Trends in Anaesthesia and Critical...
6
REVIEW Full-scale simulation may be used to train medical students in disaster medicine Monika Afzali * , Sandra Viggers Students' Society of Anaesthesiology and Traumatology, the University of Copenhagen, Denmark Keywords: Disaster medicine Teaching Medical students Simulation Anaesthesiology summary The international medical community has identified medical students as a viable resource to be used in response to national and international disasters. However today there is still no formal pre- or post- graduate training in disaster medicine for medical students in Denmark. The Students' Society of Anaesthesiology and Traumatology (SATS) in Copenhagen developed a three-day disaster medicine course called Trauma Days 2013. The course curriculum was designed to give participants insight in and the basic skills required during a disastrous event and consisted of lectures, workshops, and full-scale simulations. The course may be useful as an educational introduction to the topic of disaster medi- cine. A formalized curriculum in medical schools, eventually as an elective course, may educate medical students in disaster medicine. © 2014 Elsevier Ltd. All rights reserved. 1. Introduction Estimates indicate that more than 3.4 million people have died over the past quarter century directly due to disasters. Billions of dollars have been spent to rebuild and take care of the communities and people affected by these disasters. 1 Disasters can be defined as events in which the number of those affected and injured, and the severity of their injuries, exceed the capacity of available medical resources. 2 For disaster management to be effective it must be organized at local, regional, and national level. Moreover international contributions are often necessary as multiple casualties lead to great demands on the available health- care resources. 3 Generally speaking, medical preparedness for di- sasters can be seen as a “chain of disaster management” with medical care divided into three categories: On-scene healthcare personnel, transportation and distribution of the injured, and stationary locations such as pre-hospital facil- ities or general hospitals. 2,3 Therefore, pre-hospital cooperation between medical personnel and valuable participants in emergency care such as the Red Cross is necessary for optimal disaster management. Disasters are complex events that involve many casualties and environmental factors that are hard to reproduce inside a classroom. Simulation-based training appears to be effective 4 and in Denmark medical simulation is an increasing part of the edu- cation process for doctors and nurses, especially for those working in the field of anaesthesiology. Simulation training allows clinical situations to be recreated and trained in a controlled environment and can also be used to train teamwork and communication skills. 4,5 Simulations are traditionally performed at simulation centres. However, it is generally recommended to choose a location for simulation depending on the learning possibilities and objec- tives desired. 4 The increased use of medical simulation in both pre- and postgraduate medical training makes the use of simulation in disaster medicine obvious. In disaster medicine it is advantageous to conduct the simulation outside of the simulation centre. Research indicates that students enjoy simulation training and that it can enhance their learning experience. 6e8 Other studies have shown that students are motivated for learning about disaster medicine and that education in disaster medicine can be taught in a reasonable time. 7,9,10 Recently, the international medical community has identified medical students as a viable resource to be used in response to national and international disasters. 6,9,11e13 A 1997 workshop in disaster medicine organized by the European Community Core Group recommended the implementation of a one-week course devoted to disaster medicine in medical schools. 11 This recom- mendation was not implemented in Denmark and today there is still no formal pre- or postgraduate training in disaster medicine for medical students in Denmark. In the United States there is an * Corresponding author. Vibekegade 29, 2.tv., 2100 Copenhagen, Denmark. E-mail address: [email protected] (M. Afzali). Contents lists available at ScienceDirect Trends in Anaesthesia and Critical Care journal homepage: www.elsevier.com/locate/tacc http://dx.doi.org/10.1016/j.tacc.2014.11.005 2210-8440/© 2014 Elsevier Ltd. All rights reserved. Trends in Anaesthesia and Critical Care 5 (2015) 17e22
Transcript of Trends in Anaesthesia and Critical...

