Treatment of Mycoplasma Pneumonia: A Systematic Review ... · sessment tool fell within 6 domains:...
12
Treatment of Mycoplasma Pneumonia: A Systematic Review abstract BACKGROUND AND OBJECTIVE: Children with community-acquired lower respiratory tract infection (CA-LRTI) commonly receive antibiotics for Mycoplasma pneumoniae. The objective was to evaluate the effect of treating M. pneumoniae in children with CA-LRTI. METHODS: PubMed, Cochrane Central Register of Controlled Trials, and bibliography review. A search was conducted by using Medical Subject Headings terms related to CA-LRTI and M. pneumoniae and was not restricted by language. Eligible studies included randomized controlled trials (RCTs) and observational studies of children #17 years old with confirmed M. pneumoniae and a diagnosis of CA-LRTI; each must have also compared treatment regimens with and without spectrum of activity against M. pneumoniae. Data extraction and quality assessment were completed independently by multiple reviewers before arriving at a consensus. Data were pooled using a random effects model. RESULTS: Sixteen articles detailing 17 studies were included. The most commonly selected primary outcome was symptomatic improvement. Nine studies examined M. pneumoniae treatment in CA-LRTI secondary to M. pneumoniae, and 5 RCTs met criteria for meta-analysis. The suggested pooled risk difference of 0.12 (95% confidence interval, 20.04 to 0.20) favoring treatment was not significantly different and demonstrated significant heterogeneity. Limitations included substantial bias and subjective outcomes within the individual studies, difficulty interpreting testing modalities, and the inability to correct for mixed infections or timing of intervention. CONCLUSIONS: We identified insufficient evidence to support or refute treatment of M. pneumoniae in CA-LRTI. These data highlight the need for well-designed, prospective RCTs assessing the effect of treating M. pneumoniae in CA-LRTI. Pediatrics 2014;133:1081–1090 AUTHORS: Eric Biondi, MD, a Russell McCulloh, MD, b Brian Alverson, MD, c Andrew Klein, BS, a Angela Dixon, BSN, MLS, AHIP, a and Shawn Ralston, MD d a Department of Pediatrics, University of Rochester, Rochester, New York; b Department of Pediatrics, Children’ s Mercy Hospitals & Clinics, Kansas City, Missouri; c Department of Pediatrics, Hasbro Children’ s Hospital, Providence, Rhode Island; and d Department of Pediatrics, Children’ s Hospital at Dartmouth– Hitchcock, Hanover, New Hampshire KEY WORDS pediatric, pneumonia, macrolide, azithromycin, atypical pneumonia, mycoplasma ABBREVIATIONS CA-LRTI—community-acquired lower respiratory tract infection CAP—community-acquired pneumonia CI—95% confidence interval IDSA—Infectious Diseases Society of America RCT—randomized controlled trial URTI—upper respiratory tract infection Dr Biondi conceptualized and designed the review, reviewed articles, ran the meta-analysis, and drafted the original manuscript; Dr McCulloh conceptualized and designed the review, reviewed articles, helped to run the meta-analysis, and drafted the original manuscript; Dr Alverson participated in the design, helped interpret the included studies, and critically reviewed the manuscript; Mr Klein participated in study design, tabulated articles, and reviewed the manuscript; Ms Dixon participated in study design, helped perform the literature review, and critically reviewed portions of the manuscript; Dr Ralston participated in study design, supervised Drs Biondi and McCulloh in study interpretation and translated 1 study, and participated in the meta-analysis; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2013-3729 doi:10.1542/peds.2013-3729 Accepted for publication Feb 21, 2014 Address correspondence to Russell McCulloh, MD, Pediatric Infectious Diseases, Children’ s Mercy Hospitals & Clinics, 2401 Gillham Rd, Kansas City, MO 64108. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2014 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: No external funding. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no conflicts of interest to disclose. COMPANION PAPER: A companion to this article can be found on page 1124, and online at www.pediatrics.org/cgi/doi/10.1542/peds. 2014-0871. PEDIATRICS Volume 133, Number 6, June 2014 1081 REVIEW ARTICLE by guest on September 8, 2020 www.aappublications.org/news Downloaded from
Transcript of Treatment of Mycoplasma Pneumonia: A Systematic Review ... · sessment tool fell within 6 domains:...

