Two Immunostimulants of the ENT sphere: Thymuline and ...
12
Two Immunostimulants of the ENT sphere: Thymuline and Echinacea Doctors Pierre Dorfman and Max Tétau (Paris) After a brief review of immunology aimed at better understanding of the mechanism that is involved during a viral and / or bacterial infection, the authors report the clinical experimental work in recent years on two homeopathic remedies that have demonstrated their effectiveness in the prevention of recurrent ENT disorders. The ENT sphere, its location and its anatomical structure, is a physical and biochemical barrier for effective protection of the organism [vis-a-vis] against respiratory pathogens. Bronchial secretions contain molecules with bactericidal or bacteriostatic action such as Lactoferrin (Lactoferrin is one of the components of the immune system of the body; it has antimicrobial activity (bacteriocide, fungicide) and is part of the innate defense, mainly at mucoses ), Transferrin (Transferrin is found in the mucosa and binds iron, thus creating an environment low in free iron, where few bacteria are able to survive) and Lysosyme (Lysozyme is part of the innate immune system. Reduced lysozyme levels have been associated with bronchopulmonary dysplasia in newborns.), which causes bacterial lysis (Lysis (Greek λύσις, lysis from lyein = to separate) refers to the breaking down of a cell, often by viral, enzymic or osmotic mechanisms that compromise its integrity. ) in the presence of complement [?]. There are also immunological mediators including interferon and it's inhibitory effect on viral replication which has been shown experimentally. Lymphoid formations localized in the nasopharynx ([adenoid]vegetations, tonsils) have an essential role in immune defense mechanisms. These involve two cell types: phagocytic cells (polymorphonuclear neutrophils, monocytes and macrophages), responsible for non-specific response or natural, and lymphocytic cells involved primarily in specific immunity was still called memory [?] During the immune reaction, nonspecific immunity is the first to intervene. At this stage, the inflammatory phenomena and processes of phagocytosis predominate. They promote the migration of leukocytes, particularly neutrophils and macrophages to the site of infection. Cells called natural killer or NK cells also participate in the elimination of cells infected by viruses. The specific immune response takes over when the first defense [is exceeded] has happened. Then it is a specific immune response directed against the causative organism, leading to long-term acquisition of specific immunity. This immune response, mediated by T-lymphocyte memory, has a role in the prevention of any subsequent reinfection due to this same germ. These two families of immunocompetent cells coexist in the tonsillar crypts: 90% lymphocytes and 10% monocytes and polymorphonuclear. Non specific immunity Specific Immunity not increased after re-infection increased after re-infection Soluble factors lysozyme, complement, acute antibody phase proteins (eg PCR[?], interferon) Cells phagocytic cells, NK cells T- lymphocytes Figure1:the main effectors of specific immunity and non specific (from: Immunologie Fondamentale et appliquee.1. Roitt et al.,Ed.MEDSI) Figure 1 presents the main effectors (effector n. A muscle, gland, or organ capable of responding to a stimulus, especially a nerve impulse.) of specific immunity and nonspecific immunity. On the basis of this classification, there are products and nonspecific immunostimulants, whose
Transcript of Two Immunostimulants of the ENT sphere: Thymuline and ...

Two Immunostimulants of the ENT sphere: Thymuline and EchinaceaDoctors Pierre Dorfman and Max Tétau (Paris)
After a brief review of immunology aimed at better understanding of the mechanism that isinvolved during a viral and / or bacterial infection, the authors report the clinical experimentalwork in recent years on two homeopathic remedies that have demonstrated their effectiveness in theprevention of recurrent ENT disorders. The ENT sphere, its location and its anatomical structure, is a physical and biochemical barrier foreffective protection of the organism [vis-a-vis] against respiratory pathogens. Bronchial secretions contain molecules with bactericidal or bacteriostatic action such as Lactoferrin(Lactoferrin is one of the components of the immune system of the body; it has antimicrobial activity (bacteriocide,fungicide) and is part of the innate defense, mainly at mucoses ), Transferrin (Transferrin is found in the mucosa andbinds iron, thus creating an environment low in free iron, where few bacteria are able to survive) and Lysosyme(Lysozyme is part of the innate immune system. Reduced lysozyme levels have been associated with bronchopulmonarydysplasia in newborns.), which causes bacterial lysis (Lysis (Greek λύσις, lysis from lyein = to separate) refers tothe breaking down of a cell, often by viral, enzymic or osmotic mechanisms that compromise its integrity. ) in thepresence of complement [?]. There are also immunological mediators including interferon and it's inhibitory effect on viralreplication which has been shown experimentally.Lymphoid formations localized in the nasopharynx ([adenoid]vegetations, tonsils) have an essentialrole in immune defense mechanisms.These involve two cell types: phagocytic cells (polymorphonuclear neutrophils, monocytes andmacrophages), responsible for non-specific response or natural, and lymphocytic cells involvedprimarily in specific immunity was still called memory [?]