lable at ScienceDirect
Trends in Anaesthesia and Critical Care 5 (2015) 17e22
Contents lists avai
Trends in Anaesthesia and Critical Care
journal homepage: www.elsevier .com/locate/ tacc
REVIEW
Full-scale simulation may be used to train medical students in disastermedicine
Monika Afzali*, Sandra ViggersStudents' Society of Anaesthesiology and Traumatology, the University of Copenhagen, Denmark
Keywords:Disaster medicineTeachingMedical studentsSimulationAnaesthesiology
* Corresponding author. Vibekegade 29, 2.tv., 2100E-mail address: [email protected] (M. A
http://dx.doi.org/10.1016/j.tacc.2014.11.0052210-8440/© 2014 Elsevier Ltd. All rights reserved.
s u m m a r y
The international medical community has identified medical students as a viable resource to be used inresponse to national and international disasters. However today there is still no formal pre- or post-graduate training in disaster medicine for medical students in Denmark. The Students' Society ofAnaesthesiology and Traumatology (SATS) in Copenhagen developed a three-day disaster medicinecourse called Trauma Days 2013. The course curriculum was designed to give participants insight in andthe basic skills required during a disastrous event and consisted of lectures, workshops, and full-scalesimulations. The course may be useful as an educational introduction to the topic of disaster medi-cine. A formalized curriculum in medical schools, eventually as an elective course, may educate medicalstudents in disaster medicine.
© 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Estimates indicate that more than 3.4 million people have diedover the past quarter century directly due to disasters. Billions ofdollars have been spent to rebuild and take care of the communitiesand people affected by these disasters.1
Disasters can be defined as events inwhich the number of thoseaffected and injured, and the severity of their injuries, exceed thecapacity of available medical resources.2 For disaster managementto be effective it must be organized at local, regional, and nationallevel. Moreover international contributions are often necessary asmultiple casualties lead to great demands on the available health-care resources.3 Generally speaking, medical preparedness for di-sasters can be seen as a “chain of disaster management” withmedical care divided into three categories:
On-scene healthcare personnel, transportation and distributionof the injured, and stationary locations such as pre-hospital facil-ities or general hospitals.2,3
Therefore, pre-hospital cooperation between medical personneland valuable participants in emergency care such as the Red Crossis necessary for optimal disaster management.
Disasters are complex events that involve many casualties andenvironmental factors that are hard to reproduce inside a
Copenhagen, Denmark.fzali).
classroom. Simulation-based training appears to be effective4 andin Denmark medical simulation is an increasing part of the edu-cation process for doctors and nurses, especially for those workingin the field of anaesthesiology. Simulation training allows clinicalsituations to be recreated and trained in a controlled environmentand can also be used to train teamwork and communicationskills.4,5 Simulations are traditionally performed at simulationcentres. However, it is generally recommended to choose a locationfor simulation depending on the learning possibilities and objec-tives desired.4 The increased use of medical simulation in both pre-and postgraduate medical training makes the use of simulation indisaster medicine obvious. In disaster medicine it is advantageousto conduct the simulation outside of the simulation centre.Research indicates that students enjoy simulation training and thatit can enhance their learning experience.6e8 Other studies haveshown that students are motivated for learning about disastermedicine and that education in disaster medicine can be taught in areasonable time.7,9,10
Recently, the international medical community has identifiedmedical students as a viable resource to be used in response tonational and international disasters.6,9,11e13 A 1997 workshop indisaster medicine organized by the European Community CoreGroup recommended the implementation of a one-week coursedevoted to disaster medicine in medical schools.11 This recom-mendation was not implemented in Denmark and today there isstill no formal pre- or postgraduate training in disastermedicine formedical students in Denmark. In the United States there is an

M. Afzali, S. Viggers / Trends in Anaesthesia and Critical Care 5 (2015) 17e2218
increasing awareness of including disaster medicine in the medicalschool curriculum12 and literature from Germany and Sweden de-scribes how a curriculum in disaster medicine has been taught foryears.9,11 Although no published works exists, at the Arctic Uni-versity of Tromsø in Norway, a week-long course in disaster med-icine is a regular part of the medical school curriculum. In Tromsoe,the students help organize and teach an annual disaster medicinecourse. The fourth year students participate in workshops, attendlectures, and ultimately participate in a one-day disaster simula-tion. The fifth and sixth year students teach some of these work-shops. On the last day there is a simulated disaster where thestudents participate as figurants and emergency personnel.
