
Two approaches to development of new drugs for Chagas Disease.
Upload
florin-claudiu-hentaCategory
view
18download
0
Two Drugs and One Target: Women with HER2+ Breast Cancer
Two Drugs and One Target: Women with HER2+ Breast Cancer
February 29, 2008
By Kimberly Martin
POSTED IN: Drug development | breast cancer
TAGS: BIG, breast, cooperative, drug, groups, HER2,
herceptin, international, lapatinib, trastuzumab, treatment, trial,
tykerb
Molecular Targets for Breast Cancer
Scientists have uncovered molecular and genetic approaches to
identify specific genes, proteins, and molecular pathways that are important for cancer
development, growth, and survival. Understanding these biological mechanisms and how they
relate to cancer has been a key factor in the development and delivery of new biologic cancer
therapies, especially for breast cancer, which is the most frequently diagnosed form of cancer in
women worldwide. Knowing a tumor’s genetic profile allows clinicians to select the best treatment
for a patient without exposing them to drugs that will not be effective against their cancer [See
2006 BenchMarks issue on TAILORx at http://benchmarks.cancer.gov/2006/05/cancer-diagnostics-
informing-the-development-of-tailored-cancer-therapy/]. Targeting therapies to cellular pathways
specific to cancer also results in less toxicity to healthy cells in the body. This may allow clinicians
to treat patients for longer periods of time, if necessary, to prevent the cancer from recurring.
Many pathways are regulated through cell receptors — proteins on the surface or within a cell that
usually bind with a specific molecule (a ligand), resulting in a signal that tells the cell to take
action. These signals travel along pathways from the outer surface of the cell, carrying a message to
the cell’s nucleus. Cell signaling is a critical activity that regulates cell activities and ensures that
cells act in a coordinated, controlled manner. However, signals can be altered at many points along
the pathways, causing cells to function abnormally. In cancer, many of the altered pathways are
related to cell growth, proliferation, and survival.
Developing Targeted Drugs
Identifying signaling pathways that play a role in the development of cancer has allowed
researchers to develop drugs that fight cancer by targeting these pathways in cancer cells. Estrogen
is known to play an important role in the development of breast cancer and about 70 percent of all
breast cancers are estrogen-receptor positive; blocking the flow of the hormone estrogen to the
receptor can help starve the tumor. Tamoxifen, which has been used for more than 20 years to treat
breast cancer, was developed to block the estrogen receptor.
The HER2 gene is another factor that can influence tumor growth and aggressiveness in breast
cancer, so scientists have been investigating drugs that target the HER2 receptor for over a decade.
Trastuzumab (Herceptin ®), first approved by the FDA in 1998, was the first molecular-based
targeted treatment for metastatic breast cancer, and has since been approved for adjuvant treatment
(used in addition to other types of therapy such as surgical excision or radiation) of early breast
cancer. Trastuzumab is only effective in HER2+ breast cancer cells. Lapatinib (Tykerb ®) was
approved in 2007 for treatment of advanced, metastatic breast cancer in combination with the
chemotherapy drug capecitabine (Xeloda ®). It acts on a number of proteins including the HER2
receptor. Both trastuzumab and lapatinib disrupt cell signaling pathways, inhibiting tumor growth.
Mechanisms of Action against HER2
Normal breast cells contain two copies of the HER2 gene and produce appropriate amounts of
HER2 receptors to enable normal cell growth and division. Some breast tumor cells, however,
contain many more copies of the HER2 gene and in turn produce too many HER2 receptors — the
receptors are overexpressed. Approximately 20 to 25 percent of breast cancers overexpress HER2.
In addition to being more aggressive, tumors overexpressing HER2 are more likely to recur than
tumors that do not express HER2.
The HER2 receptor is a member of the family of cell surface receptors known as HER/ErbB or
human epidermal growth factors (EGFR). The four primary members of the HER family include
HER1/EGFR, HER2, HER3, and HER4. These are receptor tyrosine kinases, which are receptors
for molecules such as growth factors, cytokines, and hormones.
HER receptors have three components: an extracellular ligand-binding domain receptor that is
located outside the cell, a transmembrane domain that crosses the cell membrane, and an
intracellular tyrosine kinase domain that is inside the cell. When a ligand, such as a growth factor,
binds to a HER receptor’s extracellular domain, it causes the following cascade of effects:
Each HER receptor partners, or dimerizes, with a second receptor. HER receptors can
combine with the same type of receptor, such as HER1 to HER1, forming a homodimer, or
with another member of the HER family, such as HER1 to HER2, forming a heterodimer.
Dimerization activates the intracellular receptor kinase, which adds a phosphate molecule to
the tyrosine in the intracellular domain.
This addition of the phosphate molecule activates signaling pathways important in cell
proliferation and survival.
HER2, however, does not appear to have a ligand that promotes the formation of HER2
homodimers, but overexpression of HER2 can lead to HER2 homodimers, which may result in
signaling without the presence of a ligand. In addition, HER2 is the preferred partner of other HER
receptors so it may be a co-receptor for many different ligands. The type of partners in a
heterodimer is important, because it affects signal strength. Heterodimers containing HER2
generate stronger signals and prolonged activation of signaling pathways compared to heterodimers
without HER2. Overactivity of HER receptors plays a role in the growth of many cancers and in
their resistance to cancer therapy.
