Treatment options in patients with decompensated cirrhosis, pre- … · 2017. 2. 2. · been shown...
12
Treatment options in patients with decompensated cirrhosis, pre- and post-transplantation Martina Gambato, Sabela Lens, Miquel Navasa, Xavier Forns ⇑ Liver Unit, Hospital Clinic, IDIBAPS and CIBEREHD, University of Barcelona, Spain Summary Interferon-based treatments have a poor safety profile and lim- ited efficacy in patients with advanced liver disease and in patients with hepatitis C (HCV) recurrence after liver transplanta- tion (LT). Despite the recent approval of the first interferon-free regimen, which will be followed by several other interferon-free combinations in 2014 and 2015, data in patients with advanced cirrhosis and hepatitis C after LT are still limited. One study has already proven the concept that graft HCV infection can be pre- vented in a significant proportion of patients by treating them with sofosbuvir and ribavirin while awaiting LT. Two inter- feron-free regimens have also demonstrated a high efficacy in patients with hepatitis C recurrence after transplantation. Before these treatment strategies can be implemented in clinical prac- tice, a few issues need to be addressed: (1) safety and efficacy of new antivirals in patients with decompensated cirrhosis, (2) the impact of viral clearance on liver function, (3) the potential consequences of virological failure (and the selection of multi- drug resistant HCV strains) in patients with decompensated cirrhosis or with severe hepatitis C recurrence after LT, and (4) drug-drug interactions (DDI) profiles. Finally, in the transplant setting it is also relevant to learn which strategy is most cost-effective in minimizing the negative impact of hepatitis C: preventing graft infection by treating patients before transplanta- tion or treating hepatitis C recurrence after LT. Ó 2014 European Association for the Study of the Liver. Published by Elsevier B.V. Introduction In the last year, the approval of the first interferon-free regimens for the treatment of chronic hepatitis C has been a major step for- ward in hepatology. The safety and efficacy of the combination of several direct-acting antivirals (DAAs), compared to interferon- containing regimens [1], has opened hope for groups of patients in whom interferon-based regimens were contraindicated or in whom these regimens had a very limited efficacy and poor toler- ance. In particular, the negative impact of hepatitis C recurrence on graft and patient survival following LT [2,3] makes gaining information on how to treat these patients urgent. There are three well-defined groups of individuals for which there is an urgent need to assess the safety and efficacy of inter- feron-free regimens: (1) patients awaiting liver transplantation, (2) patients with decompensated cirrhosis not included in a wait- ing transplant list and; (3) individuals with hepatitis C recurrence after transplantation. Management of patients awaiting liver transplantation Patients with advanced cirrhosis, particularly those awaiting LT, are one of the most difficult-to-treat population. The main aim of antiviral treatment for patients on the waiting list is to prevent HCV infection of the new liver, since HCV recurrence reduces graft and patient survival. Most centres indicate short term ther- apy in order to achieve undetectable HCV-RNA at LT, which is associated with a high chance of preventing graft infection following transplantation [4]. In a setting of shorting organ availability, a second potential aim is to improve liver function, and perhaps regain compensation for finally delisting. This has been shown in some patients with HBV-related cirrhosis treated with nucleo(s)tide analogues [5,6], but in HCV-infected cirrhotic patients this has not been demonstrated [7]. Journal of Hepatology 2014 vol. 61 j S120–S131 Treatment Keywords: Decompensated cirrhosis; Waiting list; Liver transplantation; HCV recurrence; DAA; Sustained virologic response; Adverse events; Fibrosis regression. Received 24 May 2014; received in revised form 3 July 2014; accepted 11 July 2014 ⇑ Corresponding author. Address: Liver Unit, Hospital Clinic, Villarroel 170, Barcelona 08036, Spain. Tel.: +34 93 227 5753; fax: +34 93 227 1779. E-mail address: [email protected] (X. Forns). Abbreviations: HCV, hepatitis C; LT, liver transplantation; DDI, drug-drug interactions; DAAs, direct-acting antivirals; PegINF, peginterferon; RBV, ribavirin; MELD, model of end-stage liver disease; PI, protease inhibitor; PR, peginterferon plus ribavirin; SAEs, serious adverse events; HCC, hepatocellular carcinoma; SMV, simeprevir; DCV, daclatasvir; SOF, sofosbuvir; SVR, sustained virological response; SVR12, sustained virologic response 12-week after the end of treatment; LDV, ledipasvir; FDV, faldaprevir; ASV, asunaprevir; DBV, deleobuvir; ABT-267, ombitasvir; ABT-333, dasabuvir; US, United States; PK, drug pharmacokinetics; RAVs, resistant-associated viral strains; LLOD, lower limit of detection; ECM, extracellular matrix; HSCs, hepatic stellate cells; FCH, fibrosing cholestatic hepatitis; EPO, erythropoietin; CsA, cyclosporine A; INR, international normalized ratio; GFR, glomerular filtration rate; EAP, expanded access program. Journal of Hepatology Update: Hepatitis C Open access under CC BY-NC-ND license.
Transcript of Treatment options in patients with decompensated cirrhosis, pre- … · 2017. 2. 2. · been shown...

Treatm
ent
Journal of Hepatology Update: Hepatitis C
Treatment options in patients with decompensated cirrhosis,pre- and post-transplantation
Martina Gambato, Sabela Lens, Miquel Navasa, Xavier Forns⇑
Liver Unit, Hospital Clinic, IDIBAPS and CIBEREHD, University of Barcelona, Spain
Summary
Interferon-based treatments have a poor safety profile and lim-ited efficacy in patients with advanced liver disease and inpatients with hepatitis C (HCV) recurrence after liver transplanta-tion (LT). Despite the recent approval of the first interferon-freeregimen, which will be followed by several other interferon-freecombinations in 2014 and 2015, data in patients with advancedcirrhosis and hepatitis C after LT are still limited. One study hasalready proven the concept that graft HCV infection can be pre-vented in a significant proportion of patients by treating themwith sofosbuvir and ribavirin while awaiting LT. Two inter-feron-free regimens have also demonstrated a high efficacy inpatients with hepatitis C recurrence after transplantation. Beforethese treatment strategies can be implemented in clinical prac-tice, a few issues need to be addressed: (1) safety and efficacyof new antivirals in patients with decompensated cirrhosis, (2)the impact of viral clearance on liver function, (3) the potentialconsequences of virological failure (and the selection of multi-drug resistant HCV strains) in patients with decompensatedcirrhosis or with severe hepatitis C recurrence after LT, and (4)drug-drug interactions (DDI) profiles. Finally, in the transplant
Journal of Hepatology 20
Keywords: Decompensated cirrhosis; Waiting list; Liver transplantation; HCVrecurrence; DAA; Sustained virologic response; Adverse events; Fibrosisregression.Received 24 May 2014; received in revised form 3 July 2014; accepted 11 July 2014⇑ Corresponding author. Address: Liver Unit, Hospital Clinic, Villarroel 170,Barcelona 08036, Spain. Tel.: +34 93 227 5753; fax: +34 93 227 1779.E-mail address: [email protected] (X. Forns).Abbreviations: HCV, hepatitis C; LT, liver transplantation; DDI, drug-druginteractions; DAAs, direct-acting antivirals; PegINF, peginterferon; RBV,ribavirin; MELD, model of end-stage liver disease; PI, protease inhibitor; PR,peginterferon plus ribavirin; SAEs, serious adverse events; HCC, hepatocellularcarcinoma; SMV, simeprevir; DCV, daclatasvir; SOF, sofosbuvir; SVR, sustainedvirological response; SVR12, sustained virologic response 12-week after the endof treatment; LDV, ledipasvir; FDV, faldaprevir; ASV, asunaprevir; DBV,deleobuvir; ABT-267, ombitasvir; ABT-333, dasabuvir; US, United States; PK,drug pharmacokinetics; RAVs, resistant-associated viral strains; LLOD, lower limitof detection; ECM, extracellular matrix; HSCs, hepatic stellate cells; FCH, fibrosingcholestatic hepatitis; EPO, erythropoietin; CsA, cyclosporine A; INR, internationalnormalized ratio; GFR, glomerular filtration rate; EAP, expanded access program.
setting it is also relevant to learn which strategy is mostcost-effective in minimizing the negative impact of hepatitis C:preventing graft infection by treating patients before transplanta-tion or treating hepatitis C recurrence after LT.� 2014 European Association for the Study of the Liver. Publishedby Elsevier B.V. Open access under CC BY-NC-ND license.
Introduction
In the last year, the approval of the first interferon-free regimensfor the treatment of chronic hepatitis C has been a major step for-ward in hepatology. The safety and efficacy of the combination ofseveral direct-acting antivirals (DAAs), compared to interferon-containing regimens [1], has opened hope for groups of patientsin whom interferon-based regimens were contraindicated or inwhom these regimens had a very limited efficacy and poor toler-ance. In particular, the negative impact of hepatitis C recurrenceon graft and patient survival following LT [2,3] makes gaininginformation on how to treat these patients urgent.
There are three well-defined groups of individuals for whichthere is an urgent need to assess the safety and efficacy of inter-feron-free regimens: (1) patients awaiting liver transplantation,(2) patients with decompensated cirrhosis not included in a wait-ing transplant list and; (3) individuals with hepatitis C recurrenceafter transplantation.
Management of patients awaiting liver transplantation
Patients with advanced cirrhosis, particularly those awaiting LT,are one of the most difficult-to-treat population. The main aimof antiviral treatment for patients on the waiting list is to preventHCV infection of the new liver, since HCV recurrence reducesgraft and patient survival. Most centres indicate short term ther-apy in order to achieve undetectable HCV-RNA at LT, which isassociated with a high chance of preventing graft infectionfollowing transplantation [4]. In a setting of shorting organavailability, a second potential aim is to improve liver function,and perhaps regain compensation for finally delisting. This hasbeen shown in some patients with HBV-related cirrhosis treatedwith nucleo(s)tide analogues [5,6], but in HCV-infected cirrhoticpatients this has not been demonstrated [7].
14 vol. 61 j S120–S131

Key Points
• Treatment with IFN-free regimens will prevent hepatitis C recurrence in a significant proportion of patients with compensated cirrhosis and hepatocellular carcinoma awaiting LT. The best treatment regimen in this scenario is still not defined, but most likely will consist of the combination of sofosbuvir with a second DAA (daclatasvir, ledipasvir, simeprevir depending on the HCV genotype). In areas where these drugs are not available, IFN-based regimens may still prevent hepatitis C recurrence in a small proportion of patients.
