Tuberculosiscenterfortuberculosis.mayo.edu/uploads/2/3/8/6/23860150/tsukayama... · Kenya 271...
53
Tuberculosis Assessment and Management Dean Tsukayama
Transcript of Tuberculosiscenterfortuberculosis.mayo.edu/uploads/2/3/8/6/23860150/tsukayama... · Kenya 271...
Tuberculosis Assessment and Management
Dean Tsukayama

I have no disclosures

Objectives
• Know the tools of assessment for tuberculosis infection and disease
• Know the risk factors for exposure to tuberculosis and for progression to disease
• Learn the basic principles of treatment of tuberculosis infection and disease

Case
• Started on treatment for pulmonary tuberculosis in Laos 3.5 months ago
• Diagnosis based on abnormal CXR and sputum growing Mycobacterium
• Sputum smear was negative, TST not done
• On daily isoniazid 300 mg, rifampin 450 mg, ethambutol 400 mg
• No pyrazinamide because she was breast feeding when treatment started
• No antibiotic susceptibility studies done
• No medications since arriving in MN 3 weeks ago
• Patient has no TB symptoms
23 year old Laotian woman!Class B evaluation

Case
• TST 21 mm
• CXR: fibronodular infiltrates in upper lobes bilaterally, no change from 10/15/10

Tuberculosis
Susceptible
Active disease Infected
Latent infection
Cure
Clinical Stages
Treatment!Transmission
Death

Questions to answer in evaluation of tuberculosis
1. TB or not TB?
2. TB infection or disease?
3. Is more information or further testing needed?
4. What treatment is needed?
5. Risk of transmission to others?

Gathering Information• History
• Risk for infection
• Family history of TB
• Liver and kidney function
• Medications
• Symptom Review
• Fever, fatigue, night sweats, weight loss
• Cough, chest pain, hemoptysis
• Other sites
• Physical Exam
• Eyes
• Lymph nodes
• Chest
• Liver
• Neurological

Risk of exposure to tuberculosis
MMWR 59 (RR-5), 2010

Risk of exposure to tuberculosis
World incidence 122
US 3
Disease incidence per 100,000 population
TUBERCULOSIS in the US among the foreign-born!Proportion of new cases- 65%!Increased risk of tuberculosis- 13 times

Poverty and TB
Eur Resp J 32:1415, 2008

Risk of exposure to tuberculosisDisease incidence per 100,000 population
Cambodia incidence
411Myanmar 377
Philippines 265Pakistan 231
Micronesia 194Bhutan 180India 176
Vietnam 147China 73Nepal 163
Muldova 160Bosnia 49Iraq 45
Croatia 14
Somalia 286Kenya 271
Ethiopia 247Nigeria 104Liberia 304
Cote d’Ivoire 172Ghana 72Haiti 213Peru 95
Ecuador 59El Salvador 25
Mexico 23

Risk of exposure to tuberculosis TB Incidence in Select US Populations
Close contact 1000HIV ~60
Homeless 40Prison 25Asian 18.7
Foreign born 15.6Black 5.8
HIspanic 5.3US born 1.2
TB Elimination Goal 0.1

US Cases of Tuberculosis
Year Cases Rate/100K1953 84304 52.61960 55494 30.71970 37137 18.11980 27749 12.21990 25701 10.32000 16309 5.82010 11182 3.62013 9588 3.0