Evolving knowledge about the HER2 receptor in the development of breast cancer and its pathways
has been instrumental in the development of trastuzumab and lapatinib. Although these two drugs
are aimed at the HER2 receptor, they work in different ways. Trastuzumab blocks the HER2
receptor’s actions from outside the cell, while lapatinib works on the inside of the cell. This
difference may explain why lapatinib works in some women for whom trastuzumab is no longer
effective.
How Trastuzumab and Lapatinib Work
Trastuzumab is a monoclonal antibody. Antibodies are proteins made by the body’s immune system
that are directed against antigens, which are molecular components of foreign and infectious agents.
Monoclonal antibodies are created in the laboratory from a single cell and are engineered to bind to
a certain target. Trastuzumab is believed to fight cancer through several mechanisms of action. The
primary mechanisms are thought to be trastuzumab’s effects on cell signaling pathways and on
immune cells.
When trastuzumab binds with the HER2 receptor, it downregulates, or suppresses, the HER2 gene
causing fewer HER2 receptors to be expressed. This decreases HER2 dimerization and the
formation of heterodimers with other HER receptors, which interferes with cell signaling pathways.
Disruption at any point in a signaling pathway can have an effect on each subsequent step. Two
enzymes in particular are often affected. The mitogen-activated protein kinase (MAPK) and
phosphatidylinositol 3-kinase (PI3K)-AKT pathways are thought to be the most affected by
trastuzumab. These are complex signaling pathways in which a series of kinases activate
subsequent kinases in response to the addition of phosphate molecules:
MAPK is important for many cellular processes such as gene expression, division, and cell
survival.
The PI3-K/AKT signaling pathway has been linked to a diverse array of cellular functions
— most notably cell proliferation and survival.
The activity of these pathways contributes to cellular events that lead to the development of cancer.
Trastuzumab is thought to kill tumor cells not only by its direct action on tumor cell signaling but
also indirectly by attracting the body’s own immune cells to help destroy the cancer cells. When
trastuzumab binds to tumor cells, it attracts and activates immune cells called natural killer cells.
These immune cells attach to the bound trastuzumab molecule and release enzymes and factors that
kill the tumor cell. Studies have indicated that when trastuzumab is present, immune cells
preferentially target HER2 overexpressing cancer cells compared with cancer cells that do not
overexpress HER2.
Trastuzumab has been an important option for many women with HER2+ breast cancer, but
because cancer can mutate, it may eventually become resistant. Therefore, scientists have looked
for other drugs that can widen that target by inhibiting HER receptors through different
mechanisms.
Lapatinib is a dual tyrosine kinase inhibitor that targets two of the four HER family receptors —
HER1 and HER2. Like trastuzumab, it disrupts signaling in the MAPK and PI3K-AKT pathways,
but lapatinib stops HER signals from within a cell. Lapatinib competes with ATP for its binding
site on the tyrosine kinase domain of the receptor. When lapatinib binds to the ATP-binding site, it
blocks receptor phosphorylation and activation. This prevents subsequent signaling events along the
MAPK and PI3K/Akt pathways.
Difference Between Lapatinib and Trastuzumab
Both lapatinib and trastuzumab have shown progress as breast cancer treatments, but small
molecule dual kinase inhibitors have distinct mechanistic differences from large monoclonal
antibodies. Small molecules can be taken as a pill so they may be more convenient for patients,
especially working women who manage breast cancer as a chronic disease. Trastuzumab is a large
protein and must be administered intravenously.
About one-third of women with HER2 breast cancer develop brain metastases. Treatment with
trastuzumab does not seem to be as effective against advanced disease of this type. It may be too
big to cross the blood-brain barrier. However, lapatinib may be small enough to cross the blood-
brain barrier and enter brain tissues, which may make it effective in treating brain tumors and
metastasis.
Monoclonal antibodies are very specific to the targets to which they bind. They bind to the outside
of the cell by recognizing certain molecular structures at the binding site. If these structures are not
present, they cannot bind. In some tumors, the HER 1 and HER2 receptors lack the portion of the
molecule that sticks out above the cell’s membrane. Trastuzumab does not recognize these altered
HER receptors, so it does not bind to them. After a time, some women quit responding to treatment
with trastuzumab and the disease progresses. Trastuzumab resistance can be mediated, at least in
part, through expression of such a modified HER2 receptor.
Tyrosine kinase inhibitors lack this specificity. These molecules exert their effect by entering the
cell and interfering with signaling pathways. Dual tyrosine kinase inhibitors such as lapatinib can
target cancer cells with more than one type of HER receptor, which gives more options for
inhibiting the development of cancer and may be more useful in a wider range of patients.
Additionally, inhibiting heterodimers containing both HER1 and HER2 may be more effective than
targeting either HER1 or HER2 alone.