Treatment of Mycoplasma Pneumonia: A SystematicReview
abstractBACKGROUND AND OBJECTIVE: Children with community-acquiredlower respiratory tract infection (CA-LRTI) commonly receive antibioticsfor Mycoplasma pneumoniae. The objective was to evaluate the effectof treating M. pneumoniae in children with CA-LRTI.
METHODS: PubMed, Cochrane Central Register of Controlled Trials, andbibliography review. A search was conducted by using Medical SubjectHeadings terms related to CA-LRTI and M. pneumoniae and was notrestricted by language. Eligible studies included randomized controlledtrials (RCTs) and observational studies of children#17 years old withconfirmed M. pneumoniae and a diagnosis of CA-LRTI; each must havealso compared treatment regimens with and without spectrum ofactivity against M. pneumoniae. Data extraction and quality assessmentwere completed independently by multiple reviewers before arrivingat a consensus. Data were pooled using a random effects model.
RESULTS: Sixteen articles detailing 17 studies were included. The mostcommonly selected primary outcome was symptomatic improvement.Nine studies examined M. pneumoniae treatment in CA-LRTI secondaryto M. pneumoniae, and 5 RCTs met criteria for meta-analysis. Thesuggested pooled risk difference of 0.12 (95% confidence interval,20.04 to 0.20) favoring treatment was not significantly differentand demonstrated significant heterogeneity. Limitations includedsubstantial bias and subjective outcomes within the individualstudies, difficulty interpreting testing modalities, and the inability tocorrect for mixed infections or timing of intervention.
CONCLUSIONS: We identified insufficient evidence to support or refutetreatment of M. pneumoniae in CA-LRTI. These data highlight the needfor well-designed, prospective RCTs assessing the effect of treating M.pneumoniae in CA-LRTI. Pediatrics 2014;133:1081–1090
AUTHORS: Eric Biondi, MD,a Russell McCulloh, MD,b BrianAlverson, MD,c Andrew Klein, BS,a Angela Dixon, BSN, MLS,AHIP,a and Shawn Ralston, MDd
aDepartment of Pediatrics, University of Rochester, Rochester,New York; bDepartment of Pediatrics, Children’s Mercy Hospitals& Clinics, Kansas City, Missouri; cDepartment of Pediatrics,Hasbro Children’s Hospital, Providence, Rhode Island; anddDepartment of Pediatrics, Children’s Hospital at Dartmouth–Hitchcock, Hanover, New Hampshire
KEY WORDSpediatric, pneumonia, macrolide, azithromycin, atypicalpneumonia, mycoplasma
ABBREVIATIONSCA-LRTI—community-acquired lower respiratory tract infectionCAP—community-acquired pneumoniaCI—95% confidence intervalIDSA—Infectious Diseases Society of AmericaRCT—randomized controlled trialURTI—upper respiratory tract infection
Dr Biondi conceptualized and designed the review, reviewedarticles, ran the meta-analysis, and drafted the originalmanuscript; Dr McCulloh conceptualized and designed thereview, reviewed articles, helped to run the meta-analysis, anddrafted the original manuscript; Dr Alverson participated in thedesign, helped interpret the included studies, and criticallyreviewed the manuscript; Mr Klein participated in study design,tabulated articles, and reviewed the manuscript; Ms Dixonparticipated in study design, helped perform the literaturereview, and critically reviewed portions of the manuscript;Dr Ralston participated in study design, supervised Drs Biondiand McCulloh in study interpretation and translated 1 study, andparticipated in the meta-analysis; and all authors approved thefinal manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-3729
doi:10.1542/peds.2013-3729
Accepted for publication Feb 21, 2014
Address correspondence to Russell McCulloh, MD, PediatricInfectious Diseases, Children’s Mercy Hospitals & Clinics, 2401Gillham Rd, Kansas City, MO 64108. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found onpage 1124, and online at www.pediatrics.org/cgi/doi/10.1542/peds.2014-0871.
