
Trials & Endpoints.“ - Cardiac Safety · "European Union Interest in Global Trials &...
17
"European Union Interest in Global Trials & Endpoints.“ TREAT Initiative Thinktank/incubator Jean-Philippe Collet JP. COLLET , DISCLOSURE: Research Grants (to the Institution) from Abbott Vascular, Bristol Myers Squibb, Boston Scientific, Cordis, Eli-Lilly, Fédération Française de Cardiologie, Fondation de France, Guerbet Medical, INSERM, Medtronic, Sanofi-Aventis Group, Société Française de Cardiologie; Consulting or Lecture Fees from Zsra-Zeneca, Bayer, Bristol-Myers Squibb, Daichi-Sankyo, Eli-Lilly, Sanofi-Aventis Group, Servier
Transcript of Trials & Endpoints.“ - Cardiac Safety · "European Union Interest in Global Trials &...
"European Union Interest in Global Trials & Endpoints.“
TREAT Initiative Thinktank/incubator
Jean-Philippe Collet
JP. COLLET, DISCLOSURE: Research Grants (to the Institution) from Abbott Vascular, Bristol Myers Squibb,
Boston Scientific, Cordis, Eli-Lilly, Fédération Française de Cardiologie, Fondation de France, Guerbet Medical,
INSERM, Medtronic, Sanofi-Aventis Group, Société Française de Cardiologie; Consulting or Lecture Fees from
Zsra-Zeneca, Bayer, Bristol-Myers Squibb, Daichi-Sankyo, Eli-Lilly, Sanofi-Aventis Group, Servier
Background: a great variability of TRI and no data in women
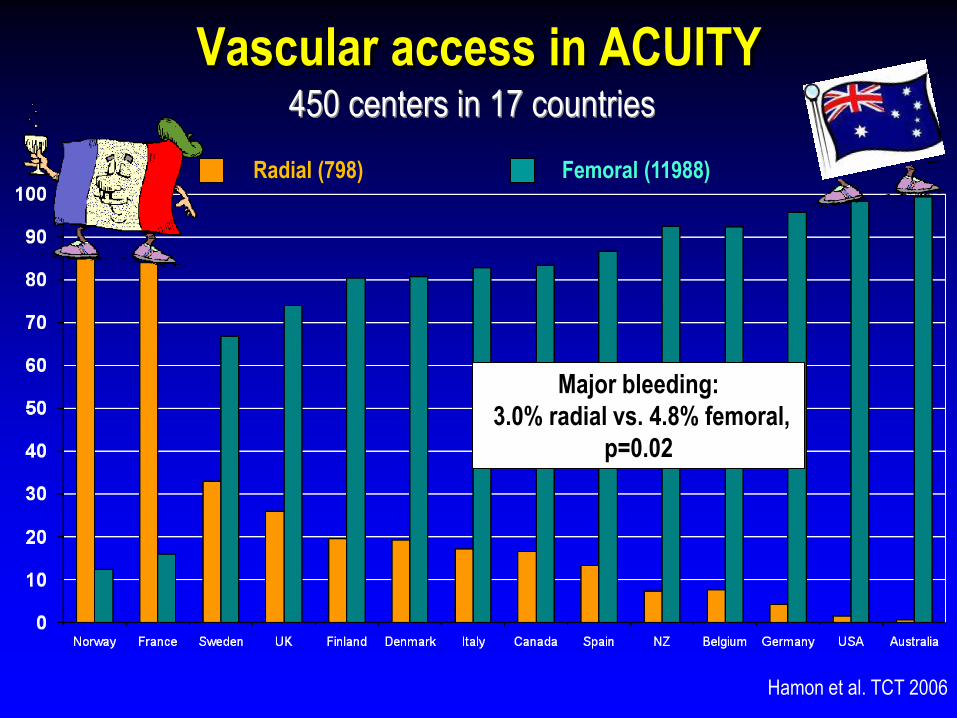
Vascular access in ACUITY 450 centers in 17 countries
Radial (798) Femoral (11988)
Hamon et al. TCT 2006
Major bleeding:
3.0% radial vs. 4.8% femoral,
p=0.02
What works well? A constant improvement over time
Preliminary Results
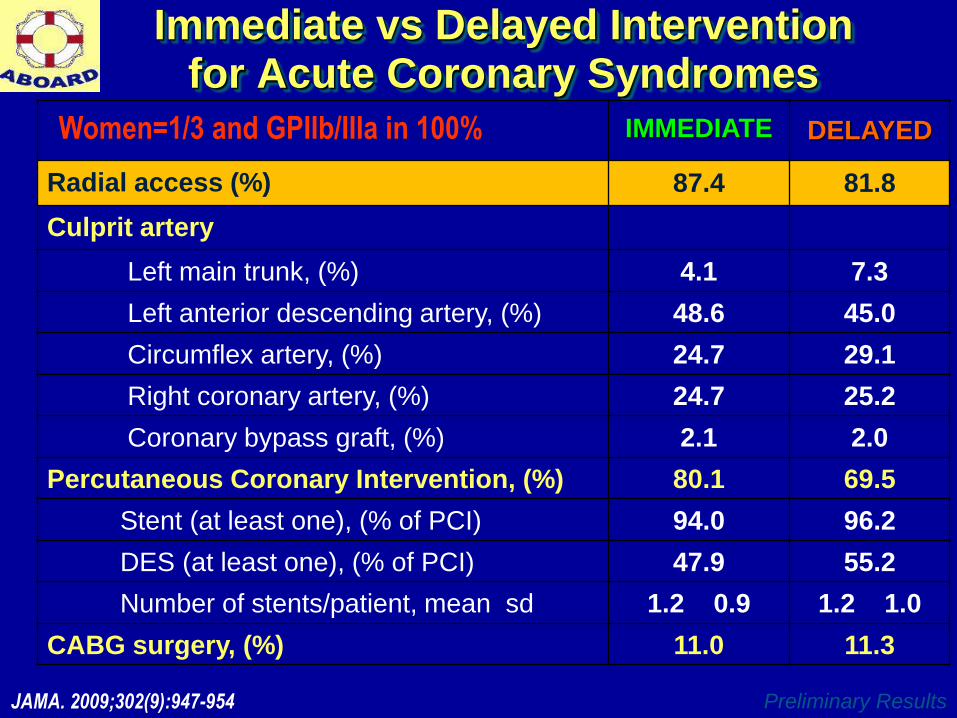
Immediate vs Delayed Intervention for Acute Coronary Syndromes
IMMEDIATE DELAYED
Radial access (%) 87.4 81.8
Culprit artery
Left main trunk, (%) 4.1 7.3
Left anterior descending artery, (%) 48.6 45.0
Circumflex artery, (%) 24.7 29.1
Right coronary artery, (%) 24.7 25.2
Coronary bypass graft, (%) 2.1 2.0
Percutaneous Coronary Intervention, (%) 80.1 69.5
Stent (at least one), (% of PCI) 94.0 96.2
DES (at least one), (% of PCI) 47.9 55.2
Number of stents/patient, mean
sd 1.2
0.9 1.2
1.0
CABG surgery, (%) 11.0 11.3
JAMA. 2009;302(9):947-954
Women=1/3 and GPIIb/IIIa in 100%
Preliminary Results
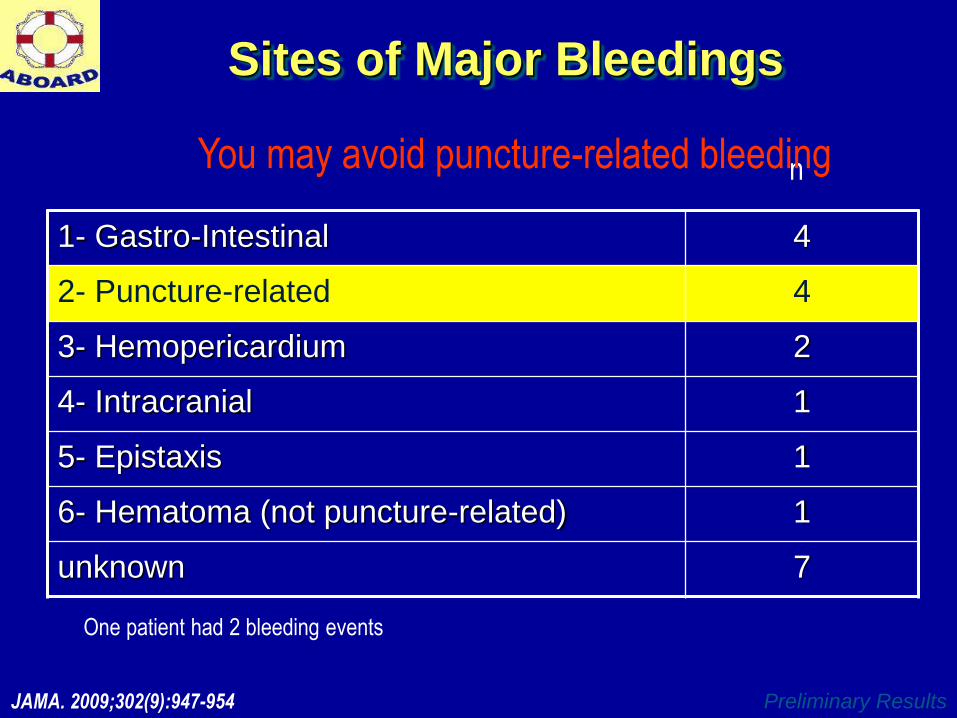
Sites of Major Bleedings
1- Gastro-Intestinal 4
2- Puncture-related 4
3- Hemopericardium 2
4- Intracranial 1
5- Epistaxis 1
6- Hematoma (not puncture-related) 1
unknown 7
One patient had 2 bleeding events
n
JAMA. 2009;302(9):947-954
You may avoid puncture-related bleeding
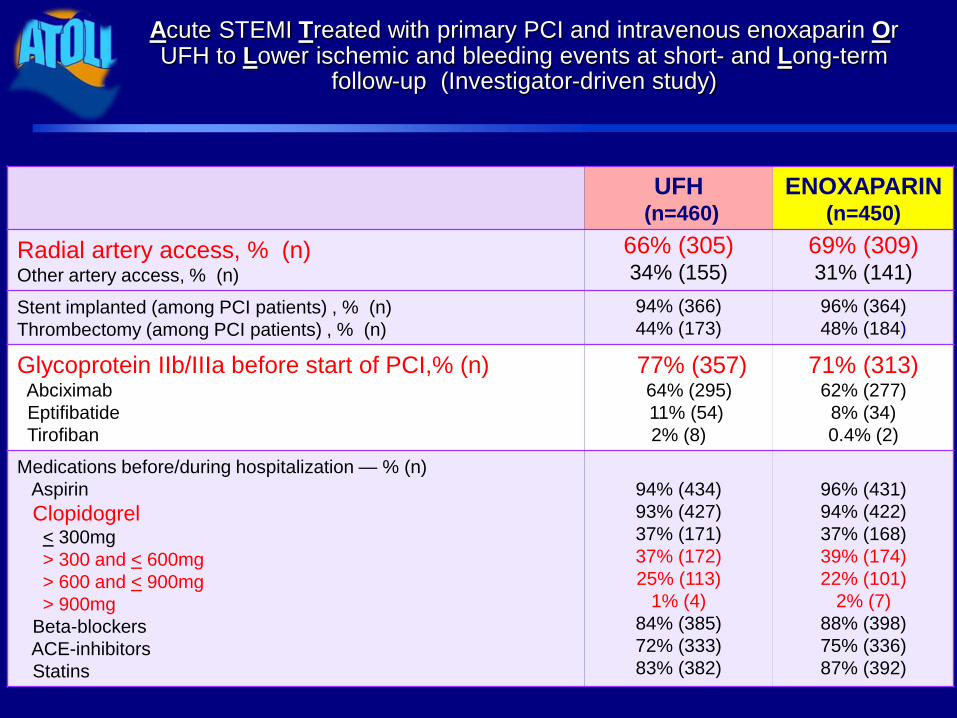
Acute STEMI Treated with primary PCI and intravenous enoxaparin Or UFH to Lower ischemic and bleeding events at short- and Long-term
follow-up (Investigator-driven study)
UFH (n=460)
ENOXAPARIN (n=450)
Radial artery access, % (n) Other artery access, % (n)
66% (305) 34% (155)
69% (309) 31% (141)
Stent implanted (among PCI patients) , % (n)
Thrombectomy (among PCI patients) , % (n)
94% (366)
44% (173)
96% (364)
48% (184)
Glycoprotein IIb/IIIa before start of PCI,% (n) Abciximab
Eptifibatide
Tirofiban
77% (357) 64% (295)
11% (54)
2% (8)
71% (313) 62% (277)
8% (34)
0.4% (2)
Medications before/during hospitalization — % (n)
Aspirin
Clopidogrel < 300mg
> 300 and < 600mg
> 600 and < 900mg
> 900mg
Beta-blockers
ACE-inhibitors
Statins
94% (434)
93% (427)
37% (171)
37% (172)
25% (113)
1% (4)
84% (385)
72% (333)
83% (382)
96% (431)
94% (422)
37% (168)
39% (174)
22% (101)
2% (7)
88% (398)
75% (336)
87% (392)
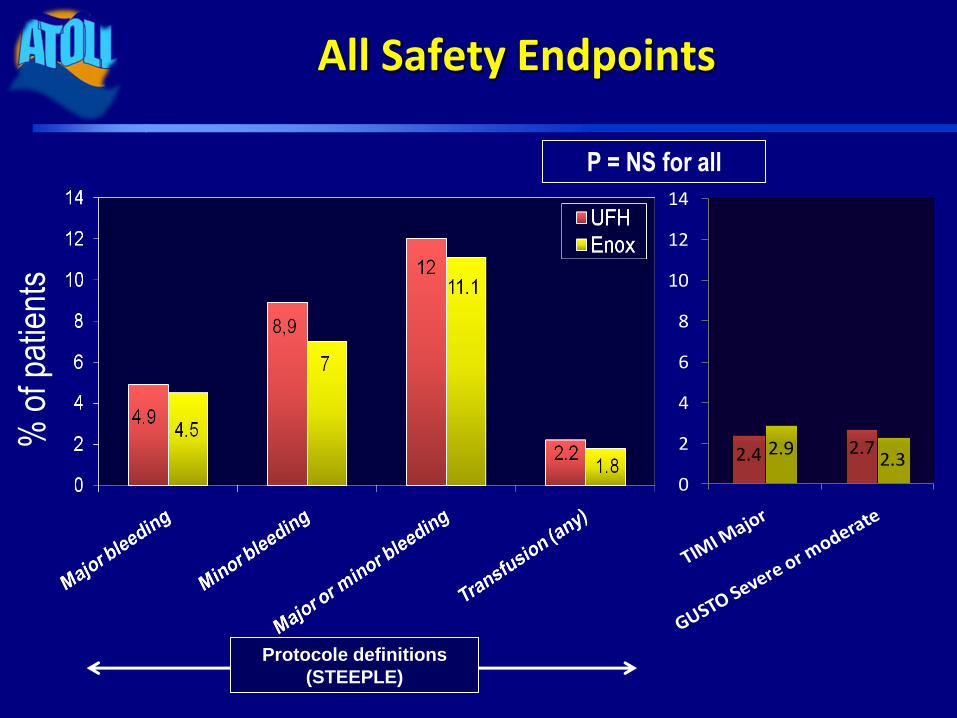
All Safety Endpoints %
of p
atie
nts
P = NS for all
Protocole definitions
(STEEPLE)
2.4 2.72.92.3
0
2
4
6
8
10
12
14
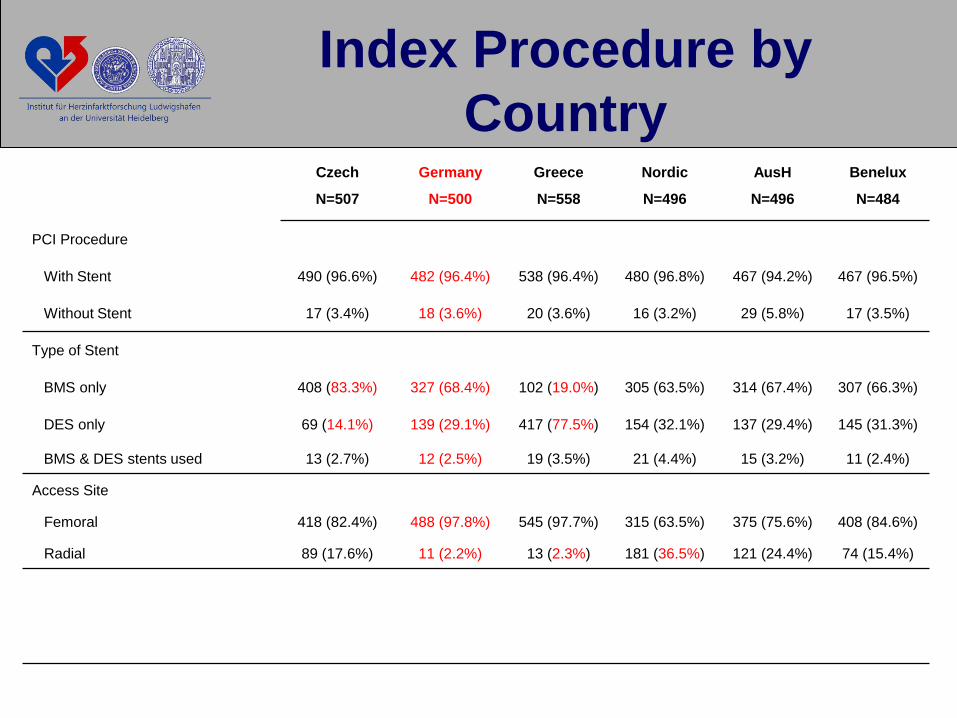
Index Procedure by
Country Czech
N=507
Germany
N=500
Greece
N=558
Nordic
N=496
AusH
N=496
Benelux
N=484
PCI Procedure
With Stent 490 (96.6%) 482 (96.4%) 538 (96.4%) 480 (96.8%) 467 (94.2%) 467 (96.5%)
Without Stent 17 (3.4%) 18 (3.6%) 20 (3.6%) 16 (3.2%) 29 (5.8%) 17 (3.5%)
Type of Stent
BMS only 408 (83.3%) 327 (68.4%) 102 (19.0%) 305 (63.5%) 314 (67.4%) 307 (66.3%)
DES only 69 (14.1%) 139 (29.1%) 417 (77.5%) 154 (32.1%) 137 (29.4%) 145 (31.3%)
BMS & DES stents used 13 (2.7%) 12 (2.5%) 19 (3.5%) 21 (4.4%) 15 (3.2%) 11 (2.4%)
Access Site
Femoral 418 (82.4%) 488 (97.8%) 545 (97.7%) 315 (63.5%) 375 (75.6%) 408 (84.6%)
Radial 89 (17.6%) 11 (2.2%) 13 (2.3%) 181 (36.5%) 121 (24.4%) 74 (15.4%)
What is the priority?
−Identify reasons for non adoption
−Set up An European Radial Program
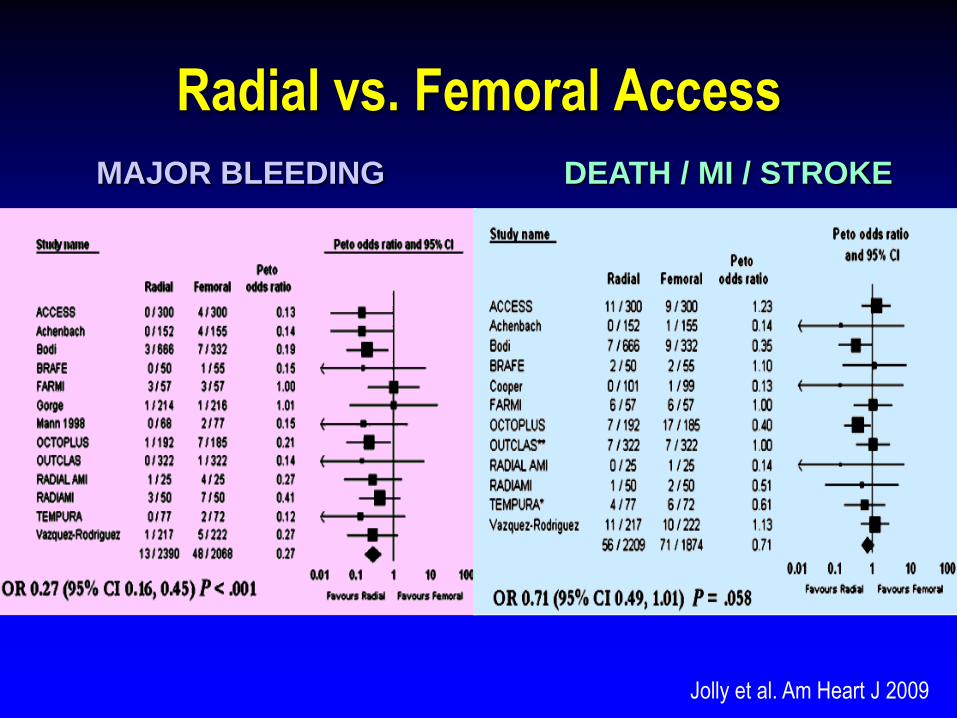
Radial vs. Femoral Access
Jolly et al. Am Heart J 2009
MAJOR BLEEDING DEATH / MI / STROKE
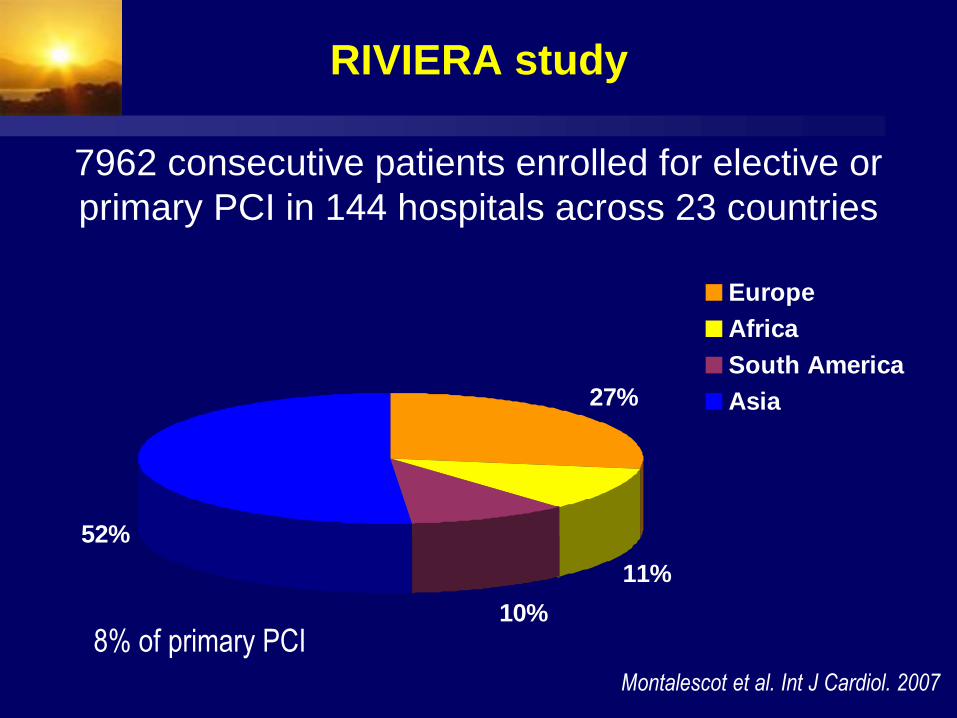
RIVIERA study
27%
11%
10%
52%
Europe
Africa
South America
Asia
7962 consecutive patients enrolled for elective or
primary PCI in 144 hospitals across 23 countries
Montalescot et al. Int J Cardiol. 2007
8% of primary PCI
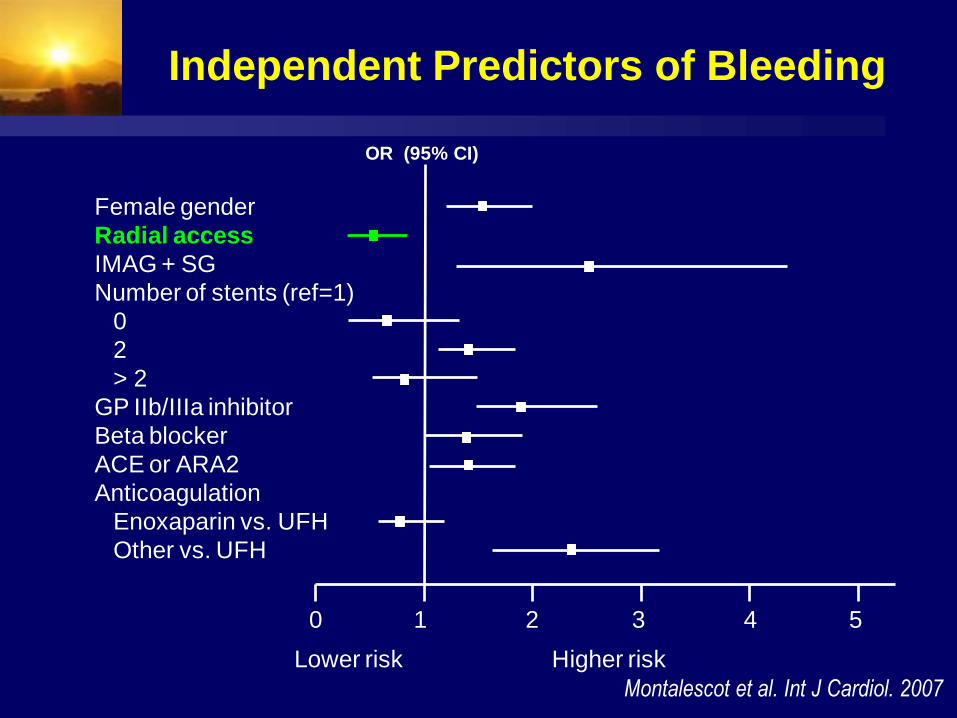
Independent Predictors of Bleeding
Female gender
Radial access
IMAG + SG
Number of stents (ref=1)
0
2
> 2
GP IIb/IIIa inhibitor
Beta blocker
ACE or ARA2
Anticoagulation
Enoxaparin vs. UFH
Other vs. UFH
Lower risk Higher risk
0 1 2 3 4 5
OR (95% CI)
Montalescot et al. Int J Cardiol. 2007
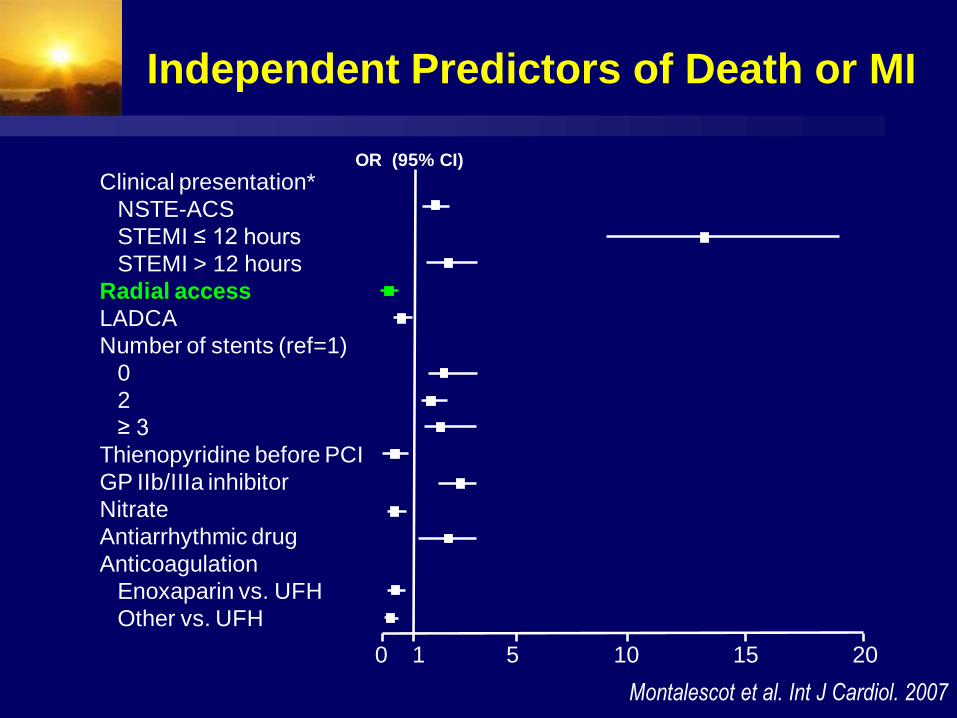