Since trastuzumab and lapatinib inhibit HER receptors by different methods, researchers are
investigating the efficacy of treating patients with these drugs simultaneously. In preclinical trials,
these drugs have been shown to have a synergistic effect against HER2+ breast cancer cells and
lapatinib was effective against cells that were resistant to trastuzumab. In an early phase study,
patients whose breast cancer had progressed while receiving trastuzumab responded, at least
partially, to treatment with lapatinib.
ALTTO (Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization trial), currently
underway in North America and Europe, is studying the efficacy of lapatinib, trastuzumab, their
sequence and combination in HER2+ early stage breast cancer. This international trial plans to
enroll 8,000 women and is conducted jointly by the Breast International Group and the North
Central Cancer Treatment Group, which is supported by the NCI. It is hoped that this trial will yield
an answer as to how effective these drugs may be in different combinations by the end of the
decade.
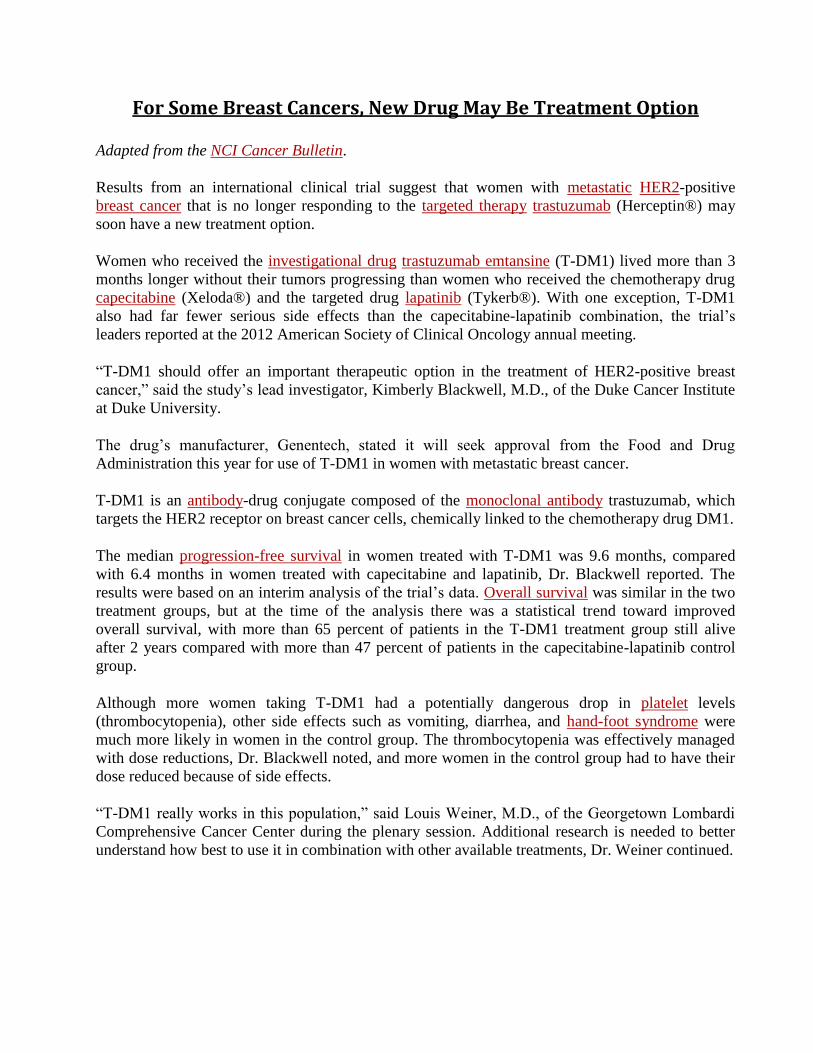
For Some Breast Cancers, New Drug May Be Treatment Option
Adapted from the NCI Cancer Bulletin.
Results from an international clinical trial suggest that women with metastatic HER2-positive
breast cancer that is no longer responding to the targeted therapy trastuzumab (Herceptin®) may
soon have a new treatment option.
Women who received the investigational drug trastuzumab emtansine (T-DM1) lived more than 3
months longer without their tumors progressing than women who received the chemotherapy drug
capecitabine (Xeloda®) and the targeted drug lapatinib (Tykerb®). With one exception, T-DM1
also had far fewer serious side effects than the capecitabine-lapatinib combination, the trial’s
leaders reported at the 2012 American Society of Clinical Oncology annual meeting.
“T-DM1 should offer an important therapeutic option in the treatment of HER2-positive breast
cancer,” said the study’s lead investigator, Kimberly Blackwell, M.D., of the Duke Cancer Institute
at Duke University.
The drug’s manufacturer, Genentech, stated it will seek approval from the Food and Drug
Administration this year for use of T-DM1 in women with metastatic breast cancer.
T-DM1 is an antibody-drug conjugate composed of the monoclonal antibody trastuzumab, which
targets the HER2 receptor on breast cancer cells, chemically linked to the chemotherapy drug DM1.