PEDIATRICS Volume 133, Number 6, June 2014 1081
REVIEW ARTICLE
by guest on September 8, 2020www.aappublications.org/newsDownloaded from

Community-acquired pneumonia (CAP)accounts for .150 000 pediatric hos-pitalizations each year in the UnitedStates, and there are great disparitiesin patterns of care and outcomes.1
Specifically, wide variations in antibi-otic prescribing practices exist amongphysicians, often because the causa-tive agent is not identified.2 For thisreason, recent evidence-based pediat-ric CAP practice guidelines publishedby the Infectious Diseases Society ofAmerica (IDSA) recommend that chil-dren hospitalized with CAP be testedfor Mycoplasma pneumoniae.3 M.pneumoniae is a common cause of CAPand other community-acquired lowerrespiratory tract infections (CA-LRTIs),particularly in school-age children andadolescents, but there are large gapsin our understanding of this disease.3,4
Prevalence estimates vary from 10% to40% in pediatric CA-LRTI,5–9 and fewstudies address treatment recommenda-tions.4,10 Additionally, the IDSA guidelinestarget the use of macrolides in CA-LRTI asan area needing additional research.3
First-line treatment of children hospi-talized with CAP currently includes ab-lactam to treat common causativebacterial agents such as Streptococ-cus pneumoniae and a macrolide toprovide additionally treatment of atypi-cal pathogens such asM. pneumoniae.3
Studies of antibiotic use in the pre–IDSA guidelines era showed markedvariability in prescription practices,2
probably because the efficacyof macrolides in the treatment ofM. pneumoniae remains unclear andtreatment recommendations, even inmajor textbooks, are variable.4,10 Theavailable evidence is also conflicting.One small trial suggests that b-lactamuse in children with CAP is more cost-effective than macrolides,11 severalrandomized controlled trials (RCTs)suggest no difference in efficacy,12,13
and 2 recent pediatric cohort studiessuggest that b-lactam–macrolide com-
bination therapy decreased length ofstay by 20% to 30% over b-lactammonotherapy.2,4 Data on antibiotic treat-ment of pediatric CA-LRTI caused byM. pneumoniae are generally consid-ered inconclusive,3,4,10,14 yet macro-lides remain the most commonlyoverprescribed antibiotic at pediatricclinics in the United States:.6 millionannual doses for respiratory symp-toms without a clear indication.15
A Cochrane review on the use of anti-biotics to treat CA-LRTI secondary to M.pneumoniae in children found in-sufficient evidence to draw any specificconclusions about the efficacy of anti-biotics for the condition.10 However,this review omitted at least 3 RCTs(roughly one-third of the total RCTs) forwhich there appeared to be applicabledata on the topic,12,16,17 and data fromobservational studies were omitted.The objective of our study was to pro-vide a more comprehensive review ofall available published literature on theuse of antibiotics in children to treatCA-LRTI secondary to M. pneumoniae.
METHODS
Search Design
This was a systematic review of allobservational and randomized trialscomparing antibioticswith spectrumofactivity for M. pneumoniae (eg, mac-rolide, tetracycline, or quinolone class)with placebo or antibiotics from anyother class without spectrum of activ-ity against M. pneumoniae in children
,18 years of age with CA-LRTI. The re-view was conducted in concordancewith the Preferred Reporting Items forSystematic Reviews and Meta-Analysesstatement.
Outcome Types
The primary outcome was clinical im-provement or cure at follow-up. Clinicalimprovement or cure could include reso-lution of fever; resolution or improvementin symptoms such as cough, congestion,shortness of breath, fatigue, or chest pain;or improvement or cure as defined by theauthors of the individual studies.
Literature Search
With the assistance of a librarian (A.D.),we performed a comprehensive searchof PubMed (January 1966–August 2012)with the Medical Subject Headingsterms and keywords (Table 1). Afterduplicates were removed, we used in-clusion and exclusion criteria to selectstudies based on their title and ab-stract to include in our review. Addi-tional studies were identified throughmanual search of the bibliographies ofqualifying studies. Before manuscriptsubmission, a second search was per-formed (August 2012–September 2013)to ensure that the review was as up-to-date as possible and any new studieswere included in the analysis.
Study Selection
Studies were considered eligible forinclusion in the review if they met the
TABLE 1 Medical Subject Headings Used for Primary Literature Search
Mycoplasma pneumoniae pediatrica antibiotica
pneumonia, mycoplasma infant anti-bacterial agentsrespiratory tract infections child macrolidea
pneumonia child, preschool roxithromycinrecurrent respiratory tract infectiona adolescent erythromycinrespiratory infectiona telithromycinRRTI macrolidescommunity-acquired infections azithromycinlower respiratory tract infectiona clarithromycinlower respiratory infectiona
a Represents open-ended term.