Therefore in May 2013 the Students' Society of Anaesthesiologyand Traumatology (SATS) in Copenhagen, Denmark hosted a three-day full-scale mass-casualty simulation course in disaster medicinefor medical students.
The goal was to increase the students' knowledge about disastermedicine and introduce the concept of triage and decision-makingin emergency care. Organizers also wanted to enhance the stu-dents' interest in disaster medicine and present and practice theskills necessary not only in disaster medicine but also in everydayclinical practice. A Lickert scale was used to describe the partici-pants' self-assessed capability and confidence in managing thepatients during a disaster.10
2. The course
The course was conducted on a military training facility inVordingborg in the southern part of Zealand, Denmark. A total of 66medical students, 62 from SATS and four from the Norwegian sisterorganization in Tromsoe, participated in the course. The partici-pants were represented from all 12 semesters, thereby rangingfrom first year to last year medical students.
The course was designed stepwise after the TüPASS model forscenario design.14 First the financial and logistic resources wereidentified, which has to be the first step in program design, andthen the subject was chosen and the key learning goals estab-lished.5 The course curriculum consisted of workshops and lecturesrelated to disaster medicine, along with three additional full-scalesimulation-training scenarios. The lectures were held by expertswithin the given fields and the workshops and simulations werefacilitated by junior doctors and paramedics with great experiencein medical simulation and workshop-based education. The pro-gram (Table 1) was organized to ensure that all students partici-pated actively. This was achieved by mixing the participants acrosssemesters during the workshops and simulations to ensureadequate competencies within the groups. The participants weredivided into four groups, three groups of 16 and one of 18 partici-pants, with two instructors per group. To optimize learning mate-rial was sent to the participants prior to arrival at the course.4 Thismaterial included articles on the systematic ABCDE approach,15
algorithm for the treatment of accidental hypothermia,16
drowning,17 and a packing list to ensure participants safety andcomfort throughout the course.
2.1. Economy and funding
A course of substantial size made by students for students, re-quires a great deal of resources. Event planning began in early 2011.The Danish Society for Anaesthesia and Intensive Care Medicine(DASAIM), The Society for Junior Anaesthesiologists in Denmark(FYA), Faculty of Health Sciences at the University of Copenhagen,the Association of Danish Medical Students (FADL), and the TrygFoundation provided funding for the event. In all V 30,000 wasreceived and along with the course fee of V 45 �a person, a total of V
33,000 was raised to fund the event. In addition to the financialsupport, a private fire and ambulance company contributed am-bulances, fire trucks, and an emergency medical service crew. TheDanish Red Cross contributed their international mobile commu-nication unit, radios and additional resuscitation equipment.
The organizing group consisted of 21 volunteers from SATSCopenhagen. Volunteer instructors and speakers conducted thelectures, workshops, and simulation scenarios. The faculty of in-structors and speakers consisted of anaesthesiologists, junior doc-tors, orthopaedic surgeons, paramedics, a police officer, and ahistorian.
2.2. Workshops
Five workshops were designed to prepare the participants forthe ensuing simulations. The workshops included training intechnical skills such as radio communications, the emergency kit,tourniquet use, and transportation of patients. The workshops alsoincluded training in non-technical skills to be used during radiocommunication and prioritizing systems including the ABCDEapproach and triage.
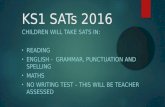
The emergency kit workshop was conducted to make all par-ticipants familiar with an emergency kit which every 2-personresponse team could make use of in the event of a disaster. The kitcontained standard basic emergency equipment for the manage-ment and interventions related to the ABCDE approach. Due tolimited resources some equipment was homemade, such as oxygenbottles made out of painted plastic bottles and finger pulse oxi-meters made out of matchboxes. Fig. 1 shows a picture of one of theemergency kits.
The triage workshop was conducted to teach the participants toprioritize patients. As volunteers were limited, patient cards wereused in place of live figurants. The triage systemwas taught from amedico-organizational point of view where casualties can bedivided into four categories2,3; patient category 0; dead and deadon arrival, patient category 1; life-threatening cases demandingimmediate attention, patient category 2; non life threatening casesdemanding immediate attention and patient category 3; casualtiesnot necessarily requiring hospitalization but less demanding care.