• Patients with decompensated cirrhosis cannot undergo IFN-based regimens. Data on safety and efficacy of IFN-free regimens in this population are very limited and thus, recommendations are not supported by data. In decompensated cirrhotic patients awaiting LT, IFN-free regimens may allow viral clearance and prevent hepatitis C recurrence. In addition, viral clearance may be associated with liver function improvement, keeping some patients away from LT (with a better use of this valuable resource). Pharmacokinetics and safety data in this patient population are available for sofosbuvir, simeprevir and daclatasvir.
• In decompensated cirrhotic patients not enlisted for transplantation, treatment with IFN-free regimens should aim at reducing clinical events and particularly at improving survival. Treatment in this population might be considered in cases without life-threatening comorbidities. Nevertheless, well designed trials are necessary to address the clinical benefit of treating this population.
• IFN-free regimens should be the goal for individuals with severe hepatitis C recurrence after LT. Early treatment of individuals with aggressive HCV recurrence may allow for a full recovery of liver function and fibrosis regression.
• In liver transplant recipients with decompensated cirrhosis IFN-free regimens may be associated with improvement in liver function in some patients. In those who do not improve, retransplantation might become a choice in the case of a high MELD score and HCV clearance.
0
20
40
60
80
100
SOF + PR SMV + PR
DCV + PR
80%
60% 58%60%
43/54 29/48 83/14212/20
SVR
12 (%
)
NaiveTreatment-exp.
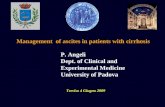
Fig. 1. Efficacy results of IFN-based therapies in cirrhotic patients. SOF + PR,sofosbuvir plus PegIFN and RBV during 12 weeks, genotype 1 (NEUTRINO study[21]). SMV + PR, simeprevir (12 weeks) plus PegIFN and RBV (24–48 weeks),genotype 1 (pooled data of QUEST-1 [22], QUEST-2 [23], PROMISE [24], ASPIRE[25], and ATTAIN studies [26]). DCV + PR: daclatasvir (12–24 weeks) plus PegIFNand RBV (24–48 weeks), genotypes 1 and 4 (COMMAND-1 study) [27].
Treatm
ent
JOURNAL OF HEPATOLOGY
Interferon-based regimens
Current interferon-based treatments are not optimal in patientswith advanced cirrhosis. Some studies have shown that peginter-feron (PegIFN) plus ribavirin (RBV) administered to patients onthe waiting list can prevent graft infection in patients whoachieve undetectable HCV RNA [4,8–10]. Virological responsesmaintained after LT are around 25%, even when using a low accel-erating dose regimen (LADR) [10]. Sustained virological response(SVR) rates are higher in individuals infected with HCV genotypes2 and 3, as well as in those with the IL28B CC genotype [11]. Nev-ertheless, interferon-based therapy can only be administered incirrhotic patients with good liver function (Child-Pugh 67 orMELD 618), in whom the indication of transplantation is hepato-cellular carcinoma (HCC) [3]. A recent study including living
Journal of Hepatology 2014
donor liver transplantation recipients and patients with HCC withMELD exception points (typically patients with better liver func-tion) demonstrated SVR rates around 50% if pre-transplant ther-apy lasted >16 weeks [9]. In patients with more advanceddisease, serious adverse events (i.e., bacterial infections, such asspontaneous bacterial peritonitis or spontaneous bacteraemia[8], grade 3 and 4 cytopenias and clinical decompensation) arefrequent and can be life-threatening. Thus, only a small propor-tion of HCV-infected patients can undergo interferon-basedtreatment.
The addition of first-generation protease inhibitors (PIs),boceprevir and telaprevir, to PR is clearly associated with anincrease in response rates in G1 infected patients [12–16], includ-ing some patients awaiting LT. Verna et al. [17] reported theresults of triple therapy in a small cohort of HCV-infectedcirrhotic patients (n = 29) on the waiting list for LT (Child-PughA 62%, Child-Pugh B 38%). The median duration of treatmentwas 27 weeks. Post-transplant SVR12 was 67% (8 out of 12 trans-planted patients). From a perspective of safety, serious adverseevents occurred in nine patients (31%), including one death(3%) and 8 hospitalizations (28%). Despite these results, the pro-portion of patients on the waiting list that may benefit from tripletherapy with telaprevir or boceprevir is small, for several reasons.First, in decompensated patients (Child-Pugh C) IFN-based thera-pies are contraindicated. Second, SVR rates are very low incirrhotic patients who are previous null-responders to PR (a com-mon situation in patients awaiting LT). Third, PI-based regimensin real-life compensated cirrhotic patients are associated withserious adverse events (SAEs), such as severe infections (4–6%),clinical decompensation (3–4%) and even death [18,19]. Patientswith a platelet count below 100,000/mm3 and serum albuminlevels below 35 g/L have a higher risk than 40% to life-threateningside effects [18].
More importantly, with the recent approval of sofosbuvir,simeprevir and daclatasvir, the use of boceprevir and telaprevirshould not be recommended in this population [20]. Despitenot having data on the efficacy of PR combined with new DAAsin patients awaiting LT, studies assessing these combinationswhich include a sufficient number of patients with cirrhosis, sug-gest good safety and efficacy in individuals with well-compen-sated disease in whom the indication for LT is HCC. SVR ratesin cirrhotic patients treated with PR plus simeprevir (SMV),daclatasvir (DCV) and sofosbuvir (SOF) are summarized in Fig. 1
vol. 61 j S120–S131 S121

Journal of Hepatology Update: Hepatitis C
[21–27]. The combination of PR plus sofosbuvir for 12 weeksseems to offer the highest efficacy and the best safety profile: thisregimen was evaluated in the NEUTRINO phase 3 trial in treat-ment-naïve G1, 4, 5, and 6 patients (most G1) [21]. The overallSVR rate was 90%: cirrhotic patients had a lower sustained viro-logic response (SVR) rate than non-cirrhotic patients (80% vs. 92%,respectively). Regretfully, data in treatment-experienced cir-rhotic patients using this combination, are only available in asmall number of G2 and G3 infected patients, with SVR rates over80% [28].Interferon-free regimens in patients awaiting LT
Sofosbuvir and ribavirin in patients awaiting LTIn a phase 2 open-label study, 61 HCV-infected patients (G1–4)awaiting LT, received sofosbuvir and ribavirin until transplanta-tion or up to 48 weeks [29]. The indication for LT was HCC; nearly75% of patients were Child-Pugh A, all had MELD score below 15and most individuals were previous non-responders to inter-feron-based regimens (75%). The median duration of therapywas 17 weeks.
Forty-six patients underwent LT and of these, 43 (92%) hadHCV RNA <25 IU/ml at time of LT. Of them, 42 reached 12 weeksof follow-up after transplantation and 29 (69%) achieved SVR at12 weeks after the end of therapy (SVR 12). The strongest predic-tor of post-LT SVR was the number of consecutive days withundetectable HCV RNA prior to transplant, with only one relapseamong the 25 individuals with undetectable HCV-RNA for>28 days while on treatment. Treatment with SOF + RBV wasgenerally well tolerated. The most frequently reported adverseevents were mild, and only 1 patient discontinued treatmentdue to anaemia. These efficacious results are encouraging. Longertreatment duration and/or the addition of a second DAA (cur-rently under evaluation with ledipasvir [LDV]), may reduce therate of virological relapse.
Future interferon-free regimens in patients awaiting LTIn most phase 2 and registration trials, the proportion ofcirrhotics is small and those with clinically significant portalhypertension are usually excluded. The data available so far arenot enough for indicating IFN-free regimens to all patients await-ing a transplant, particularly for decompensated cirrhotics. How-ever, patients with platelet counts above 50,000–60,000/mm3
(and thus with significant portal hypertension) were includedin a few trials and safety and efficacy results were still good(Tables 1 and 2). The available data support the use of IFN-freeregimens in patients with compensated cirrhosis and hepatocel-lular carcinoma awaiting LT.
For genotype 1 cirrhotic patients, the combination of sof-osbuvir and ribavirin appears suboptimal, particularly in previ-ous non-responders. Data from phase 2 studies [30,31]strongly suggest that the addition of simeprevir or daclatasvirto sofosbuvir (with or without ribavirin) significantly increasesSVR rates up to 90% (Table 1). The data are yet to be confirmedin clinical trials including a larger number of cirrhotic patients(Table 2).
Two registration phase 3 studies have assessed the safety andefficacy of sofosbuvir and ledipasvir (with or without ribavirin)for 12 vs. 24 weeks in G1 infected patients [32,33]. In the firststudy (ION-1), which included naive patients, there were 136 cir-rhotic patients and SVR rates were 100% in the RBV arms and 97%
S122 Journal of Hepatology 2014
in the non-RBV arms (Fig. 2A). In the second study (ION-2), whichincluded treatment-experienced patients (with a significantnumber of failures to PI), there were 88 cirrhotic patients: SVRrates were 100% in the 24-week regimen, but the figuredecreased to �85% in the 12-week arms (Fig. 2A). The latter sug-gests that a regimen containing sofosbuvir and ledipasvir isexcellent in compensated cirrhotics; extension to 24 weeks maybe necessary in previous non-responders.
A large randomized clinical trial performed specifically in cir-rhotic patients with an all-oral DAA combination [34] hasrecently evaluated the safety and efficacy of ABT-450 boostedwith ritonavir, ombitasvir, and dasabuvir co-administered withRBV for 12 or 24 weeks in HCV genotype 1-infected patients(both treatment-naïve and -experienced). SVR rates reached92% and 96% in the 12-week and 24-week arms, respectively(Fig 2A). A trend toward slightly lower SVR rates were observedin G1a previous null-responders, as well as in patients with moresignificant portal hypertension (platelets <100,000/mm3) or moreadvanced cirrhosis (albumin <35 g/L) in the 12-week arm.
Finally, a combination of daclatasvir and asunaprevir (ASV) for24 weeks was evaluated in 223 genotype 1b cirrhotics; SVR rateswere 91% in treatment-naïve, 81% in ineligible/intolerant patientsand 87% in treatment-experienced individuals [35].
For genotype 2 and 3-infected patients, results from fourphase 3 trials assessing sofosbuvir plus ribavirin have been pub-lished (Fig. 2B). Overall, SVR rates in G2 were consistently lowerin cirrhotic patients compared to non-cirrhotics, but 12 or 16-week regimens achieved SVR rates of around 80%. Regardinggenotype 3, it became clear that a 12-week regimen of sofosbuvirand ribavirin was insufficient for cirrhotic patients [21], in whomtreatment extension up to 24 weeks increased SVR rates up to92% in treatment-naïve patients and to 61% in previous non-responders to PR [36] (Fig. 2B). For G4-infected patients there isvery little data on interferon-free regimens, and no solid recom-mendations can be given in case of cirrhosis [20].
