Triangle Physician
32
MAY 2011 THE MAGAZINE FOR HEALTHCARE PROFESSIONALS Also in is Issue LASIK in the Military Image-guided Pain Relief Cary Orthopaedic & Sports Medicine Thrives on a Tradition of Excellence
-
Upload
dr-dean-dornic -
Category
Documents
-
view
261 -
download
2
Transcript of Triangle Physician

m a y 2 0 11
T H E M A G A Z I N E
F O R H E A L T H C A R E
P R O F E S S I O N A L S
Also in This IssueLASIK in the Military
Image-guided Pain Relief
Cary Orthopaedic & Sports Medicine
Thrives on a Tradition of Excellence

FDA-Approved for MRI Use
www.medtronic.com
The Revo MRI SureScan pacing system is MR Conditional designed to allow patients to undergo MRI under the specified conditions for use. A complete system, consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan leads is required for use in the MRI environment.
www.medtronic.com
World HeadquartersMedtronic, Inc. 710 Medtronic ParkwayMinneapolis, MN 55432-5604USATel: (763) 514-4000 Fax: (763) 514-4879
Medtronic USA, Inc. Toll-free: 1 (800) 328-2518(24-hour technical support for physicians and medical professionals)
Patient Line:Tel: 1 (800) 551-55447:00 am to 6:00 pm CT M-FFax: (763) 514-185524-hour information available on www.medtronic.com
UC2
0100
4100
EN
© M
edtr
onic
, Inc
. 201
1. M
inne
apol
is, M
N. A
ll Ri
ghts
Res
erve
d. P
rinte
d in
USA
. 02/
2011
Brief Statement The Revo MRI™ SureScan® pacing system is MR Conditional and as such is designed to allow patients to undergo MRI under the specified conditions for use.
IndicationsThe Revo MRI SureScan Model RVDR01 IPG is indicated for use as a system consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan 5086MRI leads. A complete system is required for use in the MRI environment.The Revo MRI SureScan Model RVDR01 IPG is indicated for the following:• Rate adaptive pacing in patients who may benefit from increased pacing
rates concurrent with increases in activity• Accepted patient conditions warranting chronic cardiac pacing include: – Symptomatic paroxysmal or permanent second- or third-degree AV
block – Symptomatic bilateral bundle branch block – Symptomatic paroxysmal or transient sinus node dysfunctions with or
without associated AV conduction disorders – Bradycardia-tachycardia syndrome to prevent symptomatic bradycardia
or some forms of symptomatic tachyarrhythmias
The device is also indicated for dual chamber and atrial tracking modes in patients who may benefit from maintenance of AV synchrony. Dual chamber modes are specifically indicated for treatment of conduction disorders that require restoration of both rate and AV synchrony, which include:• Various degrees of AV block to maintain the atrial contribution to cardiac output
• VVI intolerance (for example, pacemaker syndrome) in the presence of persistent sinus rhythm
Antitachycardia pacing (ATP) is indicated for termination of atrial tachyarrhythmias in bradycardia patients with one or more of the above pacing indications.
Atrial rhythm management features such as Atrial Rate Stabilization (ARS), Atrial Preference Pacing (APP), and Post Mode Switch Overdrive Pacing (PMOP) are indicated for the suppression of atrial tachyarrhythmias in bradycardia patients with atrial septal lead placement and one or more of the above pacing indications.The device has been designed for the MRI environment when used with the specified MR Conditions of Use.
ContraindicationsThe device is contraindicated for:• Implantation with unipolar pacing leads• Concomitant implantation with another bradycardia device• Concomitant implantation with an implantable cardioverter defibrillatorThere are no known contraindications for the use of pacing as a therapeutic modality to control heart rate. The patient’s age and medical condition, however, may dictate the particular pacing system, mode of operation, and implantation procedure used by the physician.• Rate responsive modes may be contraindicated in those patients who
cannot tolerate pacing rates above the programmed Lower Rate• Dual chamber sequential pacing is contraindicated in patients with
chronic or persistent supraventricular tachycardias, including atrial fibrillation or flutter
• Single chamber atrial pacing is contraindicated in patients with an AV conduction disturbance
• ATP therapy is contraindicated in patients with an accessory antegrade pathway
Warnings and PrecautionsChanges in a patient’s disease and/or medications may alter the efficacy of the device’s programmed parameters. Patients should avoid sources of magnetic and electromagnetic radiation to avoid possible underdetection, inappropriate sensing and/or therapy delivery, tissue damage, induction of an arrhythmia, device electrical reset, or device damage. Do not place transthoracic defibrillation paddles directly over the device. Use of the device should not change the application of established anticoagulation protocols.
Do not scan the following patients:• Patients who do not have a complete Revo MRI SureScan pacing system,
consisting of a SureScan device and two SureScan leads• Patients who have previously implanted devices, or broken or
intermittent leads• Patients who have a lead impedance value of < 200 Ω or > 1,500 Ω• Patients with a Revo MRI SureScan pacing system implanted in sites
other than the left and right pectoral region • Patients positioned such that the isocenter (center of MRI bore) is inferior
to C1 vertebra and superior to the T12 vertebra
See the device manuals before performing an MRI Scan for detailed information regarding the implant procedure, indications, MRI conditions of use, contraindications, warnings, precautions, and potential complications/adverse events. For further information, call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
The First and Only Pacing System to Break the Image Barrier
Introducing the Revo MRITM Pacing System engineered with SureScan® Technology – the only pacing system to provide proven cardiac care that’s designed to be used safely with MRI.
201004100_RevoAd_8.25x11_1-pager.indd 1 3/2/11 3:33 PM

FDA-Approved for MRI Use
www.medtronic.com
The Revo MRI SureScan pacing system is MR Conditional designed to allow patients to undergo MRI under the specified conditions for use. A complete system, consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan leads is required for use in the MRI environment.
www.medtronic.com
World HeadquartersMedtronic, Inc. 710 Medtronic ParkwayMinneapolis, MN 55432-5604USATel: (763) 514-4000 Fax: (763) 514-4879
Medtronic USA, Inc. Toll-free: 1 (800) 328-2518(24-hour technical support for physicians and medical professionals)
Patient Line:Tel: 1 (800) 551-55447:00 am to 6:00 pm CT M-FFax: (763) 514-185524-hour information available on www.medtronic.com
UC2
0100
4100
EN
© M
edtr
onic
, Inc
. 201
1. M
inne
apol
is, M
N. A
ll Ri
ghts
Res
erve
d. P
rinte
d in
USA
. 02/
2011
Brief Statement The Revo MRI™ SureScan® pacing system is MR Conditional and as such is designed to allow patients to undergo MRI under the specified conditions for use.
IndicationsThe Revo MRI SureScan Model RVDR01 IPG is indicated for use as a system consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan 5086MRI leads. A complete system is required for use in the MRI environment.The Revo MRI SureScan Model RVDR01 IPG is indicated for the following:• Rate adaptive pacing in patients who may benefit from increased pacing
rates concurrent with increases in activity• Accepted patient conditions warranting chronic cardiac pacing include: – Symptomatic paroxysmal or permanent second- or third-degree AV
block – Symptomatic bilateral bundle branch block – Symptomatic paroxysmal or transient sinus node dysfunctions with or
without associated AV conduction disorders – Bradycardia-tachycardia syndrome to prevent symptomatic bradycardia
or some forms of symptomatic tachyarrhythmias
The device is also indicated for dual chamber and atrial tracking modes in patients who may benefit from maintenance of AV synchrony. Dual chamber modes are specifically indicated for treatment of conduction disorders that require restoration of both rate and AV synchrony, which include:• Various degrees of AV block to maintain the atrial contribution to cardiac output
• VVI intolerance (for example, pacemaker syndrome) in the presence of persistent sinus rhythm
Antitachycardia pacing (ATP) is indicated for termination of atrial tachyarrhythmias in bradycardia patients with one or more of the above pacing indications.
Atrial rhythm management features such as Atrial Rate Stabilization (ARS), Atrial Preference Pacing (APP), and Post Mode Switch Overdrive Pacing (PMOP) are indicated for the suppression of atrial tachyarrhythmias in bradycardia patients with atrial septal lead placement and one or more of the above pacing indications.The device has been designed for the MRI environment when used with the specified MR Conditions of Use.
ContraindicationsThe device is contraindicated for:• Implantation with unipolar pacing leads• Concomitant implantation with another bradycardia device• Concomitant implantation with an implantable cardioverter defibrillatorThere are no known contraindications for the use of pacing as a therapeutic modality to control heart rate. The patient’s age and medical condition, however, may dictate the particular pacing system, mode of operation, and implantation procedure used by the physician.• Rate responsive modes may be contraindicated in those patients who
cannot tolerate pacing rates above the programmed Lower Rate• Dual chamber sequential pacing is contraindicated in patients with
chronic or persistent supraventricular tachycardias, including atrial fibrillation or flutter
• Single chamber atrial pacing is contraindicated in patients with an AV conduction disturbance
• ATP therapy is contraindicated in patients with an accessory antegrade pathway
Warnings and PrecautionsChanges in a patient’s disease and/or medications may alter the efficacy of the device’s programmed parameters. Patients should avoid sources of magnetic and electromagnetic radiation to avoid possible underdetection, inappropriate sensing and/or therapy delivery, tissue damage, induction of an arrhythmia, device electrical reset, or device damage. Do not place transthoracic defibrillation paddles directly over the device. Use of the device should not change the application of established anticoagulation protocols.
Do not scan the following patients:• Patients who do not have a complete Revo MRI SureScan pacing system,
consisting of a SureScan device and two SureScan leads• Patients who have previously implanted devices, or broken or
intermittent leads• Patients who have a lead impedance value of < 200 Ω or > 1,500 Ω• Patients with a Revo MRI SureScan pacing system implanted in sites
other than the left and right pectoral region • Patients positioned such that the isocenter (center of MRI bore) is inferior
to C1 vertebra and superior to the T12 vertebra
See the device manuals before performing an MRI Scan for detailed information regarding the implant procedure, indications, MRI conditions of use, contraindications, warnings, precautions, and potential complications/adverse events. For further information, call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
The First and Only Pacing System to Break the Image Barrier
Introducing the Revo MRITM Pacing System engineered with SureScan® Technology – the only pacing system to provide proven cardiac care that’s designed to be used safely with MRI.
201004100_RevoAd_8.25x11_1-pager.indd 1 3/2/11 3:33 PM
After a disabling illness or injury, all you want to do is get back to your life—as quickly as possible.
Durham Rehabilitation Institute at Durham Regional Hospital helps you regain your independence with care delivered in a warm, compassionate environment.
Durham Rehabilitation Institute is an award-winning facility that provides comprehensive, state-of-the-art care. Treatment programs
are led by a board-certified rehabilitation physician. Other team members include nurse practitioners, rehabilitation nurses, physical therapists, speech therapists, and others dedicated to providing personalized care to meet each patient’s needs.
Top-rated rehabilitation care with the convenience of a community hospital: this is Durham Regional Hospital.
We help you get back to your life
durhamregional.org
8114
For physician referrals, call 919-470-7226.

2 The Triangle Physician
Contents
COVER STORY
DEPARTMENTS11 Orthopedics
Total Ankle Replacement Is Revolu-tionizing Care of Ankle Arthritis
12 Your Financial Rx Reduce Your Investment Pain Threshold
14 Sleep Medicine Sleep Apnea Requires Specialized Attention
16 Orthopedics Double Bundle Technique Improves Anterior Cruciate Ligament Outcomes
18 Cardiology Atrial Fibrillation: A Perspective on Treatment Evolution
22 Women’s Health New Findings in Losing Weight
24 WakeMed News County’s fifth hospital, new Brier Creek Healthplex and more
26 GHS News Distinction for knee and hip replace-ment, and Hospital of Choice Award
27 Durham Regional News U.S. News Best Hospital ranking
27 News Upcoming events, welcome, new offices and clinical trials
FEATURES
6V o l . 2 , I s s u e 5m a y 2 0 1 1
Cary Orthopaedic & Sports Medicine Thrives on a Tradition of Excellence
21Radiology
10LASIK Advances Benefit the Military
Dr. Dean Dornic explains how the military
has embraced advances in laser-assisted in
situ keratomileus.
Ophthalmology
Raleigh Radiology’s Musculoskeletal Team Offers Image-Guided Pain Management
Dr. Jeffrey Browne gives an overview of the
pain management uses and methods of
image-guided injections.
JOHNSTONHEALTH