The radio communication workshop was conducted to train theparticipants to manage the radio equipment and to prepare theparticipants for the challenges related to communication in adisaster scenario environment.
2.3. Lectures
The goals of the lectures were to provide the participants withbasic theoretical knowledge. The lectures preceded the simulationsand were specifically related to the topic of the scenarios andlearning goals of the simulations.
The lectures were presented on infrastructure, the history ofdisasters, primary care of casualties, personal safety, triage, andgeneral theory about the ensuing simulation exercises.
2.4. Scenarios
The course included three simulation scenarios. The coursefaculty made a conscious decision to present the participants with ahigh volume of stress in these scenarios. This was done to amplifythe participants' decision-making process, which is a key elementin disaster medicine.11 To heighten the participants stress levels analarmwent off at the end of each lecture and the participants werepresented with a video played on a big screen in the auditorium.The video was prepared as a news report, briefly describing theaccident they would encounter in the field. Thereafter the

Table 1A program of the three-day course in disaster medicine.
Trauma days 2013 program
Time Place Topic
Day 1, Friday 3rd of May7.00e7.20 The Panum Institute Registration7.30e9.00 Transportation to the military training facility9.00e9.15 Auditorium Introduction9.15e10.05 Catastrophes: Now, then and the future10.15e11.00 Catastrophes: The different players11.00e11.30 Coffee break11.30e12.00 Auditorium Primary care12.00e12.30 Safety and triage12.30e13.30 LunchWorkshops Primary care and the emergency kit Cervical spine and spine board Radio communication Safety and triage13.30e14.25 Team 10 Team 20 Team 30 Team 4014.30e15.25 Team 20 Team 30 Team 40 Team 1015.25e15.40 Pause Pause Pause Pause15.40e16.35 Team 30 Team 40 Team 10 Team 2016.35e17.30 Team 40 Team 10 Team 20 Team 30
Preparation for transportation and the use of tourniquet17.30e17.50 Group 1 Group 2 Group 317.50e18.10 Group 2 Group 3 Group 118.10e18.30 Group 3 Group 1 Group 218.30e18.35 Auditorium Daily closure19:00e23.00 Social event DinnerDay 2, Saturday 4th of May07.00e08.00 Breakfast08.00e8.15 Auditorium Introduction08.15e09.00 Introduction to the course of acute medicine in Tromsø, Norway09.00e10.00 Traffic and infrastructure10.00e12.30 Training facility Simulation 1 þ debriefing12.30e13.15 Lunch13.15e14.00 Auditorium Tsunami in Thailand14.00e14.15 Pause14.15e15.15 Auditorium Hypothermia and drowning15.15e17.45 Terrain Simulation 2 þ debriefing17.45e18.00 Auditorium Daily closure19.30e Social event DinnerDay 3, Sunday 5th of May08.30e09.30 Breakfast09:30e10.00 Check out10.00e11.00 Auditorium Explosions, blasts and decelerations11.00e11.45 Auditorium A story about “Sun storm”
11.45e12.45 Alarm and transportation to Næstved12.45e14.00 Næstved Simulation 314.00e14.45 Transport back to the military facility14.45e15.15 Vordingborg Debriefing15.30e16.15 Closure, evaluations
Fig. 1. A picture of the emergency kit every team were handed in each simulation.
M. Afzali, S. Viggers / Trends in Anaesthesia and Critical Care 5 (2015) 17e22 19
participants were transported to the scene of the accident wheretheir instructors would meet them. A briefing for the upcomingscenario was delivered and learning goals were outlined. The keylearning goals for the simulation scenarios were; ensure own per-sonal safety, the ABCDE approach, patient triage, and safecommunication.
Throughout the course the participants were kept in four groupsof 16, 16, 16, and 18. The faculty believed that continuity withingroups and instructors would create the safest learning environ-ment for the participants in the stressful scenarios. The groupmembers defined the team roles themselves. At the scene of acci-dent every team had to select a team leader who was responsiblefor performing the triage of the casualties as theywere handed overby the search-and-rescue teams made up by other group members.Others would have to stay at the waiting area to assist the teamleader with triage and treatment of incoming wounded.