The median progression-free survival in women treated with T-DM1 was 9.6 months, compared
with 6.4 months in women treated with capecitabine and lapatinib, Dr. Blackwell reported. The
results were based on an interim analysis of the trial’s data. Overall survival was similar in the two
treatment groups, but at the time of the analysis there was a statistical trend toward improved
overall survival, with more than 65 percent of patients in the T-DM1 treatment group still alive
after 2 years compared with more than 47 percent of patients in the capecitabine-lapatinib control
group.
Although more women taking T-DM1 had a potentially dangerous drop in platelet levels
(thrombocytopenia), other side effects such as vomiting, diarrhea, and hand-foot syndrome were
much more likely in women in the control group. The thrombocytopenia was effectively managed
with dose reductions, Dr. Blackwell noted, and more women in the control group had to have their
dose reduced because of side effects.
“T-DM1 really works in this population,” said Louis Weiner, M.D., of the Georgetown Lombardi
Comprehensive Cancer Center during the plenary session. Additional research is needed to better
understand how best to use it in combination with other available treatments, Dr. Weiner continued.
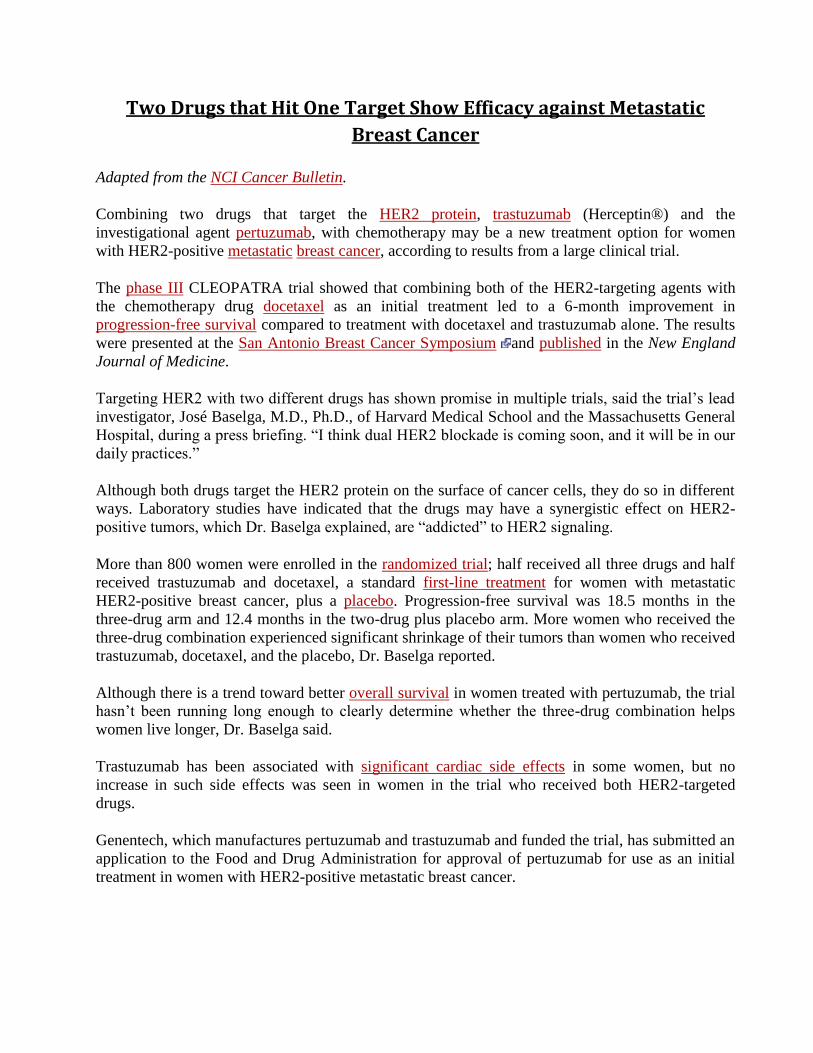
Two Drugs that Hit One Target Show Efficacy against Metastatic
Breast Cancer
Adapted from the NCI Cancer Bulletin.
Combining two drugs that target the HER2 protein, trastuzumab (Herceptin®) and the
investigational agent pertuzumab, with chemotherapy may be a new treatment option for women
with HER2-positive metastatic breast cancer, according to results from a large clinical trial.
The phase III CLEOPATRA trial showed that combining both of the HER2-targeting agents with
the chemotherapy drug docetaxel as an initial treatment led to a 6-month improvement in
progression-free survival compared to treatment with docetaxel and trastuzumab alone. The results
were presented at the San Antonio Breast Cancer Symposium and published in the New England
Journal of Medicine.
Targeting HER2 with two different drugs has shown promise in multiple trials, said the trial’s lead
investigator, José Baselga, M.D., Ph.D., of Harvard Medical School and the Massachusetts General
Hospital, during a press briefing. “I think dual HER2 blockade is coming soon, and it will be in our
daily practices.”
Although both drugs target the HER2 protein on the surface of cancer cells, they do so in different
ways. Laboratory studies have indicated that the drugs may have a synergistic effect on HER2-
positive tumors, which Dr. Baselga explained, are “addicted” to HER2 signaling.
