Trends in the Indications for Penetrating Keratoplasty in the … · 2020. 5. 13. · Trends in the...
4
Trends in the Indications for Penetrating Keratoplasty in the Midwestern United States Kendall R.B. Dobbins, M.D., Francis W. Price, Jr., M.D., and William E. Whitson, M.D. Purpose. To examine the leading indications and identify the changing trends for penetrating keratoplasty (PKP) in the midwest- ern United States. Methods. The indications for PKPs at a single center tertiary care referral practice were tabulated to assess trends from 1982 to 1996. The data analysis was prospective after 1985. Age, gender, clinical indication for PKP, date of surgery, status of the lens at the time of surgery (phakic, aphakic, pseudophakic, cataract), and any secondary diagnoses were recorded. In pseudo- phakic eyes, the type of intraocular lens (IOL) present at the time of surgery was noted. Correlation analysis and linear regression were used in the SAS system, version 6.12, to test for the statistical significance in increasing or decreasing trends over the span of the study. Results. A total of 4,217 PKPs were performed on 3,263 patients. The leading indication for PKP was pseudophakic bullous keratopathy (31.5%), with 73% of these cases associated with an anterior chamber IOL, 21% associated with a posterior chamber IOL, and 6% associated with an iris-fixated IOL. Fuchs’ dystrophy (23.2%), keratoconus (11.4%), corneal scarring (11.2%), failed graft (8.9%), and aphakic bullous keratopathy (7.5%) followed pseudophakic bullous keratopathy in frequency. These six groups accounted for approximately 93% of all cases performed. There were significant increasing trends in the incidence of failed grafts (p 0.0001) and corneal scarring (p 0.0001), and decreasing trends in the incidence of aphakic bullous keratopathy (p 0.0001). There was a significant decreasing trend in pseudophakic bullous keratopathy from 1989 to 1996 (p 0.0031). Conclu- sions. Pseudophakic bullous keratopathy was the leading indica- tion for PKP in our series. This is in agreement with the data reported in other similar studies done in North America. However, unlike most of these studies, our second leading indication was Fuchs’ dystrophy. This contrast may be secondary to different genetic demographics in the midwestern United States. Key Words: Penetrating keratoplasty—Bullous keratopathy— Fuchs’ dystrophy—Keratoconus—Corneal scarring—Failed graft. Corneal transplants have become the most successful tissue transplant secondary to advances in ocular immunology, ocular pharmacology, surgical instrument technology, surgical tech- niques, corneal storage, and eye banking procedures. 1 Over time, the leading indications for corneal transplants have changed. Be- fore the mid-1970s, keratoconus and regrafts were the primary indications for corneal transplants. 2,3 Since then, according to most North American studies, bullous keratopathy has become the lead- ing cause for penetrating keratoplasty (PKP), with the advent of cataract extraction and placement of intraocular lenses (IOLs). However, with the advancements in surgical techniques for cata- ract surgery and (IOL) technology, the incidence of post-cataract surgery bullous keratopathy is decreasing and is actually no longer the primary indication for corneal transplantation in a few regions (Europe and Australia). The objective of this study was to examine the leading indications and identify the changing trends for PKP at a large referral center in the midwestern United States. METHODS From July 1982 through 1996, a total of 4,217 PKPs were per- formed at the Corneal Consultants of Indiana, in Indianapolis, IN, U.S.A. The Corneal Consultants of Indiana is a tertiary referral center for cornea, anterior segment, and refractive surgery. Patients are referred to this practice primarily from Indiana and surround- ing midwestern states by both ophthalmologists and optometrists. The data collection was retrospective from 1982 to 1985 and prospective from 1986 to 1996. The age, gender, clinical indication for PKP, date of surgery, status of the lens at the time of surgery (phakic, aphakic, pseudophakic, or