for termination of early preg- nancy in more than 35 countries. In Europe and the USA, the approved regimen consists of 600 mg of mifepristone, fol- lowed 36–48 hours later by a prostaglandin analogue, most often misoprostol. The data from several multicentre trials conducted over the past 15 years demonstrate that a single dose of 200 mg of mifepristone has a similar efficacy to achieve complete *ISRCTN24130607; http://www.controlled-trials.com/INRCTN24130607/ ISRCTN24130607 ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 381 DOI: 10.1111/j.1471-0528.2008.02034.x www.blackwellpublishing.com/bjog Fertility control
-
Upload
ipas-mexico -
Category
Documents
-
view
212 -
download
0
description
Fertilitycontrol *ISRCTN24130607; http://www.controlled-trials.com/INRCTN24130607/ ISRCTN24130607 Theantiprogestinmifepristonefollowedbyasuitableprosta- glandinanalogueisregisteredforterminationofearlypreg- 381 Accepted5October2008. DOI:10.1111/j.1471-0528.2008.02034.x www.blackwellpublishing.com/bjog ª2009TheWorldHealthOrganization JournalcompilationªRCOG2009 BJOGAnInternationalJournalofObstetricsandGynaecology
Transcript of Two mifepristone doses and two intervals of misoprostol administration for termination of early preg

Two mifepristone doses and two intervals ofmisoprostol administration for termination ofearly pregnancy: a randomised factorialcontrolled equivalence trial*H von Hertzen, G Piaggio, D Wojdyla, L Marions, NT My Huong, OS Tang, AH Fang, SC Wu, L Kalmar,
S Mittal, R Erdenetungalag, M Horga, A Pretnar-Darovec, A Kapamadzija, K Dickson, ND Anh,
NV Tai, HTD Tuyet, A Peregoudov for the WHO Research Group on Post-ovulatory Methods of
Fertility Regulation
See Supporting Information for the full list of author affiliations
Correspondence: Dr H von Hertzen, UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in
Human Reproduction, Department of Reproductive Health and Research, WHO, 1211 Geneva 27, Switzerland. Email [email protected]
Accepted 5 October 2008.
Objective To compare the efficacy of 100 mg and 200 mg of
mifepristone and 24- and 48-hour intervals to administration of
800mg vaginal misoprostol for termination of early pregnancy.
Design Placebo-controlled, randomized, equivalence trial, stratified
by centre.
Setting 13 departments of obstetrics and gynecology in nine
countries.
Population 2181 women with 63 days or less gestation requesting
medical abortion.
Methods Two-sided 95% CI for the risk differences of failure to
complete abortion were calculated and compared with 5%
equivalence margin between two doses of mifepristone and two
intervals to misoprostol administration. Proportions of women
with adverse effects were compared between the regimens using
standard testes for proportions.
Outcome measures Rates of complete abortion without surgical
intervention and adverse effects associated with the regimens.
Results Efficacy outcome was analysed for 2126 women (97.5%)
excluding 55 lost to follow up. Both mifepristone doses were found
to be similar in efficacy. The rate of complete abortion was 92.0%
for women assigned 100 mg of mifepristone and 93.2% for women
assigned 200 mg of mifepristone (difference 1.2%, 95% CI: –1.0 to
3.5). Equivalence was also evident for the two intervals of
administration: the rate of complete abortion was 93.5% for 24-
hour interval and 91.7% for the 48-hour interval (difference –1.8%,
95% CI: –4.0 to 0.5). Interaction between doses and interval to
misoprostol administration was not significant (P = 0.92).
Adverse effects related to treatments did not differ between the
groups.
Conclusions Both the 100 and 200 mg doses of mifepristone and
the 24- and 48-hour intervals have a similar efficacy to achieve
complete abortion in early pregnancy when mifepristone is
followed by 800 micrograms of vaginally administered
misoprostol.
Keywords Medical abortion, mifepristone dose, mifepristone-
misoprostol interval.
Please cite this paper as: von Hertzen H, Piaggio G, Wojdyla D, Marions L, My Huong N, Tang O, Fang A, Wu S, Kalmar L, Mittal S, Erdenetungalag R, Horga M,
Pretnar-Darovec A, Kapamadzija A, Dickson K, Anh N, Tai N, Tuyet H, Peregoudov A, for the WHO Research Group on Post-ovulatory Methods of Fertility
Regulation. Two mifepristone doses and two intervals of misoprostol administration for termination of early pregnancy: a randomised factorial controlled
equivalence trial. BJOG 2009;116:381–389.
Introduction
The antiprogestin mifepristone followed by a suitable prosta-
glandin analogue is registered for termination of early preg-
nancy in more than 35 countries. In Europe and the USA, the
approved regimen consists of 600 mg of mifepristone, fol-
lowed 36–48 hours later by a prostaglandin analogue, most
often misoprostol.
The data from several multicentre trials conducted over
the past 15 years demonstrate that a single dose of 200 mg
of mifepristone has a similar efficacy to achieve complete*ISRCTN24130607; http://www.controlled-trials.com/INRCTN24130607/
ISRCTN24130607
ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 381
DOI: 10.1111/j.1471-0528.2008.02034.x
www.blackwellpublishing.com/bjogFertility control

abortion as the 600 mg dose.1–3 In addition, administration of
multiple small doses (five doses of 25 mg given at 12-hour
intervals), which is routine in China, was not significantly
different from a single dose of 600 mg.4 On the other hand,
the efficacy decreases when the dose of mifepristone is low-
ered to 50 mg.5 In a study on pharmacokinetics, oral admin-
istration of 100 mg or higher single doses of mifepristone
resulted in similar serum concentrations.6 Similar serum levels
can be explained by saturation of the binding capacity of the
carrier protein as mifepristone binds to the serum transport
protein alfa-1-acid glycoprotein, which limits its availability to
tissues. No previous studies, however, compared the 100 mg
dose with the commonly used dose of 200 mg of mifepristone.