More than 800 women were enrolled in the randomized trial; half received all three drugs and half
received trastuzumab and docetaxel, a standard first-line treatment for women with metastatic
HER2-positive breast cancer, plus a placebo. Progression-free survival was 18.5 months in the
three-drug arm and 12.4 months in the two-drug plus placebo arm. More women who received the
three-drug combination experienced significant shrinkage of their tumors than women who received
trastuzumab, docetaxel, and the placebo, Dr. Baselga reported.
Although there is a trend toward better overall survival in women treated with pertuzumab, the trial
hasn’t been running long enough to clearly determine whether the three-drug combination helps
women live longer, Dr. Baselga said.
Trastuzumab has been associated with significant cardiac side effects in some women, but no
increase in such side effects was seen in women in the trial who received both HER2-targeted
drugs.
Genentech, which manufactures pertuzumab and trastuzumab and funded the trial, has submitted an
application to the Food and Drug Administration for approval of pertuzumab for use as an initial
treatment in women with HER2-positive metastatic breast cancer.
Cancer News
NICE rejects lapatinib for advanced breast cancer
Thursday 10 June 2010
The National Institute for Health and Clinical Excellence (NICE) has decided not to recommend the oral drug lapatinib (Tyverb) for women with advanced breast cancer, except for use in clinical trials.
Lapatinib is designed to treat HER2-positive breast cancer, in which the tumour over-expresses the HER2 protein, which helps cancer cells to grow.
The drug works by blocking signals from the HER2 receptor on the surface of cells, thereby stopping cancer cells from growing and spreading.
Final draft guidance from NICE states that the drug is only recommended in combination with capecitabine (Xeloda) in the context of clinical trials for women with advanced or metastatic HER2-positive breast cancer.
But, those who are already receiving lapatinib should be allowed to continue taking the drug if they and their doctors wish.
NICE said that its decision was reached after an extensive consultation and evaluation of evidence, which suggested the drug has limited benefit and, at an overall cost of about £25,207 per year when combined with capecitabine, is not cost-effective.
The institute applied its new supplementary guidance for appraising treatments that may extend the lives of terminally ill patients, and took into consideration a cost-sharing proposal by the manufacturer.
Despite this proposal - under which the manufacturer would have met the cost of lapatinib for the first 12 weeks of each patient's treatment - NICE's appraisal committee concluded that the drug was still not a cost-effective use of NHS resources when compared with existing treatments.
Chief executive Sir Andrew Dillon revealed that the committee had been investigating lapatinib since 2007 and had conducted a "long and comprehensive" evaluation of the available evidence.
"We are disappointed not to be able to recommend lapatinib, but evidence suggests it only extends life by a small amount of time - around ten weeks (2.4 months) - and costs thousands of pounds more than one of the more commonly used NHS treatments for this indication - capecitabine on its own," he explained.
The committee also considered the potential of oral lapatinib to replace intravenous trastuzumab (Herceptin), which works in a similar way to lapatinib and is sometimes used in women with advanced breast cancer, even though it is not licensed for this purpose.
However, a lack of quality data meant that it was unable to fully assess the benefits of lapatinib in comparison to Herceptin.
Sir Andrew said: "The committee felt that it had not been presented with evidence of the drug's efficacy for specific groups of patients likely to continue treatment with trastuzumab (Herceptin) after their disease has progressed and that recommending lapatinib could serve to displace other cost-effective NHS treatments."
Manufacturers and other stakeholders have an opportunity to appeal against this final decision from NICE until June 24th 2010, after which final guidance will be published.
Hilary Tovey, policy manager at Cancer Research UK, said: "We are disappointed that NICE and the manufacturers have failed to come to a decision to make lapatinib available on the NHS.
"Cancer Research UK is already supporting clinical trials to find out whether lapatinib is more effective than other treatments for some women with breast cancer. We hope the results of these trials will provide better evidence to support the introduction of lapatinib on the NHS in the future."
Targeted Agents Active Against HER2-positive Breast Cancer:
Questions and Answers
Key Points
Trastuzumab (Herceptin), a drug developed in the 1990s to target HER2+ breast cancer, consists of a monoclonal antibody that once injected into patients, latches on to the portion of the HER2 protein that sits on the outer surface of the cancer cell. (Question 3)
Lapatinib (Tykerb) is an oral, small-molecule drug that is designed to strike multiple targets. It is a tyrosine kinase inhibitor that enters a cancer cell and binds to the part of the HER2 protein that juts beneath the cell surface, but researchers believe that it can also alter the function of other ErbB proteins that may be fueling cancer growth. (Question 4)
ALTTO is a trial that has been designed to examine which agent is more effective, which is safer for patients, and what benefit will be derived by taking the drugs separately, in tandem order, or together. (Question 6)
1. What are the different ways in which breast cancer is treated?
Breast cancer is the most commonly diagnosed cancer in women worldwide. Targeted therapies for
treating breast cancer have helped to reduce the death rate, according to results from clinical
studies. These treatments disable specific molecules in cancer cells that are necessary for growth
and survival of a tumor, unlike more general treatments, such as chemotherapy, that interfere with
all cells that may be dividing. Because targeted therapies are more precise, they generally have
fewer side effects. However, they also may have limited effectiveness in some patients whose
tumor growth depends on molecules that are not exclusively targeted by the agents or whose cancer
mutates to other growth pathways.
2. How is the HER2+ type of breast cancer different from other cancers?
A specific type of breast cancer called HER2+ (HER2-positive) is caused by an excess of HER2
genes or by over-production of its protein, the HER2 cell surface receptor. HER2 is a member of
the epidermal growth factor receptor (ErbB) family of genes which code for protein products
known as surface-bound tyrosine kinase proteins. Mutations or over-production of these molecules
stimulates cell division and uncontrolled growth. Fifteen to 20 percent of breast cancers are
HER2+. These tumors tend to grow faster and are generally more likely to recur than tumors that do
not overproduce HER2.
3. What drugs are available to treat HER2+ breast cancer?
There are two targeted agents that are U.S. Food and Drug Administration (FDA) approved for the
treatment of HER2+ breast cancer:
Herceptin (trastuzumab), a drug developed in 1990s to target HER2+ breast cancer, consists of large antibodies that once injected into patients, latch on to the portion of the HER2 protein that sits on the outer surface of the cancer cell. It was approved for use in the United States in 1998 and in Europe in 2000 to treat metastatic HER2+ breast cancer, in combination with chemotherapy. In
2006, European and U.S. regulators approved the use of trastuzumab, with chemotherapy, to treat early stage HER2+ breast cancer. Trastuzamab is given intravenously (into the vein).
Tykerb (lapatinib) was approved in 2007 in combination with capecitabine (a type of chemotherapy) for the treatment of advanced or metastatic HER2+ breast cancer in patients who have received prior treatment, including an anthracycline, a taxane and trastuzumab. It acts by entering a cancer cell and binding to the part of the HER2 protein that lies beneath the surface of the cell. Lapatinib is given orally (a pill by mouth).
4. Is trastuzumab always effective in HER2+ women?
While trastuzumab has reversed the course of HER2+ breast cancer in many patients, some patients
do not respond and others will acquire resistance to the agent. Edith Perez, M.D., an oncologist at
Mayo Clinic in Jacksonville, Fla., led a North Central Cancer Treatment Group (NCCTG) study
that showed a 52 percent reduction in cancer recurrence among women with early cancer who used
trastuzumab. Martine Piccart, M.D., Ph.D., professor of oncology at the Universite Libre de
Bruxelles, Belgium, led the HERA (HERceptin Adjuvant) trial, a Breast International Group (BIG)
study that showed very similar results.
5. How is lapatinib different from other drugs used to treat breast cancer?
Lapatinib is a second generation drug that is designed to strike multiple targets. It is a tyrosine
kinase inhibitor that enters a cancer cell and binds to the part of the HER2 protein that juts beneath
the cell surface. Its effect on the function of other ErbB proteins that may be fueling cancer growth
is also being studied. As a small molecule, it may be able to cross the blood-brain barrier to treat
the spread of breast cancer to the brain and central nervous system that trastuzumab cannot reach.
6. What studies have been done to prove the effectiveness of lapatinib?
To date, more than 60 clinical trials have been conducted for lapatinib. Specifically, the U.S. FDA
approval was based on a Phase III trial of 399 patients which showed that lapatinib plus
capecitabine provided a 28 percent to 43 percent reduction in risk of the disease progressing in
women with advanced or metastatic HER2+ breast cancer compared to chemotherapy alone.
Some studies have suggested that lapatinib can offer clinical benefit in HER2+ breast cancer that
does not respond to trastuzumab. While lapatinib is associated with side effects, it may not produce
the same kind of heart toxicity that can be seen with use of trastuzumab. Researchers really won't
know how promising lapatinib is until it is tested against trastuzumab.
7. What are some of the potential side effects of lapatinib and trastuzumab?
Both drugs have potential side-effects:
Lapatinib has been associated with reports of effects on the heart, in particular with a decrease in left ventricular ejection fraction. Diarrhea was the most common effect, resulting in discontinuation of study medication. Lapatinib has been associated with lung disease and pneumonitis (inflammation of lung tissue). Harm can occur to the fetus when administered to a pregnant woman and women should be advised not to become pregnant when taking the drug. Some of the most common adverse effects (greater than 20 percent) during treatment with
lapatinib plus the chemotherapy drug capecitabine were diarrhea, vomiting, nausea, fatigue, and rash.
Trastuzumab's side effects that most commonly occur during first treatment include fever and/or chills. Other possible side effects include pain, weakness, nausea, vomiting, diarrhea, headaches, difficulty breathing, and rashes. These side effects generally become less severe after the first treatment. Patients who receive trastuzumab along with chemotherapy may experience side effects that are different from those of patients who take trastuzumab by itself. For example, anemia (a condition in which the number of red blood cells is below normal) and infection, primarily mild upper respiratory infection, have been seen more often in patients given trastuzumab with chemotherapy compared with those receiving trastuzumab alone.