Specific features of interferon-free regimens in patients awaiting LTWith the current approval of sofosbuvir, simeprevir and daclatas-vir in the US and Europe, interferon-free regimens are being usedin those cirrhotic patients with compensated liver disease await-ing LT. In patients with decompensated liver disease, on the wait-ing list for LT, safety and efficacy data are still lacking and thus noclear recommendations can be given.
In any case, there are some distinct features that should betaken into consideration in individuals awaiting LT. The primarygoal of treatment in these patients is to prevent HCV graft infec-tion. Since the main source of virions (if not all) will be removed,this may be accomplished by a short course of antiviral therapy[29]. As shown above, sofosbuvir and ribavirin seem to be a goodchoice in this setting. There are, however, some problems associ-ated with this strategy: (1) timing of treatment is difficult (whento start?), (2) there is the possibility of post-LT relapse, and (3) ifa second DAA is added, there are no safety data in Child-Pugh Band Child-Pugh C patients and pharmacokinetic studies are notavailable for all drugs (Table 3). A second approach for treatingpatients on the waiting list may be to complete a full treatmentcourse to achieve SVR, not only to prevent graft infection but toassess if liver function improves. In some patients without HCC,the improvement in liver function and/or portal hypertensioncould imply delisting. In others, however, improvement maynot occur or may be insufficient for avoiding LT.
vol. 61 j S120–S131

Table 1. Phase 2 clinical trials with IFN-free regimens including cirrhotic patients.
Therapeutic regimen in trial arm including cirrhotic population(trial name)
Response to previous IFN based therapy
Lower limit of platelets(mm3)
Treatment duration in the specific arm (wk)
Cirrhotic patients enrolled in the studyN (%)
Genotypespectrum
SVR in cirrhotic patients
SOF + RBVNIH SPARE [94]
Naïve 75,000 24 13 (26)F3-4
1(G1a 70%)
SVR2450% and 29%(weight-based and low-dose RBV respectively)
SOF + RBV orGS-0938 orGS-0938 + SOF (± RBV)(QUANTUM) [95]
Naïve 50,000 1224
21 (9) 1-4 SVR12 50%(SOF + RBV arm, 24 wk)
SOF + LDV ± RBV(6th and 7th arms)(ELECTRON) [96]
Null-responder n.s. 12 19 (100) 1 SVR12100% and 70%(with and without RBV respectively)
SOF + LDV ± RBV (Cohort B)(LONESTAR) [97]
Non-responder to protease inhibitor regimen
n.s. 12 22 (55) 1(G1a 85%)
SVR12100% and 95%(with and without RBV respectively)
SOF + LDV(arm A)(NIAID SYNERGY) [98]
Naïve 50,000 12 3 (15) 1(G1a 55%)
SVR12 100%
SMV + SOF ± RBV (Cohort 2)(COSMOS) [30]
Naïve and null- responder
n.s. 1224
41 (25) 1(G1a 78%)
SVR1291% null-responders (21/33)94% naïve (17/18)
DCV + ASV + BMS-791325 [99]
Naïve n.s. 12 15 (9) 1(G1a 86%)
SVR1271% and 100% with 75 mg and 100 mg of BMS-791325 respectively
FDV + DBV ± RBV(SOUND C2) [100]
Naïve 90,000 16, 28, 40 33 (9) 1 SVR1233%-67%according to different regimen
FDV + DBV + RBV(SOUND C3) [101]
Naïve 75,000 16 4 (20) 1 SVR12100%
SOF + DCV ± RBV(A1444040) [31]
Naïve and treatment- experienced (also to protease inhibitors)
n.s. 1224
32 (15) 1-3 SVR12100%
SOF/LDV FDC ± RBV(ELECTRON-2) [102]
Naïve and treatment- experienced
50,000(CTP-A)
12 20 (100) G1* 8 (16) in G3
1,3 SVR12 G1 65%SVR12 G3 100% in LDV/SOF + RBV arm
MK-5172 + MK-8742 ± RBV(WORTHY) [103]
Null-responder 70,000 1218
123 (100) naïve and 51 (39) in NR
1 SVR8 94 and 100% in G1a and G1b respectively (both naïve and treatment- experienced)
SOF + RBV [39]* Naïve and treatment- experienced
n.s. 48 50 (100) 1-4 Week 24 of therapyHCV-RNA <LLOQ100% and 93% in CTP A and B respectively
⁄Including patients with decompensated cirrhosis.n.s., no specified platelet lower limit.wk, weeks; G, genotype; CTP, Child-Pugh; SVR12, sustained virologic response 12 weeks after the end of treatment; SVR24, sustained virologic response 24 weeks after theend of treatment.
Treatm
ent
JOURNAL OF HEPATOLOGY
A second distinct feature, particularly in those with decom-pensated disease, is the impact of liver function on drug pharma-cokinetics (PK): metabolic liver functions are significantlyinvolved in the total clearance of a number of drugs. PK studiesin patients with liver disease are an important clinical pharma-cology component of drug development [37]. PK data on a num-ber of new antivirals are already available and summarized inTable 3.
Journal of Hepatology 2014
As an example, exposure to sofosbuvir was 2-fold higher inHCV-infected patients without hepatic impairment, as comparedto patients with advanced liver disease. The latter group experi-enced a less profound viral decline than those with normal liverfunction when sofosbuvir was administered [38]. These data,supported by a recent study performed in decompensated cirrho-tics [39], may have clinical consequences and explain why inpatients with advanced liver disease longer treatment duration
vol. 61 j S120–S131 S123

Table 2. Phase 3 clinical trials with IFN-free regimens including cirrhotic patients.
Therapeutic regimen in trial arm including cirrhotic population(Trial name)
Response to previous IFN based therapy
Lower limit of platelets(mm3)
Treatment duration in
arm (wk)
Cirrhotic patients enrolled in the studyN (%)
Genotypespectrum
SVR in cirrhotic patients
SOF + RBV [104] Naïve and treatment- experienced
n.s. 1224
14 (23) 4 SVR1279% and 100% in naïve59% and 87% in treatment-experienced(12 and 24 wk respectively)
DCV + ASV + BMS-791325 [105]
Naïve n.s. 12 2 (10) 4 SVR12 100%
SOF + RBV(FISSION) [21]
Naïve 75,000 12 50 (20) 2, 3 SVR12 47%
SOF + RBV(POSITRON) [106]
IFN intolerant No lower limit
12 31 (15) 2, 3 SVR12 61%(G2 94% and G3 21%)
SOF + RBV(FUSION) [106]
Non-responder 50,000 1216
36 (35)32 (33)
2, 3 SVR12G2 60% and 78%G3 19% and 61%(12 and 16 wk respectively)
SOF + RBV(VALENCE) [36]
Naïve and treatment-experienced
50,000 12 G224 G3
10 (14) G259 (22) G3
2, 3(G3 78%)
SVR12 G2 100% and 88%G3 92% and 60%(naïve and treatment- experienced respectively)
LDV/SOF ± RBV(ION-1) [32]
Naïve 50,000 1224
136 (16) 1 SVR12 97 and 100% ± RBV (both 12 and 24 wk)
LDV/SOF ± RBV(ION-2) [33]
Treatment- experienced
50,000 1224
88 (20) 1 SVR12 82-86% 12 wk arm (± RBV) and 100% 24 wk arm
DCV + ASV [107] IFN ineligible naïve/intolerant and non-responder
n.s. 24 22 (10) 1b SVR24 90.9%
DCV + ASV (HALLMARK-DUAL) [35]
Naïve, IFN ineligible/intolerant and non-responder
n.s. 24 223 (30) 1b SVR1291%, 87% and 81% in naïve, non-responders and ineligible/intolerant respectively
ABT-450/r + ombitasvir + dasabuvir + RBV(TURQUOISE II) [34]
Naïve and treatment- experienced
60,000 1224
380 (100) 1 SVR12 91.8% and 95.9% in 12 and 24 wk
the specific
n.s., no specified platelet lower limit; W, weeks; G, genotype; CTP, Child-Pugh; SVR12, sustained virologic response 12 weeks after the end of treatment; SVR24, sustainedvirologic response 24 weeks after the end of treatment.
Treatm
ent
Journal of Hepatology Update: Hepatitis C
could be necessary to reduce the rates of virological relapse. Froma safety point of view, exposure to some new compounds (such asABT450/r) is significantly increased in Child-Pugh C patients andits use is currently not recommended. Adjustment of simepreviris not required in Child-Pugh class A or B patients [40], but par-ticular caution is recommended when prescribing simeprevir toHCV-infected patients with moderate or severe hepatic impair-ment since no studies in HCV-infected individuals are availableyet. In patients with severe hepatic impairment (Child-Pugh classC) simeprevir exposure is significantly increased and should beavoided [40] (Table 3).
A third distinct feature of patients awaiting LT is the poten-tial risk of viral breakthrough or relapse during or after treat-ment, which may theoretically induce flares that could triggerliver decompensation. It is thus very relevant to choose thebest treatment combination (high potency and high genetic
S124 Journal of Hepatology 2014
barrier) in order to minimize the possibility of virologicalrelapse or the selection of resistant-associated viral strains(RAVs). S282T is the only variant shown to confer reduced sus-ceptibility to sofosbuvir in vitro, but it has not been detected inpatients after virological failure. Differently, resistance to NS5A,non-nucleotide NS5B and NS3 protease inhibitors are fre-quently detected in individuals with virological failure. The fit-ness of resistant strains is usually lower than that of the wild-type viruses, which tend to progressively replace RAVs. NS5ARAVs, however, seem to persist for a long time. This is relevant,since the presence of multi-resistant strains may hamper anti-viral therapy if urgent treatment is required (such as in casesof decompensated cirrhosis with virological relapse or severehepatitis C recurrence after LT). A nucleotide-based regimen(such as sofosbuvir) appears to be the best salvage strategyin such cases.
vol. 61 j S120–S131

NaiveTreatment-exp. or IFN ineligible
G2 NaiveG2 Treatment-exp./IFN ineligibleG3 NaiveG3 Treatment-exp./IFN ineligible
0
20
40
60
80
100
SOF + LDV ± RBV
DCV + ASV ABT-450/r/O/D + RBV
132/1
3481
/88
98%92%
151/1
60
205/2
20
94% 93%91% 84%
29/32
145/1
73
SVR
12 (%
)A
B
0
20
40
60
80
100
12 12 16 12 24 12 16
83%
60%
78%
34%
92%
19%
61%60%
10/12 6/1
0 7/913
/3812
/13 5/26
14/23
2427
/45
SOF + RBV (wk)
SV
R12
(%)
Fig. 2. Efficacy results of phase 3 IFN-free therapies in cirrhotic patientsgenotype-1 (A) and genotypes 2/3 (B). SOF + LDV: sofosbuvir plus ledipasvirwith or without ribavirin 12-24 weeks (ION-1 [32] and 2 [33]). DCV + ASV:daclatasvir and asunaprevir for 24 weeks (only genotype 1b patients) [35]. ABT-450/r/O/D: ABT-450 boosted with ritonavir plus ombitasvir, dasabuvir andribavirin 12-24 weeks [34]. SOF + RBV: pooled data of sofosbuvir plus ribavirin12/16/24 weeks in the FISSION [21], FUSION [106] and VALENCE [36] studies.