Mifepristone pre-treatment leads to the softening and dila-
tion of the uterine cervix and it increases the sensitivity of the
uterine muscle to prostaglandins. It has been demonstrated
that the maximal sensitivity is achieved when mifepristone is
administered 36–48 hours before the prostaglandin analogue,7
and this is also the time interval to achieve maximal softening
and dilation of the uterine cervix.8 Consequently, the 36- to
48-hour interval was adopted as a standard for the medical
abortion regimen. Also, the data collected on 16 000 women
who had been treated with 600 mg of mifepristone followed by
a prostaglandin analogue 24–72 hours later suggested that the
efficacy was highest if the interval was 48 hours.9
Different time intervals between mifepristone and miso-
prostol have also been tested10 or both drugs have been
administered simultaneously,11 repeating the dose of miso-
prostol if abortion was not complete. When misoprostol
was not repeated, complete abortion rates seem to be signif-
icantly lower with shorter intervals.12 No previous studies had
been undertaken with a 100 mg dose of mifepristone when the
interval to misoprostol is 24 hours.
Based on the pharmacokinetics of mifepristone and the
published reports, we aimed to demonstrate that 100 mg
has a similar efficacy to 200 mg and that the 24- and 48-hour
intervals between mifepristone and misoprostol result in an
equivalent efficacy when using 800 micrograms of misopros-
tol administered vaginally (the null hypothesis being that
there is a difference in efficacy greater than a prestated margin
of 5%). A 24-hour interval would be more practical than 48-
hours and, if found effective, the 100 mg dose could be cheaper
than 200 mg, let alone the registered dose of 600 mg. This is
particularly important as the relatively high price of mifepris-
tone has limited its use in some countries despite its major
advantages as a pre-treatment.
We launched this randomised equivalence trial to test our
hypotheses for pregnancy termination among women with
gestational age of 63 days or less. Our main outcome was
complete abortion. We also studied adverse effects associated
with the use of these four regimens and the timing of expul-
sion. In addition, women were asked questions about their
perceptions of the treatments.
Methods
PatientsThe trial was undertaken in 13 departments of obstetrics and
gynaecology of teaching hospitals in Beijing and Shanghai,
People’s Republic of China; Hong Kong, Special Administra-
tive Region of China, Szeged, Hungary; New Delhi, India;
Ulaanbaatar, Mongolia; Targu Mures, Romania; Ljubljana,
Slovenia; Johannesburg, South Africa; Hanoi (two hospitals)
and Ho Chi Minh City, Viet Nam; and Novi Sad, Serbia.
Institutional review boards at each of the participating hos-
pitals and the WHO Secretariat Committee on Research on
Human Subjects gave ethics approval.
Women requesting early termination of pregnancy were
given information about the study, screened for eligibility
by clinic personnel if willing to participate and included if
they were healthy, older than the age of legal consent, had
haemoglobin level ‡100 g/l, intrauterine pregnancy with
duration £63 days verified by ultrasound, agreed to return
for follow-up visit(s) and agreeable, in principle, to surgical
termination of pregnancy should the treatment fail.
We excluded from this study women who had any indica-
tion of serious past or present illness, those allergic to mife-
pristone or misoprostol, chronic adrenal failure, severe
asthma uncontrolled by corticosteroid therapy, inherited
porphyria, heavy smokers (>20 cigarettes a day) with another
risk factor of cardiovascular disease, a history or evidence
of mitral stenosis, glaucoma, diastolic blood pressure >90
mmHg, systolic blood pressure <90 mmHg, history or evi-
dence of tromboembolism, evidence of liver disease, presence
of an IUD in utero, breastfeeding or haemolytic disorders. All
participants gave written informed consent before entering
the study. Relevant medical, gynaecological and obstetric his-
tories were recorded and bacteriological tests and Rh-typing
performed according to the routine of the centre.
Randomisation and interventionsA computer-generated randomisation sequence was produced
by WHO staff in Geneva to assign participants within each
centre to one of the four dose-interval combinations: 100 mg
of mifepristone and 800 micrograms of misoprostol 24 hours
later, 100 mg of mifepristone and 800 micrograms of misopros-
tol 48 hours later, 200 mg of mifepristone and 800 micrograms
of misoprostol 24 hours later and 200 mg of mifepristone and
800 micrograms of misoprostol 48 hours later. Mifepristone
was administered orally and misoprostol vaginally.
Each centre received assignments by randomly permuted
blocks with a fixed block size of 8. Randomisation was also
stratified by the gestational age (up to 49, 50–56 and 57–63
days). Allocation was concealed by the use of sealed, opaque,
sequentially numbered envelopes, which were filled and
labelled in accordance with the list of randomisation for each
centre by Magistra, Geneva, Switzerland. The 100 mg dose
von Hertzen et al.
382 ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

of mifepristone consisted of one tablet of 100 mg and one
placebo tablet and the 200 mg dose consisted of two tablets of
100 mg of mifepristone (Hualian Pharmaceuticals Ltd,
Shanghai, China). Placebo tablets were of similar shape and
colour as mifepristone tablets. The interval to misoprostol
(Cytotec; Monsanto, Paris, France) administration was not
blinded.
To establish the equivalent efficacy of the two doses of
mifepristone (100 and 200 mg) within each interval of miso-
prostol administration or of the two intervals between mife-
pristone and misoprostol (24 and 48 hours) within each dose
of mifepristone, we required the 95% CI for the difference in
complete abortion rates to be within the margin of equiva-
lence of 5% with a probability of 80%. This margin was cho-
sen using clinical judgement. If complete abortion rates by the
two doses (or with the two intervals) are both equal to 96%,
about 323 subjects will be required in each group, that is
a total of about 1300 subjects for the whole study. Allowing
for 10% of lost to follow up, at least 1450 subjects would have
to be recruited. In practice, 14 centres wished to participate,
each of them willing to recruit 156 women, that is a total of
2184 women for the whole study.
The primary outcome measure was efficacy of the treat-
ment in inducing complete abortion. Complete abortion
was defined as passing of the products of conception without
surgical intervention during the follow-up period; incomplete
abortion as expulsion of fetus but some products of concep-
tion remaining in uterus needing evacuation; missed abortion
as gestational sac in uterus without cardiac activity on ultra-
sound examination, needing emptying of the uterus; continu-
ing pregnancy as growing gestational sac with fetal heart
activity. If the woman discontinued the treatment and
requested vacuum aspiration before misoprostol administra-
tion or soon after it before the outcome could be known or
she was lost to follow up, the outcome was regarded as
undetermined.
The efficacy was assessed at the follow-up visits 2 and 6
weeks after the start of treatment.