cataract), and any secondary diagnoses were recorded. As well, in the pseudophakic eyes, the type of IOL present at the time of surgery was documented. Indications for PKPs were divided into 28 categories. These were consolidated into six groups: bullous keratopathy (divided mainly into pseudophakic and aphakic); Fuchs’ dystrophy; kera- toconus; corneal scarring; failed graft; and other, which consisted of corneal ulcer, herpes keratitis, interstitial keratitis, disciform keratitis, phakic bullous keratopathy, lattice dystrophy, granular dystrophy, macular dystrophy, posterior polymorphous dystrophy, iridocorneal endothelial syndrome, perforated cornea, wound de- hiscence, corneal melt, keratoglobus, pellucid marginal degenera- tion, band keratopathy, aniridia, pemphigoid, lipid keratopathy, spheroidal degeneration, corneal blood staining, and iris tumor. In most instances, only one clinical diagnosis was present. In situations in which there was a secondary diagnosis for cases that required a regraft, the diagnosis of failed graft was given. In situ- ations in which the patient had the diagnosis of both bullous ker- atopathy and Fuchs’ dystrophy, bullous keratopathy was the pri- mary diagnosis selected in pseudophakic patients and Fuchs’ dys- trophy was the primary diagnosis selected in phakic patients. Submitted January 8, 2000. Revision received March 20, 2000. Ac- cepted March 27, 2000. From the Cornea Research Foundation of America, Indianapolis, Indi- ana, U.S.A. Address correspondence and reprint requests to Dr. K.R.B. Dobbins, Corneal Consultants of Indiana, 9002 N. Meridian Street, Suite 100, In- dianapolis, IN 46260, U.S.A. Cornea 19(6): 813–816, 2000. © 2000 Lippincott Williams & Wilkins, Inc., Philadelphia 813
Transcript of Trends in the Indications for Penetrating Keratoplasty in the … · 2020. 5. 13. · Trends in the...
-
Trends in the Indications for PenetratingKeratoplasty in the Midwestern United States
Kendall R.B. Dobbins, M.D., Francis W. Price, Jr., M.D., andWilliam E. Whitson, M.D.
Purpose. To examine the leading indications and identify thechanging trends for penetrating keratoplasty (PKP) in the midwest-ern United States. Methods. The indications for PKPs at a singlecenter tertiary care referral practice were tabulated to assess trendsfrom 1982 to 1996. The data analysis was prospective after 1985.Age, gender, clinical indication for PKP, date of surgery, status ofthe lens at the time of surgery (phakic, aphakic, pseudophakic,cataract), and any secondary diagnoses were recorded. In pseudo-phakic eyes, the type of intraocular lens (IOL) present at the timeof surgery was noted. Correlation analysis and linear regressionwere used in the SAS system, version 6.12, to test for the statisticalsignificance in increasing or decreasing trends over the span of thestudy. Results. A total of 4,217 PKPs were performed on 3,263patients. The leading indication for PKP was pseudophakic bullouskeratopathy (31.5%), with 73% of these cases associated with ananterior chamber IOL, 21% associated with a posterior chamberIOL, and 6% associated with an iris-fixated IOL. Fuchs’ dystrophy(23.2%), keratoconus (11.4%), corneal scarring (11.2%), failedgraft (8.9%), and aphakic bullous keratopathy (7.5%) followedpseudophakic bullous keratopathy in frequency. These six groupsaccounted for approximately 93% of all cases performed. Therewere significant increasing trends in the incidence of failed grafts(p � 0.0001) and corneal scarring (p � 0.0001), and decreasingtrends in the incidence of aphakic bullous keratopathy (p �0.0001). There was a significant decreasing trend in pseudophakicbullous keratopathy from 1989 to 1996 (p � 0.0031). Conclu-sions. Pseudophakic bullous keratopathy was the leading indica-tion for PKP in our series. This is in agreement with the datareported in other similar studies done in North America. However,unlike most of these studies, our second leading indication wasFuchs’ dystrophy. This contrast may be secondary to differentgenetic demographics in the midwestern United States.Key Words: Penetrating keratoplasty—Bullous keratopathy—Fuchs’ dystrophy—Keratoconus—Corneal scarring—Failed graft.