4 The Triangle Physician
From the Editor
T H E M A G A Z I N E
F O R H E A L T H C A R E
P R O F E S S I O N A L S
EditorHeidi Ketler, APR [email protected]
Contributing EditorsKer Boyce, M.D., F.A.C.C., F.A.C.P. Jeffrey Browne, M.D Giridhar Chintalapudi, M.D. Dean Dornic, M.D. Mark Galland, M.D. Andrea S. Lukes, M.D., M.H.Sc., F.A.C.O.G Selene G. Parekh, M.D., M.B.A. Paul Pittman, C.F.P.
PhotographyJim Shaw Photography [email protected]
Creative DirectorJoseph Dally [email protected]
Advertising Sales Carolyn Walters [email protected]
News and ColumnsPlease send to [email protected]
The Triangle Physician is published byNew Dally Design9611 Ravenscroft Ln NW, Concord, NC 28027
Subscription Rates:$48.00 per year$6.95 per issue
Advertising rates on requestBulk rate postage paid Greensboro, NC 27401
Every precaution is taken to insure the accuracy of the articles published. The Triangle Physician can not be held responsible for the opinions expressed or facts supplied by its authors.
Opinion expressed or facts supplied by its authors are not the responsibility of The Triangle Physician. However, The Triangle Physician makes no warrant to the accuracy or reliability of this information.
All advertiser and manufacturer supplied photog-raphy will receive no compensation for the use of submitted photography.
Any copyrights are waived by the advertiser.
No part of this publication can be reproduced or transmitted in any form or by any means without the written permission from The Triangle Physician.
Spring into Health
It’s spring, a time to sweep out the cobwebs, which for many means self reflection about
our health and lifestyle.
Outdoor activity ramps up and body mechanics become a focus. Watching our back
and every part of our musculoskeletal being in times of injury are orthopedic specialists
and physical therapists, such as those at Cary Orthopaedic Sports Medicine and Spine
Specialists. This finely tuned team is standing by to provide early and proper diagnosis
so patients can get back to the games of life faster, more fully and with less pain.
Weight management increases in importance as the weather warms. Overweight
and obesity comprise a national problem. Its toll on human life weighs heavy on the
economy. And despite all the marvels of modern medicine, data suggests overweight
and obesity are increasing. A beacon of hope is the Medi-Weightloss Clinic. Its regimen
that includes ongoing counseling and medical supervision is possibly the surest,
healthiest approach to long-term weight management.
Also on the orthopedic front, Dr. Mark Galland reviews how a new double-bundle surgical
technique improves anterior cruciate ligament outcomes. Dr. Selene Parekh focuses on the
improvements in total ankle replacement in the treatment of ankle arthritis.
Dr. Andrea Lukes enters the weight management discussion with an overview of the use
of phentermine to suppress appetite.
In this issue we get several points of view on pain management. Certified financial
planner Paul Pittman talks about avoiding the very real pain felt when investment returns
are poor. Dr. Jeffrey Browne explains image-guided pain management.
The Triangle Physician welcomes two new contributors. Dr. Dean Dornic writes about
the benefits of laser-assisted in situ keratomileus (LASIK) surgery to the military. Dr.
Giridhar Chintalapudi (aka Dr. Chin) reviews the diagnosis and treatment of sleep apnea.
Spring also is a great time to evaluate your practice marketing strategies. If you haven’t
done so already, incorporating The Triangle Physician into the mix makes a lot of sense.
Consider that it is the only publication of its kind, dedicated to the Triangle medical
profession.
Our sincere gratitude for all you do. Happy spring!
Heidi KetlerEditor

6 The Triangle Physician
On the Cover
Known as a hotbed of athletic activity, the
Greater Raleigh and Triangle region experi-
ences its share of sports-related injuries. For
29 years Cary Orthopaedic & Sports Medi-
cine Specialists has been filling the need for
high quality diagnosis and treatment of these
injuries and many other orthopaedic related
conditions.
Since opening its doors in 1982, Cary Or-
thopaedic has grown with the community
to offer a comprehensive range of surgical,
non-surgical and rehabilitative services. The
practice is comprised of a team of orthopae-
dic sports medicine and spine-specialized
surgeons, physiatrists and physical thera-
pists at three separate locations.
All nine orthopedic surgeons are fellowship
trained. In addition to general orthopedics
and sports medicine, the range of specializa-
tion includes arthroscopic and reconstruc-
tive surgery, total joint replacement and
minimally invasive spine surgery.
Cary Orthopaedic Sports Medicine and
Spine Specialists is distinguished by its tradi-
tion of excellence that ensures every initial
patient encounter begins with an orthopae-
dic physician evaluation. “A hallmark of this
practice is continually striving to provide
early and proper diagnosis which can help
prevent prolonged difficulties and provide
the greatest value for the health care dollar
spent,” says Michael Mazzella, Cary Ortho-
paedic Chief Operating Officer.
The practice now encompasses Cary Ortho-
paedic Spine Specialists, offering a total ap-
proach to spine care. Garner Orthopaedic
Sports Medicine & Spine Specialists pro-
vides a similar offering to that community
and surrounding counties. All three ortho-
paedic locations have a dedicated Perfor-
mance Physical Therapy facility on site.
Teamwork a Practice Hallmark
“Excellence in Sports medicine and Ortho-
pedics requires that we’re all on the same
page to meet patient goals as quickly and
safely as possible,” says Douglas L. Golle-
hon, M.D., senior partner. “To ensure the
very best outcome ideally we involve the
physician, parents, the athletic trainer and
coach as part of the team focused on return-
ing that athlete back to the desired level of
activity. “
Sports Medicine Expertise
Over the years, Cary Orthopaedic Sports
Medicine and Spine Specialists services to
patients has represented the Triangle’s wide
world of sports, from the Carolina Hurri-
canes, Carolina RailHawks and Carolina Bal-
let to scholastic athletes, recreational week-
end warriors and elite triathletes.
“This is a very diverse athletic market, not
just for professional sports,” says Susan
McArdle, Cary Orthopaedic Business Man-
ager. “We see everything from acute injuries
to arthritis that may be manifested in the
older recreational athlete.”
Patients seek out Cary Orthopaedic Sports
Medicine and Spine Specialists for the lev-
Cary Orthopaedic & Sports Medicine Thrives on a Tradition of Excellence
Dr. andersen provides diagnosis and treatment of an injured wrist
PHO
TO B
Y B
RYA
N R
EGA
N P
HO
TOG
RA
PHY
By Heidi Ketler

MAY 2011 7
el of care that provides enhanced freedom
of movement without pain for all types of
musculoskeletal problems. “Our patient’s
goals can be as diverse as walking down
the driveway to get the newspaper to the
highest level of training to qualify for a ca-
reer in professional athletics,” says Doug-
las J. Martini, M.D. “Even if a patient is not
a high-level athlete or a recreational or
scholastic athlete, we treat them all with
the same high level of expertise and ex-
pectation.”
Knee ligament
reconstructive surgery
Injury to the anterior cruciate ligament, or
ACL, is common among the high-level ath-
letes and the recreationally active popula-
tion. This ligament serves as the primary
restraint to forward and pivoting motion of
the shin bone. An ACL tear can be a debili-
tating sports injury.
With the appropriate diagnosis and treat-
ment approach, “the prognosis for recov-
ery is excellent,” says William K. Andersen,
M.D. Surgical reconstruction of a torn ACL
is usually recommended for patients who
are less than 25 years old, regardless of ac-
tivity level, because they tend to have prob-
lems with instability and frequent episodes
of the knee giving way. Given the advances
in ACL reconstruction and the accelerated
approach to rehabilitation, this surgical pro-
cedure is often recommended to a wider
active patient population than in the past.
Preoperatively, “it is important to regain mo-
tion in the knee as soon as possible after
injury to prevent stiffness and secondary
problems,” says Dr. Andersen. “Resolution
of swelling and stiffness prior to ACL recon-
struction surgery improves post-operative
joint function.”
A torn ACL must be entirely removed and a
new one reconstructed. The new ligament
is positioned within the knee with screws
or other fixation devices. The reconstructed
ligament then has to heal in this position in
order to withstand the repetitive stresses of
sports activities.
Most orthopaedists recommend a minimum
of six months of progressive physical ther-
apy before returning to competitive sports.
ACL rehabilitation involves a progression of
therapeutic and sport-specific activities. The
experienced physical therapist makes the
best determination as to whether or not the
patient is able to safely progress.
Approach to Arthritic Joints
Osteoarthritis is a common, progressive and
debilitating disease that occurs commonly
at the knee, hip and shoulder. The first line
of treatment for osteoarthritis aims to relieve
pain with nonsteroidal anti-inflammatory
drugs, along with physical therapy, applica-
tions of a topical analgesic and injections of
a corticosteroid.
Viscosupplementation is commonly used
to treat chronic osteoarthritis of the knee if
conservative treatments fail. It involves the
injection of gel-like substances (hyaluro-
nates) into the knee joint to supplement the
viscous properties of synovial fluid. The pa-
tient will receive three to five injections over
the course of several weeks. Positive effects
can last several months.
Shoulder Injuries and Treatment
A rotator cuff injury may result from a trau-
matic event or develop gradually with repeti-
tive overhead activities. “Those susceptible
to overuse-related problems are athletes
who engage in repetitive overhead arm
movements, like throwing. Degenerative
changes in the shoulder may contribute to
the problem in active older adults,” says Ray-
mond M. Carroll, M.D.
Most patients experience pain relief and im-
proved shoulder function through non-sur-
gical treatment, including anti-inflammatory
medicine and strengthening exercises. Sur-
gery may be considered if a rotator cuff tear
is acute and painful, if it is in the dominant
arm of the active individual or if maximum
overhead arm strength is required for work
or sports.
Dr. armour performs specific orthopaedic maneuvers to assess the extent of a knee injury
Dr. Carroll evaluates for a rotator cuff injury

