
Treatment Sequencing for the Multiunit Restoration: … · J Oral Maxillofac Surg 65:53-63, 2007,...
11
J Oral Maxillofac Surg 65:53-63, 2007, Suppl 1 Treatment Sequencing for the Multiunit Restoration: Hard and Soft Tissue Considerations Marius Steigmann, DDS* Edentulous spans can be treated with implants in various ways. Treatment options may range from the use of removable implant-supported dentures to the creation of fixed implant-supported restorations, and depend on the patient’s anatomical limitations and desires, including acceptance of extensive surgical procedures to restore bone, soft tissue, or both. In deciding the best course of action, many factors must be weighed, including the treatment time and cost of the various options, patient expectations, and the likelihood of achieving esthetic success. This article is intended to guide the decision-making process of cli- nicians who are restoring multiple implants, particu- larly in patients with totally edentulous maxillas. Placing more than 1 implant to restore multiple adjacent missing teeth or a fully edentulous arch can be simple or complicated. The patient’s anatomical and functional status as well as treatment goal to have a fixed or removable prosthesis must be taken into consideration. When the goal is to use a fixed recon- struction to restore an edentulous span to as natural a state as possible, both the clinician and patient must be aware that missing bone 1-3 may limit the functional and esthetic results. In some situations, it will be possible to generate new bone around the implants, using relatively simple bone-regeneration proce- dures. 4 Alternatively, more complex and time-con- suming procedures may be necessary. The cost, treat- ment time, and surgical requirements must be carefully weighed against the expected treatment out- come. When bone resorption has occurred in the wake of tooth loss, the clinician must determine how much bone loss has occurred. Identifying the difference between the actual and ideal situation is essential to determine how much restoration will be necessary to recreate a natural appearance. The preoperative diag- nostic evaluation should include: taking a comprehen- sive dental history and determining the patient’s ex- pectations; evaluating the status of the soft and hard tissue, as well as the interproximal bone height, smile line, and periodontal type; and creating mounted di- agnostic models and wax-ups. A wax-up on a mounted diagnostic model that reflects the ideal oc- clusion and proportions can be replicated in a ra- diopaque material (Fig 1) so that it can be visualized in a computed tomography (CT) scan. 5 In this way, the height and width of the missing bone can be assessed. The results will help determine whether bone graft- ing is necessary, which surgical technique 6-13 will be optimal, and the probable treatment time and cost. Knowing the amount of bone grafting required can also reveal the relative predictability of the grafting procedure, as well as whether a removable or fixed prosthesis will yield the best results. The Treatment-Planning Sequence When placing multiple implants, the treatment- planning sequence should unfold as follows: ● Evaluation of the maxillary-mandibular relation- ship; ● Consideration of the interim prosthesis design or the impact of any prosthetic reconstruction that has occurred prior to implant treatment; ● Evaluation of the bone quantity, both coronal- apical and buccal-palatal; ● Evaluation of the soft tissue quality and quantity; ● Selection of the number of implants to be used, along with their placement sites. The first step in the treatment-planning process is to evaluate the maxillary-mandibular relationship. Mounted diagnostic models facilitate the analysis of the interdental and interocclusal space. Sagittal hori- zontal maxillary-mandibular discrepancies can be cor- rected with removable dentures only, avoiding the need for bone grafting. Another factor in deciding whether multiple im- plants should be restored with a fixed or removable *Private Practice, Neckargemünd, Germany; Adjunct Assistant Professor, Department of Oral and Maxillofacial Surgery, Boston University, Boston, MA. Address correspondence and reprint requests to Dr Steigmann: IMF Neumarkt, Leiblstr 1, Mannheim, 68163 Germany; e-mail: [email protected] © 2007 American Association of Oral and Maxillofacial Surgeons 0278-2391/07/6507-0108$32.00/0 doi:10.1016/j.joms.2007.03.018 53
Transcript of Treatment Sequencing for the Multiunit Restoration: … · J Oral Maxillofac Surg 65:53-63, 2007,...