Corneal transplants have become the most successful tissuetransplant secondary to advances in ocular immunology, ocularpharmacology, surgical instrument technology, surgical tech-niques, corneal storage, and eye banking procedures.1 Over time,the leading indications for corneal transplants have changed. Be-
fore the mid-1970s, keratoconus and regrafts were the primaryindications for corneal transplants.2,3 Since then, according to mostNorth American studies, bullous keratopathy has become the lead-ing cause for penetrating keratoplasty (PKP), with the advent ofcataract extraction and placement of intraocular lenses (IOLs).However, with the advancements in surgical techniques for cata-ract surgery and (IOL) technology, the incidence of post-cataractsurgery bullous keratopathy is decreasing and is actually no longerthe primary indication for corneal transplantation in a few regions(Europe and Australia). The objective of this study was to examinethe leading indications and identify the changing trends for PKP ata large referral center in the midwestern United States.
METHODS
From July 1982 through 1996, a total of 4,217 PKPs were per-formed at the Corneal Consultants of Indiana, in Indianapolis, IN,U.S.A. The Corneal Consultants of Indiana is a tertiary referralcenter for cornea, anterior segment, and refractive surgery. Patientsare referred to this practice primarily from Indiana and surround-ing midwestern states by both ophthalmologists and optometrists.
The data collection was retrospective from 1982 to 1985 andprospective from 1986 to 1996. The age, gender, clinical indicationfor PKP, date of surgery, status of the lens at the time of surgery(phakic, aphakic, pseudophakic, or cataract), and any secondarydiagnoses were recorded. As well, in the pseudophakic eyes, thetype of IOL present at the time of surgery was documented.
Indications for PKPs were divided into 28 categories. Thesewere consolidated into six groups: bullous keratopathy (dividedmainly into pseudophakic and aphakic); Fuchs’ dystrophy; kera-toconus; corneal scarring; failed graft; and other, which consistedof corneal ulcer, herpes keratitis, interstitial keratitis, disciformkeratitis, phakic bullous keratopathy, lattice dystrophy, granulardystrophy, macular dystrophy, posterior polymorphous dystrophy,iridocorneal endothelial syndrome, perforated cornea, wound de-hiscence, corneal melt, keratoglobus, pellucid marginal degenera-tion, band keratopathy, aniridia, pemphigoid, lipid keratopathy,spheroidal degeneration, corneal blood staining, and iris tumor.
In most instances, only one clinical diagnosis was present. Insituations in which there was a secondary diagnosis for cases thatrequired a regraft, the diagnosis of failed graft was given. In situ-ations in which the patient had the diagnosis of both bullous ker-atopathy and Fuchs’ dystrophy, bullous keratopathy was the pri-mary diagnosis selected in pseudophakic patients and Fuchs’ dys-trophy was the primary diagnosis selected in phakic patients.
Submitted January 8, 2000. Revision received March 20, 2000. Ac-cepted March 27, 2000.
From the Cornea Research Foundation of America, Indianapolis, Indi-ana, U.S.A.
Address correspondence and reprint requests to Dr. K.R.B. Dobbins,Corneal Consultants of Indiana, 9002 N. Meridian Street, Suite 100, In-dianapolis, IN 46260, U.S.A.
Cornea 19(6): 813–816, 2000. © 2000 Lippincott Williams & Wilkins, Inc., Philadelphia
813
-
Correlation analysis and linear regression were used in the SASsystem, version 6.12, to test for the statistical significance in in-creasing or decreasing trends in the indications for PKP over thespan of the study.