Signs and symptoms were recorded before mifepristone,
before misoprostol and at 1, 2 and 3 hours after misoprostol
administration at the clinic as well as daily until the first
follow-up visit by women. Signs and symptoms were classified
as pregnancy related, treatment related and those related to
the abortion process itself.
ProceduresThe first dose of treatment (two tablets of 100 mg of mife-
pristone or one 100 mg of mifepristone tablet and one placebo
tablet) was administered at the clinic. Women returned either
24 or 48 hours later for vaginal administration of four tablets
of 200 micrograms of misoprostol each, after which they
stayed at the clinic for 3 hours under supervision, during
which period signs and symptoms were recorded hourly.
When leaving the clinic, the women were asked to keep a diary
about adverse effects and bleeding until the follow-up visit.
The initial clinical judgement about the outcome was made
at the first follow-up visit 2 weeks after the treatment. If the
findings at pelvic examination were suggestive of a continuing
pregnancy, an ultrasound examination was performed. In
case of live pregnancy, vacuum aspiration was performed.
If clinical findings were compatible with incomplete abortion,
no further action was taken unless judged necessary by the
investigator. For these women, the final outcome of therapy
was made at the second follow-up visit on day 43 of the study.
Statistical analysisData were analysed with SAS� System statistical software
(version 9.1.3) centrally at WHO. This trial was compliant
with CONSORT guidelines for reporting equivalence trials.13
An independent data monitoring committee reviewed the
data from two interim analyses performed after 509 and
1050 subjects were included in the study. According to the
protocol, a decision to discontinue a treatment regimen due
to low efficacy was based on the comparison with the regimen
of 200 mg of mifepristone followed by 800 micrograms of
misoprostol vaginally 48 hours later.
For the main analysis, women with unknown outcomes
due to lost to follow up were excluded. Additionally, a
per-protocol analysis excluding noncompliant cases was per-
formed. For each treatment regimen, percentages and
two-sided 95% CI were computed for complete abortion
and failure to complete abortion, which included incomplete
abortion, missed abortion, continuing live pregnancy and
undetermined outcomes.
Interaction between mifepristone dose and interval of
misoprostol administration was assessed adding an interac-
tion term to a logistic regression model including dose and
interval effects. Equivalence of mifepristone doses was
assessed within each interval of misoprostol administration
and also combining both intervals. Two-sided 95% CI for the
risk differences of failure to complete abortion were calcu-
lated by standard methods and compared with the equiva-
lence margin (5%). Similarly, equivalence of intervals of
misoprostol administration was assessed within each mife-
pristone dose and combining the doses. Analyses adjusting
by centre and baseline characteristics were carried out using
a logistic regression model. A stratified analysis by gestational
age was carried out together with comparisons of adverse
effect occurrence among the four regimens.
The role of funding sourceThe UNDP/UNFPA/WHO/World Bank Special Programme
of Research, Development and Research Training in Human
Reproduction funded this study including misoprostol tab-
lets. Mifepristone and placebo tablets were donated by
Hualian Pharmaceuticals Ltd. Neither the donors and
Mifepristone dose and interval to misoprostol administration for early abortion
ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 383
sponsors of the Programme nor Hualian Pharmaceuticals Ltd
had a role in the study design, data collection, data analysis,
data interpretation, writing of the report or the decision to
submit the paper for publication. The corresponding author
had full access to all final data in the study and had the final
responsibility for the decision to submit for publication.
Results
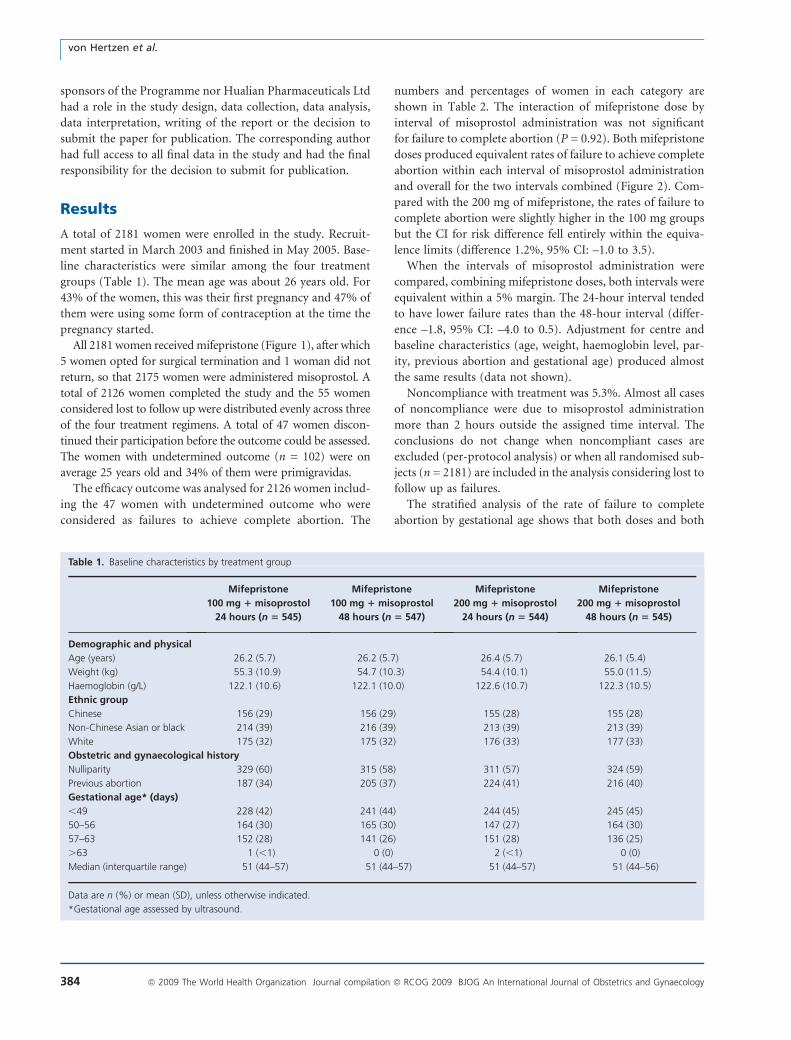
A total of 2181 women were enrolled in the study. Recruit-
ment started in March 2003 and finished in May 2005. Base-
line characteristics were similar among the four treatment
groups (Table 1). The mean age was about 26 years old. For
43% of the women, this was their first pregnancy and 47% of
them were using some form of contraception at the time the
pregnancy started.
