Trigeminal neuralgia (tic douloureux) painful twitch CT guided interventional treatment Jalal Jalal...
46
Trigeminal neuralgia (tic douloureux) painful twitch CT guided interventional treatment Jalal Jalal Shokouhi- MD ISR Iran Shahyar Pashaie-MD Tehran. Uni. Iran Mohammad hossein Herischi Baku Republic Azerbaijan [email protected] www.medimage.ir www.neurocongress.com
-
Upload
conrad-brown -
Category
Documents
-
view
238 -
download
0
Transcript of Trigeminal neuralgia (tic douloureux) painful twitch CT guided interventional treatment Jalal Jalal...

Trigeminal neuralgia (tic douloureux) painful twitch
CT guided interventional treatment
Jalal Jalal Shokouhi- MD ISR IranShahyar Pashaie-MD Tehran. Uni. IranMohammad hossein Herischi Baku Republic Azerbaijan
www.neurocongress.com

TRIGEMINAL NEURLAGIA

Trigeminal NeuralgiaWhat is it?
Fifth cranial nerve pain in the cheek, lips, gums or chin on the one side

Function:ChewingSalivaTearsFacial sensations

Topogram:
Ophtalmic branch: around eyes and forhead
Maxillary branch: lips, nose, cheek
Mandibular branch: tongue, lower lip

TGN-Historical perspective
• Fallopius : documented the trigeminal nerve in the 16th
century in an anatomical study
• John Locke : American physician in Paris – gave a full detailed
description of TGN. The patient was the Countess of
Northumberland, wife of British Ambassador to the
French Court.
• Nicolas Andre : called the clinical entity ‘Tic douloureaux’ in 1756
describing 5 patients who suffered from a :
‘cruel and obscure illness which causes in the face some violent motions, some
hideous grimaces, which are an insurmountable obstacle to the reception of
food, which put off sleep’
• Fothergill’s disease : after eponymous London Physician in 1776.
• Trousseau : 1853 suggested that the paroxysmal nature of TGN was due to
abnormal conduction and called it ‘neuralgia epileptiform’
TGN : Clinical features• Female > Male• Incidence : 4.3 / 100,000• Age group : 50 - 60 years• Paroxysmal recurrent pain of short duration• Trigger point(s), allodynia• Periods of remission• Recurrent episodes of pain with progressively shorter
periods ofremission• Distribution of pain :– localised to Trigeminal nerve– 80% Maxillary / Mandibular combination– Right side > Left side• Clinical examination : Usually normal
TGN-Differential diagnosis• Dental / Sinus related pain• Cluster headache / Migrainous neuralgia• Atypical facial pain• Post - herpetic neuropathy• TM joint dysfunction– Degenerative , Rheumatoid arthritis• Trigeminal neuropathy– Demyelination : Multiple sclerosis• Facial myalgia

Trigeminal NeuralgiaWhat causes it

Pathophysiology• Compression at root exit zone : at junction of central myelin(oligodendroglial cells) and peripheral myelin (Schwann
cells) : theObersteiner-Redlich line– Vascular cross compression of Root Exit Zone• Atherosclerotic degeneration causing elongation and
tortuosity– Neoplastic compression• Meningioma, Schwannoma, Neuroma, Epidermoid• Focal segmental axonal demyelination with abberantsynaptogenesis resulting in transaxonal ephaptic transmission• Spontaneous discharge occur at site of compression• Evoked potentials studies demonstrate increased latency &
thresholdconsistent with nerve compression

