

Tubulointerstitial kidney diseases: Pathophysiology ... NORTIER compressed.pdf ·...
56
Tubulointerstitial kidney diseases: Pathophysiology, diagnosis and clinical management Joëlle Nortier, MD, PhD Nephrology Dept & Lab. Experimental Nephrology Faculty of Medicine, Université Libre de Bruxelles Belgian Core Curriculum Course Nephrology June 16, 2018
Transcript of Tubulointerstitial kidney diseases: Pathophysiology ... NORTIER compressed.pdf ·...

Tubulointerstitial kidney diseases:
Pathophysiology, diagnosis and
clinical management
Joëlle Nortier, MD, PhD
Nephrology Dept & Lab. Experimental Nephrology
Faculty of Medicine, Université Libre de Bruxelles
Belgian Core Curriculum Course Nephrology
June 16, 2018

CONTENT
1) Definitions / characteristics
2) Acute interstitial nephritis: pathophysiology, diagnosis, clinical cases & management
3) Chronic interstitial nephritis: pathophysiology, diagnosis, clinical cases & management

CONTENT
1) Definitions / characteristics
2) Acute interstitial nephritis: pathophysiology, diagnosis, clinical cases & management
3) Chronic interstitial nephritis: pathophysiology, diagnosis, clinical cases & management

15 juin 2018 4
1) DEFINITION / TERMINOLOGY
Group of diseases primarily manifested by
inflammation and/or injury of renal tubules and
interstitium
Synonyms: (tubulo)interstitial nephritis
Abbreviations
Acute interstitial nephritis (AIN)
Chronic interstitial nephritis (CIN)
Acute tubular necrosis (ATN)
Acute tubular injury (ATI)
4

15 juin 2018 5
AIN >< CIN: CHARACTERISTICS
Acute IN
Acute, often reversible disease
Inflammatory infiltrates within
the interstitium
Uncommon cause of AKI (<
5%)
Up to 25% of renal biopsies for
drug-induced AKI
Bilateral flank pain
Increased size and
echogenicity of the kidneys
Mild proteinuria (< 1g/day)
Chronic IN
Frequent lesions reflecting the
progressive degradation of
renal function
Primary forms of CIN reaching
ESRD are quite rare
15% to 20% of CKD
Insidious development of renal
insufficiency
Anemia, hypertension…
Signs of proximal tubular
dysfunction…
Mild proteinuria (< 1g/day)
5

15 juin 2018 6
AIN >< CIN: MAIN ETIOLOGIES & HISTOLOGICAL FINDINGS
Acute IN
1. Drugs
2. Infections
3. Autoimmune diseases
Nonspecific lesions
variable size of enlarged
interstitial compartment (edema +
inflammatory infiltrate)
! No vascular or glomerular
lesions
! No immune deposit in most
cases…
Chronic IN
1. Toxins
2. Infections
3. Systemic diseases
6

15 juin 2018 7
Typical histological findings in case of
AIN : interstitial inflammatory infiltrate
with edema and tubular lesions (HE
staining)
7
Normal renal cortex (PAS staining)

15 juin 2018 8
AIN >< CIN: MAIN ETIOLOGIES & HISTOLOGICAL FINDINGS
Acute IN
1. Drugs
2. Infections
3. Autoimmune diseases
Nonspecific lesions
variable size of enlarged
interstitial compartment (edema +
inflammatory infiltrate)
! No vascular or glomerular
lesions
! No immune deposit in most
cases…
Chronic IN
1. Toxins
2. Infections
3. Systemic diseases
Interstitial fibrosis
Tubular cell atrophy
Mononuclear cell infiltration
(variable intensity)
Noncaseating granulomatous
patterns in specific situations
8

15 juin 2018 9
Typical lesions of hypertensive
nephroangiosclerosis
Remodelling of arterial walls (thickening
of the media and intimal fibrosis),
tubular atrophy and interstitial fibrosis
9
Normal renal cortex (PAS staining)

CONTENT
1) Definitions / characteristics
2) Acute interstitial nephritis: pathophysiology, diagnosis, clinical cases & management
3) Chronic interstitial nephritis: pathophysiology, diagnosis, clinical cases & management

Pathogenesis of AIN (experimental models)