J Oral Maxillofac Surg65:53-63, 2007, Suppl 1
Treatment Sequencing for the Multiunit
Restoration: Hard and Soft
Tissue ConsiderationsMarius Steigmann, DDS*
Edentulous spans can be treated with implants in
various ways. Treatment options may range from the
use of removable implant-supported dentures to the
creation of fixed implant-supported restorations, and
depend on the patient’s anatomical limitations and
desires, including acceptance of extensive surgical
procedures to restore bone, soft tissue, or both. In
deciding the best course of action, many factors must
be weighed, including the treatment time and cost of
the various options, patient expectations, and the
likelihood of achieving esthetic success. This article is
intended to guide the decision-making process of cli-
nicians who are restoring multiple implants, particu-
larly in patients with totally edentulous maxillas.
Placing more than 1 implant to restore multiple
adjacent missing teeth or a fully edentulous arch can
be simple or complicated. The patient’s anatomical
and functional status as well as treatment goal to have
a fixed or removable prosthesis must be taken into
consideration. When the goal is to use a fixed recon-
struction to restore an edentulous span to as natural a
state as possible, both the clinician and patient must
be aware that missing bone1-3 may limit the functional
and esthetic results. In some situations, it will be
possible to generate new bone around the implants,
using relatively simple bone-regeneration proce-
dures.4 Alternatively, more complex and time-con-
suming procedures may be necessary. The cost, treat-
ment time, and surgical requirements must be
carefully weighed against the expected treatment out-
come.
When bone resorption has occurred in the wake of
tooth loss, the clinician must determine how much
bone loss has occurred. Identifying the difference
between the actual and ideal situation is essential to
determine how much restoration will be necessary torecreate a natural appearance. The preoperative diag-nostic evaluation should include: taking a comprehen-sive dental history and determining the patient’s ex-pectations; evaluating the status of the soft and hardtissue, as well as the interproximal bone height, smileline, and periodontal type; and creating mounted di-agnostic models and wax-ups. A wax-up on amounted diagnostic model that reflects the ideal oc-clusion and proportions can be replicated in a ra-diopaque material (Fig 1) so that it can be visualized ina computed tomography (CT) scan.5 In this way, theheight and width of the missing bone can be assessed.The results will help determine whether bone graft-ing is necessary, which surgical technique6-13 will beoptimal, and the probable treatment time and cost.Knowing the amount of bone grafting required canalso reveal the relative predictability of the graftingprocedure, as well as whether a removable or fixedprosthesis will yield the best results.
The Treatment-Planning Sequence
When placing multiple implants, the treatment-planning sequence should unfold as follows:
● Evaluation of the maxillary-mandibular relation-ship;
● Consideration of the interim prosthesis design orthe impact of any prosthetic reconstruction thathas occurred prior to implant treatment;
● Evaluation of the bone quantity, both coronal-apical and buccal-palatal;
● Evaluation of the soft tissue quality and quantity;● Selection of the number of implants to be used,
along with their placement sites.
The first step in the treatment-planning process isto evaluate the maxillary-mandibular relationship.Mounted diagnostic models facilitate the analysis ofthe interdental and interocclusal space. Sagittal hori-zontal maxillary-mandibular discrepancies can be cor-rected with removable dentures only, avoiding theneed for bone grafting.
Another factor in deciding whether multiple im-plants should be restored with a fixed or removable
*Private Practice, Neckargemünd, Germany; Adjunct Assistant
Professor, Department of Oral and Maxillofacial Surgery, Boston
University, Boston, MA.
Address correspondence and reprint requests to Dr Steigmann:
IMF Neumarkt, Leiblstr 1, Mannheim, 68163 Germany; e-mail:
© 2007 American Association of Oral and Maxillofacial Surgeons
0278-2391/07/6507-0108$32.00/0
doi:10.1016/j.joms.2007.03.018
53

prosthesis is the patient’s previous prosthetic experi-ence. Dentures with a labial flange create the illusionof a natural labial ridge profile. When patients whohave worn such dentures receive dental implants andthose implants are temporarily restored with an in-terim removable prosthesis with a labial flange, theinterim prosthesis will maintain the facial appearancetemporarily. However, when a final fixed restorationis placed after the period of osseointegration, theresulting lack of support for the lips will worsen thepatient’s profile. Unless the patient has been fore-warned of this consequence and agrees to it, disap-pointment will almost certainly be inevitable (Fig 2),and a costly substitution of the fixed for a removablerestoration may even be necessary (Fig 3).
For this reason, a fixed final implant-supported res-toration is almost never the best choice for a patientwho has been wearing a denture with a labial flange.Even for previously unrestored patients, when a fixed
final restoration is planned, care must be taken increating the interim removable restoration. Use of aremovable prosthesis without a labial flange14 canavoid setting the patient up for disappointment whenthe final fixed restoration is placed.
Alternatively, if the patient has never worn a den-ture and multiple implants can be placed and loadedimmediately with a fixed restoration, no negativechanges in the patient’s facial aspect will occur.
Bone Quantity
Bone quantity in both the coronal-apical (vertical)and buccal-palatal (horizontal) dimensions is anotherfactor to be considered in deciding whether a remov-able or fixed prosthesis should be used to restoreimplants placed in the totally edentulous maxilla.1,2
CORONAL-APICAL (VERTICAL) BONE RESORPTION
The extent of the vertical bone loss related to therecommended prosthodontic solution15 is summa-rized as follows: 1) no vertical bone loss: the fixedprosthesis replaces only natural-looking crowns;2) limited vertical bone loss: a fixed prosthesis re-places the crown and a portion of the root, creatingcrown contours that appear normal in the occlusalhalf but are elongated or hyper-contoured in the gin-gival half; 3) moderate vertical bone loss: a fixedprosthesis replaces missing crowns, gingival color,and a portion of the edentulous site. The prosthesismost often used is denture teeth and acrylic, but mayalso be porcelain-fused-to-metal; 4) extensive verticalbone loss: a removable overdenture is supported com-pletely by implants; 5) most severe vertical bone loss:a removable overdenture is supported by both thesoft tissue and the implants.
A simplification of bone presence in the edentulous
maxilla includes 3 categories: 1) no resorption, 2)limited bone resorption, and 3) severe bone resorp-tion. Figure 4 illustrates this simpler classificationscheme.
Cases of severe vertical bone resorption typicallyrequire extensive surgical procedures to restore thelost tissue. Even so, such procedures are not alwayssuccessful. Usually a removable prosthesis is the su-perior alternative when severe bone loss has occurred(Fig 5). Figures 6 through 10 show a removable pros-thesis used successfully to treat a severely resorbedmaxilla.
BUCCAL-PALATAL (HORIZONTAL)
BONE RESORPTION
Horizontal bone resorption is also of major impor-tance in determining the optimal prosthetic recon-struction. When the buccal-palatal plate has also beenresorbed, one option is to graft the missing buccal
FIGURE 1. A, A computed tomography scan of the radiopaquematerial enables analysis of the ideal implant position in relation to thefinal prosthesis. In this case, the scan makes it clear that all implantsexcept one can be placed in the bone without grafting. B, The upperright canine can be grafted horizontally using guided bone-regenera-tion techniques at the same time that the implant is placed.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
54 MULTIUNIT RESTORATION AND TISSUE

bone with onlay grafts,6-12 bone splitting,16 and/orguided bone regeneration.17 A second possibility is toreplace the missing bone with the acrylic of the re-movable denture. The choice of which option toselect depends upon the amount of resorption.
Buccal-palatal bone loss also can be classified usingthe 3-category simple system (Fig 11). When verticalbone resorption is nonexistent or limited, but hori-zontal bone resorption is severe, the treatment ofchoice is also a removable denture (Fig 12). Whenvertical bone resorption is nonexistent or limited andhorizontal bone resorption is also limited, either afixed or removable implant prosthesis can be used(Fig 13). Figures 14 through 17 illustrate a case inwhich a fixed implant-supported prosthesis was usedsuccessfully to treat a patient with limited vertical andhorizontal bone resorption.
If the vertical resorption is nonexistent or limitedand there is no buccal resorption, a fixed restorationis the treatment of choice.
Soft Tissue Quantity
The quantity of available soft tissue at the implantplacement sites affects the esthetic outcome only incases for which a fixed prosthesis is planned. In such
cases, a sufficient amount of soft tissue must bepresent in order to achieve a reasonably natural-look-ing final appearance. In contrast, when a removableprosthesis is to be used for the final restoration, thepink acrylic or porcelain will cover the buccal andinterdental soft tissue or lack thereof.
Thus, even when there has been limited or novertical or horizontal bone loss, assessment of the softtissue quantity is important, as indicated in Figure 18.Soft tissue quantity also must be assessed in caseswhen multiple implants are being placed immediatelyafter extraction.
If the soft tissue is inadequate and the patient re-fuses to undergo soft tissue augmentation but insistson an esthetic result, a removable restoration will bethe treatment of choice. Otherwise, a variety of sur-gical techniques can be used to increase the amountof keratinized gingiva, the gingival thickness, or both,at the time of implant placement or uncovering.
Immediate implant placement and immediate load-ing18-21 offer a means of maintaining the quantity ofsoft tissue. Figures 19 through 22 present a case inwhich a fixed restoration was placed immediatelyafter extraction and immediate implant placement,FIGURE 2. After wearing an interim removable appliance with a
labial flange for 6 months, this patient received a fixed reconstruction(A). However, the lack of support for the lips modified the patient’soverall facial aspect appearance (B) and disappointed the patient.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
FIGURE 3. The patient’s appearance was corrected by exhangingthe fixed reconstruction for a final removable one (A). Note the im-proved profile (B).
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
MARIUS STEIGMANN 55

thus maintaining the soft tissue architecture and elim-inating the need for an interim removable appliancethat could temporarily change the macroesthetics.
Soft Tissue Quality
The soft tissue has a horizontal dimension as well asa vertical one, and this too must be considered whenplanning whether to use a fixed or removable im-plant-supported restoration. If a patient’s gingival tis-sue is very thin, the implant abutments may be visiblethrough it, and use of a removable prosthesis or gin-gival grafting may be necessary. At least in the ante-rior maxilla, a thick biotype is necessary for achievingthe best esthetic results.
Planning the Number of Implants andTheir Positioning
After the decision of whether to use a fixed or a
removable final restoration has been made, the nextconsideration is how many implants to use and whereto place them. Both biomechanical and biologicalfactors influence this decision and should be evalu-ated.
BIOMECHANICAL CONSIDERATIONS
In general, implants should be positioned so thatstress is distributed evenly throughout the bone. Rel-evant biomechanical factors include the number ofteeth to be replaced and their location in the jaw.Because the weakest bone tends to be located in theposterior, more implants will be required if the eden-tulous span is there, than if the edentulous span islocated more anteriorly. For a fixed restoration of afull arch, usually 8 to 10 implants will be required,along with adjunctive surgical procedures such as asinus lift, vertical and horizontal bone augmentation,and soft-tissue grafting. The implants must be placedin the mesio-distal position of the extracted tooth. Incontrast, removable prostheses generally requirefewer implants (typically 6 or less), and in many cases,a sinus lift can be avoided. The mesial-distal implantposition can differ from that of the extracted tooth.
When restoring a fully edentulous arch, implantsmust always be placed for ideal biomechanical load-ing. Whether additional implants are needed in theanterior zone will depend upon the maxillary anat-
FIGURE 4. The degree of vertical bone resorption is an importantfactor to consider when planning the restoration of multiple implants.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
FIGURE 5. In cases of severe vertical bone resorption, the treatment of choice is a removable denture.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 6. The pretreatment panoramic x-ray reveals severe verticalbone resorption. The treatment of choice is a removable appliance.Surgical intervention in the form of a bilateral sinus graft is still neededto create bone for the anchorage of the removable appliance.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
56 MULTIUNIT RESTORATION AND TISSUE

omy. A V-shaped anterior zone generally involves alonger span and requires the placement of 1 or 2implants within the zone. The number of implantsrequired in the posterior zone will depend on thebone quality.
BIOLOGICAL CONSIDERATIONS
When planning the number and positioning of mul-tiple implants, the final outcome of the soft tissuearound those implants must also be considered. Gar-ber et al22 have described how the soft-tissue height
varies depending upon whether the tissue is locatedbetween 2 adjacent implants, an implant and a tooth,an implant and a pontic, or 2 pontics. They found thatthe shortest papillae occurred between 2 adjacentimplants, with higher tissue levels recorded betweenimplants and pontics, and the highest levels between2 pontics.