RESULTS
A total of 4,217 PKPs were performed on 3,263 patients. Table1 categorizes these transplants by diagnosis and year performed.An average of 299 corneal transplants was performed each fullyear of the study, ranging from 36 in 1983, to 430 in 1990. Theaverage age of all patients was 67. The mean age of the kerato-conus patients was 41 years, which was significantly lower thanthe mean age in the other main groups. As seen in Table 2, of the4,217 cases, 2,677 were female and 1,540 were male (ratio of 7:4).There were four times as many female Fuchs’ dystrophy patientsrequiring PKP than males (783 vs. 195). There were 188 femalekeratoconus patients who received PKP versus 293 males, givinga male preponderance, which is different than that observed in themajority of studies4 but similar to the ratio reported by Liu andSlomovic.5
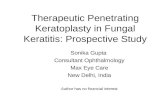
The leading indications for PKP in our study in decreasing orderwere pseudophakic bullous keratopathy (31.5%), Fuchs’ dystrophy(23.2%), keratoconus (11.4%), corneal scarring (11.2%), failedgraft (8.9%), and aphakic bullous keratopathy (7.5%), (Table 1;Fig. 1). These six groups account for approximately 93% of alloperations performed. Pseudophakic bullous keratopathy was themost common indication for PKP for 11 of the 15 years (Table 1;Fig. 2).
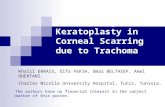
There was a significant decreasing trend in pseudophakic bul-lous keratopathy from 1989 to 1996 (p � 0.0031), as can be seenin Fig. 2. Review of the position of the IOL in pseudophakicbullous keratopathy revealed that anterior chamber IOLs were themost common (73%), with posterior chamber IOLs following at21%, and iris-fixated IOLs at 6%. In three cases, the type of IOLwas not recorded.
The second and third most common indications for PKP wereFuchs’ dystrophy and keratoconus. There was little change in thefrequency of cases in these groups over the course of the study.
The fourth and fifth most common indications were cornealscarring and failed graft, both of which showed significant increas-ing trends (p � 0.0001 for both) over the span of the study (Fig.2). Finally, aphakic bullous keratopathy was our sixth most com-mon indication, with a significant decreasing trend throughout thestudy (p � 0.0001).
DISCUSSION
In this study, we evaluated the indications for PKPs in 4,217cases in the midwestern United States over a 15-year time span.
There has never been a study of this type performed in this locale.This is also one of the largest studies of this kind ever done,surpassed only by a similar study done at Wills Eye Hospital inPhiladelphia, PA, U.S.A.,6,7 and by the Australian Corneal GraftRegistry. Wills Eye reported two studies that spanned a total of 13years and involved a total of 4,741 cases. The Australian CornealGraft Registry has an ongoing database of PKPs performed inAustralia. The database was last reported to be at 8,092 in October1997.8 However, the last reported study evaluating the indicationsfor PKP with these data only involved 3,608 cases.9 To our knowl-edge, we have the only ongoing corneal transplant database in theUnited States.
Pseudophakic bullous keratopathy was by far the most com-mon indication in our study. This is in agreement with the majorityof North American studies of this nature done in the past 15years.1,5–7,10–14 Three North American studies and most Europeanand Australian studies had keratoconus as their leading indicationfor PKPs.9,15–23 One of the three North American studies actuallyhad bullous keratopathy as the leading indication, but when thisgroup was divided into pseudophakic and aphakic, keratoconuswas the leading indication.17
There was a significant decreasing frequency in pseudophakicbullous keratopathy from 1989 to 1996 (p � 0.0031). This de-creasing trend was also shown by Liu and Slomovic5 and Mamaliset al.15 This was different from the data from Lois et al. (Wills EyeHospital),6 in which the frequency of pseudophakic bullous kera-topathy had essentially remained unchanged (1985–1995), andRamsay et al. (Scotland),24 where the frequency was actually in-creasing through to the end of the study in 1995.
With the significant advancements in cataract surgery tech-niques, the incidence of intraoperative surgical complications andthe use of anterior chamber IOLs have declined. Also, the creationand use of viscoelastics during cataract surgery have had a sig-nificant effect on decreasing intraoperative trauma to the cornealendothelium. Furthermore, with improving IOL technology, cor-neas are tolerating IOLs much better. Because of this, many be-lieve that the incidence of pseudophakic bullous keratopathyshould be decreasing. Our data support this theory.
Anterior chamber IOLs were by far the most common type oflens found in the pseudophakic bullous keratopathy cases, at 73%.This indicates that IOL position is a significant risk factor forthe development of pseudophakic bullous keratopathy. Therewas a significant shift from the use of anterior chamber IOLs toposterior chamber IOLs in the mid-1980s.25 However, there seemsto be a significant lag time between anterior chamber IOL implan-tation and explantation, the average time being 8 years, as reportedby Price et al.26 Thus, although anterior chamber IOLs willcontinue to be a significant cause of pseudophakic bullous kera-topathy, their contribution should decrease with time as we move
TABLE 1. PKP trends (total numbers)
1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 Totals
PBK 9 11 29 56 81 108 141 138 154 136 123 100 108 82 51 1,327 (31.5%)Fuchs’ 5 10 27 38 48 59 70 61 80 101 111 115 90 83 80 978 (23.2%)KCN 3 4 10 16 15 29 33 50 48 45 41 58 45 47 37 481 (11.4%)Corneal scar 2 2 12 10 18 27 36 34 48 39 48 54 58 51 35 474 (11.2%)Failed graft 2 0 7 4 12 22 32 16 33 41 42 44 42 45 34 376 (8.9%)ABK 4 9 31 28 22 30 35 24 37 28 15 18 16 12 8 317 (7.5%)Other 0 0 9 11 13 14 16 13 30 16 19 26 31 28 38 264 (6.3%)Total 25 36 125 163 209 289 363 336 430 406 399 415 390 348 283 4,217 (total)
PBK indicates pseudophakic bullous keratopathy; KCN, keratoconus; ABK, aphakic bullous keratopathy.
K.R.B. DOBBINS ET AL.814
Cornea, Vol. 19, No. 6, 2000
-
further past the mid-1980s and with better anterior chamber IOLtechnology.
The fact that 27% of the cases had posterior chamber IOLs oriris-fixed IOLs reveals that the position of the IOL is not the onlyrisk factor for developing pseudophakic bullous keratopathy. Otherfactors that have been shown to contribute are low endothelial cellcount, corneal guttata, previous ocular surgery, chronic uveitis,intraoperative trauma, drug toxicity, peripheral anterior synechiae,and a shallow anterior chamber.4
What makes our study different from most of the other similarstudies throughout the world is that our second most commonindication for PKP was Fuchs’ dystrophy. Only the combinedWills Eye Hospital studies6,7 and a study from Denmark by Haa-mann et al.27 also had Fuchs’ dystrophy as the second indication.Most other studies had Fuchs’ dystrophy ranked fourth, fifth, orsixth. There was no observable trend in the incidence of Fuchs’dystrophy over the span of the study. As mentioned earlier, therewere four times as many female Fuchs’ patients requiring PKP asthere were males (783 vs. 195), which is similar to what waspreviously reported.4 Because Fuchs’ dystrophy is a disease of theelderly, it was thought that age may be a significant factor in thedisparity of the occurrence of Fuchs’ dystrophy in men andwomen, because, on average, women live longer. However, al-though our data show that the ratio of women to men who werediagnosed with Fuchs’ dystrophy under the age of 65 is less thanthe totals reported above, at three to one (177 vs. 59), there is stilla significant difference, and thus age only partially contributes tothis disparity.
Although keratoconus was the leading indication for PKP in a
significant number of studies,9,15–23 it was third in our study. Thereason for this discrepancy is unclear. Variations in success ofcontact lens fittings or contact lens intolerance secondary to cli-matic factors may have had an influence. The discrepancy mayalso be secondary to different genetic demographics. There was nosignificant trend in the frequency throughout our study.
Corneal scarring was our fourth most common indication, witha significant increasing trend throughout the study (p � 0.0001).Failed graft was our fifth most common indication, also with asignificant increase in incidence throughout the study (p �0.0001). Previous graft failure and young age are risk factors forcorneal graft failure.28 The average age of patients in the cornealscarring group was 58, which is well below the average of allpatients (67 years) in our study. Thus, as the corneal scarring andfailed graft groups increase, this further contributes to the increas-ing trend of failed grafts. If these trends continue, regrafting couldbecome one of the most significant indications in the future, asalready reported by Sharif and Casey29 in England. Although sig-nificant improvements in surgical techniques, surgical instrumen-tation, eye banking, and tissue storage would suggest that thereshould be a decreasing trend in failed grafts, the increasing totalnumber of patients who have had corneal transplants is the prob-able reason for this increasing trend.