8. What is the ALTTO trial?
ALTTO is a trial designed to compare trastuzumab and lapatinib in women with early stage HER2+
breast cancer who have recently completed chemotherapy. Specifically, ALTTO will examine
which agent is more effective, which is safer for patients, and what benefit will be derived by taking
the drugs separately, in tandem order, or together. The ALTTO clinical trial is unique in that for all
8,000 patients, there will be a central pathology review of the primary tumor, including re-
evaluation of the cancer's estrogen receptor (ER), progesterone receptor (PR), and HER2 status
before patients are randomized. Then, patients with HER2+ tumors will be stratified according to
their ER/PR profile, lymph node involvement and chemotherapy use to determine whether hormone
status affects treatment. About 70 percent of breast cancer is predominantly HER2-negative and
ER/PR-positive, but HER2+ cancer can also exhibit estrogen receptors and/or progesterone
receptors on cancer cells.
9. How was the ALTTO trial modified in 2011?
On September 9, 2011, the leadership of ALTTO announced that it will discontinue Arm 2 of the
trial. The Independent Data Monitoring Committee review of efficacy in the trial was triggered
after a pre-specified number of events was reached, as outlined in the study’s protocol. An analysis
of these events showed a statistical imbalance in breast cancer recurrence between Arm 1 and Arm
2. According to Edith A. Perez, M.D., ALTTO principal investigator in the United States, and a
researcher with the North Central Cancer Treatment Group and Mayo Clinic, “participants assigned
to the lapatinib alone arm are not likely to do as well as participants assigned to trastuzumab alone.”
In this trial, all patients received other treatments as part of standard of care (such as chemotherapy,
radiation, anti-estrogens) after surgery, and were randomized to one of four different ways to
receive the two types of anti-HER2 therapy trastuzumab or lapatinib. The change in status of this
trial directly affects patients assigned to Arm 2, which are those patients receiving lapatinib alone.
For more information on this modification, go to the GlaxoSmithKline press release at
http://www.gsk.com/media/pressreleases/2011/2011-pressrelease-614837.htm and the ALTTO
trial website at http://alttotrials.com/patients.php .
10. How are tissue samples examined and stored in the ALTTO trial?
For ALTTO patients included in North America, paraffin samples of their tumors will be tested and
stored at the Mayo Clinic in Rochester, Minn. The European Institute of Oncology in Milan, Italy,
will test and store paraffin samples for Europe and the rest of the world. The data from these studies
can be used in future translational research studies. The outcome of that research will enable
researchers to better understand which patients are the best candidates for these targeted treatments.
11. What molecules will the ALTTO investigators focus on in the tumor samples?
Among the molecules evaluated from tumor samples will be the c-Myc oncogene (over-expression
of which is believed to make cancer extremely sensitive to trastuzumab), and the PTEN tumor
suppressor gene (because cancer which has lost this gene is thought to respond best to lapatinib).
Researchers will also collect information on p95 HER2, which are common truncations of the
normal HER2 protein that researchers suspect do not respond to trastuzumab.
12. What other biological samples will ALTTO collect?
Blood samples will be collected on all 8,000 patients to look for molecular markers that may
predict clinical outcome, and in a subset of 2,000 patients, additional blood and frozen tumor
samples will be gathered for future research on circulating tumor cells and proteomics (the study of
protein interactions). Those biological materials will be kept in Rochester, Minn., and in Brussels,
Belgium. All data resulting from the study will be held at BIG, and will be controlled and analyzed
by academic researchers.
13. How will ALTTO be funded?
Funding for ALTTO is provided by the National Cancer Institute (NCI), part of the National
Institutes of Health, and GlaxoSmithKline (GSK), the pharmaceutical company that developed
lapatinib. The NCI will contribute to each U.S. site a standard $2,000 per patient cost for the ten-
year study as well as the basic infrastructure for running all trials via existing grants. GSK's
contribution is considered proprietary information.

Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomised, open-label, multicentre, phase 3 trial
Dr José Baselga MD a b , Ian Bradbury PhD c d, Holger Eidtmann MD e, Serena Di Cosimo MD b f h, Evandro de Azambuja MD i, Claudia Aura MD g, Henry Gómez MD l, Phuong Dinh MD j, Karine Fauria PhD b, Veerle Van Dooren MSc i, Gursel Aktan MD m, Aron Goldhirsch MD n o, Tsai-Wang Chang MD p, Zsolt Horváth MD q, Maria Coccia-Portugal MD r, Julien Domont MD s, Ling-Min Tseng MD t, Georg Kunz MD u, Joo Hyuk Sohn MD v, Vladimir Semiglazov MD w, Guillermo Lerzo MD x, Marketa Palacova MD y, Volodymyr Probachai MD z, Lajos Pusztai DPhil aa, Michael Untch PhD ab, Richard D Gelber PhD ac ad, Martine Piccart-Gebhart PhD k, on behalf of the NeoALTTO Study Team
Summary
Background
The anti-HER2 monoclonal antibody trastuzumab and the tyrosine kinase inhibitor lapatinib have complementary mechanisms of action and synergistic antitumour activity in models of HER2-overexpressing breast cancer. We argue that the two anti-HER2 agents given together would be better than single-agent therapy.