8 The Triangle Physician
Proactive Approach to Recovery
Cary Orthopaedic & Sports Medicine
Specialists’ rehabilitation service, PER-
FORMANCE Physical Therapy, provides
highly trained and experienced physical
therapists to guide patients through “pre-
habilitation” in the weeks leading up to
surgery.
Pain and loss of strength and function can
spiral preoperatively and can prolong a
successful post-operative outcome. The
goal of physical therapy preoperatively is
to regain the patient’s range of motion, re-
duce pain and swelling, and enhance ba-
sic strength, setting the stage for a quicker
comeback.
Therapy pre- or post-operatively allows for
accelerated recovery. “So, they’re a step
ahead of the game,” says Marc Capannola,
Clinical Director of PERFORMANCE, add-
ing, “Patients also get a mental lift know-
ing they will be able to be active sooner.”
PERFORMANCE Physical Therapy also
provides an important therapeutic tool
called the SwimEx. “This aquatic therapy
approach to rehabilitation allows for quick-
er initiation of the rehabilitation program
for a patient who is not ready to do an ac-
tivity on a hard surface but may be able to
do it in the water,” says Mr. Capannola.
Physician Referrals
Cary Orthopaedic accepts referrals from
all physicians, regardless of specialty or
hospital affiliation. For more information,
visit the practice at www.caryortho.com
or call (919) 467-4992.
Sports Medicine Specialists:
Douglas L. Gollehon, M.D.
Brian T. Szura, M.D.
Douglas J. Martini, M.D.
William K. Andersen, M.D.
Derek L. Reinke, M.D.
Mark A. Curzan, M.D.
Raymond M. Carroll, MD.
Edouard F. Armour, M.D.
Given the prevalence and variance of neck and
back pain in our society, Cary Orthopaedic Spine
Specialists has put together a dedicated medical
team providing advanced non-surgical and surgi-
cal options to treat the sources of pain.
Neck pain is typically caused by poor posture
at work while seated in front of a computer
or during recreational activities, according to
Sameer Mathur, M.D. “Fortunately, associated
problems are not serious in approximately 80
percent of cases and can be treated non-sur-
gically through a tailored physical therapy pro-
gram or spinal injections.”
When symptoms don’t improve after two or
three months of conservative treatment, sur-
gery may be a solution.
Traditional surgical treatment for a degenera-
tive or herniated disk, one of the most common
problems, is cervical diskectomy and fusion. In
select patients, a new surgical procedure can
be performed without fusion. Similar to total
knee and hip replacement, the degenerated
cervical disk can be replaced with an artificial
implant that replicates the function of the disk-
joint complex. This allows the neck to maintain
motion and prevents adjacent-level arthritis.
Approximately two-thirds of adults suffer from
low back pain at some time in their lives. Com-
mon causes include myofascial dysfunction,
degeneration of the disc or facet joints, spon-
dylolisthesis, spinal stenosis and compression
fractures.
Spinal stenosis occurs when there is narrowing
of the spine, resulting in compression of the
spinal nerves. The traditional surgical approach
involves wide lumbar decompression and possi-
ble fusion. Patients are in the hospital for sever-
al days and may suffer from chronic back pain.
The minimally invasive X-STOP procedure revo-
lutionized the treatment for spinal stenosis.
It is placed between the spinous processes to
prevent extension of the spine. The outpatient
procedure is performed under local anesthesia.
Recovery and return to normal activity is much
quicker.
Compression fracture of the vertebral body is
common in older adults. Conservative treat-
ment includes bed rest, pain control and physi-
cal therapy. If that approach is unsuccessful
kyphoplasty is a minimally invasive treatment
option. Through two small incisions at the level
of the fracture, cement is introduced into the
vertebral body to reinforce it. This is done un-
der local anesthesia, and patients experience
immediate pain relief in the recovery room.
Most often surgery is not necessary. If surgery
is determined to be the best option, Cary Or-
thopaedic Spine Specialists will first consider
minimally invasive alternatives that produce
equal or better results than traditional surgery.
Cary Orthopaedic Spine Specialists’ physiatrists
are experienced in the use of fluoroscopic-guid-
ed epidural joint injections to treat chronic back
pain. The treatment applies a numbing agent
and anti-inflammatory on or near the inflamed
nerve.
Additional procedures available in this compre-
hensive spine center are nerve conduction and
EMG (electromyogram) studies. Acupuncture
also is offered for pain relief or resolution and
may serve as a reasonable alternative to long-
term narcotic analgesics.
Spine-Focused Physical Therapy
The physical therapists at the Spine Center are
completely focused on the spine and specially
trained in manual therapy techniques. Patients
also learn proper lifting and moving tech-
niques, and are guided on maintaining proper
body mechanics.
Physician Referrals
Cary Orthopaedic Spine Specialists accepts
direct referrals for neck and back problems
requiring evaluation, management, surgical
treatment, physical therapy and/or interven-
tional spinal injections.
Spine SpecialistsOrthopaedic Spine Surgeon
Sameer Mathur M.D.,
Physiatry Team:
Scott S. Sanitate, M.D.
Gary L. Smoot, M.D.
Chris Lin, M.D.
Nicole P. Bullock, M.D.
Spine Specialists Center Offers “Dedicated Care for the Spine”
MAY 2011 9
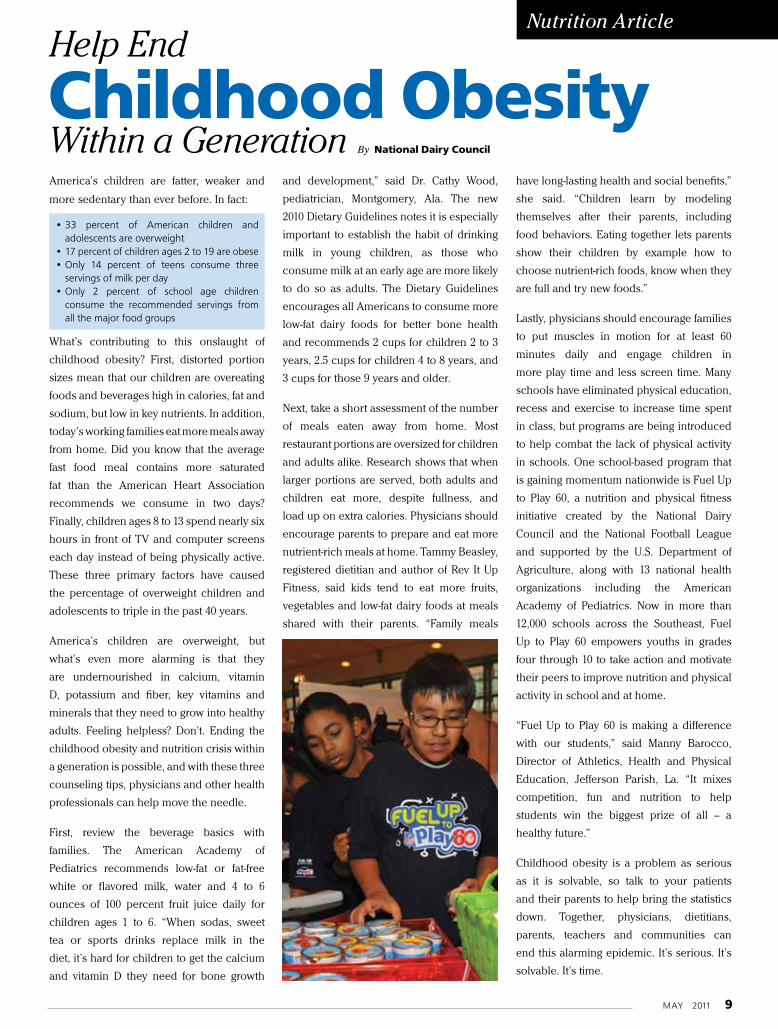
America’s children are fatter, weaker and
more sedentary than ever before. In fact:
• 33 percent of American children and adolescents are overweight
• 17 percent of children ages 2 to 19 are obese• Only 14 percent of teens consume three
servings of milk per day• Only 2 percent of school age children
consume the recommended servings from all the major food groups
What’s contributing to this onslaught of
childhood obesity? First, distorted portion
sizes mean that our children are overeating
foods and beverages high in calories, fat and
sodium, but low in key nutrients. In addition,
today’s working families eat more meals away
from home. Did you know that the average
fast food meal contains more saturated
fat than the American Heart Association
recommends we consume in two days?
Finally, children ages 8 to 13 spend nearly six
hours in front of TV and computer screens
each day instead of being physically active.
These three primary factors have caused
the percentage of overweight children and
adolescents to triple in the past 40 years.
America’s children are overweight, but
what’s even more alarming is that they
are undernourished in calcium, vitamin
D, potassium and fiber, key vitamins and
minerals that they need to grow into healthy
adults. Feeling helpless? Don’t. Ending the
childhood obesity and nutrition crisis within
a generation is possible, and with these three
counseling tips, physicians and other health
professionals can help move the needle.
First, review the beverage basics with
families. The American Academy of
Pediatrics recommends low-fat or fat-free
white or flavored milk, water and 4 to 6
ounces of 100 percent fruit juice daily for
children ages 1 to 6. “When sodas, sweet
tea or sports drinks replace milk in the
diet, it’s hard for children to get the calcium
and vitamin D they need for bone growth
and development,” said Dr. Cathy Wood,
pediatrician, Montgomery, Ala. The new
2010 Dietary Guidelines notes it is especially
important to establish the habit of drinking
milk in young children, as those who
consume milk at an early age are more likely
to do so as adults. The Dietary Guidelines
encourages all Americans to consume more
low-fat dairy foods for better bone health
and recommends 2 cups for children 2 to 3
years, 2.5 cups for children 4 to 8 years, and
3 cups for those 9 years and older.
Next, take a short assessment of the number
of meals eaten away from home. Most
restaurant portions are oversized for children
and adults alike. Research shows that when
larger portions are served, both adults and
children eat more, despite fullness, and
load up on extra calories. Physicians should
encourage parents to prepare and eat more
nutrient-rich meals at home. Tammy Beasley,
registered dietitian and author of Rev It Up
Fitness, said kids tend to eat more fruits,
vegetables and low-fat dairy foods at meals
shared with their parents. “Family meals
have long-lasting health and social benefits,”
she said. “Children learn by modeling
themselves after their parents, including
food behaviors. Eating together lets parents
show their children by example how to
choose nutrient-rich foods, know when they
are full and try new foods.”
Lastly, physicians should encourage families
to put muscles in motion for at least 60
minutes daily and engage children in
more play time and less screen time. Many
schools have eliminated physical education,
recess and exercise to increase time spent
in class, but programs are being introduced
to help combat the lack of physical activity
in schools. One school-based program that
is gaining momentum nationwide is Fuel Up
to Play 60, a nutrition and physical fitness
initiative created by the National Dairy
Council and the National Football League
and supported by the U.S. Department of
Agriculture, along with 13 national health
organizations including the American
Academy of Pediatrics. Now in more than
12,000 schools across the Southeast, Fuel
Up to Play 60 empowers youths in grades
four through 10 to take action and motivate
their peers to improve nutrition and physical
activity in school and at home.
“Fuel Up to Play 60 is making a difference
with our students,” said Manny Barocco,
Director of Athletics, Health and Physical
Education, Jefferson Parish, La. “It mixes
competition, fun and nutrition to help
students win the biggest prize of all – a
healthy future.”
Childhood obesity is a problem as serious
as it is solvable, so talk to your patients
and their parents to help bring the statistics
down. Together, physicians, dietitians,
parents, teachers and communities can
end this alarming epidemic. It’s serious. It’s
solvable. It’s time.
Childhood Obesity Nutrition Article
Within a Generation
Help End
By National Dairy Council
10 The Triangle Physician
Opthalmology
During the first three months of the Iraq
war in 2003, the military airlifted 60 service
members out of the region because of
severe corneal ulcers caused by contact
lens wear. The military now forbids contact
lenses because of the risks associated
with dusty and dirty conditions. And
while contact lens wear can be dangerous
in combat situations, eyeglasses can be
impractical. Even if the glasses don’t break,
they often can hinder soldiers on missions.
The spectacles can fog up, fall off or make
putting on a gas mask a cumbersome and
time-consuming task when seconds matter.
Many people want to get laser eye surgery
so they can be free of the hassles of glasses
or contacts. But many service members
deploying to Iraq and Afghanistan are
rushing to get it done for much different
reasons. They are getting the surgery
because it could save their life.
Over the years, vision correction technology
has evolved such that LASIK (laser-assisted
in situ keratomileus) has proven to be a
safe and effective procedure. This has led
to a growing acceptance of LASIK in the
military.
The United States armed forces have
embraced LASIK as a way to make troops
“combat ready.” Laser vision correction
has been allowed for all aspects of
military service, including aviation, special
operations and support personnel. It also is
approved for NASA astronauts. The Air Force
now allows LASIK in all aviators, including
those in high-performance aircraft.
Although the most common types of laser
eye surgery can cost between $2,500 and
$5,000 for both eyes at a private doctor,
active military personnel can now receive
LASIK free at one of 25 Warfighter Refractive
Eye Surgery Program centers.
Since its introduction to the Armed Forces
in 2000, more than 300,000 refractive
surgery procedures have been performed
at military hospitals, and more than 45
studies have been conducted to determine
the safety and efficacy of laser vision
correction among military personnel.
The Navy is currently undertaking a study
on Naval aviators. To date, more than
200 aviators have been enrolled in the
study. The results of the study have been
outstanding. Aviators were able to return to
flight status within four weeks after LASIK.
Patient satisfaction has been excellent.
One hundred percent were able to achieve
20/20 levels of vision. There were no
complaints of significant glare, halos, haze
or sharpness of vision. Ninety-eight percent
felt that LASIK helped their effectiveness
as a naval aviator and 98 percent indicated
they would definitely recommend LASIK to
their fellow aviators.
Innovations, such as blade-free and
wavefront-guided technology, have made
the LASIK procedure better and safer.
Acceptance of the new and improved
LASIK eye surgery by the Department of
Defense has helped make our troops better
and safer.
LASIKAdvances Benefit Military’s EffectivenessBy Dean Dornic, M.D.
Dr. Dean Dornic is founder and medical director of the Laser Eye Center of Carolina. A board-certified, fellowship-trained vision correction specialist, he has more than 15 years of surgical experience and has performed thousands of successful LASIK procedures. He was selected as one of “America’s Top Ophthalmologists” by Consumer’s Research Council of America and was named a LASIK Gold surgeon – an honor bestowed upon the top 50 LASIK surgeons nationwide by Sightpath Medical. Dr. Dornic has lectured at international meetings and trained other surgeons on LASIK. For more information, visit www.visionauthorities.com.
The United States armed forces have embraced LASIK as a way to make troops “combat ready.”
MAY 2011 11
Orthopedics
Total Ankle Replacement Is Revolutionizing Care of Ankle ArthritisBy Selene G. Parekh, M.D., M.B.A.
The third-generation implants require smaller bone cuts, are more anatomical and better able to restore natural ankle motion.
Ankle arthritis is a chronic condition that
causes substantial pain, disability and loss in
quality of life. In fact, a recent study published
in 2008 demonstrated end-stage ankle arthritis
to be as debilitating as hip arthritis.
Until recently, conservative options, such as
injections, bracing and anti-inflammatories,
have been used to delay surgery. When
surgery was needed, the best option was
a surgical ankle fusion. This would relieve
pain, but unfortunately, leave patients
with a loss of motion in the ankle, a limp,
and make the knee and subtalar joints
susceptible to arthritic changes. These
issues have made clinicians, orthopedic
surgeons, researchers and ankle implant
companies seek other solutions.
Total ankle replacement (TAR) has been
available in the United States since the
1970s. The earlier generations of ankle
replacements were plagued with failures.
However, the most recent, third-generation
implants have overcome many of the
shortcomings of these earlier implants.
This has renewed the interest in TAR.
Currently in the United States, there are
three TAR systems available: the STAR, the
Salto and the Inbone. These implants have
been available in Europe for years, with
promising medium- and long-term results.
In the U.S., the Inbone was approved in
2005, the Salto in 2006 and the STAR in 2009.
The goals of TAR surgeries are to reduce
pain, while preserving a natural range
of motion. The third-generation implants
require smaller bone cuts, are more
anatomical and better able to restore
natural ankle motion.
The ideal candidate for a TAR suffers from
post-traumatic ankle arthritis or rheumatoid
arthritis, is less than 250 pounds and is 50
years of age or older with little or no major
ankle deformity. However, this is changing
as orthopedic foot and ankle surgeons gain
more experience with these implants and
techniques. Depending on the specifics of
a patient, TAR surgery is being performed at
an earlier age, with greater deformities and
with a larger body mass index.
The evaluation of a patient with ankle
arthritis begins with a thorough history
and physical exam, followed by weight-
bearing radiographs. At times, a computed
tomography scan may be needed to provide
more anatomical details. Based on these
findings, treatment options are reviewed
with the patient. If a patient is a candidate
for a TAR, a medical clearance and dental
evaluation to eliminate a possible source of
infection are requested.
The surgery for TAR requires an overnight
stay. The patient is made non-weight bearing
for four to six weeks. Thereafter, intense
physical therapy is required to gait train and
strengthen the ankle. Most patients note a
tremendous improvement in their quality of
life, being able to perform activities, such
as walking, yoga, golf and swimming, which
they may have lost for years.
Total ankle replacements are revolutionizing
the care of ankle arthritis. Pain relief,
preservation of adjacent joints, restoration
of ankle motion and a more normal gait
are some of the benefits of third-generation
TAR procedures. Patients should be made
aware of this treatment option, as it holds the
promise of transforming their quality of life.
Dr. Selene G. Parekh is an associate professor of orthopedic surgery at the North Carolina Orthopaedic Clinic and Duke University, Department of Orthopaedic Surgery. His research and clinical interests include total ankle replacements, foot and ankle injuries of athletes, minimally invasive foot and ankle trauma surgery, tendon injuries of the foot and ankle, and the adoption and development of novel technologies in foot and ankle surgery. Dr. Parekh has been an active speaker at regional, national and international meetings, helping to teach other orthopedic surgeons about novel techniques for the care of foot and ankle patients.
12 The Triangle Physician
Your Financial RX
Reduce Your Investment
Pain ThresholdBy Paul Pittman, C.F.P.
“Are you having any pain today? On a scale
of 1 to 10, what is your current pain level?”
The nurse asked me these questions during
my last few doctor visits. Thank goodness, I
have not had any pain for quite awhile, but
it makes me wonder: What is a level 1? What
is a level 10?
I have had a physician tell me that I was going
to feel some “pressure” during a procedure.
“Pressure” must be the buzzword for “this is
a 5 on the pain scale.” (By the way, using the
word “pressure” instead of “pain” doesn’t
minimize the experience.)
Anyway, back to my question on what each
level means. I have experienced what I can
only imagine was a 10. I had a kidney stone
rear it’s ugly head during my daughter’s
dance recital. It was my first, and I was sure
that a rhino had rammed his horn into my
back.
I went from a 0 to a 10 in about 30 minutes.
My wife took me to the emergency room,
and thank goodness it was closer than the
gun shop.
As I writhed on the floor of the ER, the triage
nurse said it was probably a kidney stone. I
was certain that it was the size of a Buick.
But I was one of the lucky ones; mine was
so small I was going to be able to pass it on
my own. Sure enough, 12 hours later, I heard
the unmistakable “clink” in my urine screen.
If this wasn’t a 10, then I can only hope
that a 10 involves blacking out. I had been
on painkillers that could have stopped that
charging rhino in his tracks, and the stone
wasn’t much bigger than a decimal point on
this page.
How could something so small bring a
rough and tough six-foot man to the ground?
The same way opening your investment
statements might be doing to you right now.
Is the decimal point causing pain?
Are you experiencing any pain right now?
On a scale of 1 to 10, what is your current
level?
What I have witnessed in 24 years in this
business is that something as small as a
decimal point can raise an investor’s pain
level immediately to a 10. Usually the source
of pain is not the decimal point, but the
location of that decimal point.
Your broker might be telling you that this is
“pressure.” Now we all understand this term
much better.
Did you know 94 percent of all active money managers under-perform their respective indexes? Are you in the 94 herd or the elite 6?
Pain Threshold
MAY 2011 13
How does the movement of the decimal
point affect your stress level, your emotions,
your retirement, your child’s education? All
of these items should be fully taken into
account when you develop your Investment
Policy Statement in the very beginning. Do
you have clear and concise steps to lower
the pain level, or are you just trying to live
with the pain?
Pain in the investment world not only
brings doubt and fear into play, but can
also seriously derail a sound financial plan.
What you do not want is for this pain to
create a knee-jerk reaction. This is when
pain breeds panic, and panic develops
into bad decision-making. Pain does crazy
things to emotions.
If you are properly allocated, then secular
bear markets shouldn’t shoot your pain
level to a 10 and create bad decisions. Look
back over one of my previous articles on
proper allocation to better understand this
concept. (If you cannot locate it, I am happy
to e-mail it to you.)
Is overlap killing your allocation?
I’ll wager that right now you have a large
degree of “overlapping” in your portfolio.
Overlapping is a killer of proper allocation.
This is where you own certain positions
more than once and probably many times
in a standard, brokerage-firm allocation.
You may very well own Cisco Systems or
Coca-Cola or General Electric, three or four
or five times in your portfolio!
This is not to say that owning these posi-
tions is a bad thing, but owning them several
times is. It raises your risk level many times
over. True allocation is broad, covers many
asset classes, styles and countries, but most
importantly, it is designed specifically for
you. Your investment profile, risk tolerance
and goals are as individual as your
fingerprint.
Here again, I strongly advise you to find a
qualified person to help you develop your
personal allocation. Do not live with your
pain and accept what is shoveled at you.
Take the time, break the chain, find out
what is right for you and your family! It is
too important to keep on doing what you
have always done and expect a different
outcome.
Did you know 94 percent of all active money
mangers under-perform their respective
indexes? Are you in the 94 herd or the elite 6?
Until next month, good health and
happiness.
Paul J. Pittman is a Certified Financial Planner™ with The Preferred Client Group, a financial consulting firm for physicians in Cary, N.C. He has more than 25 years of experience in the financial industry and is passionate about investor education. He is also a nationally sought-after speaker, humorist and writer. Mr. Pittman can be reached at (919) 459-4171 and [email protected].
Womens Wellness half vertical.indd 1 12/21/2009 4:29:23 PM
Category
14 The Triangle Physician
Sleep Medicine
Sleep Apnea By Giridhar Chintalapudi, M.D.
About 70 million Americans suffer from
a sleep problem and nearly 60 percent of
them have a long-term disorder. Even though
sleep problems are very common, they are
very often undiagnosed and untreated. One
of the most common sleep problems is
sleep apnea. It is estimated that 4 percent of
middle-aged men and 2 percent of middle-
aged women suffer from sleep apnea.
In sleep apnea, you have one or more pauses
in breathing while you sleep. You often move
out of deep sleep and into light sleep when
your breathing pauses or becomes shallow.
This results in poor sleep quality that makes you
tired during the day. Sleep apnea is one of the
leading causes of excessive daytime sleepiness.
Doctors usually can’t detect the condition
during routine office visits. Also, there
are no blood tests for the condition. Most
people who have sleep apnea don’t know
they have it because it only occurs during
sleep. A family member and/or bed partner
may first notice the signs of sleep apnea.
Sleep Apnea Can Contribute
to Serious Medical Conditions
During normal sleep, throat muscles relax.
When this happens, if there is too little
room inside your throat or too much tissue
pressing on the outside of your throat, your
airway can become blocked. This blockage
stops the movement of air, and the amount
of oxygen in your blood drops. The drop in
oxygen causes the brain to send a signal for
you to wake up, so you open up the airway
in your throat and start breathing again. If
you have sleep apnea, this cycle may repeat
as often as 50 or more times an hour.
The frequent drops in oxygen level and
reduced sleep quality trigger the release of
stress hormones. These compounds raise
heart rate and increase your risk of high blood
pressure, heart attack, stroke and arrhythmias
(irregular heartbeats). The hormones also
raise the risk of, or worsen, heart failure
Untreated sleep apnea also can lead to
changes in how your body uses energy.
These changes increase your risk of obesity
and diabetes.
One of the most common signs of
obstructive sleep apnea is loud and chronic
(ongoing) snoring. Pauses may occur in the
snoring. Choking or gasping may follow the
pauses. You’re asleep when the snoring or
gasping happens. You likely won’t know that
you’re having problems breathing or be able
to judge how severe the problem is. Your
family members or bed partner often will
notice these problems before you do.
Other signs and symptoms of sleep apnea
may include: morning headaches; memory
or learning problems and not being able to
concentrate; feeling irritable, depressed, or
having mood swings or personality changes;
urination at night; and a dry throat when you
wake up.
Another common sign is fighting sleepiness
during the day, at work or while driving.
You may find yourself rapidly falling asleep
during the quiet moments of the day when
you’re not active.
Doctors usually can’t detect the condition during routine
office visits. Also, there are no blood tests for the
condition. Most people who have sleep apnea don’t know
they have it because it only occurs during sleep.
Requires Specialized Attention
MAY 2011 15
If a patient has problems breathing during
sleep, even if he doesn’t have daytime
sleepiness, he should talk with his doctor.
Treatment Can Restore
Regular Breathing
Doctors diagnose sleep apnea based on
medical and family histories, a physical
exam and results from sleep studies. Usually,
your primary care doctor evaluates your
symptoms first. He or she then decides
whether you need to see a sleep specialist
for diagnosis and treatment. A sleep study is
the most accurate test for diagnosing sleep
apnea. It records what happens with your
breathing while you sleep.
The goals of treating sleep apnea are to
restore regular breathing during sleep and
relieve symptoms, such as loud snoring
and daytime sleepiness. Lifestyle changes,
mouthpieces, breathing devices and surgery
may be used. Medicines typically aren’t used
to treat the condition.
Treatment may improve other medical
problems linked to sleep apnea, such as
high blood pressure. Treatment also can
reduce your risk of heart disease, stroke
and diabetes. If a patient has sleep apnea,
he should talk with his doctor or sleep
specialist about the treatment options that
will work best.
Dr. Giridhar Chintalapudi (“Dr. Chin”) earned his medical degree from Kurnool Medical College, India. Before moving to the United States, he worked in United Kingdom for five years, with special interest in neuropsychiatry. He completed his internship and residency at State University of New York, Stony Brook. He is board certified in general neurology, vascular neurology and sleep medicine. He also is a board member of North Carolina Academy of Sleep Medicine. In addition to being active in private practice, he also is involved in teaching both neurology and sleep medicine. Dr. Chin can be reached at 919-708-5008.
Financial Rx for Physicians:• AidingWealthCreation,Preservation andProtection• BusinessManagement• Tax-strategies• LiabilityProtection• AssetPreservation
Trust your wealthcare to a specialist.
Managing your patients’ health is your life’s work.Managing physicians’ wealth is mine.
The Preferred ClienT GrouPPaul J. Pittman CFP®
President and Managing Director
Securities offered through LPL FinancialMember NASD/SIPC
Wealth preservation and protect ion • estate planning • charitable g iv ing • buy-sell agreements and transfers
Wesvill Medical & Professional Center2304 Wesvill Court Raleigh, NC 27607
Leasing Opportunity with Ownership Potential
Medical Space Available in Rex Hospital Vicinity
Janet Clayton, [email protected]
Independently Owned & Operated
16 The Triangle Physician
Orthopedics
Double-Bundle Technique Improves Anterior Cruciate Ligament OutcomesBy Mark Galland, M.D.
Treatment of a once devastating knee injury
has evolved! In the all-too-recent past, tearing
one’s anterior cruciate ligament meant the
end of an active lifestyle and certainly the
end of many promising athletic careers.
New advances in surgical technique and an
enhanced understanding of the anatomy of
the ligament have improved the prognosis for
athletes suffering this once-devastating injury.
The anterior cruciate ligament (ACL) is a
ligament located in the middle of the knee
that connects the femur to the tibia. It is
a critical ligament that stabilizes the knee
during sports and physical activity. The
ACL is usually injured during a pivoting
or cutting motion and can occur with or
without contact.
ACL injuries have become more common
as participation in sports has increased.
As a result, ACL reconstructive surgery is
now one of the most common orthopedic
procedures.
New advances have greatly improved the
surgical technique of ACL reconstruction.
Traditionally ACL reconstruction has
focused on reconstruction of a single strand
or “bundle” of fibers. The results have been
largely successful in restoring knee stability
and returning athletes to play.
Unfortunately, many still experience some pain
and feelings of instability even after successful
surgery and rehabilitation. Still, others are
unable to return to their previous levels of
activity, and once-promising athletic careers
are ended. Moreover, knees reconstructed
with the traditional single-bundle technique
may be more prone to re-injury and often
develop arthritis many years later.
The latest research may explain these
uninspiring results. Through extensive
laboratory analysis, we have learned that
the ACL is composed of two separate
and distinct portions, or “bundles.”
Each functions independently and in
concert. Knowing this, it is reasonable to
conclude that reconstruction of only one
portion (and ignoring the other) will only
accomplish part of the goal – which is to
stabilize the knee and preserve the joint
from degenerative arthritis.
The newest and most progressive surgical
technique for ACL reconstruction is called
the anatomic double-bundle technique and
is superior to the single-bundle technique
in many ways.
Early results suggest that the anatomic
double-bundle technique decreases the
likelihood and severity of the post-surgical
problems associated with traditional single-
bundle technique, while increasing overall
knee stability. In addition, the knee is more
likely to regain normal range of motion as
compared to knees treated non-operatively or
with the traditional single-bundle technique.
This success is accomplished in the double-
bundle technique by accurately replacing
and restoring the native ACL.
Currently only a select few surgeons are
trained in and are performing this ground-
breaking technique. It is much more
technically demanding to perform, but there
The double-bundle technique is much more technically demanding to perform, but there is little doubt that one day it will be “The Standard.”
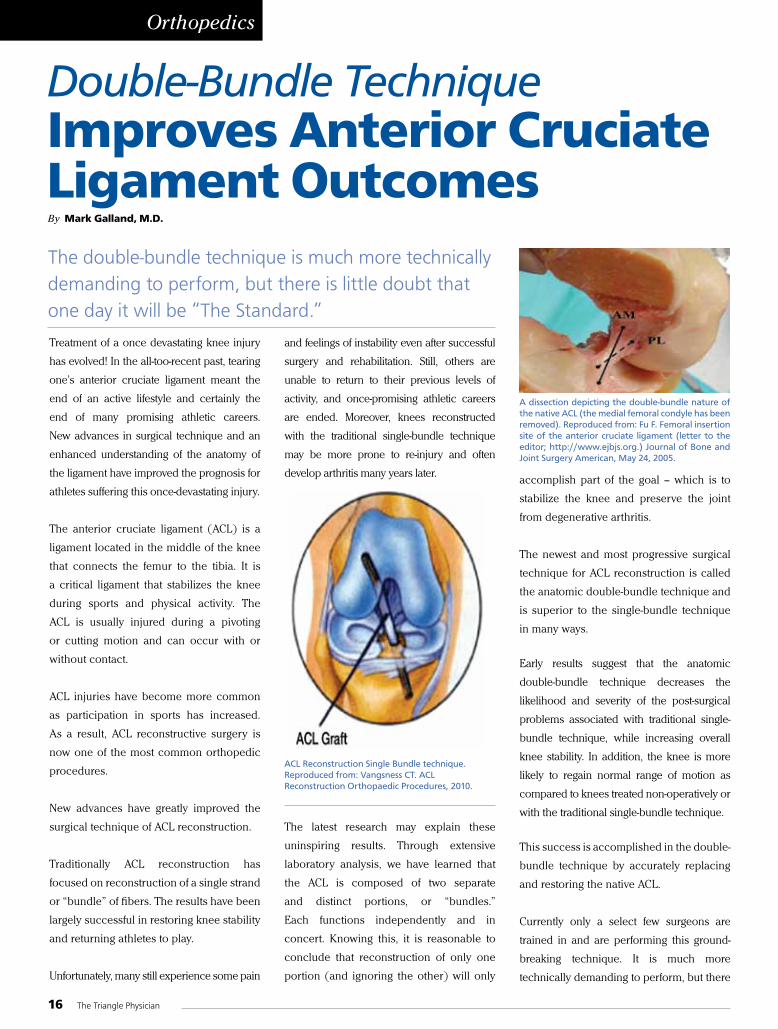
aCl Reconstruction single Bundle technique. Reproduced from: Vangsness CT. aCl Reconstruction orthopaedic Procedures, 2010.
a dissection depicting the double-bundle nature of the native aCl (the medial femoral condyle has been removed). Reproduced from: Fu F. Femoral insertion site of the anterior cruciate ligament (letter to the editor; http://www.ejbjs.org.) Journal of Bone and Joint surgery american, may 24, 2005.
MAY 2011 17
is little doubt that, one day, this double-
bundle technique will be “The Standard.”
We have entered a new era in sports
medicine. Athletes suffering a once
potentially devastating injury may now have
a reconstructive surgery to truly restore the
knee to its normal state. When suffering
a major knee injury such as an ACL tear,
surgeons who perform the anatomic
double-bundle technique may restore the
structures in the knee to a near normal state.
You can resume your life of physical activity
and sport participation with the confidence
that your knee is structurally sound.
Dr. Mark Galland of Orthopaedic Specialists of North Carolina is a board-certified orthopedic surgeon, specializing in sports medicine and practicing in Wake Forest and North Raleigh. He serves as team physician and orthopedic consultant for the Carolina Mudcats, the AA affiliate of the Cincinnati Reds, as well as several area high schools and colleges. Dr. Galland is a recognized expert in knee injuries and double-bundle ACL reconstruction. He can be reached at (919) 562-9410 or by visiting www.orthonc.com or www.drmarkgalland.com.
Our Priority Is Your Sleep!
Dr. G. Chin, (Chintapudi) MD, DABSMBoard Certified Sleep MedicineBoard Certified Neurology
Dr. H. Tellez, MDBoard Certified Neuromuscular Medicine
Board Certified Neurology
S A N D H I L L S S L E E P D I S O R D E R S C E N T E R
• Sleep Apnea • Sleep Studies• Memory Disorder • Brain/Spine MRI• Gait Problem • EEG• Neuropathy, ie: CTS • NCV- EMG Laboratory
The Specialities
295 Olmstead Blvd., Suite 12 Pinehurst, NC 28374
(910) 235-0595
112 Dennis DriveSanford, NC 27331
(919) 708-5008
609 Attain Street, Unit 101Fuquay-Varina, NC 27526
(919) 552-8917
888-614-7420 • www.SNSleepSolutions.com
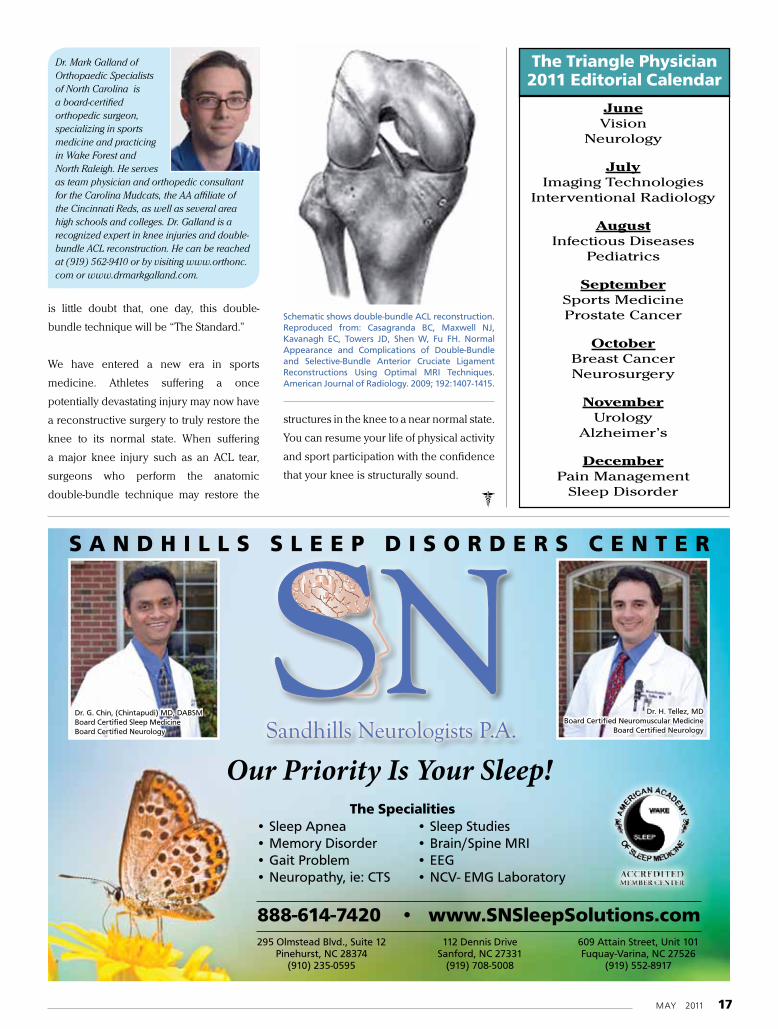
schematic shows double-bundle aCl reconstruction. Reproduced from: Casagranda BC, maxwell NJ, Kavanagh eC, Towers JD, shen W, Fu FH. Normal appearance and Complications of Double-Bundle and selective-Bundle anterior Cruciate ligament Reconstructions using optimal mRI Techniques. american Journal of Radiology. 2009; 192:1407-1415.
2011 Editorial Calendar
JanuaryEndocrinology
Glaucoma
FebruaryCardiologyLung Safety
MarchDigestive Health Care
Men’s Health
AprilWomen’s Health
Diabetes
May Orthopaedics
Allergies
June Vision
Neurology
JulyImaging Technologies
Interventional Radiology
AugustInfectious Diseases
Pediatrics
SeptemberSports MedicineProstate Cancer
OctoberBreast CancerNeurosurgery
NovemberUrology
Alzheimer’s
DecemberPain Management
Sleep Disorder
Triangle Physician’s Services
• New MDs in the area - can include a head shot, free service
• MD that has changed practices, free service
• New or relocated practice, free service
• New or changed Web Site, free service
• Events - listing of any event you are having, free service
• CMEs - listing of CMEs in the area, free service
• Editorials - in conjunction with the editorial calendar
• Clinical Trials- listing of your Clinical Trials see sample PDF, This is a paid service $50 per month with a 3 month minimum
• Profiles of new or existing doctors or practices Price depends upon 1, 2, 4, 6, or 8 page count
The Magazine for Healthcare Professionals.The Triangle Physician is being mailed to about 9,000 MDs, PAs and NPs, Administers, and Hospitals in the Greater Triangle area.Counties: Alamance, Chatham, Durham, Franklin, Granville, Harnett, Johnston, Lee, Moore, Nash, Orange, Person, Sampson, Vance, Wake, Warren, Wayne, and Wilson Counties
Cities: Raleigh, Durham, Chapel Hill, Smithfield, Roxboro, Henderson, Louisburg, Clinton, Pine Hurst, Siler City
Important InfoClose dates are the 1st of the Preceding month. ie: January will close on December 1st. For more information, please contact [email protected]
T H E M A G A Z I N E
F O R H E A L T H C A R E
P R O F E S S I O N A L S
The Triangle Physician2011 Editorial Calendar
18 The Triangle Physician
Cardiology
Atrial fibrillation is the most common rhythm
disorder resulting in hospitalization. With the
increasing population and the aging of the
baby boomers, it is becoming more prevalent
in every cardiologist’s practice.
Atrial fibrillation (AF) was probably first
described by the Chinese emperor physician
Huang Ti in his classic medical treatise about
2000 BC. The first modern description of AF
is credited to William Harvey in 1628, with
his observations of animal hearts. Willem
Einthoven published the first echocardiogram
recording of AF in 1906, calling it “pulsus
inequalis et irregularis.”
William Withering reported in 1785
administering digitalis leaf to patients with
heart failure. He noted that those with an
irregular pulse would improve and their pulse
would become steady. Karel Wenckebach in
1914 reported the use of quinine for AF after
a Dutch sailor told him how his palpitations
improved while taking quinine for malaria.
Walter Frey later reported that quinine’s
stereoisomer, quinidine, was more effective.
Atrial fibrillation was often categorized
as paroxysmal, persistent or chronic
(now permanent) for clinical purposes.
However, for most of the next century, our
understanding and treatment of AF did not
change significantly.
That has changed in the last two decades,
as we have seen a phenomenal growth in
our understanding of its pathophysiology.
Michel Haissaguerre’s group first reported
the recording of pulmonary vein potentials
in 1998. This quickly led to the concept that
paroxysmal AF is often triggered by ectopic
atrial tachycardias that commonly arise
from one or more of the pulmonary veins.
Persistent/permanent AF is usually associated
with enlarged atria and myocardial fibrosis,
which supports multiple wavelets.
New Treatment Frontier
This progress in understanding has led
to new options for therapy. The treatment
of AF still has three goals: prevention of
thromboembolism by anticoagulation,
ventricular rate control and rhythm control to
restore a sinus mechanism.
Numerous studies have been completed
showing the benefit of warfarin in AF.
The recent release of dabigatran, a direct
thrombin inhibitor, now offers an alternative.
Rate control is usually accomplished with
verapamil, dilitiazem and/or betablockers.
A nonpharmacologic alternative is AV
junction ablation and permanent pacemaker
implantation.
Rhythm control has historically been
relegated to medications. There are numerous
agents such quinidine, flecainide, sotalol, and
amiodarone, to name a few. Most recently
dronedarone was released. Unfortunately, no
agent works well, and not all are appropriate
for every patient due to coexisting conditions.
The current frontier of AF management is
nonpharmacologic treatment of AF to restore
sinus rhythm. This was first done by James
Cox with his cut-and-sew Maze operation in
1987. It evolved into the Maze III procedure
by 1992. This surgery works well but is open
chest/open heart. It is difficult to perform as
a concomitant procedure to other cardiac
surgery. For these reasons, it has not been
widely adopted.
Electrophysiologists later developed
percutaneous ablation techniques. There was
Atrial FibrillationBy Ker Boyce, M.D., F.A.C.C., F.A.C.P.
A Perspective on Treatment EvolutionDr. Ker Boyce earned his bachelor of science in chemistry from the Georgia Institute of Technology at age 18. After graduating with his medical degree from Emory University School of Medicine, he completed an internal medical residency at Emory. He then went on active duty in the United States Navy, serving first as a naval flight surgeon and force medical officer in support of the U.S. Antarctic Research Program. He then completed his cardiology fellowship at Naval Medical Center San Diego and his electrophysiology fellowship at the University of California San Diego. Dr. Boyce then returned and joined the faculty of the Naval Medical Center San Diego, eventually becoming the division chief and fellowship program director. In 1999, Dr. Boyce transferred to the U.S. Naval Reserve and entered private practice. He started the electrophysiology program at FirstHealth Moore Regional Hospital. He continued to serve in the Navy, mentoring the electrophysiology program at Naval Hospital Portsmouth and serving as an advisor to the Naval Aerospace Medical Institute until his retirement from the Navy in 2006.
Today, new catheter ablation devices are in development. Other energy sources are being evaluated. Hybrid procedures are being developed and refined. A new class of agents targeting the IKur
channels are in development.
MAY 2011 19
a rapid evolution from targeting potentials inside the pulmonary veins,
to pulmonary vein isolation, to antral isolation. This has been aided
by the development of 3-D mapping systems, importing of cardiac
computed tomography or magnetic resonance studies, irrigated-tip
radiofrequency catheters and robotics.
Despite these advances, the overall success rate for patients with
paroxysmal AF for a single ablation procedure is in the range of 60-
70 percent. It is less successful for the persistent AF patient with an
enlarged left atrium.
In the March 2011 issue of The Triangle Physician, there was an article
on a new hybrid AF procedure. This work was pioneered by Dr. Andy
Kiser at FirstHealth Moore Regional Hospital in Pinehurst.
Dr. Kiser started with an open-chest approach to assess the
epicardial ablation device and to develop a lesion set. He then
developed a minimally invasive approach through the pericardium.
In collaboration with electrophysiologists, a hybrid approach was
subsequently developed. The surgeon begins the ablation procedure
epicardially, and then the electrophysiologist completes the various
lines and tests for pulmonary vein isolation endocardially. With Dr.
Kiser’s return to his alma mater, this work will be continued at the
University of North Carolina at Chapel Hill.
So what does the future hold? New catheter
ablation devices are in development. Some
use balloons to deliver a circumferential
ablation around each pulmonary vein
ostium. Other energy sources are being
evaluated. Hybrid procedures are being
developed and refined. A new class of
agents targeting the IKur channels, found
predominantly in atrial myocardium, are in
development.
And what does this mean for patients? Each
patient is different. Some are asymptomatic
and only require anticoagulation. A few only
need a little more rate control. Many are
devastated with AF and require restoration
of sinus rhythm. With so many treatments
now available, it is imperative that the treating
physician be aware of the risks and benefits of
each, and then tailor therapy to each patient.
In the meantime, my kudos to all the
researchers, basic science and clinical, who
are continuing to explore new frontiers in
atrial fibrillation.
newsource & Associates
Make sure you connectwith your key audiencesusing strategic, cost-effectiveadvertising, marketing and publicrelations.
Our services range from consultation,to design, to creation andimplementation of strategic plans.
Our network of smart, creative,award-winning specialists servesthe health care industry throughoutthe Mid-Atlantic.
Maybe it’s happiness in a child’seyes. Whatever the desiredoutcomes, count on us to ensureyour key messages have the20/20 clarity to deliver.
Do They Like What They See?
Call (540) 650-3686 or send inquiries to [email protected].
NEWSOURCE-JUN10:Heidi 8/5/10 12:57 PM Page 1
INTRODUCING
Counties: Beaufort, Bertie, Bladen,
Brunswick, Camden, Cartert, Chowan,
Columbus, Craven, Cumberland, Currituck,
Dare, Duplin, Edgecomb, Gates, Greene,
Halifax, Hertford, Hoke, Hyde, Jones, Lenoir,
Martin, Montgomery, Moore, Nash, New
Hanover, North Hampton, Onslow, Pamlico,
Pasquotank, Pender, Perquiams, Pitt,
Richmond, Robeson, Sampson, Scotland,
Tyrrell, Washington, Wayne, Wilson
Cities: Greenville, Wilmington, Goldsboro,
New Ben, Fayetteville, Southern Pines, Pine
Hurst, Rocky Mount, Wilson, Washington,
Morehead City, Elizabeth City
DF MARKETING CONSULTING AND ASSOCIATES – 1-919-267-4296
If you’re looking for referrals from other Health Care Professionals, our publication will reach them. We directly mail our
publication to up to 6000 Physicians, PAs, NPs, and Medical Groups in the Eastern Region of North Carolina!
We are seeking EDITORIALS for our First Issue in July 2011!
Ask us about our FREE INITIAL CONSULTATION!
We offer ad development, graphic design assistance,
individualized- personal photos, head shots,
and a full service photo shoot for a nominal fee.
Want to be a featured doctor or clinic with up to 8 pages of
advertising space with a personalized brochure spread?
We can do that also.
For any assistance or questions you may have contact:
David Frank at 919-924-3751 or email at [email protected]
Kyle Blatchley at 910-992-1592 or email at [email protected]
“YOUR HAPPINESS IS OUR PRIORITY!”423 Cameron Woods Drive, Apex, North Carolina 27523
The Magazine for Healthcare Professionals. All health care professionals and health related businesses have a
new outlet for a direct publication that targets up to 6000 physicians,
PAs, NPs, medical centers and related health care professionals. The
regional physician publication is coming to the Eastern Region of North
Carolina! DF Marketing Consulting and Associates will be handling the
advertisements for the publication in the following counties:
T H E M A G A Z I N E
F O R H E A L T H C A R E
P R O F E S S I O N A L S
TheEastern
Physician

