Troubleshooting implantable cardioverter-defibrillator ...bhrs.com/files/files/How To &...
13
doi:10.1136/hrt.2007.122762 2008;94;649-660 Heart Lieselot van Erven and Martin J Schalij cardioverter-defibrillator related problems Troubleshooting implantable http://heart.bmj.com/cgi/content/full/94/5/649 Updated information and services can be found at: These include: Data supplement http://heart.bmj.com/cgi/content/full/94/5/649/DC1 "web only references" References http://heart.bmj.com/cgi/content/full/94/5/649#BIBL This article cites 21 articles, 11 of which can be accessed free at: Rapid responses http://heart.bmj.com/cgi/eletter-submit/94/5/649 You can respond to this article at: service Email alerting the top right corner of the article Receive free email alerts when new articles cite this article - sign up in the box at Topic collections (4419 articles) Epidemiology (503 articles) Pacing and electrophysiology (3122 articles) Interventional cardiology (9790 articles) Drugs: cardiovascular system (310 articles) Education in Heart Articles on similar topics can be found in the following collections Notes http://journals.bmj.com/cgi/reprintform To order reprints of this article go to: http://journals.bmj.com/subscriptions/ go to: Heart To subscribe to on 9 June 2009 heart.bmj.com Downloaded from
Transcript of Troubleshooting implantable cardioverter-defibrillator ...bhrs.com/files/files/How To &...
doi:10.1136/hrt.2007.122762 2008;94;649-660 Heart
Lieselot van Erven and Martin J Schalij
cardioverter-defibrillator related problemsTroubleshooting implantable
http://heart.bmj.com/cgi/content/full/94/5/649Updated information and services can be found at:
These include:
Data supplement http://heart.bmj.com/cgi/content/full/94/5/649/DC1
"web only references"
References
http://heart.bmj.com/cgi/content/full/94/5/649#BIBL
This article cites 21 articles, 11 of which can be accessed free at:
Rapid responses http://heart.bmj.com/cgi/eletter-submit/94/5/649
You can respond to this article at:
serviceEmail alerting
the top right corner of the article Receive free email alerts when new articles cite this article - sign up in the box at
Topic collections
(4419 articles) Epidemiology � (503 articles) Pacing and electrophysiology �
(3122 articles) Interventional cardiology � (9790 articles) Drugs: cardiovascular system �
(310 articles) Education in Heart � Articles on similar topics can be found in the following collections
Notes
http://journals.bmj.com/cgi/reprintformTo order reprints of this article go to:
http://journals.bmj.com/subscriptions/ go to: HeartTo subscribe to
on 9 June 2009 heart.bmj.comDownloaded from

ARRHYTHMIAS
Troubleshooting implantablecardioverter-defibrillator relatedproblemsLieselot van Erven, Martin J Schalij
c Additional references arepublished online only at http://heart.bmj.com/content/vol94/issue5
Department of Cardiology,Leiden University MedicalCenter, Leiden, The Netherlands
Correspondence to:Dr Martin J Schalij, Departmentof Cardiology, Leiden UniversityMedical Center, PO Box 9600,2300 RC Leiden,The Netherlands;[email protected]
Since its introduction, now more than 20 yearsago, the implantable cardioverter-defibrillator(ICD) has evolved from a non-programmable(committed) device into a sophisticated multi-programmable, multi-functional device with exten-sive diagnostic and therapeutic options. The morerecent combination with cardiac resynchronisationtherapy (CRT) further expanded its use to selectedpatients with severe symptoms of heart failure andleft ventricular dyssynchrony at risk of suddencardiac death.
Whereas ICD technology developed rapidly,endocardial ICD leads, consisting of an integratedpace/sense and shock electrode positioned in theright ventricle, remained essentially unchangedafter their introduction in the late 1980s, asidefrom a reduction in diameter.
In the early years, ICD implantation was a majorsurgical procedure associated with significantmorbidity and mortality, necessitating a thoracot-omy to place the epicardial leads and patches andan abdominal incision to insert the bulky firstgeneration device. With the introduction of endo-cardial shock electrodes and the significant reduc-tion in size and weight of the devices, thecomplexity of the implantation procedure wasreduced significantly and currently most systemscan be implanted in the catheterisation laboratoryby the electrophysiologist under local anaesthesia.
However, compared to the relative ease of thecurrent implantation procedure, follow-up andtroubleshooting of ICD patients has become amuch more complicated and challenging process,demanding extensive knowledge of cardiac electro-physiology as well as a thorough understanding ofthe different features and algorithms incorporatedin modern (CRT) ICDs. Combined with theincreasing number of ICD patients, troubleshoot-ing of ICD related problems has become achallenging task. In this overview some of themost important device related problems will bediscussed.
TROUBLESHOOTING POLICYDevice related problems in ICD patients may varyfrom relatively simple sensing or pacing problemsto life threatening episodes of inappropriate shocksor failure of shock delivery. In analysing andsolving ICD related problems, it is important to
maintain a structured approach towards everypatient presenting with possible device relatedissues.
ICD troubleshooting starts either when a patientwith a device presents at the hospital with apossible device related complaint or when a regulartechnical follow-up reveals a possible device devia-tion. In order to identify and solve the problem, thedevice should be interrogated extensively and theretrieved data should be stored on disc to allowoffline analysis and comparison with historicaldata.
After identification of the problem, the possiblecause is analysed. Different methods of evaluationmay be needed, such as manipulation of the device,observing the effect of postural changes and deepinspiration and expiration, 12 lead electrocardio-graphy, a chest x ray, and 24 h Holter monitoring.
Patients with an ICD related problem presentwith complaints which generally fall into one ofthe following four categories:
c Shocks (appropriate, inappropriate or failure todeliver therapy)
c Dizziness/fainting
c Palpitations
c Alerts (audible beeps or sensed vibrationsoriginating from the ICD).
SHOCKSWhereas ICD therapy improves survival of selectedpatient groups and patients may have the feeling ofbeing protected, the actual delivery of shocks, bothappropriate and inappropriate, may have signifi-cant psycho-sociological consequences. Severalstudies have demonstrated that the occurrence ofICD shocks negatively influences patients’ sub-jective feeling of physical and mental wellbeing.1 2
This is caused by the fact that shock delivery is atraumatic physical experience and because of thepsychological effect of confronting the patientwith his/her compromised physical status or withhis/her risk of developing life threatening arrhyth-mias.
In general, most single shocks are appropriately(and successfully) delivered to terminate an episodeof ventricular tachycardia/fibrillation, and becausethe ICD worked properly the patient may even bereassured.
