Treatment of thoracoabdominal aortic aneurysms. surgery alone or hybrid
79
Lenox Hill Heart and Vascular Institute of New York Treatment of Thoracoabdominal Aortic Aneurysms. Surgery alone or Hybrid. Konstadinos A Plestis, MD Associate Professor Director of Aortic Surgery Department of Thoracic and Cardiovascular Surgery Lenox Hill Hospital, NY
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
237 -
download
2
Transcript of Treatment of thoracoabdominal aortic aneurysms. surgery alone or hybrid

Lenox Hill Heart and VascularInstitute of New York
Treatment of Thoracoabdominal Aortic Aneurysms. Surgery alone or Hybrid.
Konstadinos A Plestis, MD
Associate Professor
Director of Aortic Surgery
Department of Thoracic and Cardiovascular Surgery
Lenox Hill Hospital, NY

Lenox Hill Heart and VascularInstitute of New York
The Risk of ParaplegiaCrawford Classification (n = 1509)
I II III IV
15% 31% 7% 4%
Svensson LG, Crawford ES: J Vasc Surg 1993; 17:357-370

Lenox Hill Heart and VascularInstitute of New York
Open Surgical Treatment
Extensive Operations
Need of CPB + DHCA
Risk of Paraplegia
Post-operative Mortality and Morbidity

Lenox Hill Heart and VascularInstitute of New York
Endovascular Treatment
Decreases Access Trauma
Decreases Blood Loss
Reduces Morbidity and Mortality?
Improves long term outcomes?

Lenox Hill Heart and VascularInstitute of New York
Hybrid repair
Kuratani et al

Lenox Hill Heart and VascularInstitute of New York
Debranching + stent
Hughes et al

Lenox Hill Heart and VascularInstitute of New York
Debranching + stent
Kabbani et al
Lenox Hill Heart and VascularInstitute of New York
Spinal Cord Protection
Cerebral Protection
Visceral Organ Protection
Goals during Open Repair of TA Aneurysms

Lenox Hill Heart and VascularInstitute of New York
Current Lenox Hill Technique
Mild systemic hypothermia, 32°C
Distal perfusion
CSF drainage
Monitoring of SSEP and MEP
Spinal cord perfusion pressure (SCPP) monitoring

Lenox Hill Heart and VascularInstitute of New York
DHCA: Indications
Proximal clamping is not feasible
Need to clamp above the left subclavian
Type II Aneurysms?

Lenox Hill Heart and VascularInstitute of New York
CSF Drainage Technique
CSF catheter : L4-L5 or L3-4
CSF pressure < 10mmHg
CSF drainage: 10 cc/h
CSF drainage for 2-3 days
Lenox Hill Heart and VascularInstitute of New York
Current Lenox Hill Technique
Mean BP: 85-95mmHg
CSF drainage for 72-96 hr
CSF drainage at 10 cc/hr
SCPP monitoring
Steroids for 48 hrs
Postoperative Management
Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
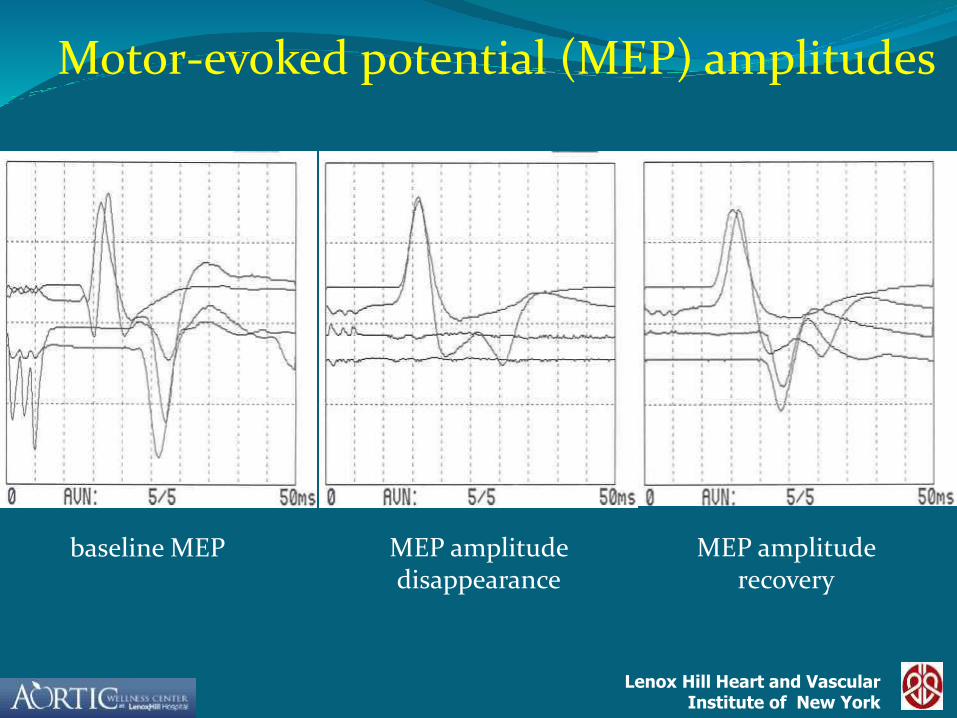
Motor-evoked potential (MEP) amplitudes
baseline MEP MEP amplitude disappearance
MEP amplitude recovery

