Two dimensional echocardiography andthe …erior leaflet is shown only on the right ventricular...
7
Br Heart J 1983; 49: 495-500 Two dimensional echocardiography and the tricuspid valve Leaflet definition and prolapse ALLEN K BROWN, VALERIE ANDERSON From the Cardiac Departmet, Royal Lancaster Infirmary, Lancaster SUMMARY The tricuspid valve was studied in 143 subjects using two dimensional echocardiography. The groups studied were 40 normal subjects, 31 patients with mitral valve prolapse, 22 with clinically probable tricuspid valve prolapse, 20 with congestive cardiac failure, and 30 with miscel- laneous cardiac conditions but no features of right heart disease. Using multiple views it was possible to record all three leaflets in 74.80/o of cases and anterior and septal leaflets in 95%. Prolapse of the tricuspid valve was recognised in 13 patients: six (19 5%) of the group with mitral valve prolapse and seven (6%) of the remaining patients. Prolapse of all three leaflets was shown in one patient, anterior and septal prolapse in six patients, anterior and posterior in three patients, septal leaflet prolapse alone in two patients, and anterior alone in one patient. Two dimensional echocardiography allows definition of individual tricuspid leaflets and prolapse of any or all leaflets can be diagnosed. Tricuspid valve prolapse is commonly associated with prolapse of mitral valve leaflets but isolated cases are recognised. Although Tajik et al. in 19781 described how all three tricuspid leaflets may be shown by two dimensional echocardiography, most descriptions refer to the anterior and septal leaflets only.'-4 In this study we describe the ability of two dimensional echocardio- graphy to show three tricuspid leaflets and to show prolapse affecting individual leaflets. Subjects and methods The 143 subjects were selected from patients referred to the non-invasive laboratory for investigation. They were divided into five groups. Group 1 consisted of 40 subjects with minimal or no heart disease who served as normal controls. There were 14 male and 26 female subjects, with a mean age of 25-85 years, range 11 to 66 years. Group 2 comprised 31 patients with mitral valve prolapse (15 male, 16 female, mean age 51-7 years, range 14 to 81 years). Group three consisted of 20 patients with congestive cardiac failure including five with cor pulmonale (12 men, 8 women, mean age 66-8 years, range 52 to 85 years). Group 4 comprised 22 patients, nine with definite clinical features of tricuspid regurgitation and 13 with probable tricuspid regurgitation (nine men, 13 women, mean age 54-2 Accepted for publication 1 February 1983 years, range 17 to 79 years). Group 5 consisted of 30 patients (16 male, 14 female patients, mean age 44-8 years, range 8 to 85 years) with miscellaneous cardiac conditions, including chronic rheumatic heart dis- ease, ischaemic heart disease, lone artrial fibrillation, and cardiomyopathy. None of these patients had clin- ical features of significant right heart disease and tricuspid regurgitation was not suspected. Echocardiograms were recorded using a Smith- Kline Ekosector I mechanical sector scanner or a Hewlett Packard phased array ultrasound imaging system, model 77020A. Transducers giving 300 and 80" images were available on the Ekosector I, but the 30° transducer gave better definition of leaflet move- ment, and the images were recorded on a Sanyo videotape recorder. 2-5 MHz and 3-5 MHz transduc- ers were used on the phased array system and the images recorded on a Sony Betamax videorecorder. In both cases images were viewed in slow motion and frame by frame for analysis, and still frame photo- graphs were obtained with a Polaroid camera. Conventional techniques were used to record M-mode echocardiograms, phonocardiograms, and jugular venous and carotid pulses. Hard copy photo- graphic records were obtained on a Cambridge fibreoptic 12 channel physiological recorder. Anterior and posterior tricuspid leaflets were 495 on March 4, 2020 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. Downloaded from on March 4, 2020 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. Downloaded from on March 4, 2020 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. Downloaded from
Transcript of Two dimensional echocardiography andthe …erior leaflet is shown only on the right ventricular...