MMWR 59 (RR-5), 2010
Risk of progression to active disease
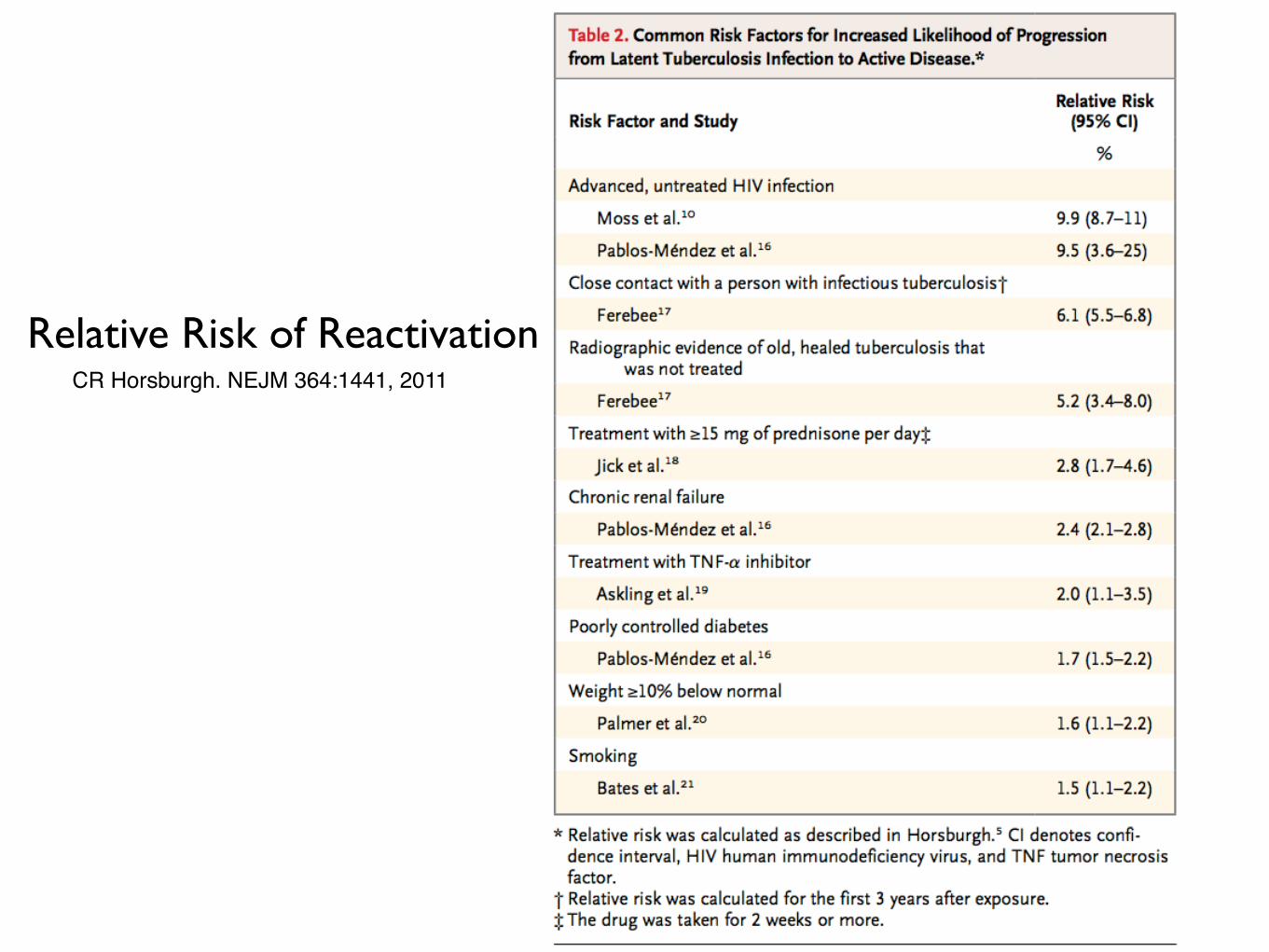
Relative Risk of ReactivationCR Horsburgh. NEJM 364:1441, 2011

Evaluation of Tuberculosis
Management Options!
• Obtain or repeat diagnostic studies!• Wait for final culture results!• Work up for extrapulmonary tuberculosis!๏ No further testing or treatment!๏ Treat latent tuberculosis!๏ Treat active tuberculosis!
- Need respiratory isolation!- Evaluation of vulnerable contacts

Testing Options• TST or IGRA (Quantiferon, TSPOT)!
• CXR!
• AFB smear and culture!
• Other Tests!
• CT scan!
• Bronchoscopy!
• Fine needle aspiration/Biopsy!
• Gastric aspirate!
• Thoracoscopy!
• Endoscopic ultrasound!
• Nucleic acid amplification!
• Molecular tests for drug susceptibility

Testing Options
• TST or IGRA!- May not react for 8-10 weeks
- Cannot distinguish latent from active
- Negative test does not rule out active disease
- Booster effect from old TB infection or BCG (TST)
• CXR!- Look for evidence of old infection as well as active
disease!
- Cannot distinguish latent from active tuberculosis!
- Negative test does not rule out active disease!
• AFB smear and culture!- Negative smear may still be culture-positive!
- Positive smear may be NTM!
- Culture needed for complete susceptibility testing

Recent TB case• 46 year old woman!• Refugee from East Africa!• Arrived in US 2013!• Admitted with!
- cough!- night sweats!- fatigue!- weight loss

• TSPOT- borderline!• Sputum smears negative x3!• Sputum NAAT negative x2!• Sputum cultures pending

Molecular studies
• Nucleic acid amplification
• PCR-based studies of MTB identification and drug resistance
• Whole genome sequencing

Molecular studies Advantages
• More specific and sensitive than AFB smear
• Faster than culture
• Identify MTB as the pathogen
• Early indication of MTB drug-resistance
• Identify specific strain of MTB
• Becoming more widely available

Molecular studies Can help to decide
• Need for empiric treatment
• Treatment drugs
• Need for isolation
• Initiation of contact investigation
• Transmission patterns of infection