Education in Heart
Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762 649
on 9 June 2009 heart.bmj.comDownloaded from
On the other hand, multiple shocks are moreoften classified as inappropriate. The experience ofreceiving multiple shocks during consciousness isextremely distressing for both patients and wit-nesses, and warrants extensive clinical evaluationto reveal the possible cause and to reprogram thedevice or take other necessary measures to preventfuture inappropriate shock episodes. Therefore,patients presenting after multiple shocks shouldalways be advised to have their ICD interrogated,
whereas patients who received a single shock cangenerally be reassured.
How does the ICD decide to deliver a shock?All devices use the signal rate recorded by the rightventricular lead as the first detection criterion. Inorder to be declared an arrhythmia, a specifiednumber or percentage of sensed events must occurat a rate higher than the programmed cut-off rate.These sensed events may originate from a real
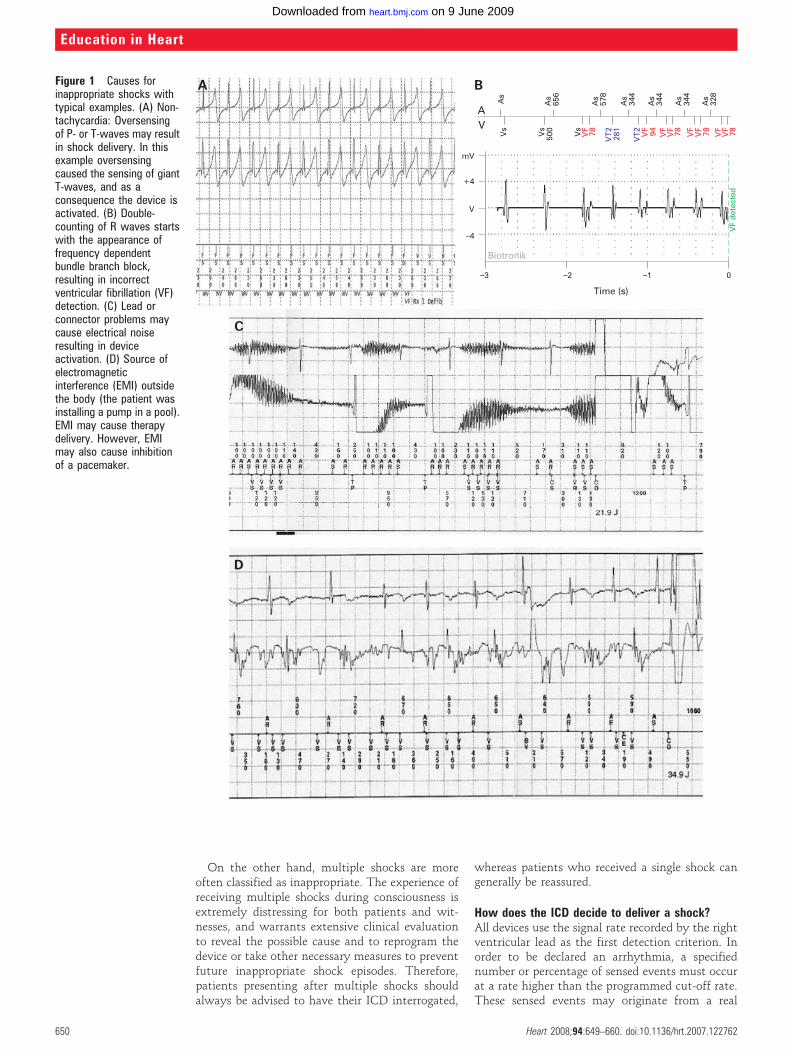
Figure 1 Causes forinappropriate shocks withtypical examples. (A) Non-tachycardia: Oversensingof P- or T-waves may resultin shock delivery. In thisexample oversensingcaused the sensing of giantT-waves, and as aconsequence the device isactivated. (B) Double-counting of R waves startswith the appearance offrequency dependentbundle branch block,resulting in incorrectventricular fibrillation (VF)detection. (C) Lead orconnector problems maycause electrical noiseresulting in deviceactivation. (D) Source ofelectromagneticinterference (EMI) outsidethe body (the patient wasinstalling a pump in a pool).EMI may cause therapydelivery. However, EMImay also cause inhibitionof a pacemaker.
Education in Heart
650 Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762
on 9 June 2009 heart.bmj.comDownloaded from

tachycardia, either supraventricular tachycardia(SVT) or ventricular tachycardia (VT), but alsofrom signals originating from another source (figs 1and 2).
To discriminate between SVTs and VTs, variousalgorithms have been developed with the intentionto improve specificity for discrimination of VT fromSVT without compromising the sensitivity for
detection and treatment of VTs.3–5 Current ICDscan be programmed into three different cycle length(CL) related zones and the detection algorithms areprogrammable in the two lowest zones (in case ofprogramming three different zones). The highestprogrammable zone is meant to detect fast VT or VFwithout any further discrimination to avoid unne-cessary therapy delivery delay.
Figure 2 Causes forinappropriate shocks withtypical examples(continued). (E) Source ofelectromagneticinterference (EMI) insidethe body: oversensing ofdiaphragmatic potentials.The implantablecardioverter-defibrillator(ICD) criteria for initialventricular fibrillation (VF)detection are met (8 out of10 intervals classified asfast), but VF is notreconfirmed as thediaphragm potentials ceaseand the ‘‘Duration’’ is notmet (Duration isprogrammed to 1 s). VFtherapy is not delivered.Note that after the firstintrinsic beat (arrow) thesensing of noise isreduced, due to the autogain sensitivity (see textfor details). (F) Atrialarrhythmia with fastconduction (but initially not1:1) and a ventricular ratefulfilling the detectioncriteria followed byantitachycardia pacing.Thereafter, the atrialarrhythmia is conducted1:1. (G) Shock deliveredduring sinus tachycardiajust above the cut-off ratefor VF (188 beats/min),resulting in a ventriculartachycardia.
Education in Heart
Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762 651
on 9 June 2009 heart.bmj.comDownloaded from

Available algorithms include sudden onset,sustained high rate duration, rate stability, andmorphology/wavelet/rhythm ID capabilities forsingle and dual chamber devices, whereas dualchamber devices can use additional informationretrieved from the atrial lead, like atrial toventricular timing relationships. All currentlyavailable algorithms have known limitations(table 1). By combining some of these algorithmsthe amount of inappropriate inhibition or therapydelivery can be further reduced.