Lenox Hill Heart and VascularInstitute of New York
CASE PRESENTATION
42 yo patient
Distal Arch/ Type I TAAA

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Visceral Perfusion
Is it necessary?

Lenox Hill Heart and VascularInstitute of New York
BUN
23.7
30.4
17.04
20.4
38.1
24.2
19.3
40.5
26.2
Pre OP Highest End
NO DHCA
BUN (all cases)
DHCA
=p<.05

Lenox Hill Heart and VascularInstitute of New York
CREATNINE
1.49
2.03
1.431.48
2.92
2.06
1.48
2.83
1.98
Pre OP Highest End
NO DHCA
Creatnine (all cases)
DHCA

Lenox Hill Heart and VascularInstitute of New York
AMYLASE
54
428
194
61
175
7962
148
62
Pre Op Highest End
DHCA
Amylase (all cases)
NO DHCA

Lenox Hill Heart and VascularInstitute of New York
Total Bilirubin
0.65
2.75
1.23
0.66
2.85
1.170.68
3.46
0.81
Pre OP Highest End
NO DHCA
T. Bilirubin (all cases)
DHCA

Lenox Hill Heart and VascularInstitute of New York
SGOT
16
344
3722
137
3323 102
36
Pre OP Highest End
DHCA
SGOT (all cases)
NO DHCA

Lenox Hill Heart and VascularInstitute of New York
16
220
54
19
84
362062
33
Pre OP Highest End
DHCA
SGPT (all cases)
NO DHCA
SGPT

Lenox Hill Heart and VascularInstitute of New York
Visceral Perfusion
Dilute Blood
Rate at 100-200 cc/min

Lenox Hill Heart and VascularInstitute of New York
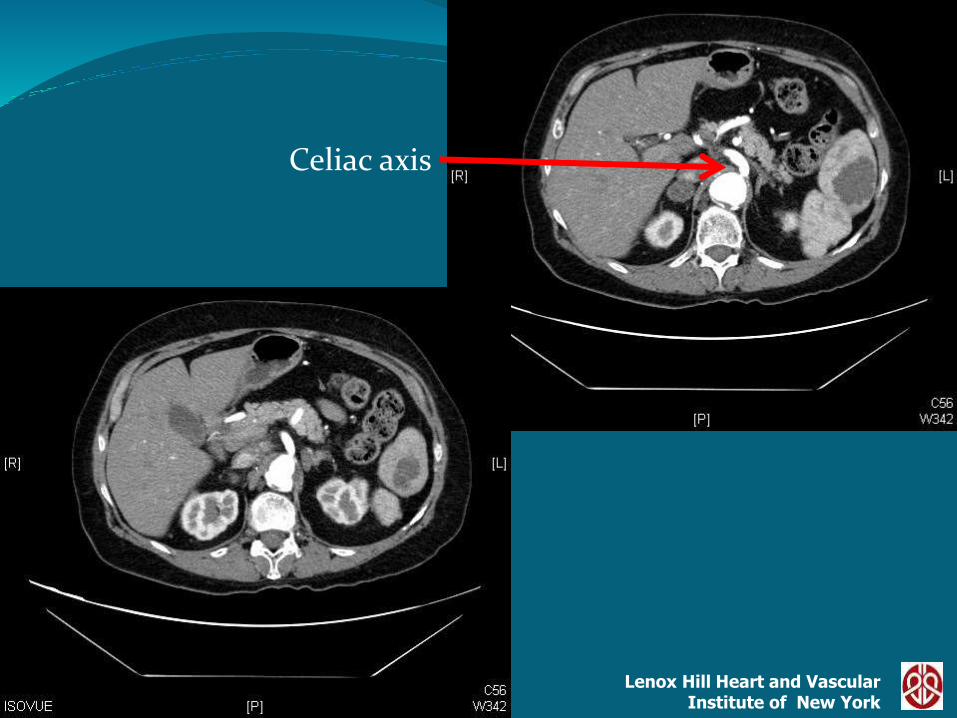
Case Presentation
67 yr old patient
Type IV TAAA
Previous Descending TA repair
Symptomatic

Lenox Hill Heart and VascularInstitute of New York
Celiac axis

Lenox Hill Heart and VascularInstitute of New York
R Renal

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Iliac Bifurcation

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Stroke Prevention
Cannulation TechniquesLeft Axillary CannulationAscending Aorta CannulationArch cannulation
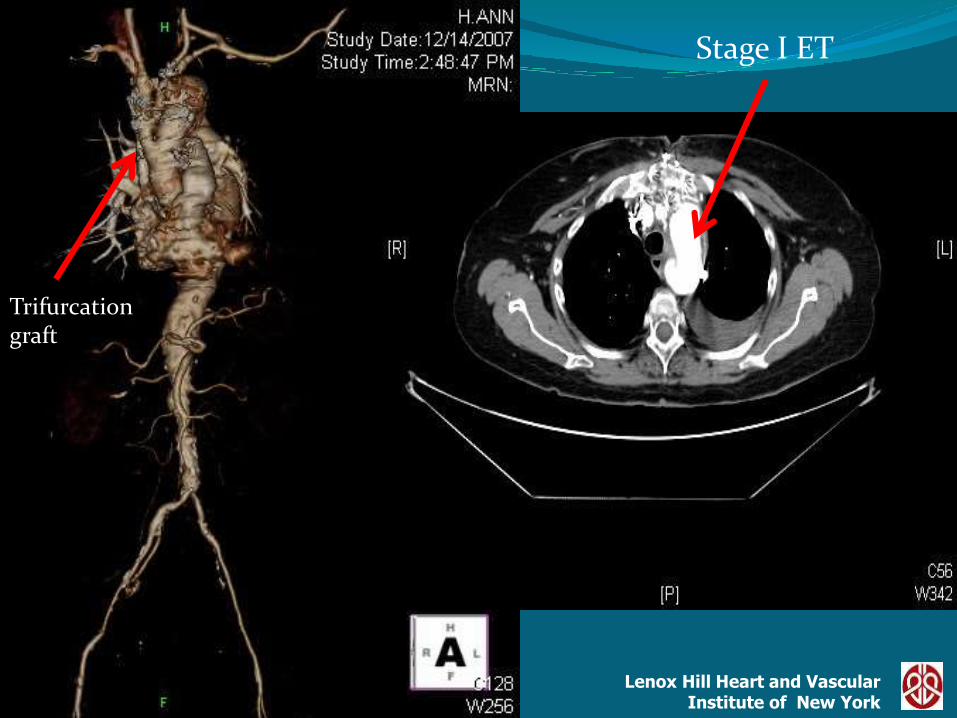
Stage I Elephant Trunk

Lenox Hill Heart and VascularInstitute of New York
62 yr old patient
Type I TAAA
Grade V aortic arch
Stenosis of the Celiac, SMA

Lenox Hill Heart and VascularInstitute of New York
Grade V Aortic Arch

Lenox Hill Heart and VascularInstitute of New York
Descending Thoracic Aorta
Lenox Hill Heart and VascularInstitute of New York
Celiac axis

Lenox Hill Heart and VascularInstitute of New York
InfrarenalAorta

Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
Stage I ET
Trifurcation graft

Lenox Hill Heart and VascularInstitute of New York
Celiac
SMA
Stage I ET
Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
January 2002 – July 2011
Total Cases 219
male 112 51%
female 107 49%
Age 66 + 13

Lenox Hill Heart and VascularInstitute of New York
Etiology: N=219
0
10
20
30
40
50
60
70
80
90
Medial
Degen.
Ather. Chr.
Diss.
Acute
Diss.
Other
38%
23%
27%
3%
9%

Lenox Hill Heart and VascularInstitute of New York
Presentation: N=219
ElectiveRuptureUrgent
66%
19%
15%

Lenox Hill Heart and VascularInstitute of New York
Aneurysm Type:N=219
0
10
20
30
40
50
60
70
80
Type I Type II Type III Type IV
36%
20%
23% 21%

Lenox Hill Heart and VascularInstitute of New York
No Distal perfusion 29 13%
Femoral-Femoral 87 40%
Atrial-Femoral 103 47%
DHCA 41 19%

Lenox Hill Heart and VascularInstitute of New York
Operative variables
Aortic X time 49 (14-173)
CPB time 87 (17-320)
DHCA time 31 (22-56)
Lenox Hill Heart and VascularInstitute of New York
Mortality 13 6%
Paraplegia 4 2%

Lenox Hill Heart and VascularInstitute of New York
Post- Op Bleeding 8 4%
Stroke 6 3%
Embolic 3
Hemorrhage 3
Operative Complications
Lenox Hill Heart and VascularInstitute of New York
New Onset Renal Complications:Cr>2.5
New onset renal insufficiency 51 24%
New Onset Hemodialysis 8 4%
Ventilation>48h 51 23%

Lenox Hill Heart and VascularInstitute of New York
Hospital Stay
Mean 12 d
Range (5-96)

Lenox Hill Heart and VascularInstitute of New York
Survival
TAAA
122 105 67 36 21 10
Lenox Hill Heart and VascularInstitute of New York
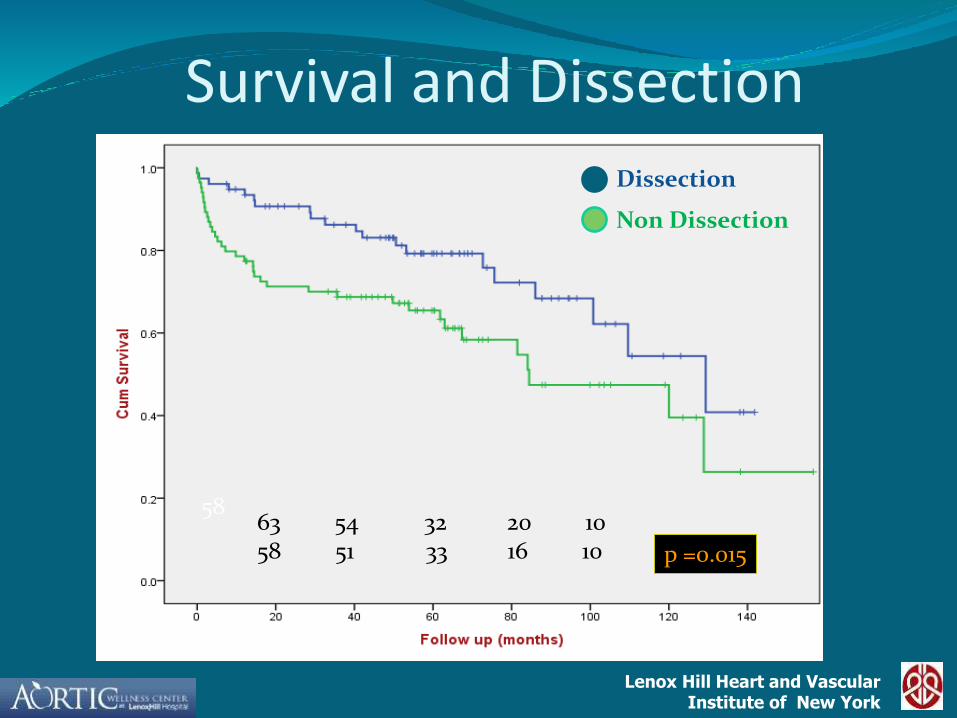
Survival and Dissection
Dissection
Non Dissection
p =0.015
5863 54 32 20 1058 51 33 16 10

Lenox Hill Heart and VascularInstitute of New York
Open – Demographics Plestis2011
N=219
Schephens199
N=258
Gambria2002
N=337
Coselli2007N=2286
Conrad-2007N=445
Age 66 65 70 66 71
Extent I + II 56% 58% 44% 64% 42%
Rupture 19% 15% 13% 6% 11%
Hybrid – Demographics Kuratani2009N=86
Choong2009N=70
Donas2009
N=58
Kabbani2010
N=36
Chiesa2009N=31
Age 71 67 64.5 71 70
Extent I + II 27% 56% 14% 31% 45%
Rupture 3% 4% 14% N/A N/A

Lenox Hill Heart and VascularInstitute of New York
Open
HybridKuratani2009N=86
Choong2009N=70
Donas2009
N=58
Kabbani2010
N=36
Chiesa2009N=31
Mortality 2.3% 16% 25% 8.3% 19.4%
SCI 1.2% 10% 3.4% 3% 8.6%
Dialysis 2.3% N/A N/A 11% 6.4%
Endoleak 10% N/A 17% 27% N/A
Plestis2011
N=219
Schephens199
N=258
Gambria2002
N=337
Coselli2007N=2286
Conrad-2007N=445
Mortality 6% 10% 8% 7% 8%
SCI 2% 11% 11% 4% 13%
Dialysis 4% 10% 13% 6% 21%

Lenox Hill Heart and VascularInstitute of New York
Follow Up Survival -Open
Kuratani2009
Kabbani2010
Chiesa2009
Bockler2008
Survival1 year3 years5 years 70%
80% 60%70%
Follow Up Survival -Endovascular
Plestis2011
Schephens2010
Conrad2007
Kouchoukos2011
Survival1 year5 years10 years
70%51%
83%63%34%
54%29%
55%%23%

Lenox Hill Heart and VascularInstitute of New York
Conclusions
Both open and hybrid operations in the thoracoabdominalaorta remain extremelly complex operations
The results of open repair of TAAA have improved significantly over the last decade in centers of excellence
The long term outcomes of hybrid operations have not been determined yet.
Open TAA repair remains the procedure of choice in appropriately selected candidates

Lenox Hill Heart and VascularInstitute of New York
Thank you

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Extent and Mortality
0
10
20
30
40
50
60
70
80
90
Type I TypeII TypeIII TypeIV Descending
Mortality
6%
0%
13%
6%
6%P>0.05
N

Lenox Hill Heart and VascularInstitute of New York
Mortality and Distal Perfusion
0
20
40
60
80
100
120
Atriofemoral Femoral Femoral None
Mortality
No Mortality"
6%
7%
10%
P>0.05

Lenox Hill Heart and VascularInstitute of New York
Mortality and Aneurysm Type
0
20
40
60
80
100
120
140
160
1 2
No
5%
6%P>0.05
TAAA DTA

Lenox Hill Heart and VascularInstitute of New York
0
20
40
60
80
100
120
140
160
180
1 2
No
Ventilation<48h Ventilation>48h
Mortality and Ventilation>48h
2.5%
13%
P<0.05

Lenox Hill Heart and VascularInstitute of New York
0
50
100
150
200
250
1 2
Mortality and HemodialysisNo
4%
19%
P<0.05
No Hemodialysis Hemodialysis

Lenox Hill Heart and VascularInstitute of New York
0
50
100
150
200
250
1 2
40%
4%
Stroke and Mortality
StrokeNo Stroke
P<0.05

Lenox Hill Heart and VascularInstitute of New York
Survival
TAAA Dissection
DTA Non Dissection
DTA Dissection
TAAA non Dissectionp =0.038

Lenox Hill Heart and VascularInstitute of New York
Survival
TAAA
DTA
44 40 29 15 9 5 79 65 50 21 11 7

Lenox Hill Heart and VascularInstitute of New York
Questions
Does endovascular surgery treat the same patients as open surgery ?
Does endovascular surgery treat the same extent of aorta?
Does endovascular surgery deliver the same long-term outcomes?