!
NO !GOLD STANDARD !FOR DIAGNOSIS!
Latent Tuberculosis

Prevalence of LTBI: US Residents
Horsburgh, Rubin. NEJM 364:1441, 2011

Tuberculin Skin Test
• Non-tuberculous mycobacteria
• BCG
• Improper reading
• Active tuberculosis!
• Cell-mediated immunosuppression by!
• disease !
• medication!
• extremes of age!
• Some chronic diseases (A)!
• Severe or febrile illness (B)!
• <1 month after !
• live virus vaccine (C)!
• some illnesses (D)!
• Improper placement or reading
A. Chronic renal failure, cirrhosis, malnutrition, sarcoidosis!
B. Includes tuberculosis!
C. MMR, Polio, Yellow Fever!
D. Measles, mumps, rubella, varicella, mononcleosis, typhoid, brucellosis, influenza
False-positive False-negative

TST Interpretation

Interferon gamma release assays
• Measures release of interferon gamma by lymphocytes to stimulation by specific MTB antigens- ESAT-6, CFP-10, TB7.7(QFT only)
• Test has positive and negative controls
• No cross-reactivity with BCG or Mycobacterium avium-intracellulare
• Cross-reactive with M. bovis, M. kansasii, M. marinum, M. szulgai
• Blood test, requires only one visit
• Two approved tests- Quantiferon and T-Spot

CDC Guidelines for IGRA Use 2010
“QFT-G may be used in place of (but not in addition to) a TST in all situations in which CDC recommends TST as an aid in diagnosing MTB infections...”
Performance of IGRA may be decreased in immunocompromised patients, including children less than 5 years old
MMWR 59 (RR-5), 2010

2010 CDC Recommendations for IGRA MMWR 59 (RR-5), 2010
• IGRA preferred • likelihood that TST will not completed
• Patient has received BCG vaccine
• TST preferred • Children less than 5 years old
• No preference • Contact investigation
• Regular screening
• Both TST and IGRA can be considered • High risk for TB infection or disease
• After positive TST in patient with BCG vaccination
• Indeterminate or borderline IGRA

Diagnosis of latent tuberculosis
• IGRA is the new BLACK but testing is still imperfect
• Assess risk for exposure and progression
• Look for evidence of infection on CXR
• In the end, diagnosis is a clinical decision

Effect of LTBI treatment

Total US Population (190M)
Latent TB
Active TB
Model developed in 1963 1. Percent LTBI in population- 13% (25M)!2. Annual reactivation TB from LTBI- 0.16% (40K)!3. New infection from each new active cases- 3
(120K)!4. New active disease from new infections- 8% (10K)
50,000 new cases of active TB per year+
Latent TB in the US
Current estimate of LTBI prevalence- 4% (11 M)!AJRCCM 171:348, 2008

What treatment is needed?‣ Latent TB
‣ Active Disease
‣ Other considerations
• Site of infection
• Drug-resistance
• Hepatic and renal function
• Risk of adverse drug effects
• Possible drug interactions
• Patient input

Treatment of Latent Tuberculosis
Regimen Duration Interval
Isoniazid 9 months 6 months
daily or twice weekly
Rifampin 4 months daily
Isoniazid and Rifapentine 3 months weekly

Once weekly LTBI treatment
• rifapentine 900 mg and isoniazid 900 mg
• total duration of treatment: 12 doses
• Recommended for health persons ≥12 years
• Preferred regimen for children 2-11 is INH alone
• NOT recommended for
• Children <2 years old
• HIV patients on anti-retroviral therapy
• Pregnant women
• Resistance to INH or RIF

Once weekly LTBI treatment
• Directly observed therapy is recommended
• Monthly clinical monitoring
• Consider in persons unlikely to complete 9 months of therapy
• Case-by-case consideration in children ages 2-11, patients with underlying conditions associated with tuberculosis.

Diagnosis of active tuberculosis
• MTB on culture/molecular studies
• Consistent histology, especially necrotizing or caseating granuloma
• Clinical manifestations
• Imaging findings consistent with disease
• Positive AFB smear
• High risk of exposure and progression
• Response to therapy with anti-tuberculosis treatment


Treatment of Tuberculosis. MMWR 52/RR-11

Treatment Regimens Length of Treatment
4 mo Culture-negative
6 mo Must include RIF and PZA
9 mo
CNS TB Bone TB
Failure to clear sputum culture in 2 months PZA for less than 2 months
HIV patient (?)
12 mo Cannot use RIF
18-24 mo MDR TB
Treatment completion determined by number of doses of therapy

Tuberculosis Disease!Standard Treatment
Time Initiation 2 months 6 months
Drugs RIPE + B6 isoniazid rifampin
end of therapy at 180 doses
CommentsCan stop ethambutol if strain of TB sensitive to
other drugs
check sputum culture at 2 months
extend treatment to 9 months if no negative
sputum culture in cavitary disease
R rifampinI isoniazidP pyrazinamideE ethambutol

