
Triage, Assessment and Treatment Planning · Triage, Assessment and Treatment Planning Prepared by...
19
Triage, Assessment and Treatment Planning Prepared by Todd Sakakibara MD, CCFP, FCFP Clinical Assistant Professor, Dept. Family Practice UBC Diplomate of the American Board of Addiction Medicine
Transcript of Triage, Assessment and Treatment Planning · Triage, Assessment and Treatment Planning Prepared by...

Triage, Assessment and Treatment Planning Prepared by Todd Sakakibara MD, CCFP, FCFP Clinical Assistant Professor, Dept. Family Practice UBC Diplomate of the American Board of Addiction Medicine
College of Physicians and Surgeons of British Columbia 2
Triage • A thorough workup will allow you to recommend the best treatment options
• Determine patient expectations/goals
• Multiple ways to treat an opioid use disorder (informed consent)
• Methadone may not necessarily be the best option
• Opioid history: Type, amount, route, frequency, last use
• Establish diagnosis for ORT: Opioid use disorder with physical dependence, rare exceptions (e.g. exiting incarceration)
• Other substances: Use vs. substance use disorders
• Other history: Detoxification, recovery, abstinence
College of Physicians and Surgeons of British Columbia 3
Triage • Consider – age of the patient and duration of opioid use, parents, consent
• Past medical history: HIV, HCV, pain, pregnancy
• Psych: Suicide attempts, psychosis, violence
• Current medications, allergies
• Problems with previous detoxes or ORT
• Motivation: Stage of change
College of Physicians and Surgeons of British Columbia 4
Triage decision tree • Outpatient detox: Healthy, supports, low risk for complications
• In-patient detox: Physical, psychological, social problems
• Offer naltrexone after detox +/- treatment centre
• Warn of OD risk post detox
• Methadone or Suboxone taper: the longer the better
• Methadone or Suboxone maintenance:
– May have previously trialed in-patient/outpatient detox
– Social issues which preclude detox
– Pregnant, HIV+, HCV+, or other urgent medical issue
College of Physicians and Surgeons of British Columbia 5
Triage to opioid replacement therapy (ORT) At the end of the triage: • Order a urine drug screen (UDS) or do a point of care (POC) UDS
• Include any speciality drugs taken in the past or suspected
• +/- urine bHCG
• Bloodwork:
– AST, ALT, GGT, HIV, Hep ABC, CBC, RPR, etc…
– +/- TB skin test
• Consider an ECG
College of Physicians and Surgeons of British Columbia 6
Assessment • Fill in details of addiction history
– Each substance first use, amount, route, frequency, diagnosis
– Community supports utilized – NA, AA, Matrix, 1:1
– Flesh out the recovery and treatment history
• Medical history: Include accidents and surgeries
• Mental health history: Diagnosis, treatment, medications, symptoms
• Family history: Draw tree (drug and alcohol, psychiatric issues)
• Social history:
– Legal, vocational/schooling, partner, roommates/family
College of Physicians and Surgeons of British Columbia 7
Assessment Physical exam: • vitals, pupils, autonomic signs, nasal septum, dentition, murmurs, liver,
tracks, jaundice, tattoos, piercings, mental status exam
– Opioid use: Small pupils, somnolent, tracks, RR
– Opioid withdrawal: Lacrimation, salivation, piloerection, temperature dysregulation, hyper-reflexic and agitated, pain all over, nausea, vomiting, diarrhoea
• Review lab work
• Collateral: Family, other MDs, PharmaNet, pharmacist
College of Physicians and Surgeons of British Columbia 8
Assessment • Review treatment agreement with patient and witness their signature
• Have them sign permission to communicate with the other MDs/health-care providers involved
• Warn of overdose risks when initiating and stopping methadone, and drug interactions
• Offer Narcan kit
• After the complete workup you may write the first methadone or Suboxone prescription
• Document everything you have covered
College of Physicians and Surgeons of British Columbia 9
Management of ongoing substance use in the context of methadone/Suboxone® maintenance • Concurrent heroin and other opioid use
• Alcohol
• Stimulants
• Benzodiazepines/zopiclone
• THC
College of Physicians and Surgeons of British Columbia 10
Concurrent heroin and other opioid use • During induction
– Adjust methadone/Suboxone
– Counselling
– Appropriate monitoring
• Episodic relapses
– Review dose
– Re-evaluate daily supervised dispensing
– Counselling to address relevant issues
– Appropriate monitoring
College of Physicians and Surgeons of British Columbia 11
Alcohol use • Screen for an alcohol use disorder
• Alcohol use is a concern with ORT
– Interaction with methadone/Suboxone
– Increased sedation and respiratory depression
• Treatment plan for alcohol use disorders is mandatory if ORT maintenance is to be continued
• Uncontrolled alcoholism may be an indication to withdraw from methadone maintenance
• BCMA Guideline: Office Based Management of Problem Drinking (www.bcguidelines.ca)
• Consider acamprosate, gabapentin
College of Physicians and Surgeons of British Columbia 12
Stimulant use Increasing incidence of cocaine and methamphetamine use • Destabilizing with methadone maintenance
• Treatment is cognitive/behavioural intervention
– Counselling
– Support services
– Relevant treatment contract
• Consider in-patient treatment
• Consider contingency management
• Determine if stimulant is the primary drug of abuse/dependence before initiating methadone maintenance
College of Physicians and Surgeons of British Columbia 13
Benzodiazepine and zopiclone use • Chronic benzodiazepine use is a concern in substance-dependent
individuals
• Outcome worse with methadone maintenance when benzodiazepines are concurrently used
• Overdose risk significant
• Screen at assessment
– Treatment plan
– Refer to Ashton manual for withdrawal procedure
– Screen and PharmaNet
College of Physicians and Surgeons of British Columbia 14
Marijuana use Screen for marijuana use disorder at initial assessment • Treatment plan
• Treatment contract
• Outline expectations
College of Physicians and Surgeons of British Columbia 15
Improving outcomes If unable to document benefits after dose adjustment and appropriate psychosocial intervention, consider alternate treatment. • Switch ORT
• Taper ORT
• Intensive outpatient treatment
• Residential/intensive in-patient treatment
• Support group (AA/NA/SMART/16 Steps etc.)