MAY 2011 21
Radiology
By Jeffrey Browne, M.D.
When a local mail courier’s hip pain became
so debilitating that he could no longer perform
his job, he discussed his options with his
physician. His arthritis would eventually require
hip replacement, but he was not quite ready for
the operation. He was an ideal candidate for
fluoroscopic-guided hip joint injection, and
his results were very gratifying. He was able to
return to work within a week and his pain was
markedly improved.
Whether an athlete or everyday patient, the team
of seven subspecialty-trained musculoskeletal
radiologists at Raleigh Radiology has you
covered for your interventional needs.
When conservative management of your
patient’s joint or tendon pathology fails or if
the cause of pain is uncertain, an image-guided
injection of a short-acting anesthetic and long-
acting corticosteroid is very useful in managing
patients.
The injections can be used to:
• Delay or eliminate need for surgery
• Diagnose cause or site of pain
• Control pain in non-operative patients
• Offer pain relief quicker than conservative
measures
Fluoroscopic-, ultrasound- and computed
tomography (CT)-guided injections increase
the precision of these procedures by confirming
correct needle placement. After administering
a local anesthetic, the needle is directed to the
site of interest, using minimal or no radiation
exposure. If a joint is the target, a small amount
of contrast is injected during fluoroscopy to
confirm intra-articular position. A combination
of a long-acting anesthetic and an intermediate-
to-long-acting corticosteroid are then injected.
The anesthetic can provide immediate pain
relief lasting four to six hours and also confirm
the site of pain. The corticosteroid begins
to work approximately one to two days after
injection, reaching its maximum effectiveness
within five to seven days.
Common indications for CT or fluoroscopic-
guided procedures include:
• Extremity (upper, lower, ankle, foot) joint
injection for pain or arthritis
• Joint aspirations
• Shoulder brisement for adhesive capsulitis
• Sacroiliac joint injections
Ultrasound is a very effective
modality when soft tissue or
fluid is the region of interest.
Procedures that can be
performed under ultrasound
include aspiration of fluid for
analysis, bursitis, treatment of
calcific tendinitis, drainage or
decompression of ganglion
cysts, Baker’s cysts, hematomas,
and abscesses. In many cases
of calcific tendinitis, the
calcifications can be aspirated
from the tendon or bursa prior
to the injection of steroids,
a procedure referred to as
shoulder barbotage.
The duration of the pain relief varies
depending on the severity and reversibility
of the patients’ condition, as well as other
factors. In the case of arthritis, the steroid will
reduce the inflammation; however, it will not
reverse the condition. If therapeutic effect is
achieved, a maximum of four injections per
year can be performed. Patients are asked to
assess changes in their pain shortly after their
injection and report the effectiveness to their
physician. Pain relief immediately following the
procedure is diagnostic of a problem at the site
of injection.
Before arriving for the procedure, patients are
requested to inform the staff if they are diabetic,
taking blood thinners or have had previous
reactions to iodinated contrast. Prior to the
injection, a radiologist will question the patient
about his or her symptoms and correlate them
with any imaging findings.
Complications are infrequent, but patients
should be aware of signs of infection at the
injection site. An allergic reaction to steroid
injection or iodinated contrast is rare and often
mild. Since the corticosteroid can take five to
seven days to reach maximum effectiveness,
we ask patients to avoid excessive activity
that could potentially prohibit the steroid from
reaching its full potential effect.
Our team of MSK radiologists offer these
injections at three convenient locations within
Raleigh: Our Blue Ridge and Cedarhurst
outpatient offices and at Rex Hospital. To
schedule a joint injection, call our Blue Ridge
facility at 781-1437 or Cedarhurst at 877-5400.
For more information, go to our website at
www.raleighrad.com.
ReferencesBoswell MV, Trescot AM, Datta S, et al. Interventional techniques: evidence-based practice guidelines in the management of chronic spinal pain. Pain Physician 2007 10:7-111.
Silbergleit R, Mehta BA, Sanders WP and Talati SJ. Imaging-guided injection techniques with fluoroscopy and CT for spinal pain management. Radiographics 2001 21:927-39.
Dussault RG, Kaplan PA, Anderson MW. Fluoroscopy-guided sacroiliac joint injections. Radiology 2000 214:273-6.
Raleigh Radiology’s Musculoskeletal TeamOffers Image Guided Pain Management
Dr. Jeffrey Browne is a musculoskeletal radiologist at Raleigh Radiology and medical director of computed tomography for Rex Hospital. He graduated from the University of Connecticut School of Medicine and completed an internship at St. Raphael’s Hospital in New Haven, Conn. He completed his residency and a fellowship in musculoskeletal radiology Duke University Medical Center. Dr. Brown is a member of the American College of Radiology, Radiological Society of North America and American Roetgen Ray Society. He joined Raleigh Radiology in 2008.

22 The Triangle Physician
Women’s Health
New Findings in Losing WeightBy Andrea S. Lukes, M.D., M.H.Sc., F.A.C.O.G.
The alarming fact is that approximately
two thirds of Americans are overweight or
obese. So when a study on the effects of a
combined drug (low-dose phentermine plus
topiramate) on excess weight and associated
comorbidities was published in Lancet in
April, health care providers took note.
Although not yet approved by the Food and
Drug Administration, the findings of the
CONQUER1 study showed significant weight
loss. Upon FDA approval, the combined
drug will be marketed as Qnexa.
In the CONQUER trial, two doses of
phentermine plus topiramate were
compared in overweight/obese subjects
as an adjunct to diet and lifestyle changes.
The term “overweight” refers to a body mass
index (BMI) greater or equal to 25 but less
than 30. Obesity refers to a BMI of greater or
equal to 30.
Adults evaluated in the study had a BMI
between 27-45 kg/m2, and two or more
comorbidities, including diabetes or
prediabetes, hypertension, dyslipidemia
or obstructive sleep apnea. Of the 2,487
subjects, 994 were assigned to placebo (979
analyzed), 498 to 7.5 mg phentermine plus
46 mg topiramate (488 analyzed), and 995 to
15.0 mg phentermine plus 92 mg topiramate
(981 analyzed).
At the lower dose, the mean weight loss was
8.1 kg, or 17.8 pounds. At the higher dose
the mean weight loss was 10.2 kg, or 22.4
pounds. These were both statistically higher
than the placebo group, which had a weight
loss of 1.4 kg, or 3.1 pounds.
At one year, this study showed that weight
loss of 10 percent or greater at one year was
seen in 7 percent of the placebo group, in
37 percent of the low-dose group and in 48
percent of the high-dose group. This was a
statistically significant difference for both
doses, compared to placebo.
Further, the cardiometabolic issues
associated with obesity improved in those
treated with the combined drug. Specifically,
there were significant reductions in systolic
blood pressure, diastolic blood pressure
(high-dose group), triglycerides, high-
sensitivity C-reactive protein (hs-CRP),
fasting glucose and total cholesterol. For
most of the risk factors, the improvement
was more in the higher dose group.
Taking Note of Side Effects
Phentermine was first approved by the
FDA as an appetite-suppressing drug back
in 1959. At one point it was combined
with a medication (fenfluramine, or
dexfenfluramine) and called Fen-Phen.
Eventually, dangerous side effects surfaced
in Fen-Phen users, with 24 cases of heart
valve disease, as well as cases of pulmonary
hypertension. Some individuals died from
the effects of Fen-Phen. Following these
reports, fenfluramine (or dexfenfluramine)
was taken off of the market voluntarily.
Afterward, studies showed that 30
percent of people taking fenfluramine,
or dexfenfluramine, had abnormal valve
findings.
The FDA did not ask manufacturers to remove
phentermine from the market. Phentermine
works on the hypothalamus portion of
the brain to release norepinephrine (a
neurotransmitter that signals a fight-or-
flight response, reducing hunger). The
most common side effects are dry mouth,
insomnia, dizziness, mild increase in blood
pressure (rarely more severe) and heart rate.
Monitoring blood pressure in important.
The precise mechanism of action for
topiramate is not clear, but theories suggest
energy expenditure increases with reduced
caloric intake, reduced salivary enzyme
activity, reduced leptin and corticosteroid
concentrations, and potential reduction in
serum glucose and insulin concentrations.
Of concern are the adverse events associated
with topiramate, including parasthesias,
memory impairment, taste distortion,
fatigue, insomnia, difficulty concentrating,
and dizziness.
Local Treatment Using Phentermine
More than 300 patients have been treated
using the drug phentermine through a
limited program at Women’s Wellness Clinic.
The medication is used for three to six
months to suppress appetite. When patients
start this program, they are told of a remote
chance of pulmonary hypertension is
possible.
It is recommended by the FDA that
phentermine be used short-term (up to
12 weeks), while incorporating healthy
dieting and exercise. In our experience and
through discussions with peers, if weight
Although not yet approved by the Food and Drug Administration, the findings of the CONQUER study showed significant weight loss.
Article Review:

MAY 2011 23
11 1234
DECNCHowever much you value
wildlife conservation in North Carolina,
That’s right! Your conservation effort is increased by a 3-to-1 matching gift. So, when you are one of the fi rst to display the new North Carolina Wildlife Habitat Foundation NCDMV license tag, your $10 tag contribution to the organization becomes $40 in lands preserved.
The all-volunteer North Carolina Wildlife Habitat Foundation assists in acquisition, management, and protection of land in North Carolina for the conservation of habitats needed to preserve wildlife
quadruple it.
right here in the Old North State. Conservation education efforts are preparing future generations to sustain your concern for the lands we protect today.
At www.ncwhf.org, download the license tag application and see the good works in process.
Your new tag shows your support and your contribution is put to work…times four.
www.ncwhf.org
feon,
ppYour n
co
w
loss continues through 12 weeks, then
continuation through 16 weeks is tolerated.
Weight-loss basics
Given that two-thirds of the United States
population is overweight (BMI greater or
equal to 25) or obese (BMI greater or equal
to 30), effective regimens for weight loss are
important to help individuals lose weight.
While effective medications are available,
there is basic information providers should
emphasize to their patients, including the
following:
• Healthy lifestyle changes in diet and
exercise should be emphasized.
• In order to lose one pound in a week, you
must have a deficit of 3,500 calories in that
week (500 calories per day for 7 days).
• Do not consume less than 1,200 calories
per day to avoid slowing down your
metabolism.
• Eat less and more often to boost
metabolism. Try to consume five to six
small meals during the day, beginning with
breakfast, within 45 minutes of walking.
• Keep a food journal – potentially an online
version that will keep a calorie count for
you. For example: www.thedailyplate.
com, www.calorieking.com, www.
sparkspeople.com, www.nutrihand.com
and www.mypyramid.com.
• Exercise! – This is so important to do for
weight loss and weight control.
• Be mindful of the food you are eating,
both in terms of quality and quantity.
• Do not multitask when you are eating, and
chew your foods well.
• Give yourself a pantry and refrigerator/
freezer makeover – Get rid of the foods
that tempt you.
• Do not eat late at night.
As new developments in weight loss emerge,
Women’s Wellness Center staff weighs the
risks and benefits. Call (919) 251-9223 for
available appointments and support with
helping patients to make healthy lifestyle
changes through weight loss.
References1Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults CONQUER: A randomized, placebo-controlled, phase 3 study. Lancet 2011; DOI:10.1016/S0140-6736(11)60505-5. Available at http://www.thelancet.com.
After earning her bachelor’s degree in religion from Duke University (1988), Dr. Andrea Lukes pursued a combined medical degree and master’s degree in statistics from Duke (1994). Then, she completed her ob/gyn residency at the University of North Carolina (1998). During her 10 years on faculty at Duke University, she co-founded and served as the director of gynecology for the Women’s Hemostasis and Thombosis Clinic. She left her academic position in 2007 to begin Carolina Women’s Research and Wellness Center, and to become founder and chair of the Ob/Gyn Alliance. She and partner Amy Stanfield, M.D., F.A.C.O.G., head Women’s Wellness Clinic, the private practice associated with Carolina Women’s Research and Wellness Clinic. Women’s Wellness Clinic welcomes referrals for management of heavy menstrual bleeding. Call (919) 251-9223 or visit www.cwrwc.com.