During the immune reaction, nonspecific immunity is the first to intervene. At this stage, the inflammatory phenomena and processes of phagocytosis predominate. They promote the migration of leukocytes, particularly neutrophils and macrophages to the site ofinfection.Cells called natural killer or NK cells also participate in the elimination of cells infected by viruses.The specific immune response takes over when the first defense [is exceeded] has happened. Then it is a specific immune response directed against the causative organism, leading to long-termacquisition of specific immunity.This immune response, mediated by T-lymphocyte memory, has a role in the prevention of anysubsequent reinfection due to this same germ. These two families of immunocompetent cells coexist in the tonsillar crypts: 90% lymphocytes and10% monocytes and polymorphonuclear.
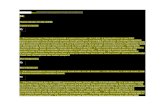
Non specific immunity Specific Immunity
not increased after re-infection increased after re-infection
Soluble factors lysozyme, complement, acute antibodyphase proteins (eg PCR[?], interferon)
Cells phagocytic cells, NK cells T- lymphocytes
Figure1:the main effectors of specific immunity and non specific (from: Immunologie Fondamentale et appliquee.1.Roitt et al.,Ed.MEDSI)
Figure 1 presents the main effectors (effector n. A muscle, gland, or organ capable of responding to a stimulus,especially a nerve impulse.) of specific immunity and nonspecific immunity.On the basis of this classification, there are products and nonspecific immunostimulants, whose
Karen Allen
Thymuline Materia Medica Article 1 of 2

action is exerted mainly on neutrophils, macrophages and indirectly on cells and mediators ofinflammation, and products with more specific action which have a direct effect on the processes ofeducation of T-lymphocytes.
ECHINACEA belongs to the first category, THYMULINE belongs to the second.Both homeopathic remedies prove to be quite complementary in their modes of action and cantherefore be used in the treatment of recurrent ENT diseases related with decreased immunedefenses.
THYMULINE
Thymulin by its specific effect on the immune system has been proposed to increase the clinicalcapabilities of humoral and cellular response. In fact, this hormone administered at too high doses proved unable to stimulate the immune system.The only significant results were obtained with Thymulin diluted and dynamised. Since the concept of immunomodulation uses low doses it has been generalized for other mediatorsof the immune system and has given rise to numerous therapeutic applications.A synthesis of the main work has been published recently in a reference book devoted toimmunomodulators (Bastide).
Experimental evaluation
Pharmacological models of ex vivo and in vitro developed in the immunology laboratory of Prof. M.Bastide (Montpellier) have served to demonstrate the activity of dilutions of THYMULINE onhumoral and cellular immunity (Bastide et al, 1987 ; Doucet-Jaboeuf et al, 1982; Doucet-Jaboeuf etal, 1985).
Immunocompromised mice (NZB) pretreated with 4 [doses?] of THYMULINE 12 CH show amarked increase in the production of antibodies specific to the test of "plaque-forming cells" (PFC)after immunization with sheep red blood cells. In this model, a decrease in humoral response is described in healthy mice.The study of cellular immunity by the method of release of chromium by cells after immunizationwith allospecific (P815) shows immunodeficient mice treated with dilutions of THYMULINE had asignificant increase in the cellular response.With these same dilutions an inverse response in healthy mice is observed. The immunodepression found among the healthy mice in these models is a negative regulator ofimmune processes brought into play by the injection of sheep red blood cells or P815 cells. (P815cells are used as an in vitro model to study tumour-specific cell-mediated immune responses and for viral transfectionstudies.)
In other experiments, it was shown that the diluted/dynamised Thymuline had a stimulating effecton Natural Killer response.
Japanese authors (Okamoto et al, 1993) have recently reported that a low dose of Thymuline (1 ng /kg) equivalent to an 5CH, could restore the humoral response test (PSC) of BALB / c micesubjected to forced immobilization. (BALB/c is an albino, laboratory-bred strain of the House Mouse fromwhich a number of common substrains are derived. Now over 200 generations from their origin in New York in 1920,BALB/c mice are distributed globally, and among the most widely used inbred strains used in animal experimentation.)This experience shows the importance of stress factors in the origin of certain disorders associatedwith lower immune defenses and the regulatory role of a physiological dose of Thymuline.