These insights can be used in planning the place-
ment of implants in the esthetic zone. After radiolog-ical diagnosis, adjacent implants should be placedwhenever possible where the bone levels are highest.
FIGURE 7. Sinus-lift augmentation of the patient shown in Figure6. After exposure of the bone (A), the sinus window is preparedwith piezosurgery (B). In this case, a septum with limited heightmade the elevation of the Schneiderian membrane more difficult.The cavity that resulted after sinus preparation was then filled withxenograft and autologous bone (C).
Marius Steigmann. Multiunit Restoration and Tissue. J OralMaxillofac Surg 2007.
FIGURE 8. Six months after the sinus augmentation seen in Figure 7, the bone quality and bone quantity achieved were ideal for implant placement.The implant positions were determined with the help of a computed tomography scan, a radiopaque stent, and computer-aided planning. Note theamount of “bone-like” material into which implants could be placed.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
MARIUS STEIGMANN 57

FIGURE 9. A, Computed tomography scan of the surgical stent (red),the host bone (yellow), and the augmented bone (turquoise). B, Theactual surgical stent in position. C, The implant in situ after delayedplacement in a second surgical intervention.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
FIGURE 10. A, Final removable prosthesis (B) in place, after osseointegration to replace teeth and missing vertical bone for a case of severe boneresorption.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 11. The simple 3-classification schema can also be applied to horizontal bone loss.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
58 MULTIUNIT RESTORATION AND TISSUE

FIGURE 12. When the vertical bone resorption is nonexistent or limited but horizontal bone resorption is severe, the treatment of choice is aremovable prosthesis.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 13. When both vertical and horizontal bone resorption are nonexistent or limited, either a fixed or removable implant prosthesis can beused.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 14. A, Both vertical and horizontal resorption are limited. A wax-up will show the amount of bone grafting necessary to place the implantsin the ideal prosthetic position (B). Because a fixed final restoration is planned, the wax-up, surgical stent, and interim removable appliance are allmade without a labial flange (C).
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
MARIUS STEIGMANN 59

FIGURE 15. A, B, The cross-sectional computed tomography scans show no vertical bone resorption and limited horizontal resorption. Horizontalbone grafting is necessary to enable a fixed reconstruction. This augmentation can be achieved by means of onlay block augmentation, bonesplitting, or guided bone regeneration.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 16. After bone exposure (A), the bone is piezosurgically split (B), and tapered implants are placed between the 2 cortical plates (C). Inthis instance, tricalcium phosphate was used to fill in the spaces adjoining the implants.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
60 MULTIUNIT RESTORATION AND TISSUE

FIGURE 17. Note the patient’s profile before treatment (A). Aftertreatment with a fixed implant reconstruction, the profile has improved(B). C, The final fixed implant reconstruction.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
FIGURE 18. If bone loss in both the vertical and horizontal dimensions is nonexistent or limited, assessment of the soft tissue is important to determinewhether a fixed or removable final restoration should be used.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
MARIUS STEIGMANN 61

Where they are most apical, 2 pontics should beplanned. Between these 2 extremes, alternating pon-tics and implants should be placed. After insertion ofthe final fixed prosthesis, the soft tissue will level out,creating a harmonious soft tissue outcome around thecrowns and pontics.
Summary
Although the predictability of treating full or partial
edentulism with dental implants has long been estab-
lished, the choice of whether to use a fixed or remov-
able prosthesis to restore such implants remains a
FIGURE 19. Maxilla with mobile remaining teeth (A). No vertical or horizontal resorption has occurred. The treatment of choice is extractionfollowed by immediate implant placement and immediate loading with a fixed restoration. This approach will maintain the soft-tissue architecture andeliminate the need for an interim removable appliance that could temporarily change the macroesthetics. B, The implants with impression copingsimmediately after surgery. Only the implants in the intrasinusal space are loaded. In the posterior maxilla, where a sinus-lift procedure was performed,the implants will be loaded in a staged procedure.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 20. Immediate loading with cross-arch stabilization for the implants placed in the intrasinusal space (A). The temporary reconstruction ismetal-reinforced. This kind of temporization does not change the patient’s overall facial appearance. B, The soft tissue development between 2pontics after the patient had worn the temporary prosthesis for 6 months. The implant positions were planned with consideration for the biology ofthe site.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
62 MULTIUNIT RESTORATION AND TISSUE
complex one. Attention to such factors as the amountof vertical and horizontal bone loss that has occurred,the quality and quantity of the soft tissue, and thepatient’s restorative history can simplify treatmentplanning.
References1. Atwood DA: Postextraction changes in the adult mandible as
illustrated by microradiographs of midsagittal sections and se-rial cephalometric roentgenographs. J Prosthet Dent 13:810,1963
2. Atwood DA: Some clinical factors related to rate of resorptionof residual ridges. J Prosthet Dent 86:119, 2001
3. Salama H, Salama MA, Garber D, et al: The interproximal heightof bone: A guidepost to predictable aesthetic strategies andsoft-tissue contours in anterior tooth replacement. Pract Peri-odontics Aesthet Dent 10:1131, 1998
4. Steigmann M, Wang HL: Esthetic buccal flap for correction ofbuccal fenestration defects during flapless immediate implantsurgery. J Periodontol 77:517, 2006
5. Ganz SD: Presurgical planning with CT-derived fabrication ofsurgical guides. J Oral Maxillofac Surg 63 Suppl 2:59, 2005
6. Degidi M, Scarano A, Piattelli A: Regeneration of the alveolarcrest using titanium micromesh with autologous bone and aresorbable membrane. J Oral Implantol 29:86, 2003
7. Koberg W: Spätergebnisse nach Augmentationsplatiken. DtschZ Zahnärztl Implantol 1:239, 1985
8. Schliephake H, Neukam FW, Scheller H, et al: Local ridgeaugmentation using bone grafts and osseointegrated implants
in the rehabilitation of partial edentulism: Preliminary results.Int J Oral Maxillofac Implants 9:557, 1994
9. Buser D, Dula K, Belser UC, Hirt HP, Berthold H: Localizedridge augmentation using guided bone regeneration. II. Surgi-cal procedure in the mandible. Int J Periodontics RestorativeDent 15:10, 1995
10. Maiorana C, Beretta M, Salina S, Santoro F: Reduction of autog-enous bone graft resorption by means of Bio-Oss coverage: Aprospective study. Int J Periodontics Restorative Dent 25:19,2005
11. Jensen SS, Aaboe M, Pinholt EM, Hjorting-Hansen E, Melsen F,Ruyter IE: Tissue reaction and material characteristics of fourbone substitutes. Int J Oral Maxillofac Implants 11:55, 1996
12. Weibrich G, Trettin R, Gnoth SH, Gotz H, Duschner H, WagnerW: [Determining the size of the specific surface of bone sub-stitutes with gas adsorption]. Mund Kiefer Gesichtschir 4:148,2000
13. Klinge B, Alberius P, Isaksson S, Jonsson J: Osseous response toimplanted natural bone mineral and synthetic hydroxylapatiteceramic in the repair of experimental skull bone defects. J OralMaxillofac Surg 50:241, 1992