All 2181women receivedmifepristone (Figure 1), after which
5 women opted for surgical termination and 1 woman did not
return, so that 2175 women were administered misoprostol. A
total of 2126 women completed the study and the 55 women
considered lost to follow up were distributed evenly across three
of the four treatment regimens. A total of 47 women discon-
tinued their participation before the outcome could be assessed.
The women with undetermined outcome (n = 102) were on
average 25 years old and 34% of them were primigravidas.
The efficacy outcome was analysed for 2126 women includ-
ing the 47 women with undetermined outcome who were
considered as failures to achieve complete abortion. The
numbers and percentages of women in each category are
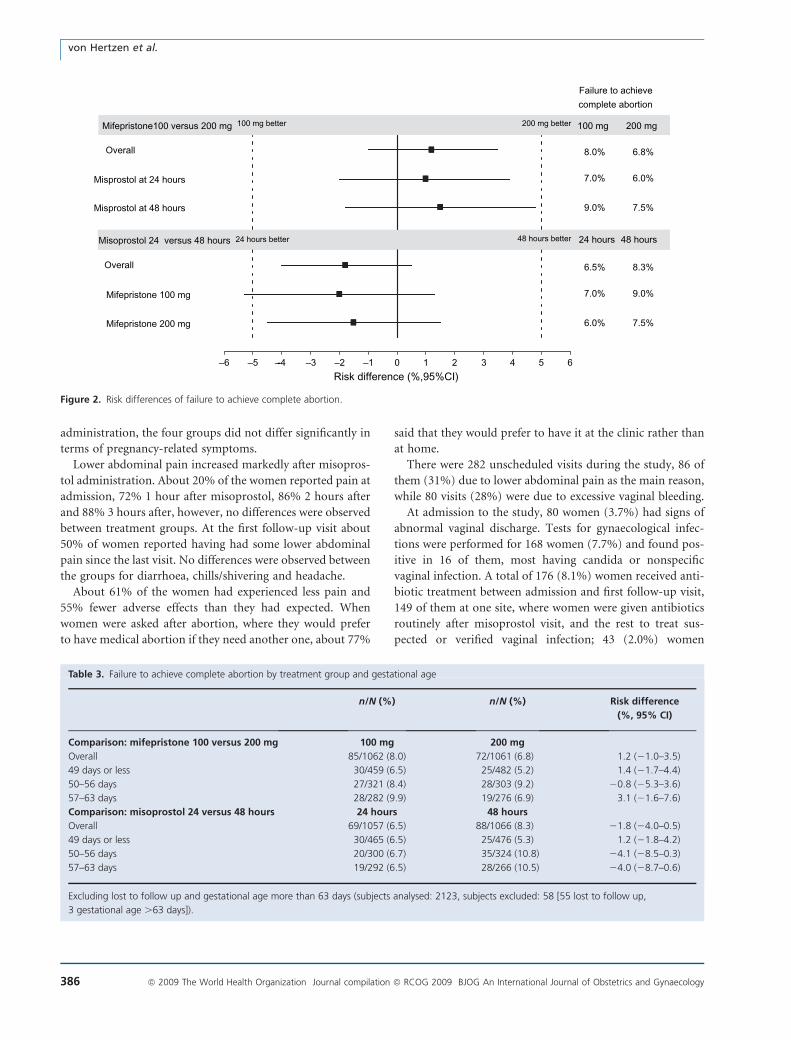
shown in Table 2. The interaction of mifepristone dose by
interval of misoprostol administration was not significant
for failure to complete abortion (P = 0.92). Both mifepristone
doses produced equivalent rates of failure to achieve complete
abortion within each interval of misoprostol administration
and overall for the two intervals combined (Figure 2). Com-
pared with the 200 mg of mifepristone, the rates of failure to
complete abortion were slightly higher in the 100 mg groups
but the CI for risk difference fell entirely within the equiva-
lence limits (difference 1.2%, 95% CI: –1.0 to 3.5).
When the intervals of misoprostol administration were
compared, combining mifepristone doses, both intervals were
equivalent within a 5% margin. The 24-hour interval tended
to have lower failure rates than the 48-hour interval (differ-
ence –1.8, 95% CI: –4.0 to 0.5). Adjustment for centre and
baseline characteristics (age, weight, haemoglobin level, par-
ity, previous abortion and gestational age) produced almost
the same results (data not shown).
Noncompliance with treatment was 5.3%. Almost all cases
of noncompliance were due to misoprostol administration
more than 2 hours outside the assigned time interval. The
conclusions do not change when noncompliant cases are
excluded (per-protocol analysis) or when all randomised sub-
jects (n = 2181) are included in the analysis considering lost to
follow up as failures.
The stratified analysis of the rate of failure to complete
abortion by gestational age shows that both doses and both
Table 1. Baseline characteristics by treatment group
Mifepristone
100 mg 1 misoprostol
24 hours (n 5 545)
Mifepristone
100 mg 1 misoprostol
48 hours (n 5 547)
Mifepristone
200 mg 1 misoprostol
24 hours (n 5 544)
Mifepristone
200 mg 1 misoprostol
48 hours (n 5 545)
Demographic and physical
Age (years) 26.2 (5.7) 26.2 (5.7) 26.4 (5.7) 26.1 (5.4)
Weight (kg) 55.3 (10.9) 54.7 (10.3) 54.4 (10.1) 55.0 (11.5)
Haemoglobin (g/L) 122.1 (10.6) 122.1 (10.0) 122.6 (10.7) 122.3 (10.5)
Ethnic group
Chinese 156 (29) 156 (29) 155 (28) 155 (28)
Non-Chinese Asian or black 214 (39) 216 (39) 213 (39) 213 (39)
White 175 (32) 175 (32) 176 (33) 177 (33)
Obstetric and gynaecological history
Nulliparity 329 (60) 315 (58) 311 (57) 324 (59)
Previous abortion 187 (34) 205 (37) 224 (41) 216 (40)
Gestational age* (days)
,49 228 (42) 241 (44) 244 (45) 245 (45)
50–56 164 (30) 165 (30) 147 (27) 164 (30)
57–63 152 (28) 141 (26) 151 (28) 136 (25)
.63 1 (,1) 0 (0) 2 (,1) 0 (0)
Median (interquartile range) 51 (44–57) 51 (44–57) 51 (44–57) 51 (44–56)
Data are n (%) or mean (SD), unless otherwise indicated.