Methods
In this parallel groups, randomised, open-label, phase 3 study undertaken between Jan 5, 2008, and May 27, 2010, women from 23 countries with HER2-positive primary breast cancer with tumours greater than 2 cm in diameter were randomly assigned to oral lapatinib (1500 mg), intravenous trastuzumab (loading dose 4 mg/m2, subsequent doses 2 mg/kg), or lapatinib (1000 mg) plus trastuzumab. Treatment allocation was by stratified, permuted blocks randomisation, with four stratification factors. Anti-HER2 therapy alone was given for the first 6 weeks; weekly paclitaxel (80 mg/m2) was then added to the regimen for a further 12 weeks, before definitive surgery was undertaken. After surgery, patients received adjuvant chemotherapy followed by the same targeted therapy as in the neoadjuvant phase to 52 weeks. The primary endpoint was the rate of pathological complete response (pCR), analysed by intention to treat. This trial is registered with ClinicalTrials.gov, NCT00553358.
Findings
154 patients received lapatinib, 149 trastuzumab, and 152 the combination. pCR rate was significantly higher in the group given lapatinib and trastuzumab (78 of 152 patients [51·3%; 95% CI 43·1—59·5]) than in the group given trastuzumab alone (44 of 149 patients [29·5%; 22·4—37·5]; difference 21·1%, 9·1—34·2, p=0·0001). We recorded no significant difference in pCR between the lapatinib (38 of 154 patients [24·7%, 18·1—32·3]) and the trastuzumab (difference −4·8%, −17·6 to 8·2, p=0·34) groups. No major cardiac dysfunctions occurred. Frequency of grade 3 diarrhoea was higher with lapatinib (36 patients [23·4%]) and lapatinib plus trastuzumab (32 [21·1%]) than with trastuzumab (three [2·0%]). Similarly, grade 3 liver-enzyme alterations were more frequent with lapatinib (27 [17·5%]) and lapatinib plus trastuzumab (15 [9·9%]) than with trastuzumab (11 [7·4%]).
Interpretation
Dual inhibition of HER2 might be a valid approach to treatment of HER2-positive breast cancer in the neoadjuvant setting.
Eribulin Improves Survival of Women with Metastatic Breast Cancer
Adapted from the NCI Cancer Bulletin.
Treatment with eribulin (Halaven™) improved overall survival in women with metastatic breast
cancer whose disease progressed despite multiple rounds of prior chemotherapy, according to the
results of a phase III clinical trial called EMBRACE. Based on these findings, the FDA approved
eribulin last November for women with metastatic disease who have already undergone at least two
previous chemotherapy regimens.
The study results were published online March 2, 2011, in The Lancet.
The improvement in overall survival makes the findings “clinically meaningful,” wrote the study’s
lead author, Javier Cortes, M.D., of the Vall d'Hebron Institute of Oncology in Barcelona, Spain,
and his colleagues. “To our knowledge, EMBRACE is the first major single-agent study of a
cytotoxic or biological agent to show significantly increased survival in patients with such heavily
pretreated metastatic breast cancer.”
Eribulin is a laboratory-made form of halichondrin B, a substance derived from a sea sponge.
Similar to some other chemotherapy drugs, it targets the protein tubulin in cells, although it binds to
tubulin in a different way, interfering with cancer cell division and growth.
In the trial—funded by Eisai Co., Ltd., which manufactures eribulin—762 patients were randomly
assigned to receive either eribulin or the treating physicians’ choice of therapy. Prior to enrolling,
trial participants had received, on average, four previous chemotherapy regimens. Because there is
no standard of care for women with progressive metastatic breast cancer, the treatments eribulin
was compared with “[reflect] real-life choices made by oncologists and their patients,” the
researchers wrote.
Women who received eribulin, on average, lived 2.5 months longer than those treated with their
physician’s choice (13.1 months versus 10.6 months). Progression-free survival was similar
between the groups. Overall, serious side effects were roughly equal in women in both trial arms,
although women treated with eribulin had more serious cases of neutropenia, leukopenia, and
peripheral neuropathy.
“EMBRACE provides much needed, high-level evidence for chemotherapy use in patients with
heavily pretreated breast cancer,” wrote Nancy Lin, M.D., and Harold Burstein, M.D., Ph.D., of
Dana-Farber Cancer Institute, in an accompanying editorial. But a number of important questions
remain about the use of eribulin in this group of patients, they noted, including whether there is a
subgroup that is more likely to respond to the drug.
“The clinical gains from EMBRACE are sufficiently narrow,” the study authors continued, “that a
better understanding of the relation between treatment, symptom control, and quality of life in study
participants remains crucial.”
This text may be reproduced or reused freely. Please credit the National Cancer Institute as the
source. Any graphics may be owned by the artist or publisher who created them, and permission
may be needed for their reuse.


