Treatm
ent
Table 3. Pharmacokinetics (change in AUC) of DAAs in hepatic impairment(graded according to CTP score) and recommendation.
Drug CTP A (5-6 points)
CTP B (7-9 points)
CTP C (≥10 points)
Sofosbuvir [38,108] NR NPD NPDSimeprevir [109]† NR NR AUC x 3Daclatasvir [110, 111]¥ NR NR NRAsunaprevir [112] NR AUC x 9.8 AUC x 32Ledipasvir [113] NR NR NRABT-450/r [114]§ NR NR AUC x 11Dasabuvir [114] NR NR NROmbitasvir [114] NR NR NRMK-8742 [103] NR NR NPDMK-5172 [103] NR NR NPD
NR, dose adjustment not required; NPD, no pharmacokinetic data or studiesongoing.�AUC14 is given.¥AUCtau is given.§AUCinf is given.
JOURNAL OF HEPATOLOGY
Journal of Hepatology 2014
Management of patients with decompensated cirrhosiswithout an indication for LT
Patients with decompensated cirrhosis who are not candidatesfor LT are usually the elderly or those in whom the presence ofcomorbidities contraindicate a LT [41,42]. In these patients, theonly chance to improve or stabilize liver function is to eradicateHCV with an interferon-free regimen. Indeed, in those individualswithout comorbidities impairing their life expectancy, HCV erad-ication may be associated with clinical improvement and finallywith increased survival. Clinical trials in patients with decompen-sated disease should include ‘‘hard’’ end points: improvement inliver function, a decrease in clinical decompensation episodesand an increase in survival.
However, the impact of SVR in patients with decompensatedcirrhosis may be heterogeneous, since it encompasses a widespectrum of disease, ranging from patients with relatively well-preserved liver function (mild ascites or recent variceal bleeding)to patients with very poor liver function and a short life expec-tancy (Child-Pugh C >10 points) [43]. It is likely that in the lattergroup viral clearance will not significantly modify patients’ clin-ical outcomes or survival. Nevertheless, only well-designed stud-ies including appropriate control groups will be able to answerthese questions. Moreover, safety issues need to be carefullyaddressed in this patient population.
Preliminary results of the first study assessing the effect ofviral suppression on liver function were recently presented atthe EASL meeting (ILC 2014) [39]. In this study, cirrhotic patientswith documented portal hypertension and compensated ordecompensated cirrhosis (Child-Pugh 5–9 points) were random-ized to sofosbuvir and ribavirin for 48 weeks vs. an observationalarm (after 6 months these patients crossed over to the treatmentarm). From a virological point of view, it was interesting to learnthat 2 and 4 weeks after treatment initiation 56% and 100% ofChild-Pugh A patients had undetectable HCV-RNA; figures forChild-Pugh B patients were only 44% and 75%, respectively. Thismight be particularly relevant in patients awaiting LT (see above)where a short treatment course of therapy might not be sufficientto prevent post-LT relapse. After a 24-week period, the resultssuggested a reduction of ascites and hepatic encephalopathy epi-sodes in patients included in the treatment arm. However thestudy was not blinded (and a bias when assessing clinical out-comes cannot be excluded). More importantly, data on the effectof treatment on portal pressure are not available yet.
There are several studies assessing interferon-free combina-tions in patients with decompensated cirrhosis (Child-Pugh Band C) (Supplementary Table 1).
Treatment of hepatitis C recurrence after liver transplantation
HCV-related cirrhosis is the leading indication for LT in indus-trialized countries [44]. Virological recurrence after transplan-tation is constant in patients with detectable viraemia at thetime of LT [45]. The main characteristic of hepatitis C recur-rence after LT is the accelerated course of the disease whencompared to immunocompetent patients [46–50]. Approxi-mately one third of the patients progress to graft cirrhosiswithin only 5 years after transplantation [51,52]. This accelerated
vol. 61 j S120–S131 S125

Table 4. Drug-drug interactions between DAAs and calcineurin inhibitors.
DAA Cyclosporine TacrolimusHealthy volunteers Dose adjustment Healthy volunteers Dose adjustment
Boceprevir [115, 116]¥ AUC ↑ 2.7 fold ↓ 2 fold AUC ↑ 17 fold ↓ 5 foldTelaprevir [77, 117] ¥ AUC ↑ 4.6 fold ↓ 4 fold AUC ↑ 70 fold ↓ 35 foldABT450/r [86] AUC ↑ 5.8 fold ↓ 5 fold AUC ↑ 58 fold ↓ 100 foldSimeprevir [118]§ AUC ↑ 19% Under investigation AUC ↓ 17% Not necessarySofosbuvir [119]¥ No change Not necessary No change Not necessaryDaclatasvir [120] No change Not necessary No change Not necessary
¥AUCinf is given.§AUCLast is given.
Treatm
ent
Journal of Hepatology Update: Hepatitis C
fibrosis rate impacts both the allograft and recipient survivals,which are significantly reduced when compared with non-HCVLT recipients [46,50,51].
The effect of SVR on disease progression has been analysedin large cohorts of non-immune compromised patients, com-paring pre- and post-treatment liver biopsies. The data demon-strate improvements in inflammation and fibrosis scoresfollowing SVR [53–60], although in a non-homogeneous pattern(a subset of patients remains at the same stage, and some evendisplay persistent inflammation and/or fibrosis progression)[61]. The most important factor that determines fibrosis regres-sion after SVR is the baseline liver fibrosis stage [60]. Actually,the rate of cirrhosis regression has been estimated at 5–15%after ten years [60,61]. Early cirrhosis might be more likelyto regress than established cirrhosis. Old fibrous septa containhigh-density fibrillar collagens (I and III) and proteoglycans,pauci-cellularity and an increase in extracellular matrix (ECM)cross-linking, which may contribute to the resistance to fibrosisregression [62–65]. Elastin, which accumulates in mature cir-rhosis, is another non-collagenous matrix component that neg-atively influences fibrosis reversion [66,67]. Moreover, thepresence of established significant portal hypertension mayalso be determinant in fibrosis irreversibility, since it is associ-ated with an inflammatory state of the endothelium that inturn, may activate hepatic stellate cells (HSCs) and fibrogenesis[68–70].
The information available in liver transplant patients is scarce,but most likely these assumptions can be translated into LTpatients, particularly those who have developed cirrhosis overthe years. In patients who develop significant fibrosis (METAVIRF P2) during the first year, the situation may be different andfibrosis appears to be more reversible. Several studies haveshown a significant histological improvement or stabilizationafter SVR, in opposition to non-responders [71,72]. Similarly, por-tal pressure measurements and determinations of transient elas-tography also suggest a beneficial effect of antiviral treatment onliver fibrosis when SVR is achieved [72]. Probably the most strik-ing case is that of fibrosing cholestatic hepatitis (FCH), where avery early massive fibrosis deposition can reverse if treatedpromptly and viral clearance is achieved.
Interferon-based regimens to treat hepatitis C recurrence after LT
The most common approach to treat hepatitis C after LT has beento start antiviral therapy once the histological damage (in partic-ular liver fibrosis) is confirmed in the graft. The presence of
S126 Journal of Hepatology 2014
significant fibrosis beyond the portal tract (METAVIR F P2), por-tal hypertension (HVPG P6 mmHg) or high liver stiffness(>8.7 kPa) one year after LT accurately identify patients at higherrisk for clinical decompensation and death [73,74], who are inurgent need of treatment. In patients with a severe recurrenceoccurring during the first months after transplantation (i.e.,FCH), antiviral therapy is critical, but IFN-based regimens areunable to eradicate HCV in many cases, and patients die or needre-transplantation.
The overall SVR rates with PegIFN plus RBV are low; rangingbetween 30% and 40% across different series [71,75,76]. Thesemodest virological results are mainly explained by high rates oftreatment discontinuation (20–38%) and dose reductions (66–73%) due to adverse events. Liver transplant recipients are proneto haematological toxicity (particularly anaemia). RBV dosereductions and the use of erythropoietin (EPO) are very frequent(75–80%) in this setting [77]. The risk of rejection is small; in theorder of �5% in treated patients [78,79].
Regarding triple therapy with PIs in the post-LT setting, severalstudies have evaluated the safety and efficacy of such regimens inover 300 patients with hepatitis C recurrence [80–82]. Two thirdsof them received telaprevir and the rest were treated with boce-previr. Most of the patients had an advanced fibrosis stage (META-VIR F P2) or FCH. Approximately half of the patients had receiveda previous course of antiviral therapy. SVR12 rates rangedbetween 48% and 62% [80–82]. Despite the increased efficacy,the major concern of triple therapy in LT recipients is the high rateof SAEs leading to treatment discontinuation. Drug-drug interac-tions (DDIs) are an additional challenge when using telaprevirand boceprevir. First generation PIs are not only substrates, butalso inhibitors of the CYP3A4 system, thus strongly interactingwith many drugs. Due to the narrow therapeutic range of cyclo-sporine (CsA) and tacrolimus, dose adjustments are crucial andrequire very close monitoring when combined with PIs (Table 4).
Data from the only clinical trial assessing the safety and effi-cacy of telaprevir in the liver transplant setting were presentedat the recent EASL meeting [83]. This was an open-label, single-arm, study including 20 sites in Europe. Patients with hepatitisC recurrence, naïve to PR and with a METAVIR score of F0–F3underwent 12 weeks of triple therapy followed by 36 weeks ofPR. Tacrolimus or cyclosporine doses were adjusted on telaprevirinitiation and discontinuation. Final data from 74 patientsincluded in the study were available at time of writing thisreview and 53 (72%) had achieved SVR12. Nine (12%) patientshad 11 SAEs and no rejection episodes were diagnosed duringthe study period.
vol. 61 j S120–S131

0
20
40
60
80
100
PegIFNα + RBVPegIFNα + RBV + PISOF + RBVSOF + RBV + PegIFNαABT 450/r/O/D + RBV
30%
72%63%
50%
70%
96%
62%
SVR
12 (%
)
4848 24 24 24Weeks of treatment
Studies including alsopatients with severe hepatitis C
recurrence(METAVIR F4 or FCH)
Studies including patients with
METAVIR fibrosis score F <4
53/74
51/81
6/12
28/40
13/30
25/26
*
Fig. 3. Efficacy results of IFN-based and IFN-free regimens in liver transplantrecipients with hepatitis C recurrence after LT. ⁄Compassionate sofosbuvir useprogram including only patients with severe hepatitis C recurrence and a lifeexpectancy <12 months. O, ombitasvir; D, dasabuvir. PegIFN + RBV [75] and [76];PegIFN + RBV + PI: SVR12 72% [83]; SVR12 63% [82]; SVR12 50% [81]; SOF/RBV[84]; SOF/RBV ± PegIFN [85]; ABT450/r/O/D [86].
Treatm
ent
JOURNAL OF HEPATOLOGY
Interferon-free regimens after LTSofosbuvir and ribavirinSofosbuvir and RBV is the first interferon-free combination thathas been assessed in hepatitis C recurrence in a clinical trial[84]. A pilot single-arm study assessed the safety and efficacyof sofosbuvir 400 mg/d and RBV (dose escalating regimen startingat 400 mg/d) for 24 weeks in 40 patients with HCV recurrence(any genotype) at least 6 months after LT.
From the 40 patients, 33 were infected with G1. The studyincluded treatment-naïve and treatment-experienced patients(some with PIs); 40% were compensated cirrhotic patients. Theprimary efficacy end point was SVR12. Despite these characteris-tics, all individuals had HCV RNA <25 IU/ml at week 4 of treat-ment initiation. SVR12 was achieved in 28 (70%) of the 40patients (Fig 3). Ribavirin dose adjustments did not influenceSVR. These results can be considered excellent, particularly dueto the good tolerance: most side effects were mild and no rejec-tion episodes occurred during therapy. Despite the small samplesize and the lack of an interferon-based control arm in the study,the safety and tolerance profile of this combination seem signif-icantly better than that of the current standard-of-care.
Results from 104 HCV-infected LT recipients included in thecompassionate use program of sofosbuvir were recently pre-sented at the EASL meeting (ILC 2014) [85]. The antiviral regimenincluded sofosbuvir 400 mg/d for up to 48 weeks, with appropri-ate doses of RBV. PegIFN was added at the investigator’s discre-tion. The patients included in this program differedsubstantially from those included in the pilot study describedabove: approximately half of these patients had severe cholestat-ic hepatitis (some of them well-documented FCH) or were rapidfibrosers (METAVIR F P2 one year after LT); the remaining halfhad compensated or decompensated cirrhosis. Sixty patients(58%) presented an improved clinical condition (decrease ofhepatic encephalopathy episodes and/or improvement/disap-pearance of ascites). Although clinical improvement was assessedby the investigators (and a bias cannot be ruled out), liver func-tion tests (bilirubin, albumin, INR) improved remarkably overtime. The other 22 patients (21%) remained stable, while in 22(21%) the disease progressed or the patient died (n = 18). Fromthe 93 patients from whom HCV-RNA testing was available atthe end of treatment, 76 (82%) had HCV-RNA below LLOD; 53(62%) of 85 patients with more than 12 weeks of follow-up afterLT achieved SVR12. Severe adverse events were frequent, butthey were mostly attributed to disease progression. Overall, thepreliminary results of this program indicate that a regimen con-taining sofosbuvir was able to inhibit hepatitis C replication inmost patients, and that this was associated with an improvementin the clinical condition in a significant number of patients.Although longer follow-up is needed to assess the rate of SVRand its impact on disease progression, these results can be con-sidered very encouraging. A particularly relevant result of thisstudy was the excellent response in patients with cholestatichepatitis (including FCH), in which deeply perturbed laboratoryvalues (bilirubin, albumin, INR) returned to normal a few weeksafter treatment initiation and viral clearance. SVR12 in patientswith acute cholestatic hepatitis/fibrosing cholestatic hepatitiswas 70%, whereas SVR12 in those with compensated or decom-pensated cirrhosis points was 40% (Forns, personal communica-tion). The latter strongly suggests the benefit of early treatmentin severe forms of hepatitis C recurrence.
Journal of Hepatology 2014
ABT450/r, ombitasvir + dasabuvir and ribavirin in HCV-infected LTrecipientsIn this phase 2 study [86] the safety and efficacy of this 3 drugcombination, plus ribavirin administered during 24 weeks, wasassessed in 34 HCV-infected liver transplant patients. The initialribavirin dose was decided by the investigators. Individuals wereinfected with G1, were naïve after transplantation and had aMETAVIR score 6F2. Based on a previous DDI study, recommen-dations regarding immunosuppression were to reduce the tacrol-imus dose by 0.5 mg/week and cyclosporine to 1/5 at time ofantiviral treatment initiation. Preliminary analysis has shownthat all 34 patients had undetectable HCV-RNA at the end oftreatment, and 25 (96%) of 26 with sufficient follow-up achievedSVR12. The only patient who experienced relapse had RAVs(R155K in NS3 protease, M28T+Q30R in NS5A, andG554S+G557R in NS5B); none of these mutations present at base-line. Tolerance of this regimen was good; no episodes of rejectionwere reported.
Other IFN-free regimensSeveral clinical trials using different DAA combinations are cur-rently recruiting patients (Supplementary Table 1). In addition,analysis of expanded access programs (such as sofosbuvir anddaclatasvir) will also provide relevant practical information inthe next few months [87].
Specific features of interferon-free regimens in HCV-infected livertransplant recipientsTreatment with interferon-free regimens in patients with hepati-tis C recurrence is challenging for several reasons. Treatment maybe indicated in individuals with very aggressive forms of hepatitisC (such as FCH), which occur very early after transplantation. Thelatter poses several difficulties, since at this early period individ-uals are still under strong immunosuppression, at risk of oppor-tunistic infections, not uncommonly recovering or being treatedfrom surgical complications and undergoing treatment with mul-tiple drugs. Fortunately, many new anti-HCV compounds do notseem to have clinically significant interactions with CsA andtacrolimus (Table 4).
vol. 61 j S120–S131 S127

After liver transplantation Waiting list
SOF + RBV (± PegIFNα)
SOF/DCV + RBV
Awaiting data fromclinical trials
Compassionate use/EAP or clinical trials
SOF + RBVSOF/LDV + RBV#
Compassionate use/EAPor clinical trials
No indication for liver transplantation
Compensated cirrhosis
CTP-A (HCC)
Decompensated cirrhosis CTP B-C
Mild recurrence F0-1
Cholestatic HCV severe recurrence
F2-4
Decompensated cirrhosis CTP B-C
Clinical trials and/or EAPSOF + RBVSOF/DCV + RBVSOF/LDV + RBV#
MK-5172/MK-8742*
Individualize (nourgent need for therapy)
SOF + RBVSOF/SMV + RBV#§
SOF/DCV + RBV§
Clinical trials Compassionate use/EAP or clinical trials
SOF/LDV + RBV#SOF + RBVSOF/DCV + RBVSOF/LDV + RBV#
ABT-450/r/O/D + RBV¥
SMV/DCV + RBV#
SOF/LDV + RBV#
SOF/DCV + RBVSMV/DCV + RBV#
ABT-450/r/O/D + RBV¥
§
SOF + RBVSOF/SMV + RBV#§
SOF/DCV + RBV§
SOF/SMV + RBV#§
SOF/DCV + RBV
Fig. 4. Therapeutic approaches of HCV infection in 3 different patient populations: cirrhotic patients with decompensated disease without the indication of LT,patients on waiting list for LT and liver transplant recipients with hepatitis C recurrence after LT. #Only GT1,4; ⁄only GT1,4–6; ¥only GT1 (pending regulatoryapproval); EAP, expanded access program; O, ombitasvir; D, dasabuvir. § Very few data are available at this time.
Treatm
ent
Journal of Hepatology Update: Hepatitis C
Renal failure is also common in liver transplant recipients.Most patients have decreased glomerular filtration rate (GFR)due (at least in part) to the long-term use of cyclosporine ortacrolimus. Sofosbuvir, for instance, is not recommended if GFRis below 30 ml/min [88].
An issue that needs particular consideration in the liver trans-plant setting is that these patients usually have high viral loads,making it easier to select for drug resistant strains. The lattermight be particularly relevant in patients with FCH.
Treating before or after liver transplantation?
The negative impact of hepatitis C infection on liver transplantrecipients is well known. With a progressive increase in the ageof the donors in recent years [89–91], the proportion of patientswith severe forms of hepatitis C recurrence has increased andthese patients will require antiviral treatment [47,73,92]. Fur-thermore, they will have a complex follow-up and consume alot of resources: in most cases differential diagnosis from otherfrequent pathologies (such as rejection) is not easy. Adjustmentof immunosuppressive drugs is complicated and patients oftenrequire hospitalization. Thus, from a theoretical point of view,treatment before transplantation seems ideal, because it maysubstantially improve the post-transplant course, it may increasesurvival, and in some cases viral clearance may be associatedwith liver function improvement and delisting (important in acontext of organ shortage). However, before this strategy can beimplemented in clinical practice, we need data on the safetyand efficacy of interferon-free regimens in patients with decom-pensated cirrhosis and data on the impact of viral clearance onliver function. Furthermore, the time on waiting list for complet-ing antiviral therapy is usually unpredictable.
There are a number of patients who have already developedgraft damage following transplantation and for whom the onlychoice in the coming years will be interferon-free regimens.These patients include individuals with early severe recurrenceafter transplantation, non-responders and intolerant-to-interferon-based regimens, and patients with decompensated
S128 Journal of Hepatology 2014
cirrhosis. In the latter group, viral clearance in individuals withhigh MELD scores might permit considering them for retrans-plantation [93].
We will probably start answering all these questions in thenext months, when real-life data and results from ongoing clini-cal trials will gather relevant information that will help us choosethe best choice for each patient. Meanwhile, a suggestedapproach to these difficult-to-treat patients is shown in Fig 4.
Financial support
X. Forns received support in part by grants from Instituto deSalud Carlos III (PI11/01907), Ministerio de Economía y Compet-itividad, co-funded by Fondo Europeo de Desarrollo Regional,Unión Europea, Una manera de hacer Europa. X. Forns alsoreceived a grant from the Roche Organ Transplantation ResearchFoundation (ROTRF, CI: 442035057). M. Gambato has beenawarded with the EASL Entry Level Research Fellowship 2014(Dame Sheila Sherlock EASL Fellowship Programme).
Conflict of interest
X. Forns has acted as advisor for Janssen, Gilead and Abbvie, andhas received unrestricted grant support from MSD and Roche.S. Lens has acted as advisor for Gilead, MSD and Janssen. M. Navasahas acted as advisor for Novartis and Astellas. M. Gambato hasnothing to declare.
Authors’ contribution
All authors have substantially contributed to the conception,analysis, and interpretation of the data. All authors have contrib-uted in the drafting of the article, its critical revision for impor-tant intellectual content, have given final approval of theversion to be published, and agreement to be accountable forall aspects of the work in ensuring that questions related to theaccuracy or integrity of any part of the article.
vol. 61 j S120–S131

JOURNAL OF HEPATOLOGY
Supplementary dataSupplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.jhep.2014.07.020.