Monitoring for Adverse Effects
Baseline Liver function panel, creatinine, CBC, platelets, visual acuity and color vision
Follow-up eye exam if on ethambutol, ALT if at risk for hepatotoxicity

Adverse Effects of First-line Drugs
Drug Adverse Effect
isoniazidhepatotoxicity, peripheral neuropathy, CNS effects, lupus-like
syndrome, monoamine poisoning
rifampin flu-like syndrome, hepatotoxicity, anemia, thrombocytopenia, renal failure, drug interactions
pyrazinamide hepatotoxicity, polyarthralgia, gout
ethambutol impaired vision, peripheral neuropathy

Extrapulmonary Tuberculosis
MMWR 52/RR-11: 59, 2003

Special Situations
PediatricMore likely to have primary disease
More likely to have disseminated disease Less likely to transmit infection
Often do not have culture results
PregnancyAminoglycoside not recommended for use
PZA not recommended for use (US) Risk for congential transmission (small)
Kidney disease Usual doses of INH and RIF Increase dosing interval for PZA, ETB, aminoglycosides
Liver diseaseRisk for catastrophic hepatitis
INH, RIF, PZA all have potential liver toxicity Need MDR regimen to avoid all hepatotoxic agents
Refusing treatmentBe creative, work with patient in choosing treatment alternatives
Consider the possibility of mental impairment in your patient Know the state law that pertains to TB treatment

Drug Resistance
Pansensitive 0.9
Single drug resistance 8
Polydrug resistance 21
Multidrug resistance 30-40
Extensive drug resistance 57
Treatment failure (%)
1. Lew. Ann Intern Med 149:123, 2008!2. Orenstein. Lancet Infect Dis 9:153, 2009 !3. Jacobson. Clin Infect Dis 51:6, 2010

Case
• Started on treatment for pulmonary tuberculosis in Laos 3.5 months ago
• Diagnosis based on abnormal CXR and sputum growing Mycobacterium
• Sputum smear was negative, TST not done
• On daily isoniazid 300 mg, rifampin 450 mg, ethambutol 400 mg
• No pyrazinamide because she was breast feeding when treatment started
• No antibiotic susceptibility studies done
• No medications since arriving in MN 3 weeks ago
• Patient has no TB symptoms
23 year old Laotian woman
• What is the diagnosis?!
• Is the treatment correct?!
• Medication!
• Doses!
• Is breast feeding an issue?!
• Is drug resistance an issue?!
• Significance of the duration of lapse of therapy!
• What should you do now?

Case
• Started on treatment for pulmonary tuberculosis in Laos 3.5 months ago
• Diagnosis based on abnormal CXR and sputum growing Mycobacterium
• Sputum smear was negative, TST not done
• On daily isoniazid 300 mg, rifampin 450 mg, ethambutol 400 mg
• No pyrazinamide because she was breast feeding when treatment started
• No antibiotic susceptibility studies done
• No medications since arriving in MN 3 weeks ago
• Patient has no TB symptoms
23 year old Laotian woman
• Diagnosis- presumed pulmonary TB!
• Treatment- should include PZA, rifampin dose appropriate for weight!
• PZA can be used with breast feeding!
• Drug resistance is a potential issue!
• Duration of lapse of therapy not sufficient to warrant restarting complete course of treatment

Case
• Started on treatment for pulmonary tuberculosis in Laos 3.5 months ago
• Diagnosis based on abnormal CXR and sputum growing Mycobacterium
• Sputum smear was negative, TST not done
• On daily isoniazid 300 mg, rifampin 450 mg, ethambutol 400 mg
• No pyrazinamide because she was breast feeding when treatment started
• No antibiotic susceptibility studies done
• No medications since arriving in MN 3 weeks ago
• Patient has no TB symptoms
23 year old Laotian woman
• Obtained sputum cultures and started 4 drug treatment!
• Repeat CXR at 2 months showed improvement of RUL infiltrate!
• Continued 4 drug treatment for a total of 6 months.

CaseAt presentation After 4 months of treatment

Keep in Mind
➡ Cannot give one drug to a patient with active tuberculosis
➡ Tuberculosis is not always pulmonary
➡ You do not need to make an immediate decision
➡ Others beside your patient may be at risk










![v P ] v X } u [Digital Electronics for IBPS IT-Officer 2014] Input Output A B C False False False False True False True False False True True True Symbol for And gate: Also C= A.B](https://static.fdocuments.in/doc/165x107/5aad019c7f8b9aa9488db79d/v-p-v-x-u-digital-electronics-for-ibps-it-officer-2014-input-output-a-b-c.jpg)