*Gestational age assessed by ultrasound.
von Hertzen et al.
384 ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

administration intervals are equivalent when the gestational
age is 49 days or less (Table 3). The results are inconclusive
when the gestational age is 50 days or more: the trial was not
powered to show equivalence in subgroups.
Among 2051 women with complete and incomplete abor-
tion timing of expulsion was assessed for 1848 women (90%).
The median time to expulsion was 28 hours for regimens with
24-hour interval to misoprostol administration and between
51 and 52 hours in regimens with 48-hour intervals. There-
fore, it would appear that expulsion occurred in all groups
approximately 4 hours after misoprostol administration. No
differences were observed in time from misoprostol adminis-
tration to expulsion between the four regimens.
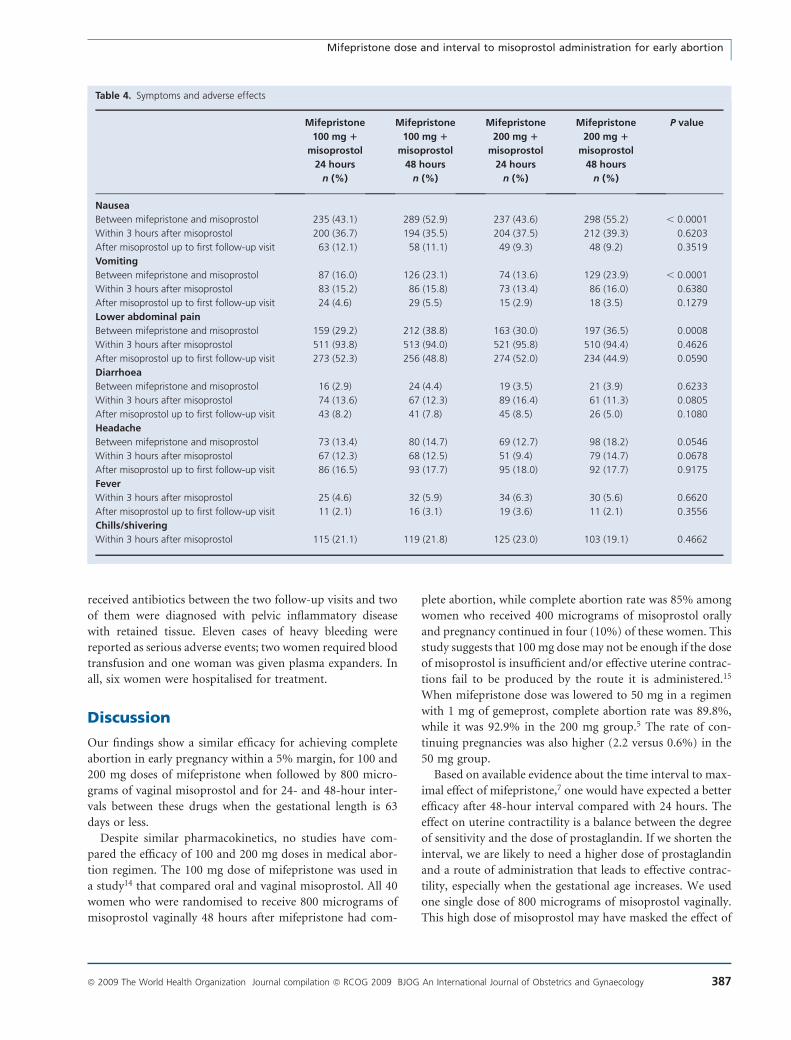
The percentage of women who reported pregnancy-related
symptoms (nausea and vomiting) and lower abdominal pain
after mifepristone administration and before misoprostol was
higher in the 48 hours of misoprostol administration interval
than in the 24-hour interval (Table 4). After misoprostol
3250 screened for elegibility
2707 eligible
543 not eligible
377 not willing to participate
149 did not participate forother reasons
2181 randomly assigned
545 assigned to100 mg of mifepristone+ 24 hours misoprostol
547 assigned to100 mg of mifepristone+ 48 hours misoprostol
544 assigned to200 mg of mifepristone+ 24 hours misoprostol
545 assigned to200 mg of mifepristone+ 48 hours misoprostol
529 analysed522 had first follow up
498 had second follow up11 VA
532 analysed521 had first follow up
497 had second follow up9 VA
531 analysed526 had first follow up
500 had second follow up10 VA
534 analysed525 had first follow up
503 had second follow up17 VA
4 VA1 VA
545 receivedmisoprostol at 24 hours
546 receivedmisoprostol at 48 hours
544 receivedmisoprostol at 24 hours
540 receivedmisoprostol at 48 hours
16 lost tofollow up
13 lost tofollow up
13 lost tofollow up
12 lost tofollow up
1 lost tofollow-up1 lost to
follow up
Figure 1. Flow chart.
Table 2. Efficacy outcome by treatment group
Outcome Mifepristone
100 mg 1 misoprostol
24 hours (n 5 529)
Mifepristone
100 mg 1 misoprostol
48 hours (n 5 534)
Mifepristone
200 mg 1 misoprostol
24 hours (n 5 531)
Mifepristone
200 mg 1 misoprostol
48 hours (n 5 532)
Total
Complete abortion 492 (93.0, 90.5–95.0) 486 (91.0, 88.3–93.3) 499 (94.0, 91.6–95.8) 492 (92.5, 89.9–94.6) 1969 (93)
Failure to complete abortion
Total 37 (7.0, 5.0–9.5) 48 (9.0, 6.7–11.7) 32 (6.0, 4.2–8.4) 40 (7.5, 5.4–10.1) 157 (7)
Incomplete abortion 17 (3.2, 1.9–5.1) 21 (3.9, 2.5–6.0) 17 (3.2, 1.9–5.1) 27 (5.1, 3.4–7.3) 82 (4)
Delayed abortion 3 (0.6, 0.1–1.7) 3 (0.6, 0.1–1.6) 1 (0.2, 0.0–1.0) 0 (0.0) 7 (,1)
Continuing pregnancy 6 (1.1, 0.4–2.5) 7 (1.3, 0.5–2.7) 4 (0.7, 0.2–1.9) 4 (0.7, 0.2–1.9) 21 (1)
Undetermined 11 (2.1, 1.0–3.7) 17 (3.2, 1.9–5.1) 10 (1.9, 0.9–3.4) 9 (1.7, 0.8–3.2) 47 (2)
Data are n (%, 95% CI) in different outcome categories.
Excluding lost to follow up (subjects analysed: 2126, subjects excluded: 55).
Mifepristone dose and interval to misoprostol administration for early abortion
ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 385
administration, the four groups did not differ significantly in
terms of pregnancy-related symptoms.
Lower abdominal pain increased markedly after misopros-
tol administration. About 20% of the women reported pain at
admission, 72% 1 hour after misoprostol, 86% 2 hours after
and 88% 3 hours after, however, no differences were observed
between treatment groups. At the first follow-up visit about
50% of women reported having had some lower abdominal
pain since the last visit. No differences were observed between
the groups for diarrhoea, chills/shivering and headache.
About 61% of the women had experienced less pain and
55% fewer adverse effects than they had expected. When
women were asked after abortion, where they would prefer
to have medical abortion if they need another one, about 77%
said that they would prefer to have it at the clinic rather than
at home.
There were 282 unscheduled visits during the study, 86 of
them (31%) due to lower abdominal pain as the main reason,
while 80 visits (28%) were due to excessive vaginal bleeding.
At admission to the study, 80 women (3.7%) had signs of
abnormal vaginal discharge. Tests for gynaecological infec-
tions were performed for 168 women (7.7%) and found pos-
itive in 16 of them, most having candida or nonspecific
vaginal infection. A total of 176 (8.1%) women received anti-
biotic treatment between admission and first follow-up visit,
149 of them at one site, where women were given antibiotics
routinely after misoprostol visit, and the rest to treat sus-
pected or verified vaginal infection; 43 (2.0%) women
–6 –5 - –3 –2 –1 0 1 2 3 4 5 6
Mifepristone100 versus 200 mg
Mifepristone 100 mg
Mifepristone 200 mg
Overall
Overall
Misprostol at 24 hours
Misprostol at 48 hours
Misoprostol 24 versus 48 hours
100 mg200 mg better100 mg better
24 hours better 48 hours better
Risk difference (%,95%CI)
200 mg
24 hours 48 hours
8.0% 6.8%
7.0% 6.0%
9.0% 7.5%
Failure to achieve
complete abortion
–-4
6.5% 8.3%
7.0% 9.0%
6.0% 7.5%
Figure 2. Risk differences of failure to achieve complete abortion.
Table 3. Failure to achieve complete abortion by treatment group and gestational age
n/N (%) n/N (%) Risk difference
(%, 95% CI)
Comparison: mifepristone 100 versus 200 mg 100 mg 200 mg
Overall 85/1062 (8.0) 72/1061 (6.8) 1.2 (21.0–3.5)
49 days or less 30/459 (6.5) 25/482 (5.2) 1.4 (21.7–4.4)
50–56 days 27/321 (8.4) 28/303 (9.2) 20.8 (25.3–3.6)
57–63 days 28/282 (9.9) 19/276 (6.9) 3.1 (21.6–7.6)
Comparison: misoprostol 24 versus 48 hours 24 hours 48 hours
Overall 69/1057 (6.5) 88/1066 (8.3) 21.8 (24.0–0.5)
49 days or less 30/465 (6.5) 25/476 (5.3) 1.2 (21.8–4.2)
50–56 days 20/300 (6.7) 35/324 (10.8) 24.1 (28.5–0.3)
57–63 days 19/292 (6.5) 28/266 (10.5) 24.0 (28.7–0.6)
Excluding lost to follow up and gestational age more than 63 days (subjects analysed: 2123, subjects excluded: 58 [55 lost to follow up,
3 gestational age .63 days]).
von Hertzen et al.
386 ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology
received antibiotics between the two follow-up visits and two
of them were diagnosed with pelvic inflammatory disease
with retained tissue. Eleven cases of heavy bleeding were
reported as serious adverse events; two women required blood
transfusion and one woman was given plasma expanders. In
all, six women were hospitalised for treatment.
Discussion
Our findings show a similar efficacy for achieving complete
abortion in early pregnancy within a 5% margin, for 100 and
200 mg doses of mifepristone when followed by 800 micro-
grams of vaginal misoprostol and for 24- and 48-hour inter-
vals between these drugs when the gestational length is 63
days or less.
Despite similar pharmacokinetics, no studies have com-
pared the efficacy of 100 and 200 mg doses in medical abor-
tion regimen. The 100 mg dose of mifepristone was used in
a study14 that compared oral and vaginal misoprostol. All 40
women who were randomised to receive 800 micrograms of
misoprostol vaginally 48 hours after mifepristone had com-
plete abortion, while complete abortion rate was 85% among
women who received 400 micrograms of misoprostol orally
and pregnancy continued in four (10%) of these women. This
study suggests that 100 mg dose may not be enough if the dose
of misoprostol is insufficient and/or effective uterine contrac-
tions fail to be produced by the route it is administered.15
When mifepristone dose was lowered to 50 mg in a regimen
with 1 mg of gemeprost, complete abortion rate was 89.8%,
while it was 92.9% in the 200 mg group.5 The rate of con-
tinuing pregnancies was also higher (2.2 versus 0.6%) in the
50 mg group.
Based on available evidence about the time interval to max-
imal effect of mifepristone,7 one would have expected a better
efficacy after 48-hour interval compared with 24 hours. The
effect on uterine contractility is a balance between the degree
of sensitivity and the dose of prostaglandin. If we shorten the
interval, we are likely to need a higher dose of prostaglandin
and a route of administration that leads to effective contrac-
tility, especially when the gestational age increases. We used
one single dose of 800 micrograms of misoprostol vaginally.