Lenox Hill Heart and VascularInstitute of New York
Hybrid Approach
Chieas et al
Lenox Hill Heart and VascularInstitute of New York
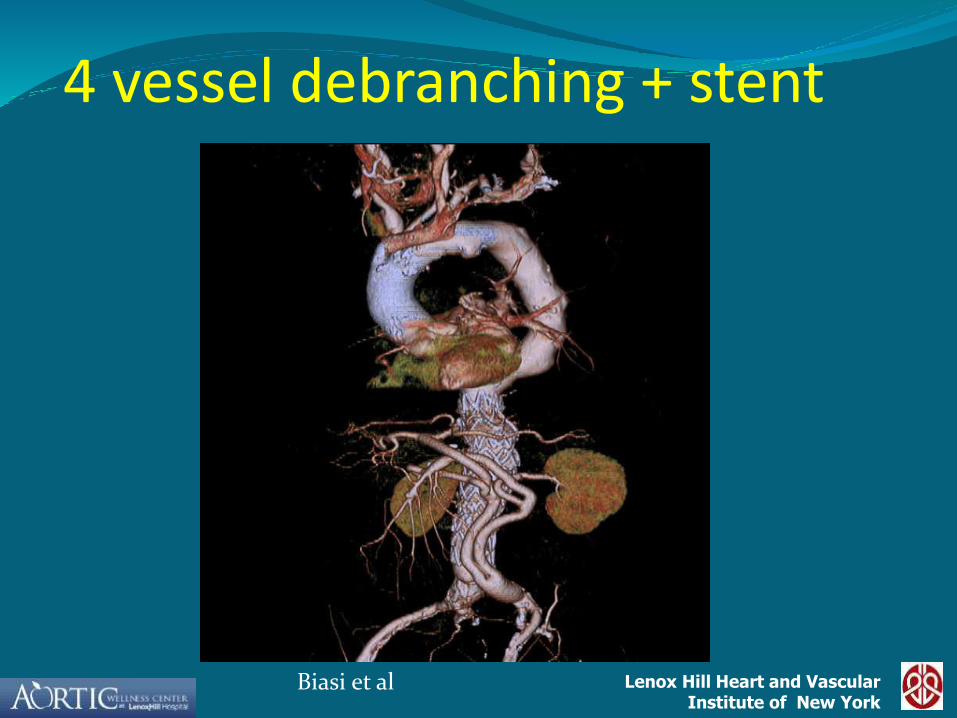
4 vessel debranching + stent
Biasi et al
Lenox Hill Heart and VascularInstitute of New York
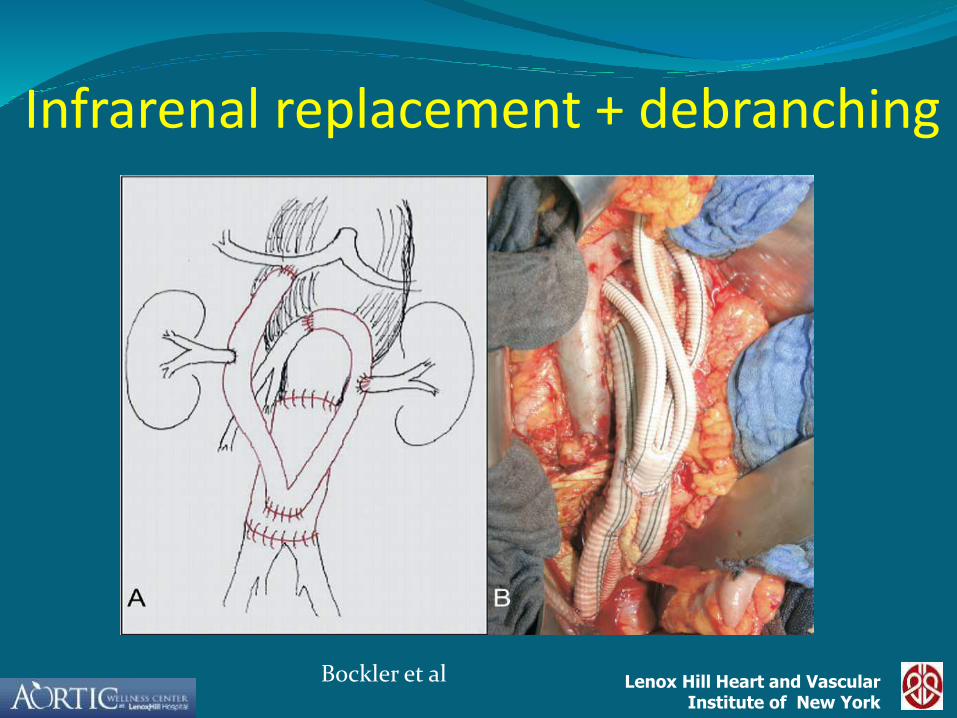
Infrarenal replacement + debranching
Bockler et al

Lenox Hill Heart and VascularInstitute of New York
MEP and SSEP guided intercostal artery reimplantation
Avoidance of subclavian artery clamping
Operative Management

Lenox Hill Heart and VascularInstitute of New York
Is it reasonable to search for a single segmental artery whose preservation will prevent paraplegia? NO
Is it reasonable to monitor spinal cord integrity in the perioperative period and treat cord ischemia when it occurs? YES
Do we yet have a strategy to assure preservation of spinal cord integrity through the perioperative period of thoracic and thoracoabdominal aortic aneurysm resection? NO
Has the neurological outcome of thoracic and thoracoabdominal aortic surgery improved markedly in the past decade? YES