The three simulation scenarios presented; a plane crash, acapsizing accident and a gas explosion. The first two scenarios werepresented in the program and were conducted at the militarytraining facility in Vordingborg. The last scenario was a surprise

M. Afzali, S. Viggers / Trends in Anaesthesia and Critical Care 5 (2015) 17e2220
scenario where participants were suddenly interrupted in themiddle of a lecture and informed that their help was requested at agas explosion in the nearby town of Naestved. This last scenariowas conducted in a ruined city normally used as a military trainingfacility.
In trying to create a life-like scenario the disaster scenariosetting imitated a movie set. Sound engineers ensured that sirensand the sound of helicopters was to be heard in the entire simu-lation area. Combined with the screaming and crying of the livefigurants radio communication was challenged. Controlled fire andsmokewas also used to set the scene and wrecked plane parts wereborrowed from Copenhagen Airports. The wrecked plane partswere placed along with old cars burning and life rafts. Moreover, aprivate fire and ambulance company contributed with ambulances,fire trucks, and emergency medical service crews to transport thecasualties from the waiting area near the site of accident to thetemporary emergency hospital provided and operated by theDanish Emergency Management Agency. At the last simulation,search-and-rescue dogs were used and the participants were toldto wear helmets. Fig. 2 shows a series of pictures from thesimulations.
2.5. Debriefing
After each simulation the teams underwent an equally longclassical group debriefing consisting of a facilitated discussion heldby two facilitators.18,19 The debriefing was divided into three pha-ses. An initial description phase where the participants gave achronological and factual description of what had happened duringthe simulation. Secondly the analysis phase where the facilitatorexplored the participants' views with clarifying questions. Finallythe application phase where the facilitators asked the team forsolutions to the problems discussed in the previous phases, led adiscussion on how those solutions could be put into practice andprovided a “take-home-message”.
There was no filming of the simulations for debriefing purposes.
Fig. 2. Pictures from the
2.6. The use of figurants
Volunteer human actors simulated casualties with various dis-orders, from superficial injuries to emotional trauma or severemedical conditions, and surgical injuries requiring one or more life-saving interventions. Figurants and instructors were provided withaction cards describing roles planned by the ABCDE approach witha triage category including the disorder of the patient, the symp-toms and how the role should evolve over time. The patient caseand correct treatment options were also described on the actioncards.
Professional makeup artists were used to create the injuries onthe figurants and were handed the same action cards with adetailed description of the makeup needed to ensure a close rela-tionship between the patients' injuries and figurants' physicalappearance. Fig. 3 shows an example of one of these action cards.
Approximately 30 figurants, consisting mostly of medical stu-dents were used in the scenarios. Figurants were used several timesin the simulation scenarios to increase the total amount ofcasualties.
3. Discussion
A group of volunteer medical students from SATS held a three-day disaster medicine course for 66 medical students inDenmark. The course consisted of lectures, workshops, and threefull-scale simulations. The coursewas designed to give participants'an insight into disaster medicine and the basic skills requiredduring a disastrous event. Although exposing students to simulateddisaster scenarios cannot mimic “real world” conditions and noevidence has proven that introducing medical students to disastermedicine directly affects patient outcome, a course as presentedhere does provide medical students with knowledge about disastermedicine. In a previously made study a total of 91% of the studentswho participated in the Trauma Days 2013 reported that their self-confidence increased.10
three simulations.

Fig. 3. An example of one of the action cards from the first simulation; Plane crash.