This high dose of misoprostol may have masked the effect of
Table 4. Symptoms and adverse effects
Mifepristone
100 mg 1
misoprostol
24 hours
Mifepristone
100 mg 1
misoprostol
48 hours
Mifepristone
200 mg 1
misoprostol
24 hours
Mifepristone
200 mg 1
misoprostol
48 hours
P value
n (%) n (%) n (%) n (%)
Nausea
Between mifepristone and misoprostol 235 (43.1) 289 (52.9) 237 (43.6) 298 (55.2) , 0.0001
Within 3 hours after misoprostol 200 (36.7) 194 (35.5) 204 (37.5) 212 (39.3) 0.6203
After misoprostol up to first follow-up visit 63 (12.1) 58 (11.1) 49 (9.3) 48 (9.2) 0.3519
Vomiting
Between mifepristone and misoprostol 87 (16.0) 126 (23.1) 74 (13.6) 129 (23.9) , 0.0001
Within 3 hours after misoprostol 83 (15.2) 86 (15.8) 73 (13.4) 86 (16.0) 0.6380
After misoprostol up to first follow-up visit 24 (4.6) 29 (5.5) 15 (2.9) 18 (3.5) 0.1279
Lower abdominal pain
Between mifepristone and misoprostol 159 (29.2) 212 (38.8) 163 (30.0) 197 (36.5) 0.0008
Within 3 hours after misoprostol 511 (93.8) 513 (94.0) 521 (95.8) 510 (94.4) 0.4626
After misoprostol up to first follow-up visit 273 (52.3) 256 (48.8) 274 (52.0) 234 (44.9) 0.0590
Diarrhoea
Between mifepristone and misoprostol 16 (2.9) 24 (4.4) 19 (3.5) 21 (3.9) 0.6233
Within 3 hours after misoprostol 74 (13.6) 67 (12.3) 89 (16.4) 61 (11.3) 0.0805
After misoprostol up to first follow-up visit 43 (8.2) 41 (7.8) 45 (8.5) 26 (5.0) 0.1080
Headache
Between mifepristone and misoprostol 73 (13.4) 80 (14.7) 69 (12.7) 98 (18.2) 0.0546
Within 3 hours after misoprostol 67 (12.3) 68 (12.5) 51 (9.4) 79 (14.7) 0.0678
After misoprostol up to first follow-up visit 86 (16.5) 93 (17.7) 95 (18.0) 92 (17.7) 0.9175
Fever
Within 3 hours after misoprostol 25 (4.6) 32 (5.9) 34 (6.3) 30 (5.6) 0.6620
After misoprostol up to first follow-up visit 11 (2.1) 16 (3.1) 19 (3.6) 11 (2.1) 0.3556
Chills/shivering
Within 3 hours after misoprostol 115 (21.1) 119 (21.8) 125 (23.0) 103 (19.1) 0.4662
Mifepristone dose and interval to misoprostol administration for early abortion
ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 387

the interval. With lower vaginal doses or with oral adminis-
tration of misoprostol or in later pregnancies, we might not
have obtained similar results. This was demonstrated in a sec-
ond-trimester abortion study16 in which the time until abor-
tion occurred was significantly longer (P < 0.0001) in the 1-
day interval group compared with 2-day interval between 200
mg of mifepristone and the start of administration of vaginal
misoprostol (400 micrograms at 3-hour intervals). Conse-
quently, the total dose of misoprostol given to women was
higher in the 1-day interval group.
A previous study that compared 1-, 2- and 3-day intervals
between 200 mg of mifepristone and 800 micrograms of vag-
inal misoprostol also reported similar rates of complete abor-
tion for both 1- and 2-day intervals.10 However, a second dose
of misoprostol was administered if abortion was not com-
plete, and it is not mentioned whether the need for additional
dose(s) was similar in all groups. Shorter than 24-hour inter-
vals between mifepristone and misoprostol have also been
tested or both drugs have been given at the same time. It
seems common for these studies that additional doses of
misoprostol are given to women who either do not abort or
do not have complete abortion. As abortion can also be
induced by multiple doses of misoprostol without mifepris-
tone,17 one may need to be cautious when drawing conclu-
sions about the efficacy of simultaneous administration when
additional misoprostol doses are given. One could question
whether these studies really compare different intervals if
insufficient success has to be compensated by additional
misoprostol doses to improve the results. When misoprostol
is administered at the same time with mifepristone and the
dose needs to be repeated even in early first trimester, the
benefits of mifepristone are partly lost and it is not clear
whether women abort with the combined regimen or multiple
doses of misoprostol.
The rates of complete abortion in all four arms of our
study were lower than in our previous studies.18 This is
likely to be due to the fact that several of the participating
centres do not provide medical abortion routinely because
mifepristone has not been licensed in their country. Expe-
rienced providers report higher complete abortion rates
than those with less experience.19 The comparison, however,
has internal validity as randomisation was within centres.
Rates of continuing pregnancies were low in all arms.
Whether pregnancies continue or not depends on the effi-
cacy of the regimen and the experience of providers have
little, if any, influence on it.
A higher percentage of women in the 48-hour interval
groups reported pregnancy-related symptoms such as nausea
and vomiting after mifepristone administration than women
in the 24-hour groups. This may be related to the fact that as
the time interval is longer, there is more chance to experience
these symptoms. This was also the case for lower abdominal
pain. As mifepristone sensitises the uterus also for endoge-
nous prostaglandins, uterine contractility is likely to increase
with time and can be experienced as painful. As the 24-hour
interval was associated with lower rates of these symptoms, it
is reasonable to recommend it, given its advantages and its
trend to a better efficacy.
The rate of suspected or verified infections in this study was
low. There has been discussion about whether routine pro-
phylactic antibiotic treatment is necessary when using medi-
cal abortion. The low rate of gynaecological infections after
treatment in this study does not support this practise.
This equivalence trial was designed with a prestated 5%
margin for the difference in percentage of women achieving
complete abortion. This margin was determined using clinical
assessment and it implies that a smaller difference is not clin-
ically relevant. Using a smaller margin would have implied
conducting a larger trial.
This trial has strong internal validity with a clear research
question and clearly defined primary and secondary outcome
measures. The sample size was calculated according to the
prestated hypothesis, randomisation and concealment of the
random allocation were used and both as randomized and
per-protocol analyses were performed (as recommended for
equivalence trials).
This trial also has external validity as it enrolled women of
several different populations and included centres with dif-
ferent levels of experience with medical abortion. Thus, the
results are likely to apply to wider populations.
In conclusion, our results show that for the termination of
early pregnancy (£63 days’ of gestation), mifepristone dose
could be lowered to 100 mg and the administration interval
shortened to 24 hours when using vaginal misoprostol of 800
micrograms.
Contributions to authorshipH.v.H., in collaboration with the members of the Steering Commit-
tee, was responsible for the conception of the trial and selection of
centres. H.v.H.and G.P. prepared the protocol. O.S.T., A.H.F.,
S.C.W., L.K., S.M., R.E., M.H., A.P.-D., A.K., K.D., N.D.A., N.V.T.,
and H.T.D.T. contributed to the final trial protocol and implemented
the trial in their respective countries. H.v.H., G.P. and L.M. super-
vised the trial. G.P. and D.W. were responsible for the statistical
analysis and N.T.M.H. and A.P. for the data management. H.v.H.,
G.P. and D.W. wrote the paper with inputs from the investigators.
WHO Research Group for the trialThe full list can be found in the online supporting information.
Country collaboratorsThe full list can be found in the online supporting information.
Conflict of interest statementOverall responsibility for this paper lies with Dr H.v.H. of the UNDP/
UNFPA/WHO/World Bank Special Programme of Research, Devel-
opment and Research Training in Human Reproduction, WHO.
von Hertzen et al.
388 ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

Neither she nor the Special Programme or any of its cosponsors have
a conflict of interest.
Ethics approvalInstitutional review boards at each of the participating hospitals and
the WHO Secretariat Committee on Research on Human Subjects
gave ethics approval.
AcknowledgementsThe study was funded by the UNDP/UNFPA/WHO/World Bank
Special Programme of Research, Development and Research Train-
ing in Human Reproduction. We thank the members of the Data and
Safety Monitoring Board for their contribution to interim analyses
and their valuable comments on the manuscript. Grateful thanks are
also due to P Van Look for his critical review of the manuscript.
Supporting information
Additional Supporting Information may be found in the
online version of this article:
List of author affiliations and WHO group and country
collaborator lists.
Please note: Wiley-Blackwell is not responsible for the con-
tent or functionality of any supporting information supplied
by the authors. Any queries (other than missing material)
should be directed to the corresponding author. j
References
1 World Health Organization Task Force on Post-ovulatory Methods for
Fertility Regulation. Termination of pregnancy with reduced doses of
mifepristone. BMJ 1993;307:532–7.
2 World Health Organization Task Force on Post-ovulatory Methods for
Fertility Regulation. Comparison of two doses of mifepristone in com-
bination of misoprostol for early medical abortion: a randomized trial.
BJOG 2000;107:524–30.
3 World Health Organization Task Force on Post-ovulatory Methods
for Fertility Regulation. Medical abortion at 57 to 63 days’ gestation
with a lower dose of mifepristone and gemeprost: a randomized con-
trolled trial. Acta Obstet Gynecol Scand 2001;80:447–51.
4 World Health Organization Task Force on Post-ovulatory Methods for
Fertility Regulation. Pregnancy termination with mifepristone and
gemeprost: a multicentre comparison between repeated doses and
a single dose of mifepristone. Fertil Steril 1991;56:32–40.
5 World Health Organization Task Force on Post-ovulatory Methods for
Fertility Regulation. Lowering the doses of mifepristone and geme-
prost for early abortion: a randomised controlled trial. BJOG 2001;
108:738–42.
6 Heikinheimo O, Kekkonen R. Dose-response relationship of RU 486.
Ann Med 1993;25:71–6.
7 Bygdeman M, Swahn ML. Progesterone receptor blockage–effect on
uterine contractility and early pregnancy. Contraception 1985;32:45–51.
8 Ashok PW, Flett GM, Templeton A. Mifepristone versus vaginally
administered misoprostol for cervical priming before first-trimester ter-
mination of pregnancy: a randomized, controlled study. Am J Obstet
Gynecol 2000;183:998–1002.
9 Ulmann A, Silvestre L, Chemama L, Rezvani Y, Renault M, Aguillaume
CJ, et al. Medical termination of early pregnancy with mifepristone
(RU486) followed by a prostaglandin analogue. Study in 16,369
women. Acta Obstet Gynecol Scand 1992;71:278–83.
10 Schaff EA, Fielding SL, Westhoff C, Ellertson C, Eisinger SH, Stadalius
LS, et al. Vaginal misoprostol administered 1, 2, or 3 days after mife-
pristone for early medical abortion: a randomized trial. JAMA 2000;
284:1948–53.
11 Creinin MD, Schreiber CA, Bednarek P, Lintu H, Wagner M-S, Meyn LA
for the MAST Study Trial Group. Mifepristone and misoprostol admin-
istered simultaneously versus 24 hours apart for abortion. Obstet
Gynecol 2007;109:885–94.
12 Guest J, Chien PF, Thomson MA, Kosseim ML. Randomized controlled
trial comparing the efficacy of same-day administration of mifepris-
tone and misoprostol for termination of pregnancy with the standard
36-48 hour protocol. BJOG 2007;114:207–15.
13 Piaggio G, Elbourne DR, Altman DG, Pocock SJ, Evans SJ; CONSORT
Group. Reporting of noninferiority and equivalence randomized trials:
an extention of the CONSORT statement. JAMA 2006;295:1152–60.
14 Creinin MC, Pymar HC, Schwartz JL. Mifepristone 100 mg in abortion
regimens. Obstet Gynecol 2001;98:434–9.
15 Aronsson A, Bygdeman M, Gemzell-Danielsson K. Effects of mifepris-
tone on uterine contractility following different routes of administra-
tion. Hum Reprod 2004;19:81–4.
16 Heikinheimo O, Suhonen S, Haukkamaa M. One-and two-day mife-
pristone-misoprostol intervals are both effective in medical termination
of second trimester pregnancy. Reprod Biomed Online 2004;8:236–9.
17 von Hertzen H, Piaggio G, Huong NT, Arustamyan K, Cabezas E,
Gomez M, et al. Efficacy of two intervals and two routes of adminis-
tration of misoprostol for termination of early pregnancy: a randomized
controlled equivalence trial. Lancet 2007;369:1938–46.
18 von Hertzen H, Honkanen H, Piaggio G, Bartfai G, Erdenetungalag R,
Gemzell-Danielsson K, et al. WHO multinational study of three miso-
prostol regimens after mifepristone for early medical abortion: I Effi-
cacy. BJOG 2003;110:808–18.
19 Suhonen S, Heikinheimo O, Tikka M, Haukkamaa M. The learning
curve is rapid in medical termination of pregnancy–first year results
from the Helsinki area. Contraception 2003;67:223–7.
Mifepristone dose and interval to misoprostol administration for early abortion
ª 2009 The World Health Organization Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 389


