1082 BIONDI et al by guest on September 8, 2020www.aappublications.org/newsDownloaded from

following criteria: randomized or ob-servational studies, included children#17 years of age, included $10 chil-dren who were diagnosed with CA-LRTIsecondary to laboratory-confirmed M.pneumoniae, data were provided for atleast 1 outcome measuring improve-ment, and the study compared anyantibiotic with spectrum of activityagainst M. pneumoniae with eitherplacebo or another antibiotic withoutactivity against M. pneumoniae. Stud-ies that examined children withchronic respiratory illnesses such ascystic fibrosis, bronchiectasis, bron-chopulmonary dysplasia, congenitalheart disease, or immunodeficiencywere excluded, as were those that ex-amined children with nosocomial andcongenital infections.
Studies were considered eligible formeta-analysis if, in addition to meetingcriteria for inclusion in the qualitativereview, information was either pro-vided or could be extrapolated re-garding the total numberandoutcomesof patients with M. pneumoniae withineach treatment group. A subgroupanalysis of the initial meta-analysiswas performed that included only theRCTs.
Identification of Trials and DataExtraction
The principal investigators (E.B. andR.M.) independently screened each ci-tation identified through the initialsearch strategy as definitely, possibly,or clearly not meeting inclusion crite-ria. Full-text articles of all studies def-initely or possibly meeting inclusioncriteria were obtained regardless ofprimary language of the publication.Reviewers (E.B. andR.M.) independentlyreviewed each full-text article and thenreached consensus before data ab-straction. For full-text articles meetingstudy criteria, reviewers (E.B. and R.M.)extracted data for each study in-dependently and then discussed their
findings to form a consensus. Dis-crepancies were resolved throughdiscussion with the collaboratingreviewers (B.A. and S.R.). When neces-sary, the principal reviewers attemptedto contact study authors to verifymethods and extracted data, althoughno responses were received.
Validity and Quality Assessment
Studies were assessed and graded forlevel of evidence based on criteriapublished by the Oxford Center forEvidence-Based Medicine.18 An 18-itemstudy quality assessment tool (Sup-plemental Information) was developedbased on recommendations publishedby the Agency for Healthcare Researchand Quality.19 Items on the quality as-sessment tool fell within 6 domains:subject selection, study performancebias, detection bias, subject attrition,reporting bias, and financial conflict ofinterest. Items were marked as factorpresent, not present, or unclear basedon review of the manuscript. Eachstudy was given a total quality score,and for this purpose, labels of “notpresent” or “unclear” were groupedtogether. Studies were considered tobe unblinded when it was not specifi-cally stated that participants or inves-tigators were blinded. Three reviewers(E.B., R.M., and B.A.) performed in-dividual assessments on all includedstudies independently and then dis-cussed each until all 3 reviewers werein agreement.
Statistical Analyses
Because much of the information rel-evant to this review was extrapolatedfrom data presented in the includedstudies, the review authors attemptedto calculate statistical significancewherever possible using x2 or Fisher’sexact tests. In cases for which M.pneumoniae and Chlamydia pneumo-niae were grouped together, a “worst-case scenario” was performed by the
review authors that assumed all C.pneumoniae were in the “improved ontreatment” group.20 These were thensubtracted from the total. This allowedan interpretation of the results thatwould ensure that, if a treatment effectwas identified, it was not secondary toC. pneumoniae. For comparison, theanalysis was also performed assumingthat C. pneumoniae andM. pneumoniaeresponded equally to treatment. Treat-ment effects for dichotomous outcomeswere calculated as risk difference usingrandom effects modeling. Study het-erogeneity was assumed for a P ,.10and I2 $25%. If the primary outcome(clinical improvement) was assessedin separatemethods and separate timeperiods, each set of outcomes was in-cluded in the review andmeta-analysis.Meta-analysis was performed by usingComprehensive Meta-Analysis Version2 (Biostat, Englewood, NJ).