It is important to have knowledge and under-standing of the incorporated automatic algorithmsfor discrimination of arrhythmias in order to applythem effectively.
Sudden onsetThe intended use of this algorithm is to discrimi-nate sinus tachycardia from VT. With the onset ofa VT, there is usually a sudden increase inventricular rate (as opposed to, for example, anexercise induced sinus tachycardia). The suddenonset criteria is effective in discriminating VT fromsinus rhythm except in the case of only a minimalCL difference when, for example, during sinustachycardia a VT is initiated, or in case of slow VT.This algorithm may lead to false positive as well asfalse negative therapy delivery decisions. Patienttailored programming is thus mandatory toimprove both sensitivity and specificity. To reducethe chance of a VT going untreated, a specifiedacceptance time for a sustained high ventricularrate can be programmed as an overriding algorithm(sustained high ventricular rate). However, thisfeature in itself has disadvantages since it can leadto inappropriate shocks—for example, an appro-priately withheld shock during sinus tachycardiawill be delivered after expiration of the preset timeinterval. On the other hand, sustained high rateduration can also (when a long duration has beenprogrammed) result in a potentially dangerousdelay of therapy delivery.
StabilityThis algorithm is intended for discrimination offast conducted atrial fibrillation/flutter from VT. Itis an effective discriminator, except in the case of arelatively stable ventricular rate during atrialfibrillation, which occurs more often at higherventricular rates (due to a limited absolute varia-tion in RR intervals). As with the onset algorithm,stability may lead to both false positive and falsenegative declarations. During atrial fibrillationwith relatively stable RR intervals, inappropriatetherapy can be delivered (false negative) and withrelatively unstable VTs, therapy may inadvertentlybe inhibited (false positive). In this case, anoverriding algorithm using the elapse of time isuseful to overcome the inappropriately inhibitedtherapy for unstable VT, but will lead tomore inappropriate therapy in the case of atrialfibrillation.
Electrogram morphologyMorphology (St Jude Medical, St Paul, Minnesota,USA), Wavelet (Medtronic, Minneapolis,Minnesota, USA) single chamber ICD, andRhythm ID (Boston Scientific, Natick,Massachusetts, USA) are features incorporatedinto the different devices to discriminate an SVTfrom a VT, especially in single chamber devicesthat lack additional information retrieved fromthe atrial lead. These algorithms are based onretrieving a template of the electrogram duringbaseline rhythm. Morphology uses the near-fieldrate electrogram derived from the small intracar-diac bipole; Wavelet uses the far-field shockelectrogram, analysing the electrical activitybetween a shock electrode and the intracardiacelectrode, and taking the electrical axis intoaccount; Rhythm ID uses the far-field shockelectrogram aligned in time to the rate electro-gram, combining electrical axis and timing. Whenan event is detected in the applied zone, themorphology of each electrogram is compared tothe baseline template and the percentage of matchor mismatch is calculated. The advantage of thesealgorithms is the independence of the atrioven-tricular (AV) sequence and timing relationship.No comparative studies on efficacy are, however,available.
Atrioventricular (AV) sequence/timing algorithmsDual chamber devices enable the use of informa-tion provided by the atrial lead. If the ventricularrate exceeds the atrial rate (V.A), the diagnosis isVT. Comparison of atrial and ventricular rateduring tachycardia can be used as an initial step inthe decision tree or as an ‘‘overrider’’ after otheralgorithms have been applied by the device. Thisinformation can also be used in combination withthe above mentioned algorithms to enhancesensitivity and specificity of arrhythmia discrimi-nation, or it can be used for separate AV timerelationship algorithms. Weaknesses with these AVsequence/time algorithms are 1:1 conducted atrial
Table 1 Detection algorithms in implantable cardioverter-defibrillators: intended useand weaknesses
Discrimination Algorithm weakness
Single and dual chamber device
Sudden onset Sinus rhythm vs VT VT starting during sinus tachycardia
VT below cut-off that accelerates
Rate stability AF vs VT Unstable VT
Stable conducted AF
Morphology/Wavelet/Rhythm ID All SVT vs VT Aberrant conduction
Mismatching with template
Dual chamber device
Atrial: ventricular rate V.A with VT Atrial undersensing with AT
with 1:1 AV relationship‘‘Double tachycardia’’: concurrent atrialand ventricular tachycardia
Misinterpretation of AV and VArelationship
AF, atrial fibrillation; AT, atrial tachycardia; AV, atrioventricular; SVT, supraventricular tachycardia; VA,ventriculoatrial; VT, ventricular tachycardia.
Education in Heart
652 Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762
on 9 June 2009 heart.bmj.comDownloaded from

tachycardias with prolonged AV time and VTswith 1:1 retrograde conduction. Although nostudies have been conducted to support thisstatement, the value of the atrial lead informationfor the human interpretation of stored electro-grams is significant, particularly during the onsetof the arrhythmia which device based algorithmscurrently do not take into account.
How to evaluate the appropriateness of a deliveredshock?ICDs are not perfect in their judgment of theperceived signals. The annotated interval markersand other markers provide information and insightinto the decision making process of the ICD.However, a careful review of stored electrograms isoften mandatory to verify appropriateness andefficacy of therapy delivery. The stored episodeelectrograms retrieved from a far-field dipole are ingeneral helpful for analysis, especially when it ispossible to compare these electrograms with a realtime reference electrogram. Furthermore, storedelectrograms can be used to analyse A–V sequenceand timing.
The first step in analysing a possible arrhythmicepisode is to differentiate a real tachycardia (SVTor VT) from a device interpreted tachycardia (figs 1and 2). This is essentially carried out by analysis ofstored episode signals and comparing these withthe information as it is perceived by the ICD whichis represented by the annotation markers. Adecision tree is shown in fig 3.
Inappropriately device interpreted tachycardiaWhen the stored electrograms do not show a realtachycardia but the markers reveal that the deviceinterpreted the signals as tachycardia, the next stepis to trace back the origin of the signals as intra- orextracardiac (figs 1 and 2).6
Intracardiac signals that may cause oversensingand false arrhythmia detection are usually the T-wave or (infrequently) the P-wave (fig 1, panel A).In both cases, VT/VF detection criteria are alreadymet at relatively low heart rates since each heartcycle leads to two sensed signals. T-wave over-sensing occurs more frequently during exercise.Another phenomenon, which occurs infrequentlyin the current generation of ICDs, is doublecounting of the R-wave (fig 1, panel B).