M. Afzali, S. Viggers / Trends in Anaesthesia and Critical Care 5 (2015) 17e22 21
It is assumed that full-scale simulationmay induce levels of highstress, which traditionally is avoided. High stress levels mayinterfere with the learning experience and clinical performancesappear vulnerable to the impact of acute stress.20 However,research indicates that those who receive preparatory informationprior to performance under high-stress conditions perform betterthan those who do not, as they feel more confident.21 Schemes andalgorithms may help to recall memory in the event of an acutestress response20 and studies also show that if participants areprepared on both a physical and a psychological impact whenparticipating in a high-stress condition, their anxiety will be lowerthan if they are not prepared.21 The participants in Trauma Days2013 were prepared for the high-stress simulation scenariosthrough workshops and lectures where relevant algorithms and
skills were trained. The participants have previously indicated thatmore training made them feel less stressful as 73% felt the stresslevel suitable in the first scenario rising to 83% in the second and91% in the third.10
After each scenario the participants underwent a classical four-step debriefing. The debriefing was performed in a room separatefrom the simulation and the groups did not extend 20e25 persons,as recommended.17,20 Debriefing large groups is a complex task. Atechnique is to divide the participants into smaller groups duringthe phase of analysis. The “fishbowl”method where a smaller circleof participants sits within a larger circle (whereby the participantsmaymove to the inner circle if they wish to actively take part in thedebriefing) can also be used.18 The different methods available,18,19
accentuate the importance of educating instructors in the desired

M. Afzali, S. Viggers / Trends in Anaesthesia and Critical Care 5 (2015) 17e2222
method why the groups at this course were not too large for aclassical debriefing.
Time was a challenge in designing Trauma Days 2013. Simula-tion courses require sufficient time for completion of both thescenarios and debriefings. In this case the simulation scenarios andthe debriefing were equally long, however it is often recommendedtomake the debriefing sessions longer than the simulations.4Whendesigning a future course curriculum for large-scale simulationcourses this challenge should be taken into account, to ensure anoptimal learning experience for the participants and sufficient timefor debriefing these stressful scenarios.
Trauma Days 2013 did not make use of any form of formalassessment of the participants. The course was evaluated with anon-site questionnaire, where participants made a self-assessmentof their increase in knowledge and performance from the course.In that previously made study on Trauma Days 2013, the partici-pants indicated that they gained knowledge.10 In future disastermedicine courses the participant's performance and skill assess-ment can be addressed by the use of standardized checklists at thebeginning and end of the course. At Trauma Days 2013, students ofall levels were initiated to participate, however in both Germanyand Norway, students are expected to be in their fourth year.9
The retention of knowledge related to specific areas of disastermedicine may be difficult when not used on a daily basis. Someskills may benefit from being trained repetitively in everyday clinic,however the retention of skills and theory related to specific areasof disaster medicine and management must be ensured. This couldbe through refresher courses, requirements of re-testing or throughmaking re-training easily accessible.
When choosing the topics covered by a course in disastermedicine, available resources may limit the extent of the course.Not all relevant areas can be covered when limited time andmoneyare available. In this course curriculum the subjects of bioterrorismand epidemics were excluded. A way of introducing more topics tothe students could be to run yearly courses preferably a mixture ofrefresher courses and courses with presentation of new topics.Inspired by Trauma Days 2013, the SATS group at the University ofAarhus in Denmark has implemented a smaller course in disastermedicine. This course is presented repeatedly and thereby not onlyeducates many students, but also allows for frequent repetition andtraining.
A course as presented at Trauma Days 2013 was made possibledue to successful fundraising. The organizations that funded thecourse were most likely the ones who may benefit from the stu-dents as a resource in the future. A close relationship betweencourse providers and humanitarian organizations in need of med-ical resources can be a productive collaboration for simulation ex-ercises of considerable size such as Trauma Days 2013.10
The absence of a course in disaster medicine in medical schoolsin Denmark may prove to be problematic. With this initiative it hasbeen shown that students are interested in the topic of disastermedicine and that theymay be able to play an active and significantrole in organizing and participating in such a course. Medical stu-dents have time devoted to learning compared to the limited timewhen graduated and working full-time. This time for learning mayalso be used to build up simulation training experiences.5 With theintroduction of disaster medicine in the medical school curriculum,students with a special interest in the field could be recruited andstudents could be used as a resource should a disaster occur.13
A three-day full-scale simulation course with workshops andlectures like the work presented as Trauma Days 2013 may be
useful as an educational introduction to the topic of disastermedicine. A formalized curriculum in medical schools in Denmark,eventually as an elective course, may educate medical students indisaster medicine.