Aphakic bullous keratopathy was our sixth most common indi-cation. There was a significant decrease in incidence throughoutthe span of the study (p � 0.0001). This can be attributed to thevast improvements in cataract surgery techniques, resulting inmany fewer aphakic states.
This is the only study of this kind performed in the midwesternUnited States. It is also one of the largest studies of this sortperformed in the world. The leading indication for PKP in ourstudy was pseudophakic bullous keratopathy, which is in agree-ment with a large number of other similar studies.1,5–7,10–14 Thereappears to be a significant association between pseudophakicbullous keratopathy and the use of anterior chamber IOLs. Themain difference in our study, compared to most others, is that oursecond most common indication for PKP was Fuchs’ dystrophy.The reason for this discrepancy is unclear; however, it could besecondary to different genetic demographics in the midwesternUnited States.
As far as future trends go, failed grafts may become the leadingindication for PKP because as technology and our surgical abilitiesimprove, more and more transplants will be performed, leading togreater numbers of patients who could potentially have a graftfailure. Also, as failed grafts continue to increase in incidence asan indication for PKP, this group will feed on itself and increaseeven further, because a history of graft failure is one of the mostsignificant risk factors for developing a graft failure.28 Anothergroup that may become a significant indication in the future ispatients with refractive surgery complications. Improved technol-ogy and techniques in the refractive surgery industry haveprompted greater surgical success and thus patient acceptance andwillingness to have refractive surgery. Hence, there has been adramatic increase in the number of refractive surgeries performed,and it is predicted that these numbers will continue to grow expo-nentially. However, this may also lead to a greater number ofpatients having complications secondary to refractive surgery.Thus, this group may potentially become an increasing source ofpatients requiring PKP.
TABLE 2. PKP by gender
Female Male
PBK 881 (66%) 446 (34%)Fuchs’ 783 (80%) 195 (20%)KCN 188 (39%) 293 (61%)Corneal scar 243 (51%) 231 (49%)Failed graft 217 (57%) 159 (43%)ABK 215 (68%) 102 (32%)Other 150 (57%) 114 (43%)Total 2,677 (63%) 1,540 (37%)
PBK indicates pseudophakic bullous keratopathy; KCN, keratoco-nus; ABK, aphakic bullous keratopathy.
FIG. 1. Total number of PKPs by indication. PBK indicates pseudo-phakic bullous keratopathy; KCN, keratoconus; ABK, aphakic bul-lous keratopathy.
INDICATIONS FOR PKP IN THE MIDWESTERN U.S. 815
Cornea, Vol. 19, No. 6, 2000
-
Acknowledgment: Supported in part by a grant from the Indiana LionsEye Bank, Indianapolis, IN.
REFERENCES
1. Flowers CW, Chang KY, McLeod SD, et al. Changing indications forpenetrating keratoplasty, 1989–1993. Cornea 1995;14:583–8.
2. Smith RE, McDonald HR, Nesburn AB, Minckler DS. Penetratingkeratoplasty. Changing indications, 1947 to 1978. Arch Ophthalmol1980;98:1226–9.
3. Arentsen JJ, Morgan B, Green WR. Changing indications for kerato-plasty. Am J Ophthalmol 1976;81:313–8.
4. Krachmer JH, Palay DA. Cornea. St. Louis: Mosby, 1995.5. Liu E, Slomovic AR. Indications for penetrating keratoplasty in
Canada, 1986–1995. Cornea 1997;16:414–9.6. Lois N, Kowal VO, Cohen EJ, et al. Indications for penetrating kera-
toplasty and associated procedures, 1989–-1995. Cornea 1997;16:623–9.
7. Brady SE, Rapuano CJ, Arentsen JJ, et al. Clinical indications for andprocedures associated with penetrating keratoplasty, 1983–1988. Am JOphthalmol 1989;108:118–22.
8. Williams KA, Muehlberg SM, Lewis RF, et al. Influence of advancedrecipient and donor age on the outcome of corneal transplantation.Australian Corneal Graft Registry. Br J Ophthalmol 1997;81:835–9.
9. The Australian Corneal Graft Registry. 1990 to 1992 report. Aust N ZJ Ophthalmol 1993;21(suppl 2):1–48.
10. Hyman L, Wittpenn J, Yang C. Indications and techniques of pen-etrating keratoplasties, 1985–1988. Cornea 1992;11:573–6.
11. Mohamadi P, McDonnell JM, Irvine JA, et al. Changing indicationsfor penetrating keratoplasty, 1984–1988. Am J Ophthalmol 1989;107:550–2.
12. McNeill JI. Corneal transplant recipient diagnoses report 1995: eyebank association of america 1995 eye banking statistical report. EyeBank Assoc Am 1996;:1–13.
13. Robin JB, Gindi JJ, Koh K, et al. An update of the indications forpenetrating keratoplasty. Arch Ophthalmol 1986;104:87–9.
14. Price FW, Whitson WE, Collins KS, et al. Five-year corneal graftsurvival. Arch Ophthalmol 1993;111:799–805.
15. Mamalis N, Anderson CW, Kreisler KR, et al. Changing trends in theindications for penetrating keratoplasty. Arch Ophthalmol 1992;110:1409–11.
16. Lindquist TD, McGlothan JS, Rotkis WM, et al. Indications for pen-etrating keratoplasty, 1980–1998. Cornea 1991;10:210–6.
17. Damji KF, Rootman J, White VA, et al. Changing indications forpenetrating keratoplasty in Vancouver, 1978–1987. Can J Ophthalmol1990;25:243–8.
18. Kervick GN, Shepherd WFI. Changing indications for penetratingkeratoplasty. Ophthalmic Surg 1990;21:227.
19. Legeais JM, Labetoulle M, Renard G, et al. Indications for penetratingkeratoplasty. A retrospective study of 2,962 cases over 11 years. J FrOphtalmol 1993;16:516–22.
20. De Cock R. Penetrating keratoplasty in the West Bank and Gaza. Eye1994;8(pt 1):29–34.
21. Morris RJ, Bates AK. Changing indications for keratoplasty. Eye1989;3(pt 4):455–9.
22. Claoue C, Falcon M, Shilling J. Penetrating keratoplasty in south eastLondon 1981–1986: epidemiological aspects and demands on medicalresources. J R Soc Med 1990;83:245–8.
23. Brooks AMV, Weiner JM. Indications for penetrating keratoplasty: aclinicopathological review of 511 corneal specimens. Aust N Z J Oph-thalmol 1987;15:277–81.
24. Ramsay AS, Lee WR, Mohammed A. Changing indications for pen-etrating keratoplasty in the west of Scotland from 1970 to 1995. Eye1997;11:357–60.
25. Coopersmith LW, Carr M. Forecasting cataract surgeries and intraoc-ular lens implantation to 1990 using a model of population dynamics.J Cataract Refract Surg 1987;13:302–8.
26. Price FW, Whitson WE, Collins K, et al. Changing trends in explantedintraocular lenses: a single center study. J Cataract Refract Surg 1992;18:470–4.
27. Haamann P, Jensen OM, Schmidt P. Changing indications for pen-etrating keratoplasty. Acta Ophthalmol 1994;72:443–6.
28. Price FW, Whitson WE, Johns S, et al. Risk factors for corneal graftfailure. J Refract Surg 1996;12:134–47.
29. Sharif KW, Casey TA. Changing indications for penetrating kerato-plasty, 1971–1990. Eye 1993;7:485–8.
FIG. 2. Trends in the indications for PKPfrom 1982 to 1996. –, pseudophakic bul-lous keratopathy; �, Fuch’s; �, kerato-conus/aphakic bullous keratopathy; �,corneal scar; *, failed graft; and �, kera-toconus/aphakic bullous keratopathy.
K.R.B. DOBBINS ET AL.816
Cornea, Vol. 19, No. 6, 2000