Oversensing of extracardiac signals can be easilyrecognised as high frequency, low amplitudesignals that are not related to the intrinsic electricalactivity of the heart. Electromagnetic interferencefrom an external source, such as a power drill (fig 1,panel C), usually has a more continuous character,may be visible on several channels and cangenerally be tracked back by careful history taking.Internal sources causing oversensing are signalsproduced in case of lead or connector related make-break contacts (fig 1, panel D). Since thesephenomena may occur intermittently, impedance,threshold and sensing parameters may be normalat the time of examination. However, pocketmanipulation or postural changes may revealchanges in these parameters or may show ‘‘noise’’on the real time intracardiac electrogram.
Figure 3 Schematicrepresentation of thepossible causes of shockdelivery. Shocks can beeither delivered because ofa tachycardia (ventricular:appropriate, orsupraventricular:inappropriate) or becauseof oversensing problems(all inappropriate). SVT,supraventriculartachycardia; VF, ventricularfibrillation; VT, ventriculartachycardia.
Education in Heart
Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762 653
on 9 June 2009 heart.bmj.comDownloaded from

These high frequency signals typically start toshow some time after an intrinsic or paced beat.The algorithm of increasing sensitivity which istypical for ICDs (‘‘auto gain sensitivity’’) allowssensing of the low amplitude signals from thediaphragm. This will lead to VF detection (andtherapy delivery) unless the sensing level issuddenly reduced with a subsequent intrinsicbeat or by release of the diaphragm. As these
myopotential related signals may also inhibitpacing, when no intrinsic beat occurs—as inpatients with no or slow intrinsic rhythms—ashock may follow. Fortunately, most patientsrelax at an earlier moment and the diaphragmaticpotentials cease. Myopotentials originating fromthe pectoral muscle may be sensed in case of anisolation defect of the pace/sense lead part of theICD electrode.
Figure 4 (A) ‘‘Trending’’(Boston Scientific) or (B)‘‘Cardiac flash back’’(Medtronic) revealing aventricular rate under thedetection zones.
Education in Heart
654 Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762
on 9 June 2009 heart.bmj.comDownloaded from

Appropriately device interpreted tachycardiaWhen, after an episode, the retrieved signals arejudged not to be due to oversensing but to anactual tachycardia, further evaluation of thearrhythmia has to be performed to verify appro-priateness of the shock since SVT–VT discrimina-tion algorithms are not always perfect. Thisevaluation essentially follows the same algorithmsthat are described above. However, whereas theICD starts applying the algorithm formulas afterthe criteria for initial detection are met, the humaninterpretation has a wider scope and can start atthe actual onset of the arrhythmia. In certain ICDs(Medtronic, Boston Scientific) this extra informa-tion is graphically represented as the interval cyclelength versus the time elapsed since the onset ofthe episode (fig 4). Other information can beretrieved by comparing the episode electrogramsand annotations with data obtained at deviceexamination. For example, the similarity of themorphology of an isolated ventricular extrasystolerecorded by the shock electrode and the morphol-ogy during VT may lead to the diagnosis. Also, theabsence of retrograde conduction during ventricu-lar pacing may help to reject the diagnosis ofventricular tachycardia when during tachycardia a1:1 AV relation exist.
High ventricular rates during atrial fibrillation oratrial flutter are the most frequent cause ofinappropriate detection and therapy (fig 2, panelF). Atrial fibrillation causes typically an unstableventricular rate (although this becomes less athigher ventricular rates as mentioned earlier) butusually does not fulfil the sudden onset criterion.Atrial flutter also results in unstable ventricularrates and is often clearly distinguishable in a dualchamber device unless 1:1 AV conduction occurs.Sinus tachycardia (fig 2, panel G) is sometimeshard to differentiate from 1:1 conducted atrialtachycardia, except for the gradual onset seen insinus tachycardia. The Flashback memory(Medtronic) or Trending feature (BostonScientific) may provide helpful information todiscriminate between the different supraventricu-lar arrhythmias. To distinguish a VT with 1:1
retrograde conduction from a supraventriculartachycardia with 1:1 AV conduction, both onsetof the tachycardia and the morphology recordedwith the far-field dipole may be of help.
Lastly, after a first unsuccessful shock in case ofconcurrent termination of the episode of VT, SVTor device interpreted tachycardia, an inappropriatesecond shock may be delivered. This second shockis so-called ‘‘committed’’, meaning that it isdelivered without further pre-evaluation, for rea-sons of safety to prevent underdetection andundertreatment of arrhythmias. Commitment alsostarts when the first therapy of an episode has beendiverted but the arrhythmia restarts before theepisode has ended.
How to reduce the chance of deliveringinappropriate shocksSince most inappropriate shocks are delivered forsupraventricular arrhythmia, and shocks have animportant negative effect on the quality of life ofpatients, all efforts should be undertaken to reducethe chance of inappropriate shock delivery.
Awareness of risk factors for inappropriateshocks can help to prevent them by customisingthe programming of the ICD at implant.7 Forexample, a history of atrial fibrillation is associatedwith an increased risk for inappropriate shocks.Also, especially in young patients, sinus ratesduring exercise may reach the arrhythmia detec-tion zones easily and it is therefore important toadjust settings if necessary.
Theoretically, the most effective way to avoidinappropriate shocks in these patients would be toprogram the ICD as a single zone device with ahigh rate cut-off, but obviously this is undesirablefor safety reasons since ventricular arrhythmiasmay be missed. However, lowering the VF zonecut-off rate will increase the number of inappropri-ate shocks. Therefore, the best solution in patientswith paroxysmal atrial tachycardia or expected fastsinus rates is multiple zone programming withimplementation of discriminators in the lower twozones, thereby allowing to program the cut-off ratefor the VF zone relatively high (210–220 beats/min). Delivery of shocks for non-sustained VT orSVT can be delayed or even prevented by prolong-ing the programmed time for the device to detect.However, it is important to realise that after thefirst shock, the following shock(s) within a singleepisode, when becoming committed, cannot beavoided.
Inappropriate shocks for other reasons thantachycardiaT-wave oversensing as a cause of inappropriateshocks is an important issue. ICD specific char-acteristics such as filter settings may make somepatients more vulnerable to T-wave oversens-ing and inappropriate shocks. Patient characteris-tics like a high T-wave amplitude, a low R-waveand younger age may contribute to this phenom-enon.8 T-wave oversensing can be prevented by
Box 1: Causes of dizziness, syncope andpalpitations. Most causes for dizziness andsyncope may also give rise to palpitations
c Causes of dizziness and syncope– undersensing of ventricular arrhythmias– polymorphic ventricular tachycardia (VT)– unstable VT around cut-off rate– VT below cut-off rate– non-effective therapy– non-sustained VT
c Causes of palpitations– atrial tachyarrhythmias– frequent premature ventricular contractions
(PVCs)– ventricular pacing
Education in Heart
Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762 655
on 9 June 2009 heart.bmj.comDownloaded from

programming the sensitivity level of the automaticgain control to a less sensitive level (this howevermay increase the risk of underdetection of ordelayed therapy for VF). When T-wave oversensingis unmanageable, the only solution may bechanging the device to another brand with morespecific filtering to reject T-waves.
R-wave double-counting, another cause ofinappropriate detection and therapy, can bemanaged by either reprogramming the ventricularblanking period, or by reducing the minimumsensitivity level or, when the other options fail, bylead revision (change of lead position).
Electromagnetic interference (EMI): Thepotential sources of EMI are ubiquitous, especiallyin the hospital (for example, electrocautery, mag-netic resonance imaging, lithotripsy) but also atwork (for example, welding, high voltage powersource, electric motors) and in daily life (forexample, metal detectors, electronic article surveil-lance devices, cellular telephone).9 The mostfrequent responses to EMI are inappropriateinhibition or triggering of pacemaker stimuli andspurious ICD tachycardia detection and inap-propriate therapy. The effects of EMI on pace-makers and ICDs depend on the intensity of theelectromagnetic field, the frequency of the signal,the distance and orientation of the device relativeto the source, device characteristics and patientfactors. Measures have been taken to make ICDsless susceptible—for example, by incorporating afilter. The fear for EMI is high compared to the realclinical problem. In fact, EMI is only rarely a causeof inappropriate shocks.10 The best way to avoidEMI related shocks/device inhibition is to keep asufficient distance from the EMI emitting source.Good advice is essential and, when indicated, afield evaluation may be necessary to identifypossible hazards. However, testing for EMI is not100% conclusive.
Sensing of diaphragmatic potentials infre-quently results in shock delivery. In case ofdiaphragmatic potential sensing, setting the sensi-tivity level at the lowest level can be helpful but, aswith T-wave oversensing, may compromise VFdetection (and appropriate therapy delivery).Therefore, increasing the mandatory detectiontime seems to be more logical advice. If, despitereprogramming, the problem of oversensing dia-phragmatic potentials is unsolvable, lead reposi-tioning may be a reasonable alternative.
Lead/device related problems are frequentand may cause all kind of phenomena. Leadfracture or connector problems give rise to make-break contacts, leading to intermittent high fre-quency signals, sometimes associated with posturalchanges and limited to the sensing electrogram.Impedance may be within normal limits. Shocksmay ensue, often multiple. Isolation defects maylead to oversensing of signals and inappropriatetherapy.
All extracardiac sources of oversensing in pacingdependent patients lead to the additional problemof pacing inhibition. Special noise reduction modesimplemented in modern devices are not alwayshelpful in this respect.
In case of a pace/sense problem, implantation ofan additional pace/sense lead may overcome theseproblems. In case of a structural problem of thelead, lead replacement may become necessary.
How to reduce the number of appropriate shocks?The delivery of appropriate shocks can, in the caseof a VT, be reduced by programming antitachy-cardia pacing (ATP) modes in different zones. ATPhas been shown to be very effective in terminatingventricular arrhythmias, even in the cases of highventricular rates.11 12 Empirical programming (forexample, 8 pulses at 88% of the VT cycle length)
Figure 5 Ventriculartachycardia. Theventricular egrams (lowerchannel) are clearly fasterthan the atrial egrams(middle channel). There isan alternating ventricularcycle length with the cyclelength of each secondcycle falling below the cut-off zone (‘‘VS’’) leading tonon-diagnosis of ventriculartachycardia. Symptoms ofdizziness or syncope maybe the effect.
Education in Heart
656 Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762
on 9 June 2009 heart.bmj.comDownloaded from

without tailoring of the ATP sequences has beenshown to be safe and effective. Therefore, ATPshould be programmed ‘‘on’’, even if its efficacy inthe individual patient has not been assessed yet.
Further reduction of the number of shocks canbe achieved by other measures.13–15 b-blockers,sotalol and amiodarone and other antiarrhythmicdrugs are usually helpful although side effects maylimit their use. Azimilide was shown to be effectivebut is not clinically available yet.16 In general, it isof course important that in ICD patients with alow left ventricular ejection fraction, other drugs
such as angiotensin converting enzyme (ACE)inhibitors and diuretics are given.
In patients with recurrent VTs for which ICDtherapy is delivered, radiofrequency catheter abla-tion may be an effective approach to reduce orabolish the number of VT episodes and ICDdischarges acutely and in the long term. Ifrefractory to other treatment options, surgicalelimination of arrhythmogenic foci may be per-formed usually in combination with other opera-tive goals such as revascularisation, surgicalventricular reconstruction and valvular repair.
How to deal with multiple shocks?The first objective in the management of a patientreceiving multiple shocks is to avoid delivery offurther shocks while conscious. Thus, dependingon the haemodynamic and mental state of thepatient, the heart rhythm and the cause of theshocks, sedation of the patient is usually helpful inachieving stress reduction.
If the patient’s rhythm is supraventricular inorigin, it is sound to switch the ICD off either byusing a programmer or a magnet. The same holdstrue for all non-tachycardia causes of shocks. Ifnecessary, while the ICD is switched off, shockscan still be delivered by the ICD using theemergency button present on the programmers ofall manufacturers or by removing the magnet.
Management of the patient is more difficultwhen the patient’s rhythm is ventricular in originor when recurrent episodes of ventricular arrhyth-mias occur. The shocks are appropriate but at thesame time a disruptive experience for the patient ifconscious. In the acute situation, antiarrhythmicdrug therapy can be effective, such as theintravenous administration of amiodarone orprocainamide. b-blocker treatment has been shownto be valuable as well. When VTs still recur,(manual) overpacing may be helpful. Furthermore,suppression of VT can be achieved in some patientsby increasing the lower rate of the pacemaker.Longer term management includes evaluation andtreatment of the underlying cause, such asworsening heart failure symptoms or ischaemiaor more general causes such as hyperthyroidism ora systemic infection.14 17
DIZZINESS AND SYNCOPEDizziness is a well known, frequently occurring,symptom in patients with an impaired leftventricular function (as in the majority of ICDpatients). Mild heart failure is associated withautonomic derangement, especially weakening ofthe arterial baroreflex sensitivity with permanentactivation of the sympathetic nervous system.Dizziness is often distinct in these patients inwhom the autonomic nervous system is furtheraffected by heart failure medication. History takingis helpful in differentiating this form of dizzinessfrom other causes for dizziness and syncope in ICDpatients (box 1). To reveal a non-arrhythmogenicorigin of dizziness or syncope, interrogation of the
Figure 6 Underdetection of polymorphic ventricular tachycardia due to rarely occurringrapid changes in intrinsic amplitude. The sensitivity level auto-adjusts but not fastenough, resulting in underdetection of intrinsic events; consequently intervals fall in alower zone (‘‘VS’’). Thus, the device is not coming to detection and does not delivertherapy (‘‘divert-reconfirm’’).