RESULTS
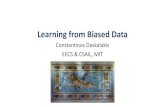
The initial database search identified4667 articles. One other citation wasidentified via bibliography review.4
Most articles were excluded based ona preliminary screen of the abstracts,leaving 40 full-text articles to beassessed for eligibility. Before sub-mission, a second search was per-formed (August 2012–September 2013)to ensure that no recent articles weremissed in the review. This searchrevealed 275 new articles, 1 of whichwas assessed for full-text eligibilitybut did not meet study criteria.2 Of the4943 total citations reviewed, 16 metcriteria for inclusion in the qualitativesynthesis.5,12,13,16,17,20–30 One RCT20 useddifferent outcome metrics at 2 differ-ent times and, for the purposes of thisreview, was considered 2 separateRCTs. Therefore, 17 studieswere included.Four citations were non-English and weretranslated by the review authors (2 inSpanish,23,30 1 in French,21 and 1 inGerman29). Eight studies provided
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 1083 by guest on September 8, 2020www.aappublications.org/newsDownloaded from

data20,22,27,28 orenabled the reviewauthors(E.B. and R.M.) to extract data13,16,23
specifically comparing treatment withno treatment of M. pneumoniae in chil-dren diagnosed with M. pneumoniaeand were included in the quantitativeanalysis; 5 were RCTs (Fig 1).13,16,20,23
Therewere4294patientsenrolled in the17 included studies (Table 2). Of these,an aggregate 2648 patients could beused to compare an agent treating M.pneumoniae with an agent that did nottreat M. pneumoniae in CA-LRTI. Thisnumber excludes comparator arms inwhich antibiotics of the same class orspectrum were compared and patientsin whom therapy could not be de-termined. One randomized trial pro-vided data on a total of 155 patients butcompared macrolide therapy with ei-ther a b-lactam or another macrolideand did not provide separate statis-tics.30
Ten RCTs12,13,17,20,23,24,26,29,30 and 3 co-hort studies5,22,25 compared a mac-rolide with a nonmacrolide in thetreatment of CA-LRTI. One RCT16 com-pared levofloxacin with a b-lactam, 1retrospective cohort study21 compared
M. pneumoniae spectrum with non–M.pneumoniae spectrum antibiotics, and2 case–control studies27,28 comparedmacrolide treatment in patients withmacrolide-sensitive and macrolide-resistant M. pneumoniae. Espositoet al20 included upper respiratoryinfections (URTIs) (199/352, 57%) inaddition to CA-LRTI (153/352, 43%) butdid not provide a separate analysis,and therefore all are included in thisreview, as was done previously.10 Onestudy did not report the total numberof pediatric patients.17 Studies usedvarious combinations of methods forM. pneumoniae detection; 5 used cultureof nasopharyngeal specimens,17,23,24,27,28
15 used serology,5,12,13,16,17,20–26,28–30
and 6 used polymerase chain reac-tion assays of upper airway speci-mens.12,20,23,25,26,28 No trials wereplacebo controlled, and a number ofstudies received pharmaceutical com-pany funding.12,13,16,20,24,25
When we evaluated for overall qualityamong all studies included, detectionbias, which included items such asvalidity and reliability of study out-comes, was the most frequently iden-
tifiedbiascategory (12/17studies, 71%)(Table 3). The most common cause ofstudy performance bias was unblindedparticipants or observers. More thanhalf of the RCTs (6/11, 55%) reporteda potential conflict of interest, which inall cases was pharmaceutical spon-sorship with use of that company’sdrug in the study.
Spectrum-Specific Treatment inPediatric CA-LRTI Secondary toM. pneumoniae
Nine studies5,13,16,20,22,23,27,28 providedenough detail to allow a comparison ofM. pneumoniae spectrum and non-spectrum treatment in pediatricpatients with CA-LRTI secondary to M.pneumoniae and included a total of 723such patients (Table 4). In terms ofoverall clinical improvement, 4 of 5RCTs found no clinical benefit.13,16,20,23
One retrospective cohort study identi-fied a significant improvement in du-ration of fever in patients treated withmacrolides, although clinically therewas a large overlap in fever durationrange (3.0–6.8 vs 3.4–7.9 days; P = .04),and there was not a significant
FIGURE 1Flowchart for included studies. a One article20 used 2 different outcome metrics at 2 different time periods and was therefore treated as 2 separate studies.
1084 BIONDI et al by guest on September 8, 2020www.aappublications.org/newsDownloaded from

TABLE2
StudyCharacteristicsandQuality,inChronologicalOrder
Study
Design/Length
Patients
Intervention/Comparator
Relevant
Outcom
esRelevant
Results
Levelof
Evidence
Sterneretal(1967)
RCT/1.5y
N=180(unknown
ages)with
CAP
EES/cephaloridine
Failure
=daily
fevers
for5dor
fever$10
d8/87
(EES)vs
17/93(cephaloridine)failures.aMean
fever=2.7vs
3.8d.Inthosewith
MP,0/13
vs3/9
failures.aDoes
notseparateadultsandchildren.
2b
Ruhrmannetal(1982)
RCT/1y
N=120(6
mo–14
yr)
with
CAP
EES/am
oxicillin
Feverduration
Meanfever=2.66
4.1d(EES)vs
2.46
1.9d
(amoxicillin).