Independent Predictors of Death or MI
Clinical presentation*
NSTE-ACS
STEMI ≤ 12 hours
STEMI > 12 hours
Radial access
LADCA
Number of stents (ref=1)
0
2
≥ 3
Thienopyridine before PCI
GP IIb/IIIa inhibitor
Nitrate
Antiarrhythmic drug
Anticoagulation
Enoxaparin vs. UFH
Other vs. UFH
0 1 5 10 15 20
OR (95% CI)
Montalescot et al. Int J Cardiol. 2007
Reasons for adoption of radial Patient preference (comfort)
Shortens hospitalization (day case PCI program)
“New” technical aspects of PCI, widely applicable
Literature shows improved outcomes
Cost = 0
Reasons for non-adoption of radial
Lack of teachers
Learning curve
Spasm (nitrates/calcium blockers)
Tortuosities (technical skills and tricks)
Occlusion (anticoagulation + 5/6F catheters)
Radial vs femoral in STEMI non-randomized
Similar procedural success
More dual access site required with radial
Similar procedure time
Contrast and radiation less with radial
Shorter length of stay with radial
Hetherington et al. Heart, 2009
Conclusions
A radial program starts with coronary angios, then elective PCI
When learning curve is finished, and radial used in more than 2/3 of scheduled cases, no reason not to perform radial primary PCI
The benefits seen in elective PCI are even more obvious in primary PCI
Femoral access limited to specific cases





![BLINDED EVALUATIONS OF EFFECT SIZES IN CLINICAL TRIALS ... 2013 Turkoz.pdf · endpoints in addition to sample size re-estimation • Blinded treatment effects for survival endpoints[7]](https://static.fdocuments.in/doc/165x107/608545b9f250640ece537beb/blinded-evaluations-of-effect-sizes-in-clinical-trials-2013-turkozpdf-endpoints.jpg)