24 The Triangle Physician
WakeMed News
WakeMed North to Become Wake County’s Fifth Hospital
Construction Commences on Healthplex
WakeMed Health & Hospitals will begin
expansion in fall 2011 of the existing
WakeMed North Healthplex into Wake
County’s fifth hospital – WakeMed North
Hospital.
With an anticipated opening date of
October 2013, WakeMed North Hospital
will be a 61-bed acute care hospital, with
a focus on inpatient women’s specialty
services, offering a full range of obstetric
and gynecological services, including
comprehensive preventive, diagnostic and
therapeutic care. The facility will continue to
serve men and children through the existing
emergency department, outpatient surgery,
imaging, lab and physician services already
offered at the facility.
“Since opening in 2002, WakeMed North
Healthplex’ consumer-driven volumes
have consistently outpaced projections,
demonstrating the great demand for health
care services in this community,” said Dr.
Bill Atkinson, WakeMed president and chief
executive officer.
Currently WakeMed North
Healthplex offers a full-
service, 24/7 emergency
department, ambulatory
surgery center, imaging
and laboratory services
and a host of additional
clinical capabilities. The
campus also features
an 85,000-square-foot
medical office building.
“Transitioning to a hospital is the next logical
step, as the infrastructure is already in place
and the community has a critical mass of
262,000 residents living within a seven-mile
radius of the facility,” said Dr. Atkinson.
“While the hospital will initially open with a
women’s focus, our plan is for it to continue
to expand to meet the needs of women, men
and children, alike.”
Construction is expected to create 500
construction jobs. Hospital officials also said
the current 150 employees will be expanded
to about 442 full-time equivalent employees,
with an average salary of $48,760, by the
second year of hospital operation. The cost
of the project is estimated to be nearly $62
million.
WakeMed received approval to add 41
licensed acute care beds to WakeMed
North Hospital in 2009. These beds were in
addition to the 20 acute care beds already
approved for relocation from WakeMed
Raleigh Campus, making the total bed count
for WakeMed North Hospital 61. The inpatient
beds will be constructed in an approximate
90,000-square-foot addition to the existing
North Healthplex.
Construction has begun on WakeMed Brier
Creek Healthplex located at the corner of
US-70 on T.W. Alexander Drive.
The facility will include the county’s third
24/7 full-service, stand-alone emergency de-
partment with 12 private treatment rooms. It
will be staffed by the same board-certified
physicians that serve WakeMed’s five addi-
tional emergency departments.
Laboratory and imaging services, including
computed tomography and X-ray, also will
be available for emergency department pa-
tients and outpatient visits.
The facility, which will be owned, de-
veloped, and managed by Duke Realty,
will be 50,000 square feet, including a
26,000-square-foot emergency department
and 24,000 square feet of medical office
space.
Construction is slated to be completed by
November 2011 and the building will be op-
erational by January 2012. The project Cer-
tificate of Need was granted in September
2009 for $36 million. WakeMed’s total invest-
ment in the project is $14 million.
WakeMed Brier Creek Healthplex will ini-
tially employ 74 full-time employees and will
serve northwest Raleigh and Wake County.
It is located at 8001 T.W. Alexander Drive in
Brier Creek, less than one mile from I-540
and US-70. The complex sits on 12 acres, al-
lowing room for future development.
For more information, visit www.wakemed.org.