Treatm
ent
References
[1] Lange CM, Zeuzem S. Perspectives and challenges of interferon-free therapyfor chronic hepatitis C. J Hepatol 2013;58:583–592.
[2] Garcia-Retortillo M, Forns X. Prevention and treatment of hepatitis C virusrecurrence after liver transplantation. J Hepatol 2004;41:2–10.
[3] Crespo G, Marino Z, Navasa M, Forns X. Viral hepatitis in liver transplan-tation. Gastroenterology 2012;142:1373–1383.
[4] Forns X, Garcia-Retortillo M, Serrano T, Feliu A, Suarez F, de la Mata M, et al.Antiviral therapy of patients with decompensated cirrhosis to preventrecurrence of hepatitis C after liver transplantation. J Hepatol 2003;39:389–396.
[5] Peng CY, Chien RN, Liaw YF. Hepatitis B virus-related decompensated livercirrhosis: benefits of antiviral therapy. J Hepatol 2012;57:442–450.
[6] Kim WR, Terrault NA, Pedersen RA, Therneau TM, Edwards E, Hindman AA,et al. Trends in waiting list registration for liver transplantation for viralhepatitis in the United States. Gastroenterology 2009;137:1680–1686.
[7] Iacobellis A, Siciliano M, Perri F, Annicchiarico BE, Leandro G, Caruso N, et al.Peginterferon alfa-2b and ribavirin in patients with hepatitis C virusand decompensated cirrhosis: a controlled study. J Hepatol 2007;46:206–212.
[8] Carrion JA, Martinez-Bauer E, Crespo G, Ramirez S, Perez-del-Pulgar S,Garcia-Valdecasas JC, et al. Antiviral therapy increases the risk of bacterialinfections in HCV-infected cirrhotic patients awaiting liver transplantation:a retrospective study. J Hepatol 2009;50:719–728.
[9] Everson GT, Terrault NA, Lok AS, Rodrigo DR, Brown Jr RS, Saab S, et al. Arandomized controlled trial of pretransplant antiviral therapy to preventrecurrence of hepatitis c after liver transplantation. Hepatology2013;57:1752–1762.
[10] Everson GT, Trotter J, Forman L, Kugelmas M, Halprin A, Fey B, et al.Treatment of advanced hepatitis C with a low accelerating dosage regimenof antiviral therapy. Hepatology 2005;42:255–262.
[11] Coto-Llerena M, Perez-Del-Pulgar S, Crespo G, Carrion JA, Martinez SM,Sanchez-Tapias JM, et al. Donor and recipient IL28B polymorphisms inHCV-infected patients undergoing antiviral therapy before and after livertransplantation. Am J Transplant 2011;11:1051–1057.
[12] Poordad F, McCone Jr J, Bacon BR, Bruno S, Manns MP, Sulkowski MS, et al.Boceprevir for untreated chronic HCV genotype 1 infection. N Engl J Med2011;364:1195–1206.
[13] Jacobson IM, McHutchison JG, Dusheiko G, Di Bisceglie AM, Reddy KR,Bzowej NH, et al. Telaprevir for previously untreated chronic hepatitis Cvirus infection. N Engl J Med 2011;364:2405–2416.
[14] Sherman KE, Flamm SL, Afdhal NH, Nelson DR, Sulkowski MS, Everson GT,et al. Response-guided telaprevir combination treatment for hepatitis Cvirus infection. N Engl J Med 2011;365:1014–1024.
[15] Bacon BR, Gordon SC, Lawitz E, Marcellin P, Vierling JM, Zeuzem S, et al.Boceprevir for previously treated chronic HCV genotype 1 infection. N EnglJ Med 2011;364:1207–1217.
[16] Zeuzem S, Andreone P, Pol S, Lawitz E, Diago M, Roberts S, et al. Telaprevirfor retreatment of HCV infection. N Engl J Med 2011;364:2417–2428.
[17] Verna EC, Shetty K, Lukose T, Terry N, Mentore K, Olsen SK, et al. High post-transplant virologic response in hepatitis c virus infected patients treatedwith pre-transplant protease inhibitor-based triple therapy. Liver Int 2014.http://dx.doi.org/10.1111/liv.12616, [Epub ahead of print].
[18] Hezode C, Fontaine H, Dorival C, Larrey D, Zoulim F, Canva V, et al. Tripletherapy in treatment-experienced patients with HCV-cirrhosis in a multi-centre cohort of the French Early Access Programme (ANRS CO20-CUPIC) –NCT01514890. J Hepatol 2013;59:434–441.
[19] Rutter K, Ferlitsch A, Maieron A, Stattermayer A, Graziadei I, Dulic M, et al.Safety of triple therapy with telaprevir or boceprevir in hepatitis C patientswith advanced disease-predictive factors for sepsis. J Hepatol 2013;58:S30.
[20] Pawlotsky JM, Aghemo A, Dusheiko G, Forns X, Puoti M, Sarrazin C. EASLRecommendation on treatment of hepatitis C; 2014. Available from:<http://files.easl.eu/easl-recommendations-on-treatment-of-hepatitis-C/index.html>.
Journal of Hepatology 2014
[21] Lawitz E, Mangia A, Wyles D, Rodriguez-Torres M, Hassanein T, Gordon SC,et al. Sofosbuvir for previously untreated chronic hepatitis C infection. NEngl J Med 2013;368:1878–1887.
[22] Jacobson IM, Dore GJ, Foster GR, et al. Simeprevir with pegylated interferonalfa 2a plus ribavirin in treatment-naive patients with chronic hepatitis Cvirus genotype 1 infection (QUEST-1): a phase 3, randomised, double-blind,placebo-controlled trial. Lancet 2014;384(9941):403–413.
[23] Manns M, Marcellin P, Poordad F, et al. Simeprevir with pegylatedinterferon alfa 2a or 2b plus ribavirin in treatment-naive patients withchronic hepatitis C virus genotype 1 infection (QUEST-2): a randomised,double-blind, placebo-controlled phase 3 trial. Lancet 2014;384(9941):414–426.
[24] Forns X, Lawitz E, Zeuzem S, Gane E, Bronowicki JP, Andreone P, et al.Simeprevir with peginterferon and ribavirin leads to high rates of SVR inpatients with HCV genotype 1 who relapsed after previous therapy: a phase3 trial. Gastroenterology 2014;146(7):1669–1679.
[25] Zeuzem S, Berg T, Gane E, Ferenci P, Foster GR, Fried MW, et al. Simeprevirincreases rate of sustained virologic response among treatment-experi-enced patients with HCV genotype-1 infection: a phase IIb trial. Gastro-enterology 2014;146:430–441.
[26] Reddy K, Zeuzem S, Zoulim F, Weiland O, Horban A, Stanciu C, et al. A PhaseIII randomised, double-blind study to evaluate the efficacy, safety andtolerability of simeprevir vs. telaprevir in combination with pegylatedinterferon and ribavirin in chronic hepatitis C virus genotype 1 treatment-experienced patients: the ATTAIN study. In: (APASL) 24th Conference of theAsian Pacific Association for the Study of the Liver. Brisbane, Australia;2014.
[27] Hezode C, Hirschfield GM, Ghesquiere W, Sievert W, Rodriguez M, ShafranSD, et al. Daclatasvir, an NS5A replication complex inhibitor, combinedwith peginterferon Alfa-2a and ribavirin in treatment-naive HCV-genotype1 or 4 subjects: phase 2b COMMAND-1 SVR12 results. Hepatology2012;56:553A.
[28] Lawitz E, Poordad F, Brainard DM, Hyland RH, An D, Symonds WT, et al.Sofosbuvir in combination with PegIFN and ribavirin for 12 weeks provideshigh SVR rates in HCV-infected genotype 2 or 3 treatment- experiencedpatients with and without compensated cirrhosis: results from theLONESTAR-2 study. Hepatology 2013;58(6):LB–4.
[29] Curry MP, Forns X, Chung RT, Terrault N, Brown Jr RS, Fenkel JM, et al.Pretransplant sofosbuvir and ribavirin to prevent recurrence of HCVinfection after liver transplantation. Hepatology 2013;58:314A.
[30] Lawitz E, Sulkowski MS, Ghalib R, et al. Simeprevir plus sofosbuvir, with orwithout ribavirin, to treat chronic infection with hepatitis C virus genotype1 in non-responders to pegylated interferon and ribavirin and treatment-naive patients: the COSMOS randomised study. Lancet 2014;58. http://dx.doi.org/10.1016/S0140-6736(14)61036-9, [Epub ahead of print].
[31] Sulkowski MS, Gardiner DF, Rodriguez-Torres M, Reddy KR, Hassanein T,Jacobson I, et al. Daclatasvir plus sofosbuvir for previously treated oruntreated chronic HCV infection. N Engl J Med 2014;370:211–221.
[32] Afdhal N, Zeuzem S, Kwo P, Chojkier M, Gitlin N, Puoti M, et al. Ledipasvirand sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med2014;370:1889–1898.
[33] Afdhal N, Reddy KR, Nelson DR, Lawitz E, Gordon SC, Schiff E, et al.Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection.N Engl J Med 2014;370:1483–1493.
[34] Poordad F, Hezode C, Trinh R, Kowdley KV, Zeuzem S, Agarwal K, et al. ABT-450/r-ombitasvir and dasabuvir with ribavirin for hepatitis C with cirrho-sis. N Engl J Med 2014;370:1973–1982.
[35] Manns M, Pol S, Jacobson I, Marcellin P, Gordon S, Peng C-Y, et al. All-oraldual therapy with daclatasvir and asunaprevir in patients with HCVgenotype 1b infection: phase 3 study results. J Hepatol 2014;60:S524.
[36] Zeuzem S, Dusheiko GM, Salupere R, Mangia A, Flisiak R, Hyland RH, et al.Sofosbuvir and ribavirin in HCV genotypes 2 and 3. N Engl J Med2014;370:1993–2001.
[37] Guidance for industry pharmacokinetics in patients with impaired hepaticfunction: study design, data analysis, and impact on dosing and labeling.[cited; Available from] <http://wwwfdagov/downloads/Drugs/Guidance-ComplianceRegulatoryInformation/Guidances/ucm072123pdf>.
[38] Lawitz E, Rodriguez-Torres M, Cornpropst M, Denning JM, Clemons D,McNair L, et al. The effect of hepatic impairment on the pharmacokineticsand antiviral activity of PSI-7977 in hepatitis C infected subjects treated forseven days. J Hepatol 2012;56:S398.