1. Drug-induced AIN Antimicrobial agents Antiviral agents Nonsteroidal anti-inflammatory drugs
(NSAIDs) including salicylates Antalgics Antiulcer agents (cimetidine and proton
pump inhibitors) Anticonvulsants Diuretics
hypersensitivity reaction, not dose dependent
Clinical presentation (within days after drug ingestion): Low-grade fever Maculopapular rash Mild arthralgias Eosinophilia

1. Drug-induced AIN Antimicrobial agents Antiviral agents Nonsteroidal anti-inflammatory drugs
(NSAIDs) including salicylates Antalgics Antiulcer agents (cimetidine and proton
pump inhibitors) Anticonvulsants Diuretics
hypersensitivity reaction, not dose dependent
Clinical presentation (within days after drug ingestion): Low-grade fever Maculopapular rash Mild arthralgias Eosinophilia

15 juin 2018 14
SPECIFIC DRUG ASSOCIATIONS
Rifampicin: usually after readministration of the
drug; fever and gastrointestinal syptoms and
myalgias; hemolysis and thrombocytopenia,
hepatitis
Allopurinol: more frequent in CKD patients; rash +
liver dysfunction !
NSAIDs (including COX-2 selective inhibitors):
nephrotic syndrome (75% cases; 50 % of cases
with fenoprofen): after months of regular intake
(even more than 1 year); edema ++ but no other
extrarenal symptoms
14

15 juin 2018 15
On light microscopy, search
for the characteristic features
- Interstitial infiltration with
mononuclear cells
(eosinophils)
- Usually associated with
interstitial edema and
tubular lesions
- Some drugs can induce
the formation of interstitial
granulomas, reflecting a
delayed-type
hypersensitivity reaction
15
PATHOLOGY OF DRUG-INDUCED ACUTE INTERSTITIAL NEPHRITIS
(Courtesy of Pr. I. Brochériou)

15 juin 2018 16 16
PATHOLOGY OF DRUG-INDUCED ACUTE INTERSTITIAL NEPHRITIS
(Courtesy of Pr. I. Brochériou)

15 juin 2018 17 17
INFLAMMATORY INFILTRATES IN ACUTE INTERSTITIAL NEPHRITIS
- Often patchy , predominating in the deep cortex and in
the outer medulla
- Can be diffuse in most severe diseases
- Composed mostly of T cells and monocyte-macrophages
+ eosinophils, plasma cells may be present… a few
neutrophilic granulocytes
- CD4+ and CD8+ T cells in variable proportions
- Signs of tubulitis: T cells infiltrate across the tubular
basement membrane and between tubular cells (mainly
in distal tubules)

15 juin 2018 18
PATHOLOGY OF DRUG-INDUCED ACUTE INTERSTITIAL NEPHRITIS
(Courtesy of Pr. I. Brochériou)

15 juin 2018 19
Interstitial granulomas
- Sparse and non-necrotic
- With few giant cells
- Associated with
nongranulomatous
interstitial infiltrates
!!!! Granulomas are also
found in AIN related to
infections, sarcoidosis,
Sjögren’s syndrome and
Wegener’s granulomatosis
PATHOLOGY OF DRUG-INDUCED ACUTE INTERSTITIAL NEPHRITIS
(Courtesy of Pr. I. Brochériou)

15 juin 2018 20
Immunofluorescence may be
positive !
- Staining of the tubular basement
membrane for IgG or
complement
- Granular or linear staining
pattern…. Indicating the
presence of antibodies directed
against membrane antigens or
against drug metabolites bound
to the membrane
- Mostly seen in patients taking
methicillin, NSAIDS, phenytoin,
allopurinol
20
PATHOLOGY OF DRUG-INDUCED ACUTE INTERSTITIAL NEPHRITIS
Linear deposits of IgG in a case of methicillin-
induced AIN (Courtesy of Dr. B. Mougenot)

!!! ACUTE INTERSTITIAL NEPHRITIS >< ACUTE TUBULAR NECROSIS
Interstitial inflammatory
infiltrate
Tubulitis
Granulomas
Tubular granular casts
Loss of the brush border
Necrosis of the tubular cells
Polymorphonuclear
neutrophils in the vasa recta
Hyaline, granular casts
- The most frequent form of
AKI (85%)
- Ischemic or toxic origin
21

CISPLATIN NEPHROTOXICITY
Acute and focal tubular necrosis
Signs of tubular regeneration

Diagnosis of drug-induced AIN
RENAL BIOPSY !
and also…
- Eosinophiliuria but low sensitivity and low positive predictive value
- Gallium-67 renal scanning but not specific (positive in case of cancer, pyelonephritis…)
In Comprehensive Clinical Nephrology, 3rd ed.

15 juin 2018 24
IDENTIFICATION OF THE CAUSATIVE AGENT
Not so easy in patients with polymedication !
2 tests but of limited diagnostic value:
- antidrug circulating antibodies (rifampicin)
- lymphocytic stimulation test: proliferative index is
associated with a sensitization of T lymphocytes against
the suspected drug
24
15 juin 2018 25
IDENTIFICATION OF THE CAUSATIVE AGENT / NATURAL HISTORY
Not so easy in patients with polymedication !
2 tests but of limited diagnostic value:
- antidrug circulating antibodies (rifampicin)
- lymphocytic stimulation test
NATURAL HISTORY
Disappearance of extrarenal Ʃ within 2 weeks
Recovery of renal function is often delayed (average
recovery time 1.5 months)
Prognostic factors
Duration of AKI
Severity of interstitial fibrosis
25

15 juin 2018 26
2. AIN SECONDARY TO INFECTIONS: MAIN CAUSES
Bacteria
Staphylococcus spp.
Streptococcus spp.
Tuberculosis spp.
Legionella spp.
Leptospirosis spp.
Chlamydia spp.
Mycoplasma spp.
26
Viruses Cytomegalovirus Epstein-Barr virus Hantaan Hepatitis A and B Herpes simplex virus HIV Rickettsia
Parasites Toxoplasma Leischmania donovani

15 juin 2018 27
= infection of the renal parenchyma
In 95% of cases: secondary to
ascending infection of the urinary
tract
Gram neg (E Coli), strepto, staph…
27
ACUTE PYELONEPHRITIS
Predominance of polymorphonuclear
neutrophils (PMN) in the interstitial
inflammatory infiltrate
(Courtesy of Pr. I. Brochériou)

15 juin 2018 28
« Hemorrhagic fever with renal
syndrome », « epidemic
hemorrhagic fever »
- Extrarenal Ʃ: fever, headache,
lightheadedness, abdominal pain,
nausea, vomiting
- Thrombocytopenia
- Acute renal failure; proteinuria in
the nephrotic range, hematuria
- IF: granular immune deposits
balong the TBM or within glomeruli
- Δ: serologic tests
- Complete recovery is the rule but
may be complicated by
hemorrhagic episodes or shock
28
HANTAVIRUS INFECTIONS: A WORLDWIDE PROBLEM
Vascular congestion and foci of medullary hemorrhage are suggestive of the diagnosis

15 juin 2018 29
3. AIN ASSOCIATED WITH SYSTEMIC DISEASES
Sarcoidosis
Gougerot Sjögren (rare)
Systemic lupus erythematosus (rare with minimal
glomerular abnormalities; granular pattern of immune deposits along
the TBM)
IgG4 related diseases
ΔΔ AIN associated with malignancies
Idiopathic AIN (TINU syndrome):
anterior uveitis, in pubertal girls/boys…ocular pain and
visual impairment, pseudoviral Ʃ; good response to
steroid therapy
29

15 juin 2018 30
1. Hypercalcemia and hypercalciuria
renal dysfunction
2. AKI with mild proteinuria
- Extrarenal Ʃ in 90% cases: lymph
nodes, lung, eye, liver
- Hilar lymphadenopathy or pulmonary
interstitial fibrosis in 1 /2 cases at the
time of Δ
- High-dose corticosteroids are
mandatory (1 mg/kg prednisone
daily), slow tapering… min 9-12
months
30
SARCOIDOSIS AND RENAL INVOLVEMENT
Granulomatous AIN in a patient with
sarcoidosis (Courtesy of Dr. B. Mougenot)

IGG4 RELATED DISEASES
31
IgG4-related tubulointerstitial nephritis and/or glomerulonephritis

32
AI pancreatitis
AI interstitial nephritis
Corticosteroids Corticosteroids + azathioprine

A CASE OF IGG4 RELATED ACUTE INTERSTITIAL NEPHRITIS…
33
IgG4 immunostaining (medulla)
Severe interstitial inflammation
Clin Kidney J (2012) 5: 225

Management of AIN
• Dependent upon the underlying disease process
• Drug-induced AIN: identify and stop offending drug early steroid treatment may improve the recovery of renal function !! If worsening renal function or requiring RRT: prednisolone 1 mg/kg/day orally, taper over a period of 1 month according to the response (bone and GI protection + monitor glucose)
!! NSAID-induced AIN is less responsive to corticosteroid therapy MMF has been used in patients with steroid-resistant AIN
Blue bars: patients treated with corticosteroids Yellow bars: patients free of corticosteroids

CONTENT
1) Definitions / characteristics
2) Acute interstitial nephritis: pathophysiology, diagnosis, clinical cases & management
3) Chronic interstitial nephritis: pathophysiology, diagnosis, clinical cases & management

MAJOR ETIOLOGIES OF CHRONIC INTERSTITIAL NEPHRITIS
Kidneys are
macroscopically normal
Drugs and toxins
Metabolic
Heavy metals (Pb, Cd, As,
Hg)
Radiation
Atherosclerosis
Hematologic disturbances
(multiple myeloma)
Progressive glomerular
disease of all etiologies
Kidneys are
macroscopically abnormal
Analgesic nephropathy
Chronic obstruction
Hereditary
Infection
36

CHRONIC PYELONEPHRITIS
Almost exclusively in case of
obstruction of urinary tract or
reflux nephropathy
37
(Courtesy of Pr. I. Brochériou)

TWO PARTICULAR CASES OF CHRONIC PYELONEPHRITIS…
Women 50-60 yrs
Unilateral flank pain,
fever, anorexia, weight
loss, nausea
Biol: inflammatory
syndrome
Pyuria; Gram neg (E.
Coli, Proteus sp.,
Pseudomonas
aeruginosa)
38

39
Histiocytes and large
macrophages
Xanthogranulomatous
pyelonephritis

A 2ND CASE…
Man 60 yrs, kidney recipient (2nd)
SP/acute pyelonephritis (E. Coli)
and prostatitis (Enterococcus
faecalis)
Fever and diarrhea
Renal graft degradation; urinary
infection (E. Coli)
Fluoroquinolone therapy but no
improvement of renal function
kidney biopsy
40

41
Diagnosis ??

RENAL MALAKOPLAKIA
First described in 1902 by Michaelis and Gutmann
Genito-urinary tract (bladder +++)
Bilateral renal localization (35-50 %)
3 F / 1 H (peak 50-60 yrs)
Microscopy: interstitial infiltration by macrophages
containing concentric cytoplasm inclusions (5-10 µ) =
Michelis Gutmann bodies; bacterial residues + for Ca and
Fe
Pathogenesis: BGN infections (E. Coli) + primary defect of
macrophages (altered degranulation process)
42

43

CHRONIC URATE NEPHROPATHY
Hyperuricemia
Hypertension
Gout for many years
44 The crystalline masses are refractile under
polarized light

Aristolochic acid I + II (R=OCH3 / H)
«Stephania Tetrandra»
Han Fang-Ji
Vanherweghem et al. Lancet (1993); Vanhaelen et al. Lancet (1994)
Guang Fang-Ji
Aristolochia fangchi

Aristolochic acid nephropathy
Depierreux et al. Am J Kidney Dis 1994
Cosyns et al. Kidney Int 1994

Autoradiogram of specific AA-related
DNA adducts in renal tissue
Schmeiser HH, Arlt VM. Cancer Res (1996)
Arlt VM. Mutagenesis (2002)
AA biotransformation
(cytochrome P450)

AA-associated urothelial malignancies
Cosyns et al. Am J Kidney Dis (1999)
Nortier et al. N Engl J Med (2000)
Right ureteral tumor

15 juin 2018 49
Select cystoscopy screening suggests a stage migration toward
detection of non-muscle-invasive bladder cancer (BC)
Kidney recipients, n 48
Patients lost to follow-up 2
Median follow-up, months 90.5 ± 36
Bladder cancer, no. 25 (52 %)
Noninvasive BC at first diagnosis, no. 22 (46 %)
Muscle-invasive BC at first diagnosis in 0 (0 %)
patients who accepted screening, no.
Patient-refused follow-up / Deaths, no. 3 (6%)
Zlotta et al. Eur Urol 2011:59:1026-31 49

What about outside Belgium ?
Debelle et al. Kidney Int. (2008) 74:158
?
?
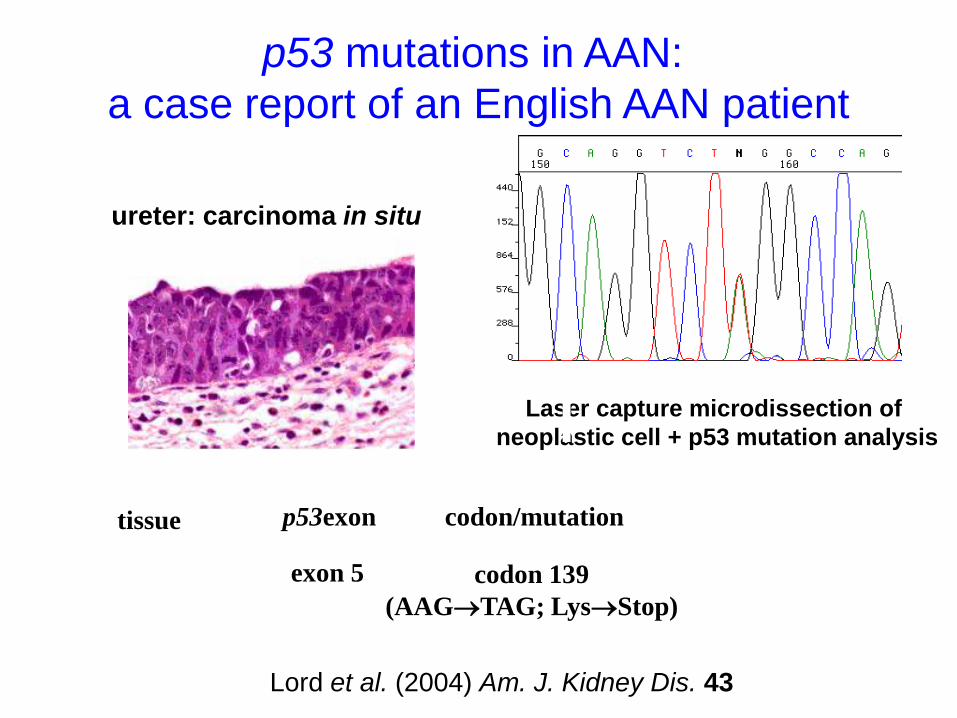
p53 mutations in AAN:
a case report of an English AAN patient
ureter: carcinoma in situ
Laser capture microdissection of
neoplastic cell + p53 mutation analysis
mutation type tissue
urothelial tumour
codon/mutation
codon 139
(AAGTAG; LysStop)
p53exon
exon 5 A T transversion
Lord et al. (2004) Am. J. Kidney Dis. 43
Courtesy of Dr
B. Jelakovic

Aristolochia clematitis

Proposed diagnostic criteria of AAN
(European consensus panel)
Major criteria (2 out of 3 should be needed)
- Confirmed ingestion of AA by phytochemical analyses
- Histopathological demonstration of interstitial fibrosis
- Detection of specific AA-DNA adducts in renal tissue
Minor criteria (2 in association with 1 major)
- History of exposure to AA
- Presence of urothelial carcinoma
Gökmen MR. et al. Ann. Intern. Med. (2013)

REFERENCES
Oxford Desk Reference Nephrology. Barratt J, Harris K &
Topham P (ed) Oxford University Press 2009.
Comprehensive Clinical Nephrology, 3rd ed. Feehally J, Floege J
& Johnson RJ (ed) Mosby Elsevier 2007.
Fundamentals of Renal Pathology (Stand-Alone CDRom). Fogo
AB, Bruijn JA, Cohen AH, Colvin RB, Jennette JC (ed) Springer
2008.
Atlas de Pathologie Rénale. Noël LH (ed) Médecine-Sciences
Flammarion 2008.
Clinical Nephrotoxins, 2nd ed. De Broe ME, Porter GA, Bennett
WM, Verpooten GA (ed) Kluwer Academic Publishers 2003.
15 juin 2018 56


