MAY 2011 25
WakeMed News
CON to Add 101 BedsWakeMed Health & Hospitals today
submitted two complementary Certificate
of Need (CON) applications to add 101
beds in accordance with the bed-need
allocation identified in North Carolina’s
2011 State Medical Facilities Plan. WakeMed
is proposing to add 79 acute care beds to
Raleigh Campus and 22 acute care beds to
Cary Hospital.
Both Raleigh Campus and Cary Hospital
currently operate above the state’s CON
performance occupancy threshold of
71.4 percent for hospitals the size of Cary
Hospital and 75.2 percent for hospitals the
size of Raleigh Campus. By 2015, growth
coupled with an aging population, will cause
Raleigh Campus and Cary Hospital to have
occupancy rates at or above 90 percent if no
additional beds are opened at these facilities,
according to a press release.
“WakeMed is the leading provider of inpatient
health care services in Wake County – the
second fastest-growing county in North
Carolina. And, WakeMed’s high inpatient
occupancy drove the allocation of 101 beds
in North Carolina’s State Medical Facilities
Plan,” said Stan Taylor, WakeMed vice
president corporate planning. “Additionally,
the other hospitals in Wake County currently
have unutilized or under-utilized acute care
beds and have not shown a good track
record in providing the inpatient capacity
that the community needs.”
Wake County will have five hospitals, with
the opening of WakeMed North Hospital
in October 2013, and four stand-alone
emergency departments. “Wake County
does not need more hospitals. It needs to
add more inpatient capacity in the county’s
two busiest existing hospitals, leveraging
existing infrastructure and support services
already in place to add beds quickly, cost-
effectively and efficiently,” says Taylor.
Physicians’ Office Pavilion at WakeMed North Healthplex
Medical Office Space Available
Capture the High-Growth, Affluent North Raleigh Market!
Janet Clayton, [email protected]
Independently Owned & Operated
26 The Triangle Physician
Granville Health System News
GHS Named Blue Distinction Center for Knee and Hip Replacement
Granville Health System in Top 10 of Most Customer-Friendly Hospitals
Granville Health System has been named
a Blue Distinction Center for Knee and Hip
Replacement.
Blue Distinction is a Blue Cross and Blue
Shield Association (BCBSA) program that
recognizes facilities that meet objective,
evidence-based thresholds for clinical
quality. These facilities have demonstrated
experience in offering comprehensive
inpatient knee and hip replacement
services, including total knee replacement
and total hip replacement.
BCBSA collaborated with expert physicians
and medical organizations to determine the
selection criteria for all Blue Distinction
programs. Candidates for Blue Distinction
Centers for Knee and Hip Replacement must
present clinical-based evidence to establish
that they meet the selection criteria.
Examples of some of the criteria GHS met
include:
• An established acute care inpatient
facility, including intensive care,
emergency care, and a full range of
patient support services
• An established knee and hip
replacement program, performing
required annual volumes for certain
procedures
• An experienced knee and hip
replacement surgery team, including
surgeons with board certification,
subspecialty fellowship training, and
case volumes that meet selection
criteria
• Preoperative patient education
• Processes to support transitions of care
• Multidisciplinary teams and clinical
pathways to coordinate and streamline
care
• Use of an internal registry or database
to track patient outcomes over time
• Clinical outcomes for specific
procedures that meet objective
thresholds, such as complication rates
and length of stay.
“When it comes to spine surgery, and hip
and knee replacement, there is compelling
evidence that institutions with experience
that also adheres to their care protocols
deliver better outcomes,” said Don Bradley,
M.D., chief medical officer of Blue Cross
and Blue Shield of North Carolina. “We’re
providing that information to our members
to help them make informed choices about
where to receive care that’s proven to meet
national quality standards.”
The American Alliance of Healthcare Pro-
viders named Granville Health System one
of the top 10 hospitals in the country in its
2011 Hospital of Choice Awards.
The award recognizes America’s “most cus-
tomer-friendly hospitals,” according to Ric
Vincent Parr, president of American Alli-
ance of Healthcare Providers (AAHCP). It is
“designed to find America’s most customer-
friendly hospitals based either on an exten-
sive application process, or by a review of
a facility’s public communication and staff
interaction with customers,” according to
an AAHCP press release.
Each year, AAHCP evaluates approxi-
mately 400 hospitals for consideration of
this award. Approximately 100 hospitals
are recognized annually. The application
process requires a review of six principal
areas of consideration including standards
of conduct, performance management and
improvement, staff development and train-
ing, systems of communication, good citi-
zenship, and educational and promotional
consumer material.
“We are pleased to be chosen as one of the
top hospitals in the nation,” says L. Lee Is-
ley, Granville Health System chief executive
officer. “This award recognizes the high lev-
el of quality care provided by our dedicated
doctors, nurses and staff to the patients of
Granville County and the surrounding ar-
eas. As we move forward, Granville Health
System will continue to invest further in the
hospital, supporting our commitment to de-
liver new medical programs, technologies
and expanded services to the community.”
Granville Health System ranked third after
first-place University of Kansas Hospital and
second-place UCLA Medical Center. The
Top 10 winners will have an opportunity to
compete for the Hospital of the Year Award,
to be announced this month.
Past Hospital of Choice Award recipients
include The Johns Hopkins Hospital, the
Mayo Clinic and the Cleveland Clinic.
MAY 2011 27
Durham Regional News
U.S. News Ranks Durham Regional Fourth in Metro Area Durham Regional Hospital has been ranked
fourth out of 18 hospitals in Raleigh-Durham in
U.S. News & World Report’s first-ever “Best Hos-
pitals” metro area rankings.
The newly expanded U.S. News & World Report
rankings of hospitals in the 52 most-populous
metropolitan areas show that in three specialties
Durham Regional offers Raleigh-Durham high-
quality care. In those specialties, which include
kidney disorders, orthopedics and urology, its
performance puts it above most other hospitals
that are not nationally ranked.
The new rankings recognize 622 hospitals in
or near major cities with a record of high per-
formance in key medical specialties. There are
nearly 5,000 hospitals nationwide.
Duke University Medical Center and University
of North Carolina Hospitals, respectively, ranked
in the top three hospitals in the Raleigh-Durham
metro area, according to the 2011 U.S. News Best
Hospitals metro ranking. Wake Medical Center
ranked No. 3 in nine specialty areas, including
kidney disorders, orthopedics and urology.
U.S. News created Best Hospitals more than
20 years ago to identify hospitals exceptionally
skilled in handling the most difficult cases, such
as brain tumors, typically considered inoper-
able, and delicate pancreatic procedures. Duke
and UNC also have achieved this U.S. News na-
tional ranking.
The new metro area rankings are relevant to a
much wider range of health care consumers.
They are aimed primarily at consumers whose
care may not demand the special expertise
found only at a nationally ranked Best Hospital.
The added centers boast a strong record of high
performance for most conditions and proce-
dures in one or more specialties, according to a
Durham Regional Hospital press release.
Patients and their families will have a far better
chance of finding a U.S. News-ranked hospital
in their health insurance network and might not
have to travel to get care at a high-performing
hospital, according to the Durham Regional re-
lease.
“Durham Regional is honored to be recognized
for our treatment of kidney disorders, orthope-
dics and urology,” said Kerry Watson, Durham
Regional Hospital president. “This recognition
reflects the dedication of our team of physi-
cians, employees and volunteers who care for
our patients every day.”
To be ranked in its metro area, a hospital had to
score in the top 25 percent among its peers in at
least one of 16 medical specialties.
“All of these hospitals provide first-rate care for
the majority of patients, even those with seri-
ous conditions or who need demanding proce-
dures,” said Health Rankings Editor Avery Co-
marow. “The new Best Hospitals metro rankings
can tell you which hospitals are worth consider-
ing for most medical problems if you live in or
near a major metro area.”
For the full list of metro area rankings visit
www.usnews.com/hospitals.
Upcoming Event
National prosthetic expert to host clinic
Ruben Preciado knows the power of a prosthetist. A below-knee amputee for three years, Preciado, 57, of Ra-leigh has forged a lifelong bond with nationally recognized prosthetist David R. Sickles, a certified prosthe-tist/orthotist and certified pedorthist with Peak Prosthetic Performance Clinic.
Sickles and his team will share their expertise with Raleigh/Durham amputees and friends or family members, by providing free, no-risk, one-on-one prosthetic evaluations May 17-19, 8 a.m. to 8 p.m., behind the Duke Raleigh Hospital. Registration is required.
Sickles has three decades of experi-ence and service in the design, fit and manufacturing of prosthesis. He is the current chief operating officer of the Center for Orthotic and Prosthetic Care (COPC) of North Carolina and New York. He is direc-tor of the National Commission on Orthotic and Prosthetic Education (NCOPE) Accredited Residency Pro-gram at COPC of North Carolina and president-elect of the North Carolina Chapter of the American Academy of Orthotics and Prosthetics (AAOP).
“The aim of Peak Prosthetic Perfor-mance Clinic is to provide anyone who has suffered a traumatic limb loss the chance to be heard, the chance to know what technology is available today and the ability to reach their peak prosthetic perfor-mance,” said Sickles, who is certified by the American Board for Certifica-tion in Orthotics, Prosthetics and Pedorthics Inc. (ABC).
“From microprocessor-controlled knee units to vacuum-assisted suspension sockets, my team and I have coupled the latest technology with exceptional patient care for countless amputees on their path to independance.”
To contact Sickles or to register for a complementary prosthetic evalu-ation, call (919) 821-5221 or (919) 684-2474. For more information on the Peak Prosthetic Performance Clinic, visit www.centeropcare.com.
After a disabling illness or injury, all you want to do is get back to your life—as quickly as possible.
Durham Rehabilitation Institute at Durham Regional Hospital helps you regain your independence with care delivered in a warm, compassionate environment.
Durham Rehabilitation Institute is an award-winning facility that provides comprehensive, state-of-the-art care. Treatment programs
are led by a board-certified rehabilitation physician. Other team members include nurse practitioners, rehabilitation nurses, physical therapists, speech therapists, and others dedicated to providing personalized care to meet each patient’s needs.
Top-rated rehabilitation care with the convenience of a community hospital: this is Durham Regional Hospital.
We help you get back to your life
durhamregional.org
8114
For physician referrals, call 919-470-7226.
28 The Triangle Physician
News
PhysiciansTiffany Linn Reed, DOInternal Medicine, GeriatricsDuke University Hospitals, Durham
Robert Thomas Abbott, MDDuke Health, Durham
Kristen Elizabeth Amann, MDInternal Medicine, PediatricsUniversity of North Carolina HospitalsChapel Hill
Mark Robert Anderson, MDUrological SurgeryDuke University Hospitals, Durham
Alison Dawn Bartel, MDAGAPE Clinic, Washington
Raymond Mark Bernal, MDDuke Health - Division of Urology, Durham
Elizabeth Jane Brant, MDUNC Kidney Center, Chapel Hill
Michelle Richardson Brownstein, MDGeneral SurgeryUNC Department of General SurgeryChapel Hill
Long Bao Cao, MDECU, Greenville
Devin Traer Caywood, MDRadiologyDuke University Hospitals, Durham
Rebecca Jean Chancey, MDPediatricsDuke University Hospitals, Durham
Matthew Alan Collins, MDEastern Urological Associates, Greenville
Lauren Jamie Ehrlich, MDDiagnostic Radiology, Pediatric RadiologyDuke University Hospitals, Durham
Amy Minchi Fang, MDDuke Eye Center, Durham
Kasey Kincaid Fiorini, MDAnesthesiologyUniversity of North Carolina HospitalsChapel Hill
Jillian Roxanna Foley, MDUNC - Division of Cardiology, Chapel Hill
Thomas Andrew Gebhard, MDDiagnostic RadiologyDuke University Hospitals, Durham
Katherine Lynn Harlow, MDEmergency MedicineUniversity of North Carolina HospitalsChapel Hill
Johann Hsin-heng Hsu, MDUNC Chapel Hill, Chapel Hill
David Paul Johnson, MDPediatricsDuke University Hospitals, Durham
Paul McPherson Johnson, MDInternal MedicineUniversity of North Carolina HospitalsChapel Hill
Shivanand P Lad, MDDuke University Medical Center, Durham
Robert Aaron Lambert, MDECU Dept of Family Medicine, Greenville
Marshall Andrew Mazepa, MDInternal MedicineUniversity of North Carolina HospitalsChapel Hill
Hannah Imwold Messer, MDPhysical Medicine and RehabilitationUniversity of North Carolina HospitalsChapel Hill
Tiffany Lynn Morton, MDUniversity of North Carolina HospitalChapel Hill
Todd Brandon Nelson, MDDermatologyPitt County Memorial Hospital, Greenville
Dana Michelle Neutze, MDFamily PracticeUniversity of North Carolina HospitalsChapel Hill
Erica Lynn O’Neill, MDObstetrics and GynecologyUniversity of North Carolina HospitalsChapel Hill
Andrew Fletcher Parker, MDEmergency MedicineDuke University Hospitals, Durham
Jose Luis Piscoya, MDGeneral SurgeryDurham
Alison Schmidt Powell, MDAnesthesiologyUniversity of North Carolina HospitalsChapel Hill
Shveta Shah Raju, MDDuke General Internal Medicine, Durham
Sarah Rodgers, MDDermatologyDuke University Hospitals, Durham
David Hallmark Ryan, MDObstetrics and GynecologyUniversity of North Carolina HospitalsChapel Hill
Justin Richard Scruggs, MDPhysical Medicine and RehabilitationUniversity of North Carolina HospitalsChapel Hill
Frank William Shields, MDDiagnostic RadiologyUniversity of North Carolina HospitalsChapel Hill
David Kristofer Sutton, MDOphthalmologyUniversity of North Carolina HospitalsChapel Hill
John Edward Thordsen, MDRetina Associates PC, Raleigh
Charles John Viviano, MDDuke Urology of Raleigh, Raleigh
Edward Scott Vokoun, MDNaval Hospital Camp LeJeun
De Benjamin Winter, MDECEP, Wilmington
Charles Ryan Woodard, MDDuke University Medical Center, Durham
Kanecia Obie Zimmerman, MDInternal Medicine, PediatricsDuke University Hospitals, Durham
Physician Assistants Jessica Eleanor Elder, PAGoldsboro
William H Etheridge, PARoanoke Chowan Hospital Emergency DeptAhoskie
Erin Christina Jones, PADayspring Family Medicine Associates, Eden
Kristin Dermody Maggi, PASunset Beach
Jessica Kristen Roberts, PAAtlantic Orthopedics, Wilmington
Kristina Marie Stover, PACoastal Carolina Orthopaedic SurgeonsJacksonville
Cary Gastroenterology Associates’ The new office is located at 555 Medical Park Place, Suite 108, inside the WakeMed Clayton Medical Park.
All six of Cary Gastroenterology’s board-certified physicians will treat patients at both the Cary and Clayton offices. Phone and fax numbers will be the same for both locations. To schedule an appointment at either office, call (919) 816-4948.
Raleigh Orthopaedic Clinic
The new office is located near Rex at 3633 Harden Road, Suite 100.
In addition to providing complete orthopedic services, this office will serve as the Raleigh Orthopaedic Clinic Pediatric Center. On-site services will include: fellowship-trained pediatric orthopedic surgeons, digital X-ray and therapy services.
The new location is an extension of our main Raleigh office, located at 3515 Glenwood Ave. Raleigh Orthopaedic Clinic (ROC) is Wake County’s largest and oldest orthopedic practice. The orthopedic surgeons are fellow-ship trained in their respective subspecialty areas, which include: foot and ankle, hand and wrist, spine, hip, shoulder and elbow surgery, total joint replacements, sports med-icine and pediatric orthopaedic care. Ancillary services include physical therapy, magnetic resonance imaging, radiology, shock wave therapy, and orthotics and pedorthics.
“We are very excited to be in this facility,” says Karl Stein, executive director of Raleigh Orthopaedic Clinic. “The Raleigh area is growing rapidly and we want to ensure easy access to our services for our patients.”
Complete practice information is available at www.raleighortho.com.
Pain Medicine for ShinglesWake Research AssociatesWayne Harper, MDPain after shingles? Has your shingles rash healed, yet you are still suffering from symptoms including burning, stabbing pain, sharpness or sensitivity? If so, you may have a condition called post-herpetic neuralgia, also known as PHN. We are conducting a clinical research study for people who have experienced these symp-toms for at least nine months after the onset of their shingles rash.
This study will evaluate the effectiveness of an investigational medication for PHN.Study-related medical exams and study medication are provided at no cost, and compensation will be provided for time and travel.
For additional information and qualifica-tion criteria please call (919) 781-2514 or visit us online at www.wakeresearch.com.
GastroenterologyStomach UlcersWake Research AssociatesCharles F. Barish, MDHave you suffered from a heart attack or stroke and take 325 mg of aspirin daily to prevent another from occurring? If so, Wake Research is conducting a research study of an investigational medication that combines aspirin with a second medi-cation to see if It can help prevent stom-ach ulcers. You’ll receive investigational medication and study-related exams at no cost and compensation up to $500 for time and travel.
For additional information and qualifica-tion criteria please call (919) 781-2514 or visit us online at www.wakeresearch.com.
General Medicine/InfectionsWake Research AssociatesCharles F. Barish, MDDo you have an upcoming hospitalization? You could be at risk of infection by Clos-tridium difficile (C.diff.), a bacteria that can cause severe gastrointestinal prob-lems.You may qualify for this study if you are between 40 and 75 years old and have an upcoming hospitalization.
Study-related medical exams and study medication are provided at no cost, and compensation will be provided for time and travel.
For additional information and qualifica-tion criteria please call (919) 781-2514 or visit us online at www.wakeresearch.com.
Welcome to the Area
New Office
New Office
Clinical Trials Do you have patients with any of these problems?

Your LocaL cardioLogY ProfessionaLsin Johnston countY
dedicated to QuaLitY, service, and integritY
cardioLogY servicesCoronary and Peripheral Vascular InterventionsPacemakers/DefibrillatorsAtrial Fibrillation AblationsEchocardiographyNuclear CardiologyVascular UltrasoundClinical CardiologyCT Coronary AngiographyStress TestsHolter MonitoringCardiovascular MedicineEchocardiographyNuclear CardiologyCardiac Catheterization
Smithfield Heart & Vascular Associates910 Berkshire RoadSmithfield, NC 27577Phone: 919-989-7909Fax: 919-989-3147
Eric M. Janis, MD, FACC
Ravish Sachar, MD, FACC
Nyla Thompson, PA-C
Diane E. Morris, ACNP
MateenAkhtar, MD, FACC
Benjamin G.Atkeson, MD, FACC
Christian N. Gring, MD, FACC
Matthew A. Hook, MD, FACC
Wake Heart & Vascular Associates2076 NC Hwy 42 West, Suite 100Clayton, NC 27520Phone: 919-359-0322Fax: 919-359-0326
the highest QuaLitY cardiovascuLar care, cLose to home.
2 Locations to serve our Patients
Kevin RayCampbell, MD, FACC
RandyCooper, MD, FACC
TTPFebruary 20118.45” x 10.9”
1 number to call, 17 locations serving the Triangle area. | Scheduling: 919-232-4700 | wakerad.com
The Easiest ImagingOrder Is Now Online.
Make life easier for your schedulers today!
©2
01
0 W
ake
Rad
iolo
gy.
All
right
s re
serv
ed.
Rad
iolo
gy S
aves
Liv
es.
Scan now to learn allabout Wake Radiology.
Download any QR Reader App foryour Smartphone!
As a referring provider, you can now place your imaging orders online with our new CMS-compliant provider portal. You or your schedulers can login and view each of our sub-specialty order forms to make ordering a breeze. The WR Provider Portal includes:
• Fast ordering with auto-fill cells• Online CPT code lists for MR and CT exams for quick reference• Order logs showing archived orders and orders pending authorization• Quick access to all WR patient forms and location maps• Complete training available for your staff
Get started today by calling our referral services staff at 919-788-7909.
Wake Radiology. Making your life easier.
C
M
Y
CM
MY
CY
CMY
K
WR_TTP Feb 2011_1.1.pdf 1 1/13/11 4:27 PM

![Page 236 Classify the triangle below A.Acute Triangle B.Obtuse Triangle C.Equiangular Triangle [Default] [MC Any] [MC All]](https://static.fdocuments.in/doc/165x107/5697bff71a28abf838cbef04/page-236-classify-the-triangle-below-aacute-triangle-bobtuse-triangle-cequiangular.jpg)