Acknowledgements
We would like to thank the organizing group behind TraumaDays 2013 for all their time and dedication and the economicsupport from the Tryg foundation, Østifternes association, FADL,The University of Copenhagen, FALCK, FYA and DASAIM.
Conflict of interest
There is no conflict of interest.
References
1. Hogan D, Burstein J. Disaster medicine. 1st ed. Pennsylvania: Lippincott Wil-liams and Wilkins; 2002.
2. De Boer J, Brismar B, Eldar R, et al. The medical severity index of disasters.J Emerg Med 1989;7(3):269e73.
3. De Boer J. An introduction to disaster medicine in Europe. J Emerg Med1995;13(2):211e6.
4. Ostergaard D, Dieckmann P, Lippert A. Simulation and CRM. Best Pract Res ClinAnaesthesiol 2011 Jun;25(2):239e49.
5. Birsner ML, Satin AJ. Developing a program, a curriculum, a scenario. SeminPerinatol 2013 Jun;37(3):175e8.
6. Scott LA, Swartzentruber DA, Davis CA, Maddux PT, Schnellman J,Wahlquist AE, et al. Competency in chaos: lifesaving performance of careproviders utilizing a competency-based, multi-actor emergency preparednesstraining curriculum. Prehosp Disaster Med 2013 Aug;28(4):322e33.
7. Scott LA, Carson DS, Greenwell IB. Disaster 101: a novel approach to disastermedicine training for health professionals. J Emerg Med 2010 Aug;39(2):220e6.
8. Ten Eyck RP, Tews M, Ballester JM. Improved medical student satisfaction andtest performance with a simulation-based emergency medicine curriculum: arandomized controlled trial. Ann Emerg Med 2009 Nov;54(5):684e91.
9. Pfenninger EG, Domres BD, Stahl W, Bauer A, Houser CM, Himmelseher S, et al.Medical student disaster medicine education: the development of an educa-tional resource. Int J Emerg Med 2010 Jan;3(1):9e20.
10. Afzali M, Ballegaard C, Viggers S. A three-day course can increase knowledgeand interest in disaster medicine for medical students. Ugeskr Laeger 2014;176.pii: V01140022.
11. Lennquist S. Education and training in disaster medicine. Scand J Surg 2005Jan;94(4):300e10.
12. Smith J, Levy MJ, Hsu EB, Levy JL. Disaster curricula in medical education: pilotsurvey. Prehosp Disaster Med 2012 Oct;27(5):492e4.
13. Mortelmans LJM, Dieltiens G, Anseeuw K, Sabbe MB. Belgian senior medicalstudents and disaster medicine, a real disaster? Eur J Emerg Med 2014Feb;21(1):77e8.
14. Dieckmann P, Rall M. Designing a scenario as a simulated clinical experience:the TüPASS scenario script. In: Kyle R, Murray BW, editors. Clinical simulation:operations, engineering, and management. Burlingtion: Academic Press; 2008.p. 541e50.
15. Thim T, Krarup NH, Grove EL, et al. ABCDE e systematisk tilgang til patientermed kritisk sygdom. Ugeskr læger. Almindelige danske lægeforening; 172(47):3264e3266.
16. Brown DJA, Brugger H, Boyd J, Paal P. Accidental hypothermia. N Engl J Med2012 Nov 15;367(20):1930e8.
17. Szpilman D, Bierens JJLM, Handley AJ, Orlowski JP. Drowning. N Engl J Med 2012May 31;366(22):2102e10.
18. Steinwachs B. How to facilitate a debriefing. Simul Gaming 1991 Nov 30;23(2):186e95.
19. Fanning RM, Gaba DM. The role of debriefing in simulation-based learning.Simul Healthc 2007 Jan;2(2):115e25.
20. Leblanc VR, Regehr C, Tavares W, Scott AK, Macdonald R, King K. The impact ofstress on paramedic performance during simulated critical events. PrehospDisaster Med 2012 Aug;27(4):369e74.
21. Inzana CM, Driskell JE, Salas E, Johnston JH. Effects of preparatory informationon enhancing performance under stress. J Appl Psychol 1996 Aug;81(4):429e35.