Definitions for Indications
Given its profile of activity, Thymulin in homeopathic dilutions has been suggested as animmunomodulator in the treatment of repeated nasopharyngitis, but also in most acute or chronicinfectious diseases associated with lower immune defenses. Its indications have, over the years, been better identified (Tetau, 1989).It is now commonly prescribed in dose 9 CH-granules in Influenza-like-Illness (ILI), together withInfluenzinum 9CH, in viral skin affections (herpes, zona), or characteristics of the tuberculardiathesis [such] as infectious mononucleosis, in ENT diseases (angina [tonsillaris], otitis), andrecurrent urinary infections (cystitis), in addition to biotherapeutic medication, and, finally, somerespiratory symptoms of allergic origin (hay fever, asthma ...).Thymuline should be considered as a complementary remedies for remedies widely used in thedisposition for recurrent Ear, Nose and Throat affections, such as Silica.
Clinical Validation
The immunostimulatory activity of thymulin 7 and / or 9 CH was compared to that of severalreference immunomodulators in the prevention of recurrences and complications of nasopharyngitisin a first study conducted during the winter 1988/89 (Huning et al, 1990). The analysis of 88 observations of children aged 1 to 6 years (Thymulin 9CH, n = 47;immunostimulants, n = 41) showed that the effectiveness of Thymulin was similar to that of thereference immunostimulants.There is no difference between the two types of treatment [vis-a-vis] when considering theevaluation criteria: number and duration of episodes, frequency of complications, number of dayson antibiotics.
Clinical investigations conducted since have confirmed these initial results.During the winter 1991/92 193 children aged 1 to 6 years who presented with at least two episodesof nasopharyngitis accompanied with fever over the past 12 months were recruited. Treatments consisted of either the prescription of Thymulin 9 CH, one dose-granules per week thefirst month, then every 15 days during the winter period, with or without a background ofhomeopathic medicines, or the administration of the recommended dose of referenceimmunostimulants. The clinical control showed a marked reduction in the number of episodes of nasopharyngitis andassociated complications (otitis, bronchitis ...) compared to the previous season. The effect of Thymulin 9 CH prescribed alone is comparable to that of immunostimulants.The administration of homeopathic drugs in addition to background Thymulin reduced thefrequency of infectious episodes even more significantly.
Clinical studies were also conducted in Italy to evaluate the immunomodulatory activity ofThymulin prescribed alone or in combination with other homeopathic remedies in the form of acomplex (Dolisobios no * 15).
• Study of Thymulin: Dr. La Torre, head of the Department of Pediatrics at the Hospital of Penne(Italy) studied the influence of a winter treatment by Thymulin 9 CH and objectively, on the onehand, a significant reduction of number of rhino-pharyngitis treated, equivalent to that obtainedwith the reference [control] product, and secondly, a significant increase in total lymphocyte or CD3in children treated for three months by Thymulin dilutions (p <0,05 test matches).
• Study of a complex base Thymulin: a population of 254 children aged 1 to 13 years with episodesof frequent nasopharyngitis and not treated with immunostimulants drugs was followed by aconsultation of the pediatric hospital Casorate (Pavia) by Drs G. Trapani and G. Legna during two

consecutive winters (1990/91 and 1991/92).
The first year, all infants were treated by symptomatic drugs, prescribed in cases of infectiousepisodes. The second year, half of the children (n = 127) received in November for five months involving ahomeopathic complex of Thymuline, Silicea and Calcarea sulfuricum 7/9 CH and Aconite,Mercurius solubilis and Nasopharyngeal Mucosa in 4/5 CH, administered one dose per week thefirst month, then one dose per month [for 5 months in total]. The same pattern as the previous year was applied to the other [control] group (n = 127). The two groups are strictly comparable vis-a-vis the distribution of age classes. A marked decrease in the total number of infective episodes after homeopathic treatment isobserved . The same trend is noted for the other evaluation criteria: duration of episodes, frequency ofcomplications, number of days on antibiotics. The overall assessment of the doctor is in favor of the effectiveness of treatment.The percentage of therapeutic failure (no significant improvement or deterioration) is 45% to 20%respectively for the control group and the treated group.
Guermonprez also tested Thymulin 9 CH and above in autoimmune diseases, PCR and dissiminatedlupus erythematosus, with encouraging but inconsistent results which confirm the "modulator"character of the activity of the product (Guermonprez et al, 1997).