Box 2: Events eliciting alerts in ICDs (list notcomplete)
c Battery voltage lowc Prolonged charge timec Magnet applied or in neighbourhoodc Ventricular fibrillation (VF) detection offc VF therapy partially programmedc Electrical reset of systemc Lead impedance out of range
– pacing– high voltage
c Pacing programmed to fixed ratec Intrathoracic impedance change
Education in Heart
Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762 657
on 9 June 2009 heart.bmj.comDownloaded from
device may be helpful as these symptoms may becaused by arrhythmias also. Dizziness or evensyncope may also be caused by underdetection ofventricular arrhythmias. Underdetection mayoccur when there is a variation in cycle lengthduring VT and the cycle length alternates aroundthe cut-off rate of the detection zone (fig 5). Thismay be solved by lowering the cut-off rate. It mayalso be caused by a variation in amplitude of theintracardiac signals as may occur during a poly-morphic VT or VF (fig 6). Committed shockdelivery, still a feature in modern ICDs, may beused to solve this issue. Adjustment of thesensitivity level or shortening of the detectiontime, if possible, may also be helpful to solve theseproblems.
Another reason for dizziness may be theoccurrence of non-sustained VTs that do producesymptoms but do not continue long enough tomeet the programmed detection criteria of thedevice. In the case of non-sustained VT, anti-
arrhythmic drugs may help to lower the number ofepisodes.
Whereas the aforementioned arrhythmias will beapparent at interrogation of the device, a VT witha cycle length below the cut-off rate, unlessongoing during clinical evaluation, is less easilydetectable since the detection criteria have notbeen met and no episodes will be stored. However,clues hidden in the Cardiac flash back (Medtronic)or the Trending (Boston Scientific) (fig 4) help toreveal the arrhythmia. Such relatively slow VTsparticularly occur in patients with jeopardisedmyocardium using amiodarone to treat fasterventricular arrhythmias. Although in general theseproblems can be solved by lowering the cut-offrate, in cases of extremely slow ventriculararrhythmias reprogramming is often not possibledue to overlap with brady pacing settings orbecause the lowest programmable cut-off rate isreached (Boston Scientific 90 beats/min,Medtronic and Biotronik 100 beats/min, St Jude102 beats/min). In that case additional anti-arrhythmic drugs or ablation may be reasonablealternatives.
Rapidly conducted but well-discriminated atrialarrhythmias may cause dizziness as well, particu-larly in patients with reduced left ventricularejection fraction. Drug therapy or His bundleablation may resolve this issue.
Dizziness or even syncope may also occur in theICD patient who is pacemaker dependent whenthe pacemaker is erroneously inhibited. Treatmentis guided by the cause of inhibition (see sectionsabove).
PALPITATIONSAlthough patients do not usually present com-plaining of palpitations in an emergency setting(like those with shocks, dizziness and/or syncope),palpitations are a frequent complaint at regularICD follow-up. Palpitations can be due to severalreasons, overlapping with those causing dizzinessor syncope (box 1). ICD interrogation will givemore insight into the underlying cause since it mayreveal the occurrence of irregular or fast atrialarrhythmias, ventricular extrasystole or non-sus-tained VTs. Sustained VTs with a cycle lengthbelow the cut-off rate are especially difficult todiagnose when the VT is not ongoing duringfollow-up. The already mentioned Trending fea-ture (Boston Scientific) may be helpful in revealingthe arrhythmia. The Flashback memory(Medtronic) stores the egrams preceding an episodeor preceding interrogation. If history is pointing inthis direction, the monitor zone can be adjusted tostore these arrhythmias. Particularly patients withsingle chamber ICDs may complain of palpitationsat rest, at times keeping them from their sleep,caused by lower rate pacing. Decreasing the lowerrate of the pacemaker or lowering the b-blockerdosage may resolve these complaints.
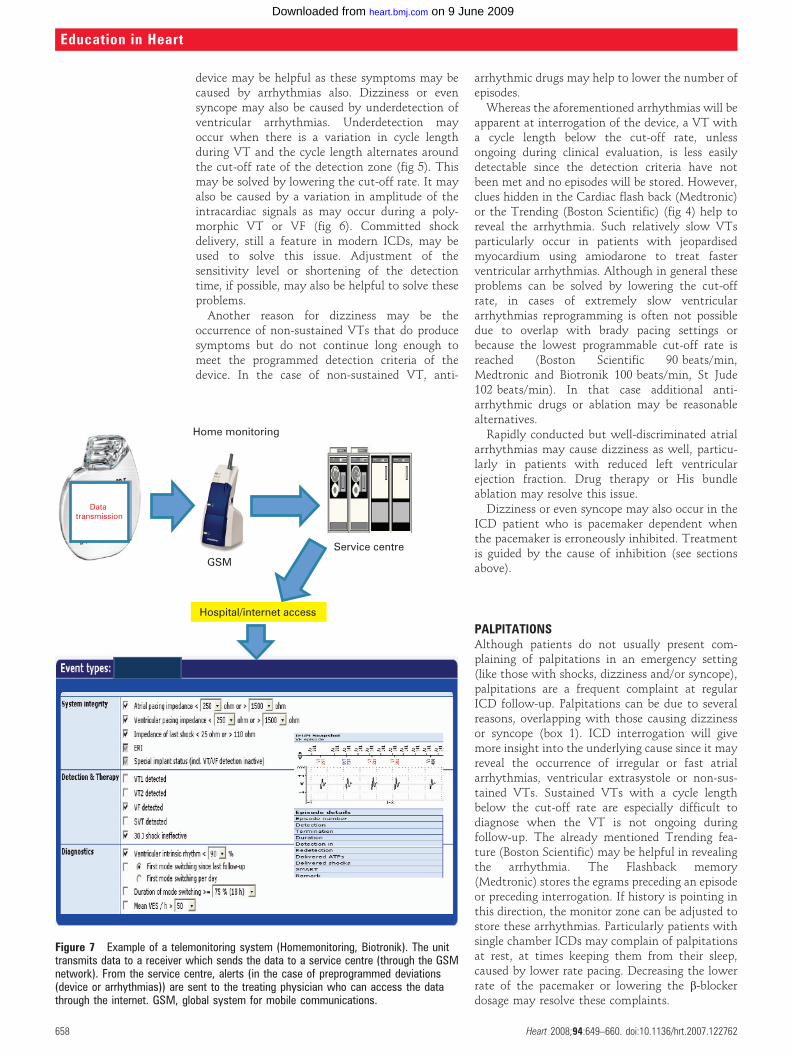
Figure 7 Example of a telemonitoring system (Homemonitoring, Biotronik). The unittransmits data to a receiver which sends the data to a service centre (through the GSMnetwork). From the service centre, alerts (in the case of preprogrammed deviations(device or arrhythmias)) are sent to the treating physician who can access the datathrough the internet. GSM, global system for mobile communications.