14. Kinsel RP, Lamb RE: Development of gingival esthetics in theedentulous patient prior to dental implant placement using aflangeless removable prosthesis: A case report. Int J Oral Max-illofac Implants 17:866, 2002
15. Misch CE: Prosthetic options in implant dentistry, in Misch CE(ed): Contemporary Implant Dentistry, St Louis, MO, Mosby,1999, pp 67-72
16. Schlee M, Steigmann M, Bratu E, Garg AK: Piezosurgery: Basicsand possibilities. Implant Dent 15:334, 2006
17. Steigmann M: Pericardium membrane and xenograft particu-late grafting materials for horizontal alveolar ridge defects.Implant Dent 15:186, 2006
18. Misch CE, Degidi M: Five-year prospective study of immediate/early loading of fixed prostheses in completely edentulous jawswith a bone quality-based implant system. Clin Implant DentRelat Res 5:17, 2003
19. Horiuchi K, Uchida H, Yamamoto K, Sugimura M: Immediateloading of Brånemark system implants following placement inedentulous patients: A clinical report. Int J Oral MaxillofacImplants 15:824, 2000
20. Tarnow DP, Emtiaz S, Classi A: Immediate loading of threadedimplants at stage 1 surgery in edentulous arches: Ten consec-utive case reports with 1- to 5-year data. Int J Oral MaxillofacImplants 12:319, 1997
21. Degidi M, Piattelli A: Immediate functional and non-functionalloading of dental implants: A 2- to 60-month follow-up study of646 titanium implants. J Periodontol 74:225, 2003
22. Garber DA, Salama MA, Salama H: Immediate total tooth re-placement. Compend Contin Educ Dent 22:210, 2001
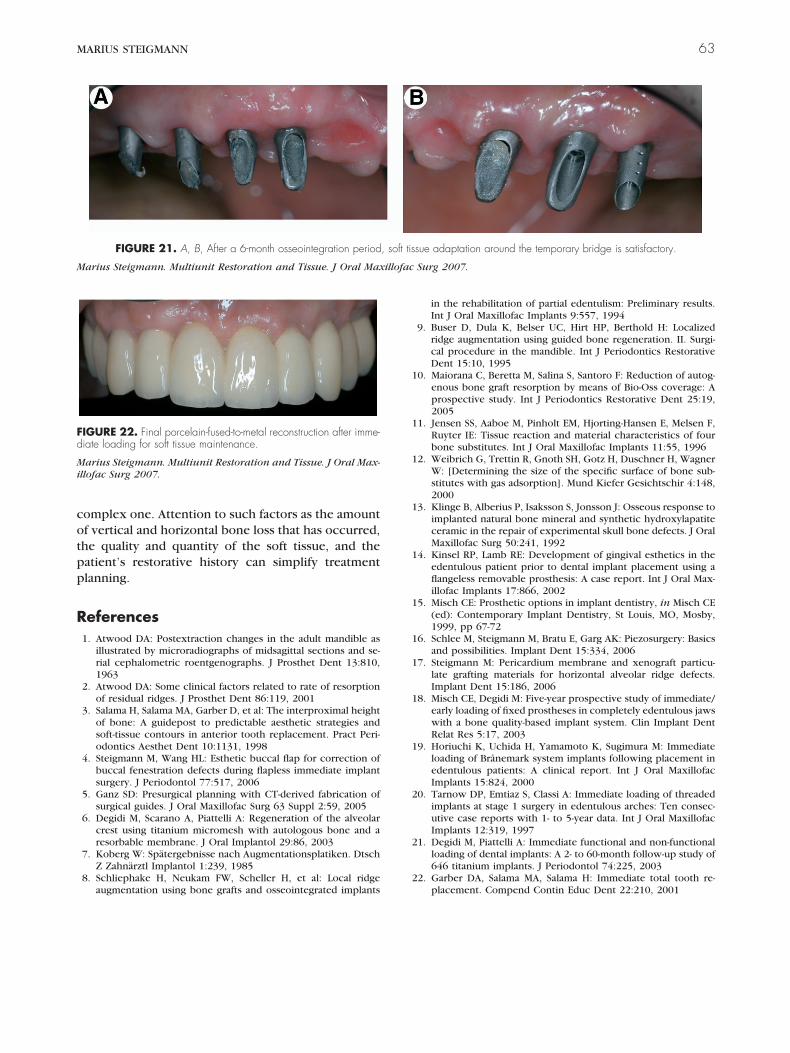
FIGURE 21. A, B, After a 6-month osseointegration period, soft tissue adaptation around the temporary bridge is satisfactory.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Maxillofac Surg 2007.
FIGURE 22. Final porcelain-fused-to-metal reconstruction after imme-diate loading for soft tissue maintenance.
Marius Steigmann. Multiunit Restoration and Tissue. J Oral Max-illofac Surg 2007.
MARIUS STEIGMANN 63













![[Architecture eBook] Architectural Design - Multiunit Housing](https://static.fdocuments.in/doc/165x107/5477ff69b4af9f9f518b45aa/architecture-ebook-architectural-design-multiunit-housing.jpg)