• Addiction medicine consult
College of Physicians and Surgeons of British Columbia 16
Imagery
• Overall rate of sustained successful taper: 4.4% among all episodes initiating a taper and 2.5% among all completed episodes.
• Longer tapers had higher odds of success [12-52 weeks versus <12 weeks (OR: 3.58 (2.76-4.65); >52 weeks versus <12 weeks: (6.68 (5.13-8.70)).
• A gradual, stepped tapering schedule, with dose decreases scheduled in only 25-50% of the weeks of the taper, provided the highest odds of sustained success (vs. <25%: (1.61 (1.22-2.14)).
Nosyk et al, Addiction 2012; 107(9):1621-9.
College of Physicians and Surgeons of British Columbia 17
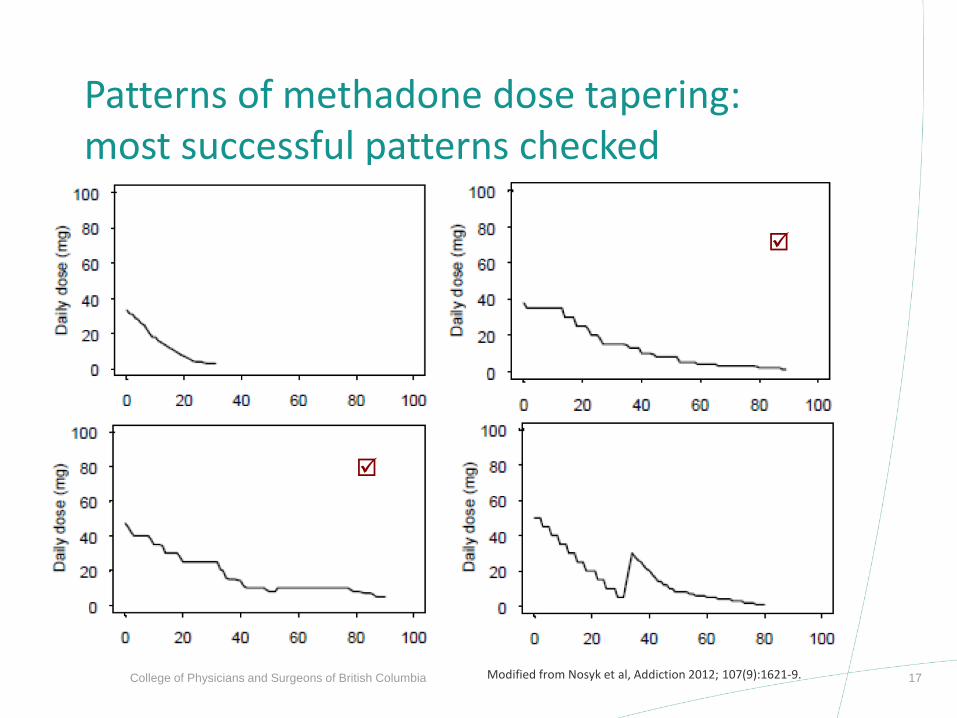
Patterns of methadone dose tapering: most successful patterns checked
Modified from Nosyk et al, Addiction 2012; 107(9):1621-9.
College of Physicians and Surgeons of British Columbia 18
Transfers/cessation of treatment If patient transfers to alternate ORT provider • Communication between new and current physician required prior to
transfer – preferably by phone; otherwise valuable information is lost and therapeutic interventions can be undermined
• Records should then be transferred and reviewed when accepting the client long term
College of Physicians and Surgeons of British Columbia 19
Summary Consistent application of basic set of principles results in: • Improved patient care
• Containment of overall risk to patient/public
• Reduced conflict during visits
• Reduced risk of coroner’s cases
Well done!


