Education in Heart
658 Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762
on 9 June 2009 heart.bmj.comDownloaded from

ALERTSMost ICDs have alerts that notify the patient ofundesired settings or electrical events of the ICDand/or leads.18–20 Recently, Medtronic has intro-duced a diagnostic feature intended to predict aforthcoming episode of heart failure (box 2).21 22
The alerts produce audible signals (Medtronic,Boston Scientific) or a vibrational sensation (StJude). Alerts are repetitive, discontinuous signalsthat can be programmed to a specified time. Mostalerts are programmable (on/off), except ‘‘systemalerts’’ that convey debilitated functioning withrespect to proper treatment of tachycardia. Thesystem alerts the patient with the intention thathe/she should contact the physician in case theprogrammed parameters are undesirable or themeasured parameters are not within normal limits.The time and character of the alerts and interval
between alerts inform the physician or technicianabout its cause, without interrogation of thedevice. Instruction may be helpful and relativelyeasy. Although the alerting systems have beenshown to be valuable in many cases, the sensitivityis limited.20 Furthermore, the alerts have an under-estimated distressing effect on patients, whogenerally feel well at the moment of the alert anddo not anticipate being alerted. Instruction doesnot eliminate all of the confusion and inconve-nience coinciding with an alert. Thus, effortsshould be made to avoid false negative alerts, andwhen programming the alerts it is important to beaware of this effect and ensure the patient is wellinformed.
Presently, remote monitoring systems arebecoming available for evaluation of ICD/leadsystems which may replace the necessity of alertsin the future. Monitoring systems allow systemintegrity checks, usually on a daily basis.Furthermore, these systems allow continuousfollowing of the clinical status of the patientwhich may help (in the near future) to preventdeterioration of the clinical status by timelyinterventions. In fig 7, a schematic example ofone of these systems (Home-monitoring,Biotronik, Erlangen, Germany) is given. At thistime all telemonitoring systems provide a one waydataflow (from patient to the hospital) and it isnot possible to program devices using the tele-monitoring system.
PATIENTS WITH A DEVICE OR LEAD UNDER‘‘RECALL’’In recent years a significant number of so-called‘‘dear doctor’’ letters concerning a possible deviceor lead malfunction have been issued by almost alldevice companies. To handle such a situation(depending on the seriousness of the warning)may be a challenging task as, although these lettersdescribe a potentially dangerous situation, theresulting advice to the clinician is not alwaysstraightforward. In the recent past this has resultedin large numbers of devices being replaced world-wide, whereas (in retrospect) it may have beensufficient to intensify follow-up; such large scalereplacements may even have caused serious com-plications.23
To help the clinician, among others, the HeartRhythm Society (HRS) and the European HeartRhythm Association (EHRA) installed device com-mittees which should issue a clinical advice in caseof a device recall.
In general, to deal with such a situation a fewthings are important for every implanting centre:
c Keep track of the device patients implanted atthe centre. An up-to-date patient database willensure patients involved in a recall areinformed quickly. Furthermore an up-to-datedatabase will make it easy to follow theperformance of implanted devices and leads.Preferably a nationwide database should beavailable.
Troubleshooting ICD related problems: key points
c Implantable cardioverter-defibrillator (ICD) troubleshooting starts when apatient presents with a possible device related problem or when technicalfollow-up reveals a possible problem. ICD troubleshooting should beperformed in a structured manner following interrogation of the device andexamining the patient. Important issues include:– complaints of patient related to device activity?– device activity: arrhythmia related or caused by malfunction of device, or
lead (or both) or related to an external source?– device activity: caused by supraventricular or ventricular arrhythmia?– device activity: appropriate or inappropriate?– device activity: adjustment of settings necessary?
c Patients with an ICD related problem present with complaints which generallyfall into one of the following four categories:– shocks (appropriate, inappropriate or failure to deliver therapy)– dizziness/fainting– palpitations– alerts (audible beeps or sensed vibrations originating from the ICD)
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College ofPhysicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). Toaccess the questions, click on BMJ Learning: Take this module on BMJLearning from the content box at the top right and bottom left of the onlinearticle. For more information please go to: http://heart.bmj.com/misc/education.dtlc RCP credits: Log your activity in your CPD diary online (http://www.
rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.c EBAC credits: Print out and retain the BMJ Learning certificate once you have
completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now beconverted to AMA PRA Category 1 CME Credits and are recognised by allNational Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit = men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learningwebsite for medical professionals from the BMJ Group. If prompted, subscribersmust sign into Heart with their journal’s username and password. All users mustalso complete a one-time registration on BMJ Learning and subsequently log in(with a BMJ Learning username and password) on every visit.
Education in Heart
Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762 659
on 9 June 2009 heart.bmj.comDownloaded from

c Follow the initial guidance of the company andadjust according to the final guidance by HRSor EHRA.
c If a patient with a device or lead under recallpresents with problems (for example, shocks)investigate if the problem is related to therecall.
c In the case of an unexpected death of a patient,try to retrieve information from the device toestablish the cause of death.
c Inform the company that a device or leadrelated problem occurred. This is the only wayto obtain a reliable picture.
Competing interests: In compliance with EBAC/EACCMEguidelines, all authors participating in Education in Heart havedisclosed potential conflicts of interest that might cause a biasin the article. Dr Schalij and Dr van Erven received researchgrants from Boston Scientific, Medtronic, and Biotronik. DrSchalij received speaker fees from Boston Scientific andBiotronik. Dr van Erven received speaker fees from BostonScientific and Medtronic.
REFERENCES1. Irvine J, Dorian P, Bakker B, et al. Quality of life in the
Canadian Implantable Defibrillator Study (CIDS). Am Heart J2002;144:282–9.
2. Schron EB, Exner DV, Yao Q, et al for the AVID Investigators.Quality of life in the Antiarrhythmics Versus ImplantableDefibrillator trial: impact of therapy and influence of adversesymptoms and defibrillator shocks. Circulation 2002;105:589–94.
c These are two large studies in which the quality of life wasassessed after ICD implant with a follow-up of more than ayear. The occurrence of ICD shocks was associated withdecreased mental wellbeing and increased patientconcerns.
3. Dorian P, Philippon F, Thibault B, et al for the ASTRIDInvestigators. Randomized controlled study of detectionenhancements versus rate-only detection to prevent inappropriatetherapy in a dual-chamber implantable cardioverter-defibrillator.Heart Rhythm 2004;1:540–7.
4. Theuns DA, Rivero-Ayerza M, Boersma E, et al. Prevention ofinappropriate therapy in implantable defibrillators: a meta-analysisof clinical trials comparing single-chamber and dual-chamberarrhythmia discrimination algorithms. Int J Cardiol 2007 April 17[Epub ahead of print].
5. Friedman PA, McClelland RL, Bamlet WR, et al. Dual-chamberversus single-chamber detection enhancements for implantabledefibrillator rhythm diagnosis. The Detect SupraventricularTachycardia study. Circulation 2006;113:2871–9.
c Three papers giving more insight into discrimination of SVTvs VT in single and dual chamber ICDs.
6. Rauwolf T, Guenther M, Hass N, et al. Ventricular oversensing in518 patients with implanted cardiac defibrillators: incidence,complications and solutions. Europace 2007;9:1041–7.
c This retrospective study describes the causes of andsolutions for oversensing by the ICD in a relatively largepatient group, leading to ICD interpreted arrhythmias.
7. Nanthakumar K, Dorian P, Paquette M, et al. Is inappropriateimplantable defibrillator shock therapy predictable? J Interv CardElectrophys 2003;8:215–20.
c This is an interesting article on the predictability of shocks.New York Heart Association functional class I and prioratrial fibrillation predicted the occurrence of inappropriateshock.
8. Sacher F, Probst V, Iesaka Y, et al. Outcome after implantation ofa cardioverter-defibrillator in patients with Brugada syndrome. Amulticenter study. Circulation 2006;114:2317–24.
9. Pinski SL. Electromagnetic interference and implantable devices.In: Ellenbogen, Kay, Lau, Wilkoff, eds. Clinical cardiac pacing,defibrillation, and resynchronization therapy. Saunders, 2007:1149–76.
c This book chapter provides a good and balanced overviewof the nature and sources of electromagnetic interferencewith ICDs and of the measures that can be taken withpatients exposed to it.
10. Kolb C, Zrenner B, Schmitt C. Incidence of electromagneticinterference in implantable cardioverter-defibrillators. PACE2001;24:465–71.
11. Wilkoff BL, Ousdigian KT, Sterns LD, et al. A comparison ofempiric to physician-tailored programming of implantablecardioverter-defibrillators: result from the prospectiverandomized multicenter EMPIRIC trial. J Am Coll Cardiol2006;48:330–9.
12. Wathen M. Implantable cardioverter defibrillator shock reductionusing new antitachycardia pacing therapies. Am Heart J2007;153:S44–52.
c Standard programming of ATP was shown to reduce thenumber of appropriate shocks. This reference gives asummary of the two ‘‘painfree’’ trials in which this has beenclearly proven. ATP before shock in the VF zone is beingincorporated as a default programming in current ICDs.
13. Ferreira-Gonzalez I, Dos-Subira L, Guyatt H. Adjunctiveantiarrhythmic drug therapy in patients with implantablecardioverter defibrillators: a systematic review. Eur Heart J2007;28:469–77.
14. Della Bella P, Riva S. Hybrid therapies for ventricular arrhythmias.PACE 2006;29:S40–7.
15. Doenst T, Faerber G, Grandinac S, et al. Surgicaltherapy of ventricular arrhythmias. Herzschr Elektrophys2007;18:62–7.
c Three overview papers on adjunctive therapies in ICDpatients: antiarrhythmic drug therapy, ablation ofventricular arrhythmias, and surgical therapy.
16. Singer I, Al-Khalidi H, Niazi I, et al. Azimilide decreasesrecurrent ventricular tachyarrhythmias in patients withimplantable cardioverter defibrillators. J Am Coll Cardiol2004;43:39–43.
17. Tandri H, Griffith LS, Tang T, et al. Clinical course and long-termfollow-up of patients receiving implantable cardioverter-defibrillators. Heart Rhythm 2006;3:762–8.
18. Becker R, Rug-Richter J, Senges-Becker JC, et al. Patient alert inimplantable cardioverter defibrillators: toy or tool? J Am Coll Cardiol2004;44:95–8.
19. Duru F, Luechinger R, Scharf C, et al. Automatic impedancemonitoring and patient alert feature in implantable cardioverterdefibrillator: being alert for the unexpected. J CardiovascElectrophysiol 2005;16:444–8.
20. Vollman D, Erdogan A, Himmrich E, et al for the SAFE StudyInvestigators. Patient alert to detect ICD lead failure: efficacy,limitations and implication for future algorithms. Europace2006;8:371–6.
21. Vollmann D, Nagele H, Scheuerte P, et al for the European InSyncSentry Observational Study Investigators. Clinical utility ofintrathoracic impedance monitoring to alert patients with animplanted device of deteriorating chronic heart failure. Eur Heart J2007;28:1835–40.
c The largest study so far evaluating the predictive value of adiagnostic feature like intrathoracic impedance fordecompensated heart failure implemented in one type ofCRT-D device.
22. Ypenburg C, Bax JJ, van der Wall EE, et al. Intrathoracicimpedance monitoring to predict decompensated heart failure.Am J Cardiol 2007;99:554–7.
c Complications associated the device replacement.23. Gould PA, Krahn AD, Canadian Heart Rhythm Society Working
Group on Device Advisories. Complications associated withimplantable cardioverter-defibrillator replacement in response todevice advisories. JAMA;2006:295:1907–11.
Education in Heart
660 Heart 2008;94:649–660. doi:10.1136/hrt.2007.122762
on 9 June 2009 heart.bmj.comDownloaded from


