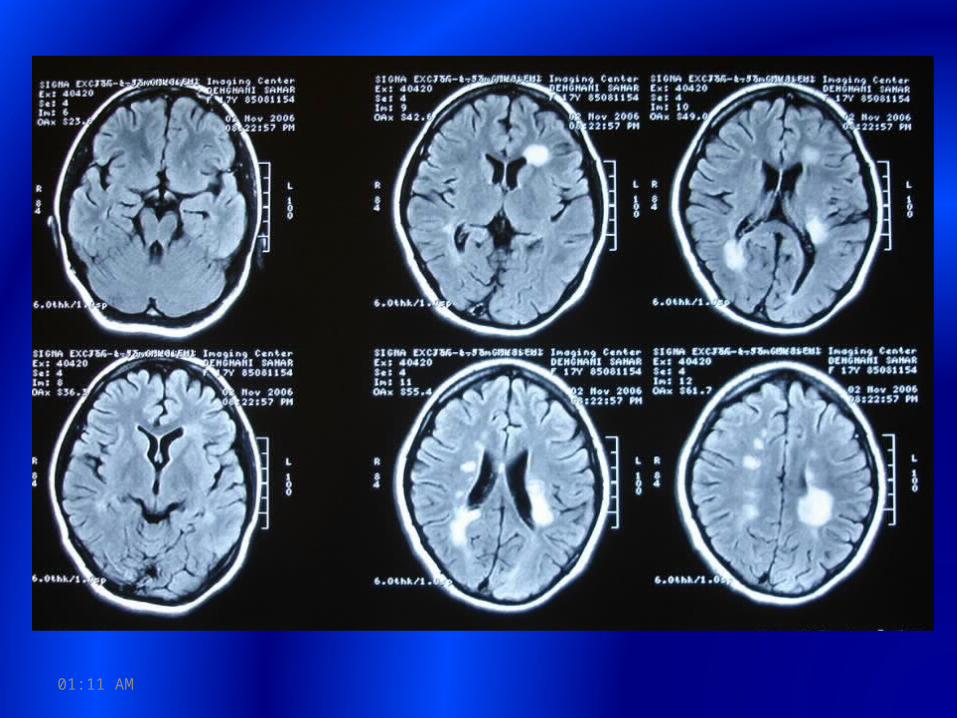
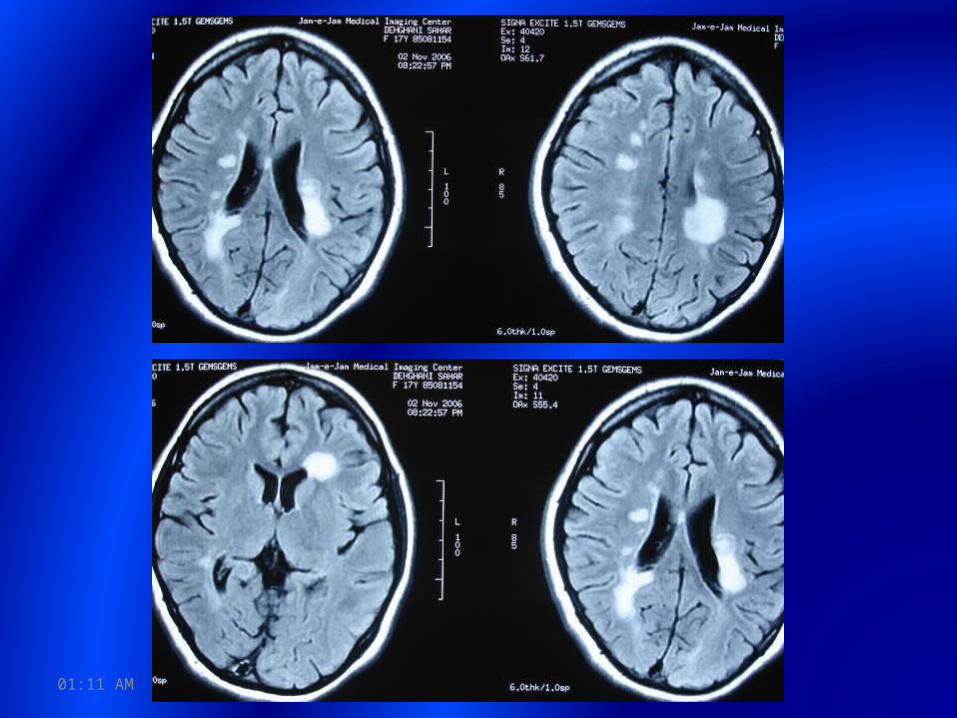
Pathophysiology• Association between multiple sclerosis anddemyelination– 4% of patients with MS have TGN• Harris 1950 Rare forms of paroxysmal
trigeminal neuralgiaand their relation to disseminated sclerosis BMJ
2 1015 - 1019– 2% of patients with TGN have MS



Treatments:1. Drug: antiepileptic: carbamazepine or
tegretol,phenytoin or dilantin


Treatments:1. Drug: antiepileptic: carbamazepine or
tegretol,phenytoin or dilantin2. Surgery of tumor or vascular decompression,
microendoscopy (2.7mm)





Treatments:1. Drug: antiepileptic: carbamazepine or
tegretol,phenytoin or dilantin2. Surgery of tumor or vascular decompression,
microendoscopy (2.7mm)3. Radio surgery(γ-knife,RF)

Treatments:1. Drug: antiepileptic: carbamazepine or
tegretol,phenytoin or dilantin2. Surgery of tumor or vascular decompression,
microendoscopy (2.7mm)3. Radio surgery(γ-knife,RF)4. Interventional radiology: glycerol, ethanol,
RFA









63 patients13 Female50 Male
33 Idiopathic (dental operations)??16 M.S14 ?

Techniques and drugs:Needle G22Spiral CT guidanceLocal anesthesia (marcaine, pubivicaine 6-8-10cc)Iodine 0.5 ccEthanol 65-95% 2-3cc
11:27 AM
11:27 AM

11:27 AM

Nerve blockage, if there is no organic lesion in meckle cave, cavernous sinus and parasellar, also mandibular nerve branch
11:27 AM

M.S and Pain:
53 to 82%
Acute: Neuropathic in acute phase
Chronic: 90% Neuropathic or musculoskeletal
11:27 AM
Site of lesions:
Trigeminal entry zone in brain stem: Tri. G. Neuralgia
Brain stem, spinal cord: muscle spasm, pain full cramp
Corticospinal, Corticobulbar, Spasticity, LBP, extremity
pain
11:27 AM

11:27 AM

11:27 AM

11:27 AM

11:27 AM

Results:All patients: pain free immediately after
injection• Repeat injection: 2-3
11:27 AM

Take home message:
M.S. has diplopia, parestesia, paralysis, vertigo,... Also MS has pain.
11:27 AM

Thank youAny Question?