ECHINACEA ANGUSTIFOLIA
The major homeopathic materia medica (Clarke, Duprat, Voisin ...) mention the interest of lowdilutions of Echinacea angustifolia in infectious syndromes and suppurative processes. The anti-infective activity of this plant, widely used in Germany may be related to its effect on theimmune system.
Many pharmacological and clinical studies carried out mainly by the team of Professor Wagner,have, indeed, confirmed the traditional use of Echinacea as an immunostimmulant and anti-infectives, and an hypotheses about its mechanism of action has been formulated.
Several active ingredients acting in synergy on different levels of the non-specific response seem tobe responsible for its immunostimulatory properties.Prescribed in low dilutions, Echinacea appears to be a drug of choice in the treatment of chronicinfectious diseases of viral or bacterial origin in children as in adults.
Experimental evaluation
By its complex chemical composition, Echinacea acts on different levels of nonspecific immuneresponse.
After administration of Echinacea, an increase in blood levels of Properdin (Properdin or factor P is aglobulin protein found in the blood serum of more complex animals. In the complement system, an innate-immunityseries of proenzymes dissolved in the circulation, it is also called "Factor P".), a protein of the alternativepathway of the complement system activation, is observed.This effect, mainly due to the echinaceine, is the cause of stimulation of the humoral nonspecific[immune] response, a key element of anti-infective activity of Echinacea.
Polysaccharides I and II would be responsible for an activity anti-hyaluronidase: they form acomplex polysaccharide hyaluronic acid, which indirectly inhibits hyaluronidase, an enzyme

produced by bacteria to promote their growth in tissue. (The hyaluronidases (EC 3.2.1.35) are a family ofenzymes that degrade hyaluronic acid .Wikipedia )Thus, the spread of bacteria would be limited and the focus of infection circumscribed.The echinaceine and polysaccharides of Echinacea also possess anti-inflammatory [properties],demonstrated experimentally using the carrageenan-induced rat paw edema test and testing of thegranuloma induced by croton oil in mice.
The immunostimulatory activity of Echinacea has been studied in mice through [the]carbonclearance test. This test involves injecting intravenously a suspension of colloidal carbon and measuring theresidual carbon concentration in the blood by photometry ex vivo.(Ex vivo (Latin: out of the living) meansthat which takes place outside an organism. In science, ex vivo refers to experimentation or measurements done in oron tissue in an artificial environment outside the organism with the minimum alteration of natural conditions.)Samples taken at different time can establish the kinetics of elimination of carbon particles whichare phagocytized in the liver at the spleen. Activation of phagocytosis leads to increased clearance of carbon.
The oral or interperitoneal administration of Echinacea induced relative to controls, increasedphagocytic index, reflecting the non-specific activation of granulocytes (Figure 2).Capacity assessment of phagocytosis of granulocytes was also performed in vitro. Cells isolated from human blood have been put into yeast, various extracts of Echinacea and freshserum.The number of phagocytosed yeast is counted by microscopy after staining and allows to determinean index of phagocytosis. As for the in vivo test, the answer lies in the stimulation of alternative pathway by the addition ofcomplement. The complement system is a biochemical cascade that helps, or “complements”, the ability ofantibodies to clear pathogens from an organism. It is part of the immune system called the innate immune system that isnot adaptable and does not change over the course of an individual's lifetime. However, it can be recruited and broughtinto action by the adaptive immune system. Functions of the Complement:The following are the basic functions of the complement
1. Opsonization - enhancing phagocytosis of antigens 2. Chemotaxis - attracting macrophages and neutrophils 3. Lysis - rupturing membranes of foreign cells 4. Clumping of antigen-bearing agents 5. Altering the molecular structure of viruses
Low concentration Echinacea extracts also show a significant non-specific immunostimulatoryactivity with phagocytosis indexes close to 30%.

More recently, a model in vitro using a macrophage culture has been developed by Professor M.Bastide (Faculty of Pharmacy, Montpellier) to study the anti-inflammatory and immuno-modulatoryaction of the 3 CH dilution of Echinacea angustifolia.
Nitrite production by macrophages was taken as the evaluation parameter. Ubiquitous chemical mediator, Nitric Oxide or NO is involved in many physiological mechanisms.It is currently one of the most powerful vasodilators known. Stimulation of macrophages by pathogens induces the release of NO and production of stablederivative, nitrite (NO2). These molecules play an important role in the genesis and maintenance of inflammatory processes. Their direct bactericidal activity was also demonstrated.
Macrophage lineage of the MALU (The MALU macrophage cell line is an in vitro coculture of mesothelial cellsand alveolar macrophages from mice) were incubated in the presence of a dilution of CH 3 Echinaceaangustifolia, or for 24 hours, either immediately before addition of LPS [LipoPolySaccharide],specific stimulation of macrophages.
The determination of nitrite by colorimetric method was performed after 48 h or 72 h of incubation.Six independent experiments were performed.The results show a significant increase (+21%) of the release of NO with the dilution of Echinacea3 CH compared with controls.
In humans, similar results were obtained with extracts from Echinacea administered orally orparenterally: trials versus placebo in healthy subjects show a stimulation of granulocytephagocytosis.
Definition of information
Echinacea is a drug traditionally prescribed to specific action in low dilutions of the MT to 4CH.The main indications of Echinacea in homeopathy are: - infectious syndromes: the patient is aching, presents with chills, nausea and drowsiness. - suppuration: abscess, phlegmon (Phlegmon is a spreading diffuse inflammatory process with formation ofsuppurative/purulent exudate or pus) or not associated with lymphangitis.
Echinacea is also used for the topical treatment of cutaneous wounds and a [good] gargle 5ml in aglass of water in case of beginning [onset] of tonsillitis, painful mouth ulcers and dental abscesses.
CLINICAL FACT SHEET
Drainage and to stimulate the immune defenses.
ECHINACEA ANGUSTIFOLIA
Orally in low dilutions and MT:
- children 15 to 30 drops, 1 to 2 times a day
- adults, 30 to 60 drops 1 to 2 times per day.
In courses of one week per month during the winter period.
Locally MT: 2 tablespoons in a glass of water, gargle 3 to 4 per day.

THYMULINE 9 CH
Usual dose: a dose-granules per week in the morning on an empty stomach for a month. Then onedose per month for five months.
Clinical ValidationAll studies on Echinacea confirm that hydro-alcoholic extracts administered in low dilutions inanimals and humans stimulate the non-specific immune system and promote resorption of the seatof inflammation.The use of Echinacea in homeopathy is guided by a specific reactivity of some subjects predisposedto recurrent infectious diseases (tubercular).Echinacea with its established immunostimulatory properties can therefore be proposed in thetreatment and prevention of recurrent respiratory and ENT disorders in children and in all infectiousdiseases associated with reduced immune defenses.
Drs P. Dorfman and M. Tetau
BibliographyBASTIDE (M.), BOUDARD (F.): An alternative concept of immunomodulation. In Forum onImmunomodulators.M. Guenounou ed., John Libbey Publishers, Paris, 1995, 303-316BASTIDE (M.), DAURAT (V.), DOUCET-JABŒUF (M.), PELEGRIN (A.), DORFMAN (P.):Immunomodulatory activity of very low doses of thymulin in mice. Int. J. Immunotherapy, 1987,3,pp. 191-200BAUER (R.), WAGNER (H.): Echinacea, der Sonnenhut. Stand der Forschung, Zeitschrift furPhytotherapie, 1988, 2, pp. 151-159.CICERI (A.), BARNOUIN (J.), GRANDMONTAGNE (Y.), GAVARET (T.), ENNE (G.): Studiodell'attivita'immunostimulante di un complesso omeopatico nei polli da carne. XVLI ConvegnoNazionale Societa Italiana Scienze Veterinaria, Brescia, sept. 1992.CLARKE (J.H.): A dictionary of practical materia medica. Rustington Health Science Press, 1962,3, p. 1624DORFMAN (P.), TÉTAU (M.): Applications cliniques de la recherche pharmacologique. Cahiersde Biothérapie, 1994, 125, pp. 51-56DOUCET-JABŒUF (M.), GUILLEMAIN (J.), PIECHACZYK (M.), KAROUBY (Y.), BASTIDE(M.): Évaluation de la dose limite d'activité du facteur Thymique sérique. CR Acad. Sci, 1982, 295,III, pp. 283-287GOETZ (P.): Echinacea. Potentialités immunostimmulantes et problèmes galénique. Revue dePhytothérapie pratique. 1989, 3, pp.14-19GUERMONPREZ (M.), PINKAS (M.), TORCK (M.): Thymuline. In Matière médicalehoméopatique. Lyon, Editions Boiron, 1997, p.485HUNIN (M.), TISSERAND (G.), DORFMAN (P.), TÉTAU (M.): Intérêt de la Thymuline dans laprévention des pathologies ORL récidivantes de l'enfants. Cahiers de Biothérapie. 1990, 107 suppl.,pp. 77-82JULIAN (O.A.): Influenzinum. In Traité de microimmunothérapie dynamisée. Paris, Le François,1977, 2, pp. 219-224JURCIC (K.), MELCHART (D.), HOLZMANN (M.), MARTIN (P.), BAUER (R.), DOENECKE(A.), WAGNER (H.): Stimulation de phagocytose granulocytaire par des préparations contenant unextrait d'Echinacea. 2 études cliniques. Phytotherapy. 1990, 31, pp.21-23

TÉTAU (M.): Observations cliniques sur Thymuline. Cahiers de Biothérapie. 1989, 103, pp. 51-52TÉTAU (M.): L'homéopathie végétale. Éditions Similia, Paris, 1990, pp.32-33TUBARO (A.), TRAGNI (E.), DEL NEGRO (P.), GALLI (C.L.), DELLA LOGGIA (R.): Anti-inflammatory activity of a polysaccharidie fraction of Echinacea angustifolia. J. Pharm. Pharmacol,1987, 39, pp. 567-569WAGNER (H.), PROKSCH (A.), RIESS-MAURER (I.), VOLLMAR (A.), ODENTUAL (S.),STUPPNER (H.), JURCIC (K.), LE TURDU (M.), FANG (J.N.): Immunstimmulierend wirkendePolysaccharide (Heteroglykane) aus höheren Pflanzen Arzneimittel Forschung, 1985, 35, 7, pp.1069-1075.

ThymulinumAlain Sarembaud
Homeopathic medicine has gained acclaim with the pathogenesis [provings] of traditional wellknown remedies. However, speaking at a symposium on allergic diseases in the eye and ENTspheres (homeopathic scientific institute, February 8, 2004), modernity allows us to recall a recentdrug, thymulin or thymulinum, listed among the classifications of homeopathic drugs, which is notreimbursed by health insurance funds, although widely prescribed.
Description
Thymuline is a hormone of the thymusgland present in the human serum and many animal species(1) designated as "serum thymic factor," which is principally engaged in the maturation of T-lymphocytes ( intra-thymic maturation and extra-thymic). This hormone also stimulates thehumoral and cellular responses. This product was obtained by peptide synthesis and its active part iscommon to most mammals, including mice and humans.
The work of Professor Madeleine Bastide (6, 7, 8, 10) showed the action of diluted and dynamizedthymulin in immunosuppressed mice to be a significant increase in humoral and cellular responses.To conduct this experiment, the protocol includes a first solution of thymulin 1 mg / ml of distilledwater and then successively diluted 1 / 100 and agitated (vortex for about thirty seconds or astimulus for two minutes). Immunomodulation is effected with dilutions of 10-9, 10-15, 10-19 and 10-23
corresponding respectively to 4 CH, 7 CH, 9 CH and 11 CH. Further dilutions were tested.Furthermore, in healthy mice, the experimenters have observed a significant decrease in the cellularresponse, the stimulation of NK response and a renewable effect with 9 CH. In diseasedimmunocompromised mice the experiment leads to rising CD4 T lymphocytes. These responses arehighly dependent on dilution. This work on diluted and dynamised "Immunomodulators" offers a new pharmacology based on thestimulation of the body by an exogenous element of information, not aggressive, according to themethod of Hahnemann.
Pathogenesis
For some, including Michel Guermonprez, Thymulinum has no pathogenesis [proving?] (19). Itsuse is based on the work of Professor Madeleine Bastide who extrapolated it's clinical use for adisorder attributed to immunity. This prescription is justified by the analogous action of otherremedies with systematic uses (Influenzinum, Oscillococcinum, etc) in this case it was ordered withsome success in children for repeated ENT disorders and adults with influenza, pharyngitis andrepeated winter viruses , see after vaccination. For others, like Max Tetau, Thymulinum is atubercular nosode which he has attributed with a "slight" pathogenesis.ORIGIN: nonapeptide [?]containing the metals (zinc, manganese, aluminum, etc.), isolated fromthymic factor and thymus homogenate lyophilized [?], obtained by peptide synthesis[?].
Causation- following a cold snap- following a viral respiratory infection - following vaccination (BCG, Pertussis, MMR)- following repeated E.coli infections
Karen Allen
Thymuline Materia Medica Article 2 of 2

Mind- Slender type (Phosphorus) with compromised immune system - rapidly decompensated in all affections- lively intellectual excitability - nervous, irritable, depressed, can not concentrate - nervous fatigue can be extreme
Generals- shaking with fatigue and need fresh air - nervousness, extreme sensitivity to cold, catch cold easily- weight loss despite periods of strong appetite contrasting with shorter stages of anorexia - agitated sleep with erotic dreams- headache, especially frontal, [from?] intellectual work
Digestive- tongue whitish coated with yellowish in the posterior half;- distaste for meat, desire for sweets- tendency to painless but tiring diarrhea, especially during febrile period; - pain right hypochondrium with heat, and around appendix
ENT and Respiratory- enlarged red tonsils with hypertrophy of cervical lymph node- recurrent rhinitis with purulent discharge, heat - Acute otalgia, mostly left, cold - catching cold from slightest chill- dry cough, hacking spasmodic, returning at night. The child is coughing all night, asphyxia.- cough < lying down - cough sputum is abundant, greenish or yellowish, at night- wheezing- pain at the base of the left lung- cough with nausea- cough > heat < cold ; cardiovascular- hypotension- frequent palpitations, tachycardia
Uro-genital- burning < before micturition > after- abundant urine, troublesome micturition, recurrent cystitis
Skin- perspires easily [despite?] nervousness- sweating hands and feet- perspiration back < at night, < coughing
Fever- period of high temperature, sudden and prolonged- dragging on febricula (a slight and short fever), apparently without cause- lymphocytosis with decreased CD4
Modalities- Aggravation from cold (but desires fresh air ):- in a closed room; by uncovering

- movement; by the sea as in the mountain, wine- Amelioration from heat, but requires a ventilated room; by rest; in the countryside
Sides- left
Complements- acute: Drosera, Pulsatilla- chronic: Nat mur, Sulfur iod, Tuberculinum, VAB, Aviare
Homeopath, P. Souk-Aloun, made a personal pathogenesis [proving] by taking 5 pellets Thymulin30CH morning and evening. In the morning of the third day he felt a strange oppression and a"rush", ideas crowding and jostling in his head. Other symptoms were: constipation, abdominalpain, dysphagia.
Clinical UsesWe distinguish four approaches:
The first is that of Michel Guermonprez, already mentioned, an integration into the homeopathicarsenal with with few modalized symptoms. however, it was tested in 9 CH and beyond inautoimmune diseases, PCR and systemic lupus erythematosus, with encouraging but inconsistentresults, which confirms its character as "modulator" [of the activity of the product].
The second is that of Max Tetau which encourages its use in influenza epidemics on the basis ofone dose of 9CH at the onset of symptoms [and] 24 hours later [?], and proposes it for recurrentENT problems in children, with remedies chosen by similarity: Thymulinum one dose per week thefirst month and then once weekly for five months. The most encouraging results are obtained inchildren "good responders" of the tubercular diathesis.
Still others have prescribed for AIDS patients in 5CH, 1 dose every two weeks. The effects are oftenassociated with increased CD4 lycocytes and an improvement of diarrhea. Sometimes observed inthe beginning of treatment, was an increase in volume and lymph node pain followed by animprovement. It seems that Thymulinum induces itching, and it should be avoided in children witheczema.The reviews of homeopathy used in AIDS are divided on the use of dilution and the choice of lowor high potency that may aggravate these cases. Others advise on these diseases 9 CH doses, threetimes a week.
For my part, I prescribe Thymulinum: • prevention of influenza disease among adults as a monthly dose 9 CH for 4 to 6 months.• in patients with allergies, difficult to define, 7 CH daily • in patients who underwent chemotherapy.
References
1. Bach J.-F., Dardenne M., Pleau J., Rosa J. - Biochemical characterization of serum thymic factor.In: Nature, 1977, 266: 55-57.2. Id, Thymulin (FTS-Zn). In: Clin. immunol. Allergy, 1983; 3:133-156.3. Bastide M., Doucet-Jabœuf M., Guillemain J., Pélegrin A., Tétau M. -Mise en évidence duprincipe de similitude par action des doses infinitésimales de thymus et d'hormone thymique chez lasouris. In: Cah. biothér., 1985;88:45-47.

4. Id., Doucet-Jabœuf M., Daurat V. - Activity and chronopharmacology of very low doses ofphysiological immune inducers. In: Immunol. Today, 1985;6:234-235.5. Id., Daurat V., Doucet-Jabœuf M., Pélegrin A., Dorfman P. - Immunomodulatory activity of verylow doses of thymulin in mice. In: Int. J. Immunotherapy, 1987;3:191-200.6. Id., Réflexions sur l'étude expérimentale de l'activité immunomodulatrice de certaines moléculesutilisées à doses infinitésimales. In: Cah. biothér., 1990;107 suppl.:45-49.7. Id., Boudard F. - Hautes dilutions et approche immunologique. In: Cah. biothér., 1993;120:29-378. Id., A novel concept of immunomodulation. In: Forum on Immunomodulators, M. GuenounouEd, John Libbey Publishers Paris, 1995;303-316.9. Id., Effet immunomodulateur de hautes dilutions de peptides issus du systéme immunitaire:Thymuline, Bursine, etc. In: Cah. biothér., 1999;160:41-46.10. Carrière V., Cabaner C., Casolari B., Bastide M. - Action de très faibles doses de thymuline surla pathologie pseudolupique des souris MRL/lpr. In: Cah. biothér., 1991;109:60-61.11. Daurat V., Dorfman P., Tétau M., Bastide M. - Modulation de la reponse immunitaire cellulairede la souris par des doses infra-pharmacologiques d'immunomédiateurs: thymuline, interferon ab,interleukine2. In: Cah. biothér., 1988;99:81-94.12. Desgor J. - Le drainage biotherapiques. In: Cah. biothér., 1996;142:49-50.13. Dorfman P., Tétau M. - Applications cliniques de la recherche pharmacologique. In: Cah.biothér., 1994;125:51-56.14. Id., Deux immunostimulants de la sphère ORL: Thymuline et Echinacea. In: Cah. biothér. 1997;148:47-52.15. Doucet-Jabœuf M., Guillemain J., Piechaczyk M., Karouby Y., Bastide M. - Évaluation de ladose limite d'activité du facteur thymique sérique. In: CR Acad SC., 1982;295:283-286.16. Duflo-Boujard O. - Affections oculaires dans les pathologies rhumatismales, les connectivites etles maladies auto-immunes. In: Homeop. europ., 1997;5(3):7-13.17. Affections oculaires dans les pathologies. In: Homeop. europ., 1998;7(3):26-33.18. Grandmontagne Y., Dorfman P., Tétau M. - État actuel de la recherche en homéopathievétérinaire. In: Cah. biothér. 1992;118:73-79.19. Guermonprez M, Pinkas M., Torck M. - Matière médicale homéopathique,Sainte-Foy-lès-Lyon,Boiron, 2/1997, p.485.20. Heiz J.-F. - Thymuline et types sensibles homéopathiques. In: Cah. biothér., 1993;119:21-22.21. Hunin M. - Les rhino-pharyngites des enfants. In: Cah. biothér., 1993-2000;164:49-54.22. Id., Tisserand G., Dorfman P., Tétau M. - Intérêt de la Thymuline dans le traitement préventifdes pathologies ORL récidivantes de l'enfant. In: Cah. biothér., 1990;107 suppl.:77-82.23. Libotte R. -La Prévention en homéopathie et en biothérapie. In: Cah. biothér., 1993;121:11-14.24. Pitron P. - Déficit immunitaire: application en clinique quotidienne de Thymuline. In: Cah.biothér., 1993;119:24-25.25. Id., Les fièvres éruptives. In: Cah. biothér., 1997;145:47-50.26. Sarembaud A. - Le syndrome grippal. In: Encyclopédie des médecines naturelles, t. i: Le Traité- Homéopathie,(sous la direction de P. Cornillot), Frison-Roche, 1995;393-398.27. Souk-Aloun P. - Quatre pathogénésies incomplès. Rev. belge homœop.,1994;27(2):73-80.28. Stinghe R. Homéopathie et gériatrie. In: Cah. biothér., 1992;116:29-37.29. Tétau M., - Biothérapies des affections hivernales. In: Cah. biothér.,1999;160:25-26.30. Id., Biothérapiques des états tuberculiniques. In: Cah. biothér., 1994;127:34-36.31. Id., Observations cliniques sur Thymuline. In: Cah. biothér., 1989;103:51-52.32. Id., Un grand nosode Tuberculinique: Thymuline. In: Cah. biothér., 1994;127:64-66.33. Id., Petites cliniques dermatologiques. L'herpès, le zona et les mycoses cutanées. In: Cah.biothér., 1997;145:37-40.34. Id., Présentation général des nosodes. In: Cah. biothér., 1993;123:7-20.35. Velin M. - Pathologies hivernales, homéopathie et grossesse. In: Cah. biothér., 1999;160:29-31.36. Vericel-Deloix M. - Asthme et sphère O.R.L. In: Cah. biothér., 1995;136:51-58.
Karen Allen
www.trinityhealthhub.com “We go together, you and I”