[39] Afdhal N, Everson G, Calleja JL, McCaughan G, Symonds WT, Denning J, et al.Sofosbuvir and ribavirin for the treatment of chronic HCV with cirrhosisand portal hypertension with and without decompensation: early virologicresponse and safety. J Hepatol 2014;60:S28.
vol. 61 j S120–S131 S129

Treatm
ent
Journal of Hepatology Update: Hepatitis C
[40] Ouwerkerk-Mahadevan S, Simion A, Spittaels K, Beumont-Mauviel M, et al.Pharmacokinetics of simeprevir (TMC435) in volunteers with moderate orsevere hepatic impairment. J Hepatol 2013;58:S365.
[41] Lucey MR, Brown KA, Everson GT, Fung JJ, Gish R, Keefe EB, et al. Minimalcriteria for placement of adults on the liver transplant waiting list: a reportof a national conference organized by the American Society of TransplantPhysicians and the American Association for the Study of Liver Diseases.Transplantation 1998;66:956–962.
[42] Collins BH, Pirsch JD, Becker YT, Hanaway MJ, Van der Werf WJ,D’Alessandro AM, et al. Long-term results of liver transplantation in olderpatients 60 years of age and older. Transplantation 2000;70:780–783.
[43] Planas R, Balleste B, Alvarez MA, Rivera M, Montoliu S, Galeras JA, et al.Natural history of decompensated hepatitis C virus-related cirrhosis. Astudy of 200 patients. J Hepatol 2004;40:823–830.
[44] Adam R, McMaster P, O’Grady JG, Castaing D, Klempnauer JL, Jamieson N,et al. Evolution of liver transplantation in Europe: report of the EuropeanLiver Transplant Registry. Liver Transpl 2003;9:1231–1243.
[45] Garcia-Retortillo M, Forns X, Feliu A, Moitinho E, Costa J, Navasa M, et al.Hepatitis C virus kinetics during and immediately after liver transplanta-tion. Hepatology 2002;35:680–687.
[46] Belli LS, Burroughs AK, Burra P, Alberti AB, Samonakis D, Camma C, et al.Liver transplantation for HCV cirrhosis: improved survival in recent yearsand increased severity of recurrent disease in female recipients: results of along term retrospective study. Liver Transpl 2007;13:733–740.
[47] Berenguer M, Ferrell L, Watson J, Prieto M, Kim M, Rayon M, et al. HCV-related fibrosis progression following liver transplantation: increase inrecent years. J Hepatol 2000;32:673–684.
[48] Yilmaz N, Shiffman ML, Stravitz RT, Sterling RK, Luketic VA, Sanyal AJ, et al.A prospective evaluation of fibrosis progression in patients with recurrenthepatitis C virus following liver transplantation. Liver Transpl2007;13:975–983.
[49] Walter T, Dumortier J, Guillaud O, Hervieu V, Scoazec JY, Boillot O. Factorsinfluencing the progression of fibrosis in patients with recurrent hepatitis Cafter liver transplantation under antiviral therapy: a retrospective analysisof 939 liver biopsies in a single center. Liver Transpl 2007;13:294–301.
[50] Neumann UP, Berg T, Bahra M, Seehofer D, Langrehr JM, Neuhaus R, et al.Fibrosis progression after liver transplantation in patients with recurrenthepatitis C. J Hepatol 2004;41:830–836.
[51] Forman LM, Lewis JD, Berlin JA, Feldman HI, Lucey MR. The associationbetween hepatitis C infection and survival after orthotopic liver transplan-tation. Gastroenterology 2002;122:889–896.
[52] Gane EJ. The natural history of recurrent hepatitis C and what influencesthis. Liver Transpl 2008;14:S36–S44.
[53] Lee YA, Friedman SL. Reversal, maintenance or progression: what happensto the liver after a virologic cure of hepatitis C? Antiviral Res2014;12:23–30.
[54] Shiratori Y, Imazeki F, Moriyama M, Yano M, Arakawa Y, Yokosuka O, et al.Histologic improvement of fibrosis in patients with hepatitis C who havesustained response to interferon therapy. Ann Intern Med2000;132:517–524.
[55] Balart LA, Lisker-Melman M, Hamzeh FM, Kwok A, Lentz E, Rodriguez-Torres M. Peginterferon alpha-2a plus ribavirin in Latino and Non-LatinoWhites with HCV genotype 1: histologic outcomes and tolerability from theLATINO Study. Am J Gastroenterol 2010;105:2177–2185.
[56] D’Ambrosio R, Aghemo A, Rumi MG, Ronchi G, Donato MF, Paradis V, et al. Amorphometric and immunohistochemical study to assess the benefit of asustained virological response in hepatitis C virus patients with cirrhosis.Hepatology 2012;56:532–543.
[57] George SL, Bacon BR, Brunt EM, Mihindukulasuriya KL, Hoffmann J, DiBisceglie AM. Clinical, virologic, histologic, and biochemical outcomes aftersuccessful HCV therapy: a 5-year follow-up of 150 patients. Hepatology2009;49:729–738.
[58] Manns MP, Pockros PJ, Norkrans G, Smith CI, Morgan TR, Haussinger D,et al. Long-term clearance of hepatitis C virus following interferon alpha-2bor peginterferon alpha-2b, alone or in combination with ribavirin. J ViralHepat 2013;20:524–529.
[59] Maylin S, Martinot-Peignoux M, Moucari R, Boyer N, Ripault MP, Cazals-Hatem D, et al. Eradication of hepatitis C virus in patients successfullytreated for chronic hepatitis C. Gastroenterology 2008;135:821–829.
[60] Poynard T, McHutchison J, Manns M, Trepo C, Lindsay K, Goodman Z, et al.Impact of pegylated interferon alfa-2b and ribavirin on liver fibrosis inpatients with chronic hepatitis C. Gastroenterology 2002;122:1303–1313.
[61] Poynard T, Moussalli J, Munteanu M, Thabut D, Lebray P, Rudler M, et al.Slow regression of liver fibrosis presumed by repeated biomarkers after
S130 Journal of Hepatology 2014
virological cure in patients with chronic hepatitis C. J Hepatol2013;59:675–683.
[62] Schuppan D, Ruehl M, Somasundaram R, Hahn EG. Matrix as a modulator ofhepatic fibrogenesis. Semin Liver Dis 2001;21:351–372.
[63] Schuppan D, Krebs A, Bauer M, Hahn EG. Hepatitis C and liver fibrosis. CellDeath Differ 2003;10:S59–S67.
[64] Issa R, Zhou X, Trim N, Millward-Sadler H, Krane S, Benyon C, et al.Mutation in collagen-1 that confers resistance to the action of collagenaseresults in failure of recovery from CCl4-induced liver fibrosis, persistence ofactivated hepatic stellate cells, and diminished hepatocyte regeneration.FASEB J 2003;17:47–49.
[65] Issa R, Zhou X, Constandinou CM, Fallowfield J, Millward-Sadler H, GacaMD, et al. Spontaneous recovery from micronodular cirrhosis: evidence forincomplete resolution associated with matrix cross-linking. Gastroenter-ology 2004;126:1795–1808.
[66] Pellicoro A, Aucott RL, Ramachandran P, Robson AJ, Fallowfield JA, SnowdonVK, et al. Elastin accumulation is regulated at the level of degradation bymacrophage metalloelastase (MMP-12) during experimental liver fibrosis.Hepatology 2012;55:1965–1975.
[67] Pellicoro A, Ramachandran P, Iredale JP. Reversibility of liver fibrosis.Fibrogenesis Tissue Repair 2012;5:S26.
[68] Roberts S, Gordon A, McLean C, Pedersen J, Bowden S, Thomson K, et al.Effect of sustained viral response on hepatic venous pressure gradient inhepatitis C-related cirrhosis. Clin Gastroenterol Hepatol 2007;5:932–937.
[69] Friedman SL. Mechanisms of hepatic fibrogenesis. Gastroenterology2008;134:1655–1669.
[70] Wiest R, Groszmann RJ. The paradox of nitric oxide in cirrhosis and portalhypertension: too much, not enough. Hepatology 2002;35:478–491.
[71] Berenguer M, Palau A, Aguilera V, Rayon JM, Juan FS, Prieto M. Clinicalbenefits of antiviral therapy in patients with recurrent hepatitis C followingliver transplantation. Am J Transplant 2008;8:679–687.
[72] Carrion JA, Navasa M, Garcia-Retortillo M, Garcia-Pagan JC, Crespo G,Bruguera M, et al. Efficacy of antiviral therapy on hepatitis C recurrenceafter liver transplantation: a randomized controlled study. Gastroenterol-ogy 2007;132:1746–1756.
[73] Blasco A, Forns X, Carrion JA, Garcia-Pagan JC, Gilabert R, Rimola A, et al.Hepatic venous pressure gradient identifies patients at risk of severehepatitis C recurrence after liver transplantation. Hepatology2006;43:492–499.
[74] Carrion JA, Navasa M, Bosch J, Bruguera M, Gilabert R, Forns X. Transientelastography for diagnosis of advanced fibrosis and portal hypertension inpatients with hepatitis C recurrence after liver transplantation. LiverTranspl 2006;12:1791–1798.
[75] Wang CS, Ko HH, Yoshida EM, Marra CA, Richardson K. Interferon-basedcombination anti-viral therapy for hepatitis C virus after liver transplan-tation: a review and quantitative analysis. Am J Transplant2006;6:1586–1599.
[76] Xirouchakis E, Triantos C, Manousou P, Sigalas A, Calvaruso V, Corbani A,et al. Pegylated-interferon and ribavirin in liver transplant candidates andrecipients with HCV cirrhosis: systematic review and meta-analysis ofprospective controlled studies. J Viral Hepat 2008;15:699–709.
[77] Coilly A, Roche B, Samuel D. Current management and perspectives for HCVrecurrence after liver transplantation. Liver Int 2013;33:56–62.
[78] Chalasani N, Manzarbeitia C, Ferenci P, Vogel W, Fontana RJ, Voigt M, et al.Peginterferon alfa-2a for hepatitis C after liver transplantation: tworandomized, controlled trials. Hepatology 2005;41:289–298.
[79] Samuel D, Bizollon T, Feray C, Roche B, Ahmed SN, Lemonnier C, et al.Interferon-alpha 2b plus ribavirin in patients with chronic hepatitis C afterliver transplantation: a randomized study. Gastroenterology2003;124:642–650.
[80] Faisal N, Renner EL, Bilodeau M, Yoshida EM, Wong P, Ma MM, et al.Protease inhibitor-based triple therapy is highly effective in liver transplantrecipients with genotype 1 hepatitis C recurrence: a Canadian multicentreexperience. Hepatology 2013;58:238A.
[81] Coilly A, Roche B, Dumortier J, Leroy V, Botta-Fridlund D, Radenne S, et al.Safety and efficacy of protease inhibitors to treat hepatitis C after livertransplantation: a multicenter experience. J Hepatol 2013;60:78–86.
[82] Burton Jr JR, O’Leary JG, Verna EC, Saxena V, Dodge JL, Stravitz RT, et al. A usmulticenter study of hepatitis C treatment of liver transplant recipientswith protease-inhibitor triple therapy. J Hepatol 2014;61(3):508–514.
[83] Forns X, Samuel D, Mutimer D, Fagiouli S, Navasa M, Agarwal K, et al.Interim SVR12 results from the telaprevir phase3B REPLACE study intreatment-naive stable liver transplant patients with genotype 1 HCVinfection. J Hepatol 2014;60:S481.
vol. 61 j S120–S131

Treatm
ent
JOURNAL OF HEPATOLOGY
[84] Samuel D, Charlton M, Gane E, Brown Jr R, Curry M, Kwo P, et al. Sofosbuvirand ribavirin for the treatment of recurrent hepatitis C infection after livertransplantation: results of a prospective, multicenter study. J Hepatol2014;60:S499.
[85] Forns X, Prieto M, Charlton M, McHutchinson JG, Symonds WT, Denning JM,et al. Sofosbuvir compassionate use program for patients with severerecurrent hepatitis C including fibrosing cholestatic hepatitis followingliver transplantation. J Hepatol 2014;60:S26.
[86] Kwo P, Mantry P, Coakley E, Te H, Vargas H, Brown Jr R, et al. Results of thephase 2 study M12–999: interferon-free regimen of ABT-450/r/ABT-267 + ABT-333 + ribavirin in liver transplant recipients with recurrentHCV genotype 1 infection. J Hepatol 2014;60:S47.
[87] Pellicelli AM, Lionetti R, Montalbano M, Durand C, Ferenci P, D’Offizi G,et al. Sofosbuvir and daclatasvir for recurrent hepatitis C after livertransplantation: potent antiviral activity but lack of clinical benefit iftreatment is given too late. J Hepatol 2014;60:S532.
[88] Cornpropst M, Denning J, Clemons D, et al. The effect of renal impairmentand end stage renal disease on the single-dose pharmacokinetics of PSI-7977. J Hepatol 2012;56:S433.
[89] Sela N, Croome KP, Chandok N, Marotta P, Wall W, Hernandez-Alejandro R.Changing donor characteristics in liver transplantation over the last 10years in canada. Liver Transpl 2013;19:1236–1244.
[90] Halldorson J, Roberts JP. Decadal analysis of deceased organ donation inSpain and the United States linking an increased donation rate and theutilization of older donors. Liver Transpl 2013;19:981–986.
[91] Duarte-Rojo A, Veldt BJ, Goldstein DD, Tillman HL, Watt KD, Heimbach JK,et al. The course of posttransplant hepatitis C infection: comparativeimpact of donor and recipient source of the favorable IL28B genotype andother variables. Transplantation 2012;94:197–203.
[92] Crespo G, Lens S, Gambato M, Carrion JA, Marino Z, Londono MC, et al. Liverstiffness 1 year after transplantation predicts clinical outcomes in patientswith recurrent hepatitis C. Am J Transplant 2014;14:375–383.
[93] Carrion JA, Navasa M, Forns X. Retransplantation in patients with hepatitisC recurrence after liver transplantation. J Hepatol 2010;53:962–970.
[94] Osinusi A, Meissner EG, Lee YJ, Bon D, Heytens L, Nelson A, et al. Sofosbuvirand ribavirin for hepatitis C genotype 1 in patients with unfavorabletreatment characteristics: a randomized clinical trial. JAMA2013;310:804–811.
[95] Lalazeri J, Nelson D, Hyland R, et al. Once-daily sofosbuvir plus ribaviringiven for 12 or 24 weeks in treatment-naïve patients with HCV: theQUANTUM study. J Hepatol 2013;58:S346.
[96] Gane EJ, Stedman CA, Hyland RH, Ding X, Svarovskaia E, Subramanian GM,et al. Efficacy of nucleotide polymerase inhibitor sofosbuvir plus the NS5AInhibitor ledipasvir or the NS5B non-nucleoside inhibitor GS-9669 againstHCV genotype 1 infection. Gastroenterology 2013;146:736–743.
[97] Lawitz E, Poordad FF, Pang PS, Hyland RH, Ding X, Mo H, et al. Sofosbuvirand ledipasvir fixed-dose combination with and without ribavirin intreatment-naive and previously treated patients with genotype 1 hepatitisC virus infection (LONESTAR): an open-label, randomised, phase 2 trial.Lancet 2013;383:515–523.
[98] Kohli A, Sims Z, Marti M, et al. Combination oral, Ribavirin free, antiviraltherapy to optimize treatment outcomes for Hepatitis C treatment naïvepatients: interim results from the NIAID SYNERGY trial. Hepatology2013;58:LB–8.
[99] Everson G, Sims K, Thuluvath P, et al. Phase 2b study of the interferon-freeand ribavirin-free combination of daclatasvir, asunaprevir and BMS-791325 for 12 weeks in treatment-naive patients with chronic HCVgenotype 1 infection. Hepatology 2013;58:LB-1.
[100] Zeuzem S, Soriano V, Asselah T, Bronowicki JP, Lohse AW, Mullhaupt B,et al. Faldaprevir and deleobuvir for HCV genotype 1 infection. N Engl J Med2013;369:630–639.
[101] Dufour J-F, Buti M, Soriano V, et al. Interferon-free treatment withfaldaprevir, deleobuvir (BI 207127) and ribavirin in SOUND-C3: 95%SVR12 in HCV-GT1b. Hepatology 2013;58:744A.
[102] Gane EJ, Hyland RH, An D, Pang PS, Symonds WT, Mchutchison JG, et al.Sofosbuvir/ledipasvir fixed dose combination is safe and effective in
Journal of Hepatology 2014
difficult-to-treat populations including genotype-3 patients, decompen-sated genotype-1 patients, and genotype-1 patients with prior sofosbuvirtreatment experience. J Hepatol 2014;60:S3.
[103] Lawitz E, Hezode C, Gane E, Tam E, Lagging M, Balart L, et al. Efficacy andsafety of MK-5172 AND MK-8742 ± ribavirin in hepatitis C genotype 1infected patients with cirrhosis or previous null-response: the C-WORTHYStudy. J Hepatol 2014;60:S25.
[104] Ruane P, Ain D, Meshrekey J, Riad J, Stryker R, Soliman M, et al. Sofosbuvirplus ribavirin, an interferon-free regimen, in the treatment of treatment-naive and treatment-experienced patients with chronic genotype 4 HCVinfection. Hepatology 2013;58:736A.
[105] Adamczyk R, Sims K, Chang I, Filoramo D, Pursley J, Charlton S, et al.Daclatasvir, asunaprevir, and BMS-791325 in a fixed-dose combination: aphase 1 bioavailability study in healthy volunteers. J Hepatol2014;60:S468.
[106] Jacobson IM, Gordon SC, Kowdley KV, Yoshida EM, Rodriguez-Torres M,Sulkowski MS, et al. Sofosbuvir for hepatitis C genotype 2 or 3 in patientswithout treatment options. N Engl J Med 2013;368:1867–1877.
[107] Chayama K, Suzuki Y, Ikeda K, et al. All-oral combination of daclatasvir plusasunaprevir in interferon ineligible naive/intolerant and nonresponderJapanese patients chronically infected with HCV genotype 1b: results froma phase 3 trial. Hepatology 2013;58:313A.
[108] Mariño Z, van Bommel F, Forns X, Berg T. New concepts of sofosbuvir-basedtreatment regimens in patients with hepatitis C. Gut 2014;63(2):207–215.
[109] Sekar V, Simion A, Peeters M, et al. Pharmacokinetics of TMC435 in subjectswith moderate hepatic impairment. J Hepatol 2011;54:S193.
[110] Bifano M, Sevinsky H, Persson A, et al. Single-dose pharmacokinetics ofdaclatasvir (DCV; BMS-790052) in subjects with hepatic impairmentcompared with healthy subjects. Hepatology 2011;54:1004A.
[111] Lee C. Daclatasvir: potential role in hepatitis C. Drug Des Devel Ther2013;7:1223–1233.
[112] Eley T, He B, Chang I, et al. The effect of hepatic impairment on thepharmacokinetics of asunaprevir, an HCV NS3 protease inhibitor. AntivirTher 2014. http://dx.doi.org/10.3851/IMP2773, [Epub ahead of print].
[113] German P, Mathias A, Yang J, et al. The pharmacokinetics of ledipasvir, anHCV specific NS5A inhibitor in HCV-uninfected subjects with moderate andsevere hepatic impairment. Hepatology 2013;58:432–433A.
[114] Khatri A, Gaultier I, Menon R, et al. Pharmacokinetics and safety of co-administered ABT-450 plus ritonavir (ABT 450/r), ABT-267, and ABT-333 asa single dose in subjects with normal hepatic function and in subjects withmild, moderate and severe hepatic impairment. Hepatology 2012;56:555A.
[115] Hulskotte E, Gupta S, Xuan F, van Zutven M, O’Mara E, Feng HP, et al.Pharmacokinetic interaction between the hepatitis C virus proteaseinhibitor boceprevir and cyclosporine and tacrolimus in healthy volun-teers. Hepatology 2012;56:1622–1630.
[116] Coilly A, Furlan V, Roche B, Barau C, Noel C, Bonhomme-Faivre L, et al.Practical management of boceprevir and immunosuppressive therapy inliver transplant recipients with hepatitis C virus recurrence. AntimicrobAgents Chemother 2012;56:5728–5734.
[117] Garg V, van Heeswijk R, Lee JE, Alves K, Nadkarni P, Luo X. Effect oftelaprevir on the pharmacokinetics of cyclosporine and tacrolimus. Hepa-tology 2011;54:20–27.
[118] Ouwerkerk-Mahadevan S, Simion A, Mortier S, Peeters M, Beumont-Mauviel M. No clinically significant interaction between the investigationalHCV protease inhibitor TMC435 and the immunosuppressives cyclosporineand tacrolimus. Hepatology 2012;56:231A.
[119] Mathias A, Cornpropst M, Clemons D, et al. No clinically significantpharmacokinetic drug-drug interactions between sofosbuvir (GS-7977)and the immunosuppressants, cyclosporine A or tacrolimus in healthyvolunteers. Hepatology 2012;56:1063A–1064A.
[120] Fontana RJ, Hughes EA, Appelman H, Hindes R, Dimitrova D, Bifano M. Casereport of successful peginterferon, ribavirin, and daclatasvir therapy forrecurrent cholestatic hepatitis C after liver retransplantation. Liver Transpl2012;18:1053–1059.
vol. 61 j S120–S131 S131