2b
Garo
etal(1988)
Retro,multisite
cohort/5
yN=182(m
eanage=
29y)with
MP
MPspectrum
/nospectrum
Feverduration
Meanfever=3d(spectrum)vs
7d(nospectrum
).84%presentedwith
atypicalpneumonia.Does
notseparateadultsandchildren.
4
Gomez
Campdera
etal(1996)
RCT/2y
N=155(6
mo–16
y)with
CAP
AZM/co-am
oxiclav
(,5y);EES
(.5y)
Curedor
improved
at3,10,or30
dAt3,10,and
30d,respectively:78/82(AZM
)vs
66/73
(com
parator),a80/82vs
68/73,aand80/82vs
69/73.aNo
differenceindurationoffeveror
cough.15
totalw
ithMP.
2b
Gendreletal(1997)
Pro,cohort/2
yN=104(1.5–13
y)with
CAP
Macrolide/b-lactam
Feverat2–18
dInchildrenwith
MP:11/11(m
acrolide)
vs2/32
(b-lactam
)becameafebrile(P
,.001).a
4
Harrisetal(1998)
Multisite,RCT/1.5y
N=456(6
mo–16
y)with
CAP
AZM/co-am
oxiclav
(,5yr);EES($
5yr)
1.Curedor
improved
at15–19
dIn,5ygroup:clinicalsuccessin114/125(AZM)
vs59/63(co-am
oxiclav)at
15–19
d,aand97/114
vs41/48at4–6wk.135/310
vs45/146
hadadverse
events(P
,.001).a
1b
2.Curedor
improved
at4–6wk
3.Adverseevents
Sáez-Llorens
etal(1998)
Multisite,RCT/2
yN=335(6
mo–15
y)with
CAP
AZM/co-am
oxiclav
(,5yr);EES($
5yr)
Curedor
improved
after
3doftreatm
ent
96/97(AZM
)vs
114/116(co-am
oxiclav)curedor
improved.IncasesofMP,9/9and5/5curedor
improved.a
2b
Wubbeletal(1999)
RCT/2y
N=174(6
mo–16
y)with
CAP
AZM/co-am
oxiclav
(,5yr);EES($
5yr)
1.Cured3daftertreatm
ent
68/69(AZM
)vs
75/78(com
parator)cured.10/69
(AZM
)vs
33/49(co-am
oxiclav)hadadverse
events(P
,.001).a
2b2.Adverseevents
Ferw
erda
etal(2001)
Multisite,RCT/3
yN=118(3
mo–12
y)with
CAP
AZM/co-am
oxiclav
1.Curedor
improved
at10–13
dSuccessin50/55(AZM
)vs
46/53(co-am
oxiclav)
at10–13
dand46/51vs
43/50at
25–30
d.33/59vs
41/58adverseevents.a
1b2.Curedor
improved
at25–30
d3.Adverseevents
Principietal(2001)
Pro,multisite
cohort/1
yN=613(2–14
y)with
CAP
Macrolide/no
spectrum
Curedor
improved
at4–6wk
Insubjectswith
MPor
CP,success
in106/109
(macrolide)
vs67/82(com
parator)(P
,.001).a
2b
Koganetal(2003)
RCT/3y
N=110(30d–14
y)with
CAP
ClassicCAP:AZM/amoxicillin
Clinicalresponse:
Meanfever=1.7d(AZM
)vs
2.0d(amoxicillin).
Byday14
all47CXRs
hadimproved
by.75%.
2bFeverduration
CXR.75%improved
Esposito
etal
(2005),study
ARCT/2y
N=352(1–14
y)with
recurrentRTI
AZMandsymptom
atic/
symptom
atic
Clinicalsuccessat
4–6wk
76/76(AZM
)vs
88/114
(com
parator)with
MP
orCP
hadclinicalsuccess(P
,.001).
2b
Esposito
etal(2005),
studyB
RCT/2y
N=352(1–14
y)with
recurrentRTI
AZMandsymptom
atic/
symptom
atic
#2RTIsat6mo
53/71(AZM)vs
61/109
(com
parator)with
MP
orCP
#2RTIs(P
=.01).a
2b
Bradleyetal(2007)
Multisite,RCT/2
yN=738(6
mo–16
y)with
CAP
Levofloxacin/b-lactam
(,5yr);macrolide($
5yr)
Improved
orcuredat
1–3dandcuredat10–17
dSuccesswas
409/441(levofloxacin)vs
138/147
(com
parator)at1–3dand439/503vs
145/170at10–17
d.
2b
Luetal(2008)
Retro,cohort/2
yN=139(8
mo–12
y)with
MPCA-RTI
Macrolide/no
macrolide
Durationoffever
Meanfever=4.90
61.89
d(m
acrolide)
vs5.63
62.22
d(nomacrolide)
(P=.04).
2b
Matsubara
etal(2009)
Retro,case–
control/4y
N=94
(0–14
y)with
MP
CAPtreatedwith
macrolide
Macrolidesensitive
MP/
resistantM
P1.Excellent
orgood
clinicalresponse
43/47(sensitive)
vs5/22
(resistant)hadpositive
clinicalresponse
(P,
.01).M
eanfever=1.5
vs4.0d(P
,.01)
andmeancough=1.5
vs4.0d(P
,.01).
3b
2.Meanfeverduration
3.Coughduration
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 1085 by guest on September 8, 2020www.aappublications.org/newsDownloaded from

difference in other signs or symptoms,white blood cell count, or C-reactiveprotein levels.5 One retrospectivecase–control study found an overallclinical benefit and 2 other studiesidentified a decrease in fever duration,although these were rated as beingamong the lowest quality of evidence inthis review.22,27,28 Esposito et al2o (studyA) was the only RCT to identify a clinicalbenefit, but the patient population in-cluded children with URTI. Additionally,the data were categorized only as“atypical” bacteria and did not sepa-rate C. pneumoniae fromM. pneumoniae.Twenty-seven patients had acute C. pneu-moniae infection only, and the “worst-case scenario” excludes all patients withC. pneumoniae after assuming each im-proved on macrolide therapy.
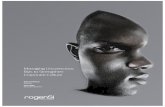
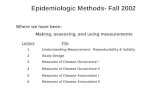
Two meta-analyses were attemptedusing risk difference as the treatmenteffect. The first included all studieslisted in Table 4 that used dichotomousvariables.13,16,20,22,23,27,28 However, therewas a large degree of heterogeneity(P, .001) in addition to publication biasand largely variable treatment effects.A second analysis used only theRCTs13,16,20,23 and demonstrated a pooledrisk difference of 0.12 (95% confidenceinterval [CI], 20.04 to 0.20) (Fig 2). Thisrisk difference represents the absolutechange in risk attributable to treat-ment with a macrolide. In our case, therisk in the treated groupminus the riskin the control group was 12% (95% CI,24% to 20%). This finding suggeststhat 12% of children treated witha macrolide will have more rapid clin-ical improvement, corresponding toa number needed to treat of 8.33, butthe confidence interval overlapping 0%negates statistical significance. Thereremained significant heterogeneitybetween the studies (P = .02). Thefunnel plot revealed potential forpublication bias against small studiesthat show a treatment effect (Fig 3). Toprovide comparison with the “worst-case
scenario,” the same meta-analysis, as-suming C. pneumoniae and M. pneu-moniae responded equally to treatment,demonstrated a pooled risk differenceof 0.12 (95% CI, 0.01 to 0.22).
DISCUSSION
The majority of studies included in oursystematic review did not show a sig-nificant clinical benefit of M. pneumo-niae spectrum therapy in CA-LRTI. Ofthe 9 studies that specifically examinedthe issue of M. pneumoniae treatmentin children with CA-LRTI secondary toM. pneumoniae, almost all the pro-spective studies showed no clinicalbenefit. The remaining studies gener-ally suggest a statistical, but not nec-essarily clinically relevant, decrease infever duration, and most of these arerated as low- or lowest-quality evi-dence. Our meta-analysis of RCTs sug-gests a small treatment benefit inpatients with CA-LRTI secondary to M.pneumoniae. However, the pooled ef-fect favoring treatment was drivenprimarily by the result of a single RCTthat included children with URTIs (57%of enrolled patients). Four of the 5studies included in the meta-analysisdid not show a benefit of M. pneumo-niae spectrum therapy, and the sum-mary statistic is not statisticallysignificant. The associated funnel plotdemonstrates a paucity of small stud-ies showing a treatment effect, sug-gesting either publication bias againstsuch studies, poor methodological de-sign, or artifact heterogeneity amongsmaller studies.
The question of M. pneumoniae spec-trum (specifically macrolide) use inCAP, or other CA-LRTIs, is commonlyencountered in pediatric practice. Twolarge, retrospective cohort studiesbased on administrative data sets haveindirectly addressed the issue of M.pneumoniae treatment by comparingdifferences in length of hospital stayamong children receiving b-lactamTA
BLE2
Continued
Study
Design/Length
Patients
Intervention/Comparator
Relevant
Outcom
esRelevant
Results
Levelof
Evidence
Kawaietal(2012)
Retro,case–
control/5y
N=29
(1–15
y)with
MP
CAPtreatedwith
macrolide
Macrolidesensitive
MP/resistantM
P1.Afebrile2dafter
startingtherapy
8/8(sensitive)
vs6/21
(resistant)became
afebrile(P
,.001).a
MeanDN
Aload
decreasedsignificantly.
3b
2.MPDN
Aload
at2d
Differences
notsignificantor
notcalculableunless
otherw
isestated.AZM
,azithromycin;CP,Chlamydiapneumoniae;CXR,chestx-ray;EES,erythromycinethylsuccinate;M
P,Mycoplasm
apneumoniae;pro,prospective;retro,retrospective;RTI,respiratory
tractinfection.
aSignificancecalculated
bythereview
authors.
1086 BIONDI et al by guest on September 8, 2020www.aappublications.org/newsDownloaded from

monotherapy and children receivingcombination therapy with a macro-lide.2,31 These studies found a shorter
length of stay among children receivingcombination therapy. However, testingforM. pneumoniaewas not recorded in
either database and therefore couldnot be assessed. Macrolides are amongthe most frequently prescribed classesof antibiotics for respiratory tractinfections in children, particularly inconditions for which antibiotics are notclearly indicated.15 Additionally, na-tional guidelines intended to reducepractice variability in the managementof CAP in children recommend consid-eration of macrolide use but state thatthis is based on limited data.3 Our re-view found insufficient evidence tosupport or refute antibiotic use in CA-LRTI secondary to M. pneumoniae. Thissuggests that macrolide use in CA-LRTIcould represent an area of opportunityfor reducing antibiotic use, which couldhave a significant impact on health carecosts and the development of antimi-crobial resistance.32,33
Our review provides novel informationin comparisonwith the previous reviewon the topic by including more enrolledpatients (4294 vs 1912) and morestudies (17 vs 7).10 Although the pre-vious review reports insufficient datato draw conclusions, we suggest thatthe available literature does not cur-rently support treatment of CA-LRTIsecondary to M. pneumoniae. We ex-amined observational studies, many ofwhich were assessed as having thesame level of evidence as the RCTs. Inthe absence of high-quality RCTs,experts suggest it is reasonable to in-clude cohort and case–control studiesin a systematic review, particularlywhen the quality of evidence is equiv-alent.34 Additionally, we identified 3randomized trials that had not beenpreviously examined, 1 of which wasassessed as having the highest level ofevidence of any included study.12,16,17
Although our review failed to identifyclear therapeutic efficacyofmacrolidesinpediatric CA-LRTI due toM.pneumoniae,there are data in support of antibi-otic treatment. Military studies fromthe 1960s, performed on recruits in
TABLE 3 Bias Assessment for Individual Studies
Study Selection Performance Detection Attrition Reporting Conflictof Interest
Overall
Sterner et al (1967) x — — — — — 4/15Ruhrmann
et al (1982)— — x — — — 5/15
Garo et al (1988) x x x — x — 8/14Gomez Campdera
et al (1996)x x x x — — 7/17
Gendrel et al (1997) x x x — x — 8/14Sáez-Llorens
et al (1998)x — x x — — 6/15
Harris et al (1998) — — — x — x 4/15Wubbel et al (1999) x x x x x x 10/15Ferwerda
et al (2001)— — — — — x 3/15
Principi et al (2001) — — x x x x 7/14Kogan et al (2003) x x x x — — 8/15Esposito et al
(2005), study A— x x — — x 6/15
Esposito et al(2005), study B
x x x x — x 8/15
Bradley et al (2007) — x x — — x 5/15Lu et al (2008) — — — — — — 2/14Matsubara
et al (2009)— — — x — — 2/15
Kawai et al (2012) — x x — x — 6/15
—, substantial bias not identified within the domain; x, substantial bias identified within the domain.
TABLE 4 Studies Comparing Spectrum With Nonspectrum Treatment of Children With AcuteRespiratory Infection With M. Pneumoniae Grouped by Outcome Terma
Clinical Improvement at #5 d
Study Time Frame Outcome Treatment (n) Comparator (n) Pb
Improