
Ttie Internationol Journai of Periodontics & Restofotive
9
Ttie Internationol Journai of Periodontics & Restofotive Dentistry
Transcript of Ttie Internationol Journai of Periodontics & Restofotive

Ttie Internationol Journai of Periodontics & Restofotive Dentistry

131
The Subepithelial Connective TissueGraft Palatal Donor Site: AnatomicConsiderations for Surgeons
Gary M. Reiser. DDS'Jahn F. Bruno. DDS, MS"Parker E. Mahan. DDS. PhD'"Lynn H. Larkin. PhD'"'
Surgeons must become completely familiar with the anatomy of thepalatal donar site to feel confident in providing the subepitheliat connec-tive tissue graft procedure. Variations in the size and shape of the hardpalate affect fhe dimensions of donor tissue harvested, as welt as the loca-tion of the greater palatine neuravascuiar bundie. This article classlfjespalatal vaults according ta height as high average, and shallow.tllustratians ond cadaver dissectian are utilized to demonstrate that sur-geans can gain substantial donor tissue specimens without encounteringthe neurovasoular bundle. Actions to be followed in the unlikely event thatthe neuravasculature is encountered are reviewed. (Int J Periodont RestDenf 1996:16:131-137.)
•Institute for Advanced Dental Studies, Swampscott.Massachusetts.
-Assistant Clinicai Professor, Periadontics, Baltimore College ofDental Surgery University of Maryland. Bdltimore. ivioryland.
"Distinguished Service Prafessor Emeritus. University ot FloridaCollege oi Dentistry. Gainesyille. Florida.
"Professor. Department ot Anatomy and Cell Biology, University ofFlorida College af Medicine. Gainesville, Florida.
Reprint requests: Dr Gary M. Reiser, institute tor AdvancedDental Studies. 90 Humphrey Street. Swampscott. Massachusetts
01907.
The subepithelial connectivetissue graft procedure'"'' hasgained wide ooceptance. Thistechnique typicaliy utilizesdonor tissue retrieved from thehord palate. The purpose of thisarticle is to describe theanatomy of the paiatai donorsite and to identify structuresfhat could potentialiy createsurgical compiications.
The hord paiate is com-posed of the palotal process ofthe maxillary bone ond the hor-izontoi process of the palatinebone. It is covered with masti-catory mucoso. The soft tissueextending superioriy from thecementoenamei junction (CEJ)of the maxillary posterior teethfor approximateiy 2 to 4 mm iscomposed ot dense laminoproprio. The connective tissuecontinuing on to the midiine ofthe palote contains iooseiyorgonized glandular ond adi-pose tissue.
The height, length, ondthickness ot donor tissue thatcan be obtained varies with thediffering anatomic dimensions
Volume 16. Number 2,199Ó

132
Fig I A strip ot palatal fissue has Peen removed in the pre-molar region cf a cadaver. A periodontal proDe demon-strates opproximoteiy 5 mm of tissue depth.
Fig 2 A strip of paiatdi tissue has been removed in fhemoiarregion af a cadaver A periodohtai probe demonstratesopproximateiy 3 mm af tissue depfh.
Fig 3a A computer-assisted Kadaohrome (Kodak) demon-strating o high paiatai vauit ih a cadaver. The anterior courseot the greater paiafine nerves and biaod vesseis can be visu-aiized. Note that the heuravascuiar bundie gradually coursesciaser to the CEJs beginning appraximoteiy af fhedistapaiatai iine angie ot the cahine (arrow).
Fig 3b Coiored yarn placed in the palatal groove that hous-es the greater and lesser palatine nerves and vesseis (si<utt).Note the thin isthmus of bane bridging over the neurovascuiarstructures (pnoW). The distonce from the paiatai OEJ ta thevessels and nerves varies with the shape of the paiatai vaultand the reglan of dissection. The thick alveoiar process paiataifo the molars can be noted.
of the paiatai vault. The greatestheight (inferior-superior dimen-sion) con be found in the high(U-shaped) poiatoi vouit. Thegreatest length (anterior-poste-rior dimension) can be found ina large polate. The thickest tis-sue can be fcund in the area
trcm the mesiai line ongie of thepaiatol root of the first molar tofhe distal line angle of thecanine (Figs 1 and 2). A thickalveolar process and/or exosto-sis is often encountered in themelar region, which iimits theiength and thickness of tissue
that may be obtained.^ Theclinician can eosiiy determinethe thickness of the donor tissueby needle soundings fallowingthe administration of iocal anes-thesia.
The Internationol Journai ot Periodontics & Restorative Dentistry

133
HighPalate
fig 4a Neurovoscuiar sfrucfures are noted of oonsiderabledistance from the CEJs in the high poiotai vouif (codover dis-section).
Fig 4b Diagram of fhe neurovascular bundie in the high (U-shaped) paiafol vouif. The overage distonce from fhe CEJ tothe neurcvoscuiar bundle is i7mm.
Greater palatineartery and nerve
Greater palatineartery and nerve
Fig 4c Diagram of fhe neurovasouiar bundle in fhe averagepaiatai vault The distonce from the CEJ fo the neurovoscuiarbundle is 12 mm.
Fig 4d Diogrom of fhe neurovascuior bundle in the shallow(fiot) paiatoi vault. The overoge distonce from Ihe CEJ fo fheneurovoscuiar bundie is 7 mm.
Neurovascular cansideratians
The greater and lesser palatinenerves and blood vesseis gainentrance into fhe palate bypassing through the greaterand iesser paiafine foramina.The foramina iocafions vary, but
generaiiy can be identified api-cal to the third moiar at thejunction of the verticai and hor-izontal parts ot the palatinebone. These nerves and vesselscourse anteriorly (Fig 3a) withina bony groove (Fig 3b), Theneurovascuiar bundle may be
iocated 7 fo 17 mm from thecementoenamei junctions ofthe maxillary premoiars andmolars (Bowers GM, personaicommunication, 1995) (Figs 4ato 4d), Prior to making fhe initialincision fo procure fhe donorfissue from fhe paiate, the
Volume 1Ó, Number 2,1996

134
Fig 5 Palpation of fhe bany groovefhaf iiauses fhe neuravascular bundle.
Fig 6a (left) Location of the greaterpaiaflne groave indicated by an indeii-b/e pen marking.
Fig 6b (right) Periodonfal probe inplace Indicafing fhdt fhe disfance fromthe CEJ af fhe second premalar to fheindelible line is Í 7 mm.
surgeon should attempt to pal-pate the bony graave (Fig 5).The groove is easiest to paipateat its most posterior extent. Thispalpation aiiows the surgeon todetermine the maximum api-cai (superior) placement of theincision that is possible beforeviolating the neuravascularbundie. The surgeon may wishto indicate this groove with aiine made by an indelibiemarker on the soft tissue sur-tace of the hard palate (Figóa), which can be a useful ref-erence when obtaining thedonor tissue (Fig 6b).
When the paiatal vault issholiow (fiat), neurovascuiarstructures wiii be iocated moreproximaily to the CEJ (see Fig4d). When the palatal vault ishigh (U-shaped), the structureswiii be iocated at a greater dis-tance from the CEJ (see Figs 3a,3b, 4a, and 4b). The retrieval ofdonor tissue from the premolarregion in the high and averagepaiate (see Figs 4b and 4c)offers a greater margin at safetythan retrieval from the shaliow(flat) palatal vault (see Fig 4d) inreference to the neurovascuiarstructures. The mean height offhe paiatGl voult (the shcrtest
distance between the midiineof the hard and soft palatesand the CEJs of the first molars)in an aduit male is 14,90 mm,with a standard deviation of2.93 mm. The mean height in onaduit femaie is 12,70 mm, with astandard deviation of 2.45 mm,^Caution must always be exer-cised not to violate the neuro-vascuior bundle when obtainingthe donor tissue, but extremecaution must be exercisedwhen the paiate is shallow.
The terminal branch of thegreater palatine artery extendsto the incisai foramen, where itpasses superiorly up the incisai
The Internationai Journai of Peiiodontics & Restorotive Dentistry

135
canal onto the nasal septuminto Kiesselbach's area.' In thisanterior palatal region, theartery drops interiorly decreas-ing the distance trom theartery to the cementoenameljunctions of the anterior feeth.Therefore, the authors recom-mend limiting the anteriorextent ot the donor site surgeryto the distal line angle ot thecanine tooth to avoid damageto the greater palatine nerveand artery (see Figs 3a and3b), which could cause postsur-gical bieeding and paresthesiaor anesthesia, instances ofparesthesia and anesthesiahave been encountered whenthe donor site has beenextended anterioriy to the iat-erai incisor region and beyond.
It the surgeon encountersbleeding tram the palatine ves-sels, the tollowihg actions canbe taken in sequence:
1, Immediate direct applica-tion ot pressure and theinjection ot a local anes-thetic containing a vaso-constrictor into the region.Pressure shouid be constanttor at least 5 minutes.
2, Piacement ot one or moresutures proximal to thebleeding site (ie, betweenthe bieeding site and thetora men).
3, Elevation of a full-fhicknessflap—the vessel is retiectedwith the fiap, visualized, and
Donor site surgery in \hecadaver
To visualize the anatomic struc-tures when obtaining donor tis-sue from fhe palafe, the proce-dure was perte rmed oncadavers tollowing the mefh-ods previousiy described byBruno.'' incisions were made inthe palafes ot cadavers, repro-ducing the palatal incisionsneeded to obtain donor tissuefor ciinicai patients (Fig 7a), Thetissue was then eievafed andremoved trom fhe palataldonor site (Figs 7b and 7c). Thedonor tissue taken from theaverage or high paiate typi-cally measured approximately5 to 8 mm in height (Fig 7d).When the donor tissue proce-dure was completed in thecadaver, the paiatai tissue cov-ering the donor site (overlyingflap) was removed, and thedonor fissue was replaced todemonstrate the distancebetween the superior edge offhe donor fissue and thepaiatai neurovascuiar struc-tures (Fig 8). In a high palatalvauit this distance measuredapproximateiy 4 to 7 mm.
Volume 16, Number 2,199Ó

136
f/g 7a Surgicai blade in place at the compietion of an inci-sion parallel to the long axis of the teeth." The length of theoutting edge af the blade can be measured and used as adepth gauge to avoid the neuravoscuiar bundie (cadaver).
Fig 7b Donor tissue being eievated (cadaver).
Fig 7c me aon^ir lisi'.j'..- uilu: Lit.-)ipalatai danor site (cadaver).
ri,-flloved from the Fig 7d The donor tissue measures 7 mm in height (cadaver).
The International Journal oí Periodcntics S Restorative Dentistry
137
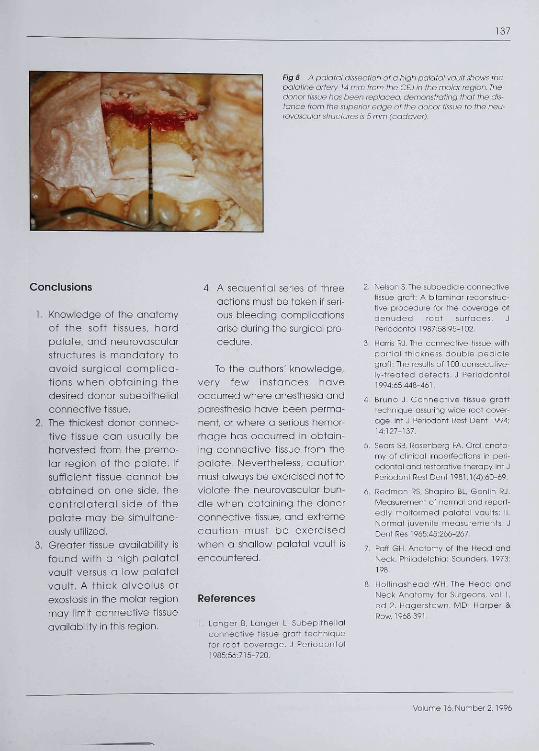
Fig 8 A palatal dissection of a high palatal vauit shows thepalatine ortery 14 mm from the CEJ in the rnaiar regian. Thedonor tissue has been replaced, demonstrating that the dis-tance from the superior edge of the donor tissue fo the neu-rovascuiar structures is 5 mm (cadaver).
Conclusions
1. Knowiedge of the onatomyot the sott tissues, hardpalate, and neurovascuiarstructures is mondatory toovaid surgical compiica-tions when obtaining thedesired donor subepithelialconnective tissue.
2. The thickest donor connec-tive tissue can usually behorvested from the premo-lar region of the palate. Ifsufficient tissue connot beobtoined on one side, thecontralqterol side of thepolote may be simultane-ously utilized.
3. Greoter tissue availability isfound with a high paiataivault versus a iow polotoivauit. A thick olveoius orexostosis in the moiar regionmay limit connective tissueavailabiiity in this region.
4, A sequential series of threeactions must be token if seri-ous bleeding compiicotionsorise during the surgicoi pro-cedure.
To the outhors' knowledge,very few instonces haveoccurred where anesthesia andparesthesia have been perma-nent, or where a serious hemor-rhage has occurred in obtain-ing connective tissue from thepaiate. Nevertheiess, cautionmust always be exercised not toviolate the neurovascuior bun-dle when obtaining the donorconnective tissue, and extremecaution must be exercisedwhen o shaiiow poiatai vauit isencountered.
References
1. Longer B, Langer L. Subepitheiialconnective tissue grott techniquefor root coverage. J Periodontoi198556:715-720,
2. Nelson S.the subpedicle connectivetissue graft: A bilominar reconstruc-tive procedure for the oouerage ofdenuded root surfaces. JPeriodontoi 1987;58:95-102.
3. Harris RJ. The connective tissue withpartial thiokness double pediclegraft: The results cf 100 consecutive-ly-treated defeots. J Periodontoi199d;ó5'448-d61.
4. Bruno J. Connective tissue grafttechnique assuring wide root cover-age. Int J Periodont Rest Dent 1994;Id: 127-137
5. Sears SB. Rosenberg FA. Orol onato-my of clinioal imperfections in peri-odontal ond restorative therapy. Int JPeriodont Rest Dent 1961jl(4):60-69.
6. Redman iiS. Shapiro BL, Gonlin RJ,Measurement of normal ond report-ediy maiformed paiatai voults: il.Nprmai juvenile measurements. JDent Res 1965:45:266-267.
7. Paff GH, Anotomy of the Head andNeck. Philadelphio: Saunders, 1973:198.
8. HQlhngshead WH. The Head andNeck Anotomy for Surgeons, vol 1,ed 2. Hagerstown, MD: Harper &Row,1968:39l.
Volume 16, Number 2,1996



