Br Heart J 1983; 49: 495-500
Two dimensional echocardiography and the tricuspidvalveLeaflet definition and prolapse
ALLEN K BROWN, VALERIE ANDERSON
From the Cardiac Departmet, Royal Lancaster Infirmary, Lancaster
SUMMARY The tricuspid valve was studied in 143 subjects using two dimensional echocardiography.The groups studied were 40 normal subjects, 31 patients with mitral valve prolapse, 22 withclinically probable tricuspid valve prolapse, 20 with congestive cardiac failure, and 30 with miscel-laneous cardiac conditions but no features of right heart disease. Using multiple views it was possibleto record all three leaflets in 74.80/o of cases and anterior and septal leaflets in 95%. Prolapse of thetricuspid valve was recognised in 13 patients: six (19 5%) of the group with mitral valve prolapse andseven (6%) of the remaining patients. Prolapse of all three leaflets was shown in one patient, anteriorand septal prolapse in six patients, anterior and posterior in three patients, septal leaflet prolapsealone in two patients, and anterior alone in one patient.Two dimensional echocardiography allows definition of individual tricuspid leaflets and prolapse
of any or all leaflets can be diagnosed. Tricuspid valve prolapse is commonly associated withprolapse of mitral valve leaflets but isolated cases are recognised.
Although Tajik et al. in 19781 described how all threetricuspid leaflets may be shown by two dimensionalechocardiography, most descriptions refer to theanterior and septal leaflets only.'-4 In this study wedescribe the ability of two dimensional echocardio-graphy to show three tricuspid leaflets and to showprolapse affecting individual leaflets.
Subjects and methods
The 143 subjects were selected from patients referredto the non-invasive laboratory for investigation. Theywere divided into five groups. Group 1 consisted of 40subjects with minimal or no heart disease who servedas normal controls. There were 14 male and 26 femalesubjects, with a mean age of 25-85 years, range 11 to66 years. Group 2 comprised 31 patients with mitralvalve prolapse (15 male, 16 female, mean age 51-7years, range 14 to 81 years). Group three consisted of20 patients with congestive cardiac failure includingfive with cor pulmonale (12 men, 8 women, mean age66-8 years, range 52 to 85 years). Group 4 comprised22 patients, nine with definite clinical features oftricuspid regurgitation and 13 with probable tricuspidregurgitation (nine men, 13 women, mean age 54-2
Accepted for publication 1 February 1983
years, range 17 to 79 years). Group 5 consisted of 30patients (16 male, 14 female patients, mean age 44-8years, range 8 to 85 years) with miscellaneous cardiacconditions, including chronic rheumatic heart dis-ease, ischaemic heart disease, lone artrial fibrillation,and cardiomyopathy. None of these patients had clin-ical features of significant right heart disease andtricuspid regurgitation was not suspected.
Echocardiograms were recorded using a Smith-Kline Ekosector I mechanical sector scanner or aHewlett Packard phased array ultrasound imagingsystem, model 77020A. Transducers giving 300 and80" images were available on the Ekosector I, but the30° transducer gave better definition of leaflet move-ment, and the images were recorded on a Sanyovideotape recorder. 2-5 MHz and 3-5 MHz transduc-ers were used on the phased array system and theimages recorded on a Sony Betamax videorecorder. Inboth cases images were viewed in slow motion andframe by frame for analysis, and still frame photo-graphs were obtained with a Polaroid camera.
Conventional techniques were used to recordM-mode echocardiograms, phonocardiograms, andjugular venous and carotid pulses. Hard copy photo-graphic records were obtained on a Cambridgefibreoptic 12 channel physiological recorder.
Anterior and posterior tricuspid leaflets were
495
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from
on M
arch 4, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.49.5.495 on 1 M
ay 1983. Dow
nloaded from
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from

viewed using a long axis view of the right ventricularinflow tract from the left parasternal area (Fig 1).Clockwise rotation of the transducer gave views ofboth inflow tracts which provided images of theanterior and septal leaflets; this was designated the"short axis" view for ease of description (Fig 2). Theanterior and septal leaflets were also viewed in theapical four chamber and subxiphoid views (Fig 3 and4). Standard criteria5S6 were used to diagnose prolapse _ _of the mitral valve, and tricuspid valve prolapse wasdiagnosed in a similar manner when two dimensionalrecordings showed that one or more tricuspid leafletsmoved superiorly in systole so that they extendedbeyond a line connecting the basal attachments of the'leaflets. Frame by frame analysis was used to definethe presence and degree of prolapse.
Results
DEFINITION OF INDIVIDUAL TRICUSPID LEAF-
LE'FS -In three patients, the tricuspid valve was not seen on _the echocardiogram. All three leaflets were recorded
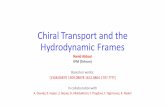
Fig. 2 In this short axis viewfrom the left parasternal border ina normal subject, the anterior and septal tricuspid valve leafletscan be seen. ATVL, STVL, anterior and septal tricuspid valveeaflets; IVS, interventricular septum; RA, RV, right atriumand ventricle; LV, left ventricle.
in 107/143 (74.8%) of subjects. Anterior and septalleaflets were seen in 136/143 (95%) cases. Details ofwhich leaflets were recorded are shown in Table 1.When only one leaflet was shown on the long axisparasternal view of the right ventricular inflow tract itwas usually the anterior; in the short axis view theseptal leaflet was recorded more often than theanterior; with the apical four chamber view it was theseptal leaflet and with the subxiphoid view it was theanterior leaflet usually. Subxiphoid views wereinferior to the precordial views in defining the leaflets.The anterior leaflet was best seen on the parasternalview of the right ventricular inflow tract and the septalleaflet was best seen on the parasternal view of bothinflow tracts or the apical four chamber view.
DEFINITION OF TRICUSPID VALVE PROLAPSEProlapse of the tricuspid valve was found in 13patients. There were six cases (19&5%) in group 2
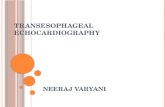
Fig. 1 Two dimensional echocardiogram showing the long axts (patients with mitral valve prolapse) and seven(6g ) ofview of the tricuspid valve in a normal heart. In this view the tie wititavalve Prolapse an see (6%) ofanterior and posterior leaflets are visible. ATVL, PTVL, the remaning patients. Prolapse of three leaflets wasanterior and posterior tricuspid valve leaflets; RA, RV, right recognised in one patient; of both anterior and septalamumini and vi'ntride: CH,. chordae. leaflets in six patients (Fig. 5); of both anterior and
Brown, Anderson496
C&1 &94,* S, v>- ,.,,- __,--
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from

Two dimensional echocardiography and tricuspid valve prolapse
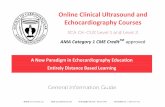
Fig. 3 The normal apicaljour chamber view, srelations of the anterior and septal ticnpid valvemiral valve. See Fig. I and 2for abbreviations. Fig. 4 The subxiphoid view of the riusPid valve in a normal
subject. As in the four chamber and short axis views, only the
anterior and septal leflets can be seen. See Fig. I and 2forabbreviations.
Table 1 Showns which leafets are recordedfrom different vews:figures show patents in whom no leaflets (0), one leqflet(A) or (P) or (S), and two leaflets (A +S) or (A +P) could be recorded
Group Long axis Short axis Four chamber Subxiphoid(no. ofpatents)
0 A P A+P O A S A+S O A S A+S 0 A S A+S
1 2 4 0 34 3 0 9 28 5 0 10 25 19 10 1 10Normal(40)2 3 2 0 26 7 0 3 21 4 0 3 24 17 2 0 12MVP(31)3 3 6 0 11 3 1 3 13 3 2 4 11 7 2 0 11CCF+Cor P(20)4 1 3 0 18 2 1 3 16 4 0 2 16 5 2 0 15Definite TRProbable TR(22)5 7 2 0 21 5 2 8 15 6 0 2 22 10 7 0 13Miscellaneous(30)Totals 16 17 0 110 20 4 26 95 22 2 21 98 58 23 1 61
A, anterior; P, posterior; S, septal; MVP, mitral valve prolapse; CCF, congestive cardiac failure; Cor P, cor pulmonale; TR, tricuspidregurgitation.
497
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from

Brown, Anderson
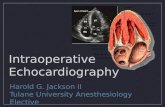
Fig. 5 The subxiphoid view shows prolapse of both anteriorand septal leaflets beyond the ticuspid annulus. See Fig. I and 2for abbreviations.
Fig. 7 Thefour chamber apical view in which the septal leafletprolapses beyond the level of the tricuspid annulus into the rightatrium. The anterior leaflet becomes horizontal. See Fig. I and 2for abbreviations.
Fig. 6 Long axis view in a patient with prolapse ofthe anteriorand posterior tricuspid valve leaflets. See Fig. I and 2 forabbreviations.
posterior leaflets in three patients (Fig. 6); and twopatients had prolapse of the septal leaflet alone (Fig.7). One of these patients was shown to have failure ofsystolic apposition of the leaflets and was presumed tohave a flail leaflet. The remaining patient showedanterior leaflet prolapse alone. Details of the cases andthe views which showed the prolapsing leaflets areshown in Table 2.
Discussion
The normal tricuspid valve comprises anterior, post-erior, and septal leaflets.78 The septal cusp is smallwith its base inserted obliquely across the membran-ous interventricular septum. The anterior cusp is thelargest and is semicircular or quadrangular. The post-erior cusp is usually semicircular, scalloped, andintermediate in length between the other two leaflets.
It has been shown that it is possible to record the
498
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from

Two dimensional echocardiography and tricuspid valve prolapse
Table 2 Details ofpatients with tricuspid valve prolapse
Group Leaflets visible Prolapse Leaflets(no. ofpatients) LA SA 4Ch Subx seen (view) prolapsing
I - _ _Normal2 AP AS AS AS 4Ch+ Subx A+SMVP (6) AP AS AS AS SA+4Ch A+S
AP AS AS - 4Ch A+SAP AS AS - LA+SA+4Ch A+SAP AS AS - LA A+PAP AS AS A LA A+P
3CCF (O)+Cor P (1) A S S AS Subx A+S4 AP AS AS AS SA A+STR definite (2) AP AS - A SA+LA A+PTR probable (1) A S AS AS 4Ch+Subx A5 - AS - AS SA SMiscellaneous (3) - S AS AS Subx S
AP AS AS A LA+SA A+P+S
LA, long axis; SA, short axis; 4Ch, apical four chamber; Subx, Subxiphoid; A, anterior; P, posterior; S, septal; MVP, mitral valve prolapse;CCF, congestive cardiac failure; Cor P, cor pulmonale; TR, tricuspid regurgitation.
three leaflets on two dimensional echocardiography. l 9Anterior and septal leaflets can be seen on parasternalviews of both inflow tracts and on four chamber viewsfrom the apex or subxiphoid positions. In our study,the anterior leaflet is less frequently demonstratedthan the septal on the precordial views, whereas thesubxiphoid approach usually shows the anteriorleaflet, and the septal is less commonly seen. Longaxis parasternal views of the right ventricular inflowtract show posterior and anterior leaflets. When thereis difficulty showing both these leaflets, the posterioris the one not seen. Using the combination of views,all three tricuspid leaflets are shown in 74-8% of ourpatients, and the anterior and septal leaflets are almostinvariably recorded (95%).
Features of tricuspid valve prolapse on two dimen-sional echocardiography have been described but onlytwo leaflets are discussed. Though Mardelliet al.3 andOgawa et al.4 describe the use of "right ventricularinflow" views, their illustrations show that they areusing the parasternal view of both right and left inflowtracts which allows definition of anterior and septalleaflets but not the posterior leaflet. Werner andassociates2 describe septal and "mural" leaflets in twocases without further qualification. From our studiesit is apparent that prolapse of any or all the tricuspidleaflets may be studied if a combination of views isused. The tricuspid ring may be represented by a linejoining the basal attachments of leaflets in each view.Prolapse is diagnosed if one or more leaflets extendbeyond this line in systole. Determination of prolapseof tricuspid leaflets is more difficult than the demonst-ration of mitral valve prolapse. The exact insertion ofthe basal attachment of the leaflets may be difficult tosee and, therefore, the tricuspid ring is not easy todefine. In addition, the leaflets of the tricuspid valveare less clearly seen than those of the mitral valve
because the images are less well defined. The obliqueinsertion of the septal leaflet and its attachment to theseptal wall by short chordae has led to the suggestionthat it is the one most prone to incompetence.7 Wehave shown that prolapse can affect any or all leafletsif appropriate views are studied, but since the post-erior leaflet is shown only on the right ventricularinflow images, this view must be sought with particu-lar care.
Prevalence studies using pathological or angio-graphic evidence suggest that 21 to 52/o of patientswith mitral valve prolapse have associated tricuspidvalve prolapse.'0 Using M-mode echocardiography,tricuspid valve prolapse was found in 3 to 21% ofpatients with mitral valve prolapse.2 Werner et al.2could find no cases of isolated tricuspid valve prolapsein 500 routine echocardiograms though after the studythey reported three patients with prolapsed tricuspidvalve, one after a right ventricular wound, one withvegetations on the valve, and one in association with alarge pericardial effusion. Single cases of tricuspidvalve prolapse diagnosed by M-mode echocardiogra-phy have been described'213 and two similar caseswere added by Karayannis et al.'4 A further studyreported 12 patients with tricuspid valve prolapse,eight with associated mitral valve prolapse. l 5 Becauseof the difficulty of recording other than the anteriorleaflet with the M-mode technique, two studies usedtwo dimensional echocardiography. Mardelli et al.3reported 64 cases of mitral prolapse, 31 (48%) ofwhich showed associated tricuspid valve prolapse, andOgawa et al .4 found tricuspid valve prolapse in 20/50(40%) patients with mitral valve prolapse. We found alower prevalence of tricuspid valve prolapse associ-ated with mitral prolapse (19.5%) even though threeleaflets have been assessed in most patients. That thisis a true difference from the other series is suggested
499
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from

500
by the number of isolated cases of tricuspid prolapsewhich we have recognised.We conclude that two dimensional echocardiogra-
phy is an appropriate technique for the demonstrationof tricuspid valve prolapse. Using multiple views it ispossible to record anterior and septal leaflets in mostsubjects. The posterior leaflet is seen only on the longaxis parasternal view and every effort must be made toobtain this view. Prolapse of the tricuspid valve iscommonly associated with mitral valve prolapse, butisolated cases occur.
References
1 Tajik AJ, Seward JB, Hagler DJ, Mair DD, Lie JT. Twodimensional real time ultrasonic imaging of the heart andgreat vessels. Mayo Clin Proc 1978; 53: 271-303.
2 Werner JA, Schiller NB, Prasquier R. Occurrence andsignificance of echocardiographically demonstratedtricuspid valve prolapse. Am Heart J 1977; 96: 180-6.
3 Mardelli TJ, Morganroth J, Chen CC, Naito M, VergelJ. Tricuspid valve prolapse diagnosed by cross-sectionalechocardiography. Chest 1981; 79: 201-5.
4 Ogawa S, Hayashi J, Sasaki H, et al. Evaluation of com-bined valvular prolapse syndrome by two-dimensionalechocardiography. Circulation 1982; 65: 174-80.
5 Gilbert BW, Schatz RA, VonRamm OT, Behar VS, Kis-slo JA. Mitral valve prolapse. Two-dimensional echocar-diographic and angiographic correlation. Circulation1976; 54: 716-23.
6 Brown AK, Anderson V. M-mode and cross-sectional(2D) echocardiograms in the diagnosis of mitral valveprolapse. Eur Heart J 1981; 2: 147-54.
Brown, Anderson
7 Silver MD, Lam JHC, Ranganathan N, Wigle ED.Morphology of the human tricuspid valve. Circulation1971; 43: 333-48.
8 Davies MJ. Tricuspid and pulmonary valve pathology.In: Pathology of cardiac valves. (Postgraduate pathologyseries.) London: Butterworths, 1980: 124-38.
9 Donaldson RM, Ballester M, Rickards AF. Rupture of apapillary muscle of the tricuspid valve. Br HeartJ 1982;48: 291-3.
10 Morganroth J, Jones RH, Chen CC, Naito M. Two-dimensional echocardiography in mitral, aortic andtricuspid valve prolapse. Am J Cardiol 1980; 46: 1164-77.
11 Rippe JM, Angoff G, Sloss LJ, Wynne J, Alpert JS.Multiple floppy valves: an echocardiographic syndrome.Am J Med 1979; 66: 817-24.
12 Sasse L, Froelich CR. Echocardiographic tricuspid pro-lapse and nonejection systolic click. Chest 1978; 73:869-70.
13 Horgan JH, Beachley MC, Robinson FD. Tricuspidvalve prolapse diagnosed by echocardiogram. Chest 1975;68: 822-4.
14 Karayannis E, Stefadouros MA, Abdulla AM, BlackwellJC. Use of echocardiography in the diagnosis of pro-lapsed tricuspid valve. J Med Assoc Ga 1978; 67: 205-8.
15 Chandraratna PAN, Lopez JM, Fernandez JJ, CohenLS. Echocardiographic detection of tricuspid valve pro-lapse. Circulation 1975; 51: 823-6.
Requests for reprints to Dr Allen K Brown, CardiacDepartment, Royal Lancaster Infirmary, LancasterLAI 4RP.
on March 4, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.49.5.495 on 1 May 1983. D
ownloaded from

Tocainide prophylaxis of ventricularfibrillation
for this and we assume that it has occurred by chance.There was a high incidence of death (two of 28) and
of cardiac events (nine of 28) in group 3 patients (pro-tocol violators and those with inadequate data). Thisphenomenon occurred both in active and placebotreated patients and, while our inclusion criteria wereprimarily designed to prevent inappropriate adminis-tration of tocainide, the figures indicate that patientswho should be excluded from such investigations arethemselves a high risk group. Similar findings havebeen noted in other studies.5 6
This study is one of very few which has arrived at afirm conclusion regarding the efficacy of a drug forventricular fibrillation prophylaxis. Further investiga-tions of drug prophylaxis of ventricular fibrillationare required and should employ a study design whichpermits a positive statistical statement ofdrug efficacy.
References
1 Lie KI, Wellens HJJ, Van Capelle FJ, Durrer D.Lidocaine in the prevention of primary ventricular fibril-lation. N Engl J Med 1974; 291: 1324-6.
2 Lie KI, Liem KL, Louridtz WL, Janse MJ, WillebrandsAF, Durrer D. Efficacy of lignocaine in preventing ven-tricular fibrillation within 1 hour after a 300 mgintramuscular injection. A double-blind, randomizedstudy of 300 hospitalized patients with acute myocardialinfarction. Am J Cardiol 1978; 42: 486-8.
3 Koch-Weser J, Klein SW, Foo-Canto LL, Kastor JA,DeSanctis RW. Antiarrhythmic prophylaxis with pro-cainamide in acute myocardial infarction. N EnglJ7 Med1969; 281: 1253-60.
4 Jones DT, Kostuk WJ, Gunton RW. Prophylacticquinidine for the prevention of arrhythmias after acutemyocardial infarction. Am J Cardiol 1974; 33: 655-60.
5 Campbell RWF, Achuff SC, Pottage A, Murray A,Prescott LF, Julian DG. Mexiletine in the prophylaxis of
563
ventricular arrhythmias during acute myocardial infarc-tion. J Cardiovasc Pharmacol 1979; 1: 43-52.
6 Campbell RWF, Bryson LG, Bailey BJ, Murray A,Julian DG. Prophylactic administration of tocainide inacute myocardial infarction. In: Pottage A, Ryden L,eds. Workshop on tocainide. Goteborg: AB Hassle, 1981:201-4.
7 Ryden L, Arnman K, Conradson T-B, Hofvendahl S,Mortensen 0, Smedgird P. Prophylaxis of ventriculartachyarrhythmias with intravenous and oral tocainide inpatients with and recovering from acute myocardialinfarction. Am HeartJ 1980; 100: 1006-12.
8 Prescott LF. Pharmacokinetic abnormalities in myocar-dial infarction. In: Sand0e E, Julian DG, Bell JW, eds.Management of ventricular tachycardia-rok of mexikeine.Amsterdam: Excerpta Medica, 1978: 465-71.
9 Anderson JL, Mason JW, Winkle RA, et al. Clinicalelectrophysiologic effects of tocainide. Circulation 1978;57: 685-91.
10 Rehnquist N. Comparison of tocainide with lidocaine inAMI. In: Pottage A, Ryden L, eds. Workshop ontocainide. Goteborg: AB H-assle, 1981: 187-9.
11 Graffner C, Conradson T-B, Hofvendahl S, Ryden L.Tocainide kinetics after intravenous and oral administra-tion in healthy subjects and in patients with acutemyocardial infarction. Clin Phannacol Ther 1980; 27:64-71.
12 Winkle RA, Meffin PJ, Fitzgerald JW, Harrison DC.Clinical efficacy and pharmacokinetics of a new orallyeffective antiarrhythmic agent, tocainide. Circulation1976; 54: 884-9.
13 Moore EN, Spear JF, Horowitz LN, Feldman HS, Mol-ler RA. Electrophysiologic properties of a new antiar-rhythmic drug-tocainide. Am J Cardiol 1978; 41: 703-9.
14 Young MD, Hadidian Z, Hom HR, Johnson JL, Vas-sallo HG. Treatment of arrhythmias with oral tocainide.Am HeartJf 1980; 100: 1041-5.
Requests for reprints to Dr RW F Campbell, Univer-sity Department of Cardiology, Freeman Hospital,Newcastle upon Tyne NE7 7DN.
Erratum
The authors regret the following error in their paperin the May issue on "Two dimensional echocardiog-raphy and the tricuspid valve. Leaflet definition andprolapse". In the Summary, page 495, line 3, "tricus-pid valve prolapse" should read "tricuspid valve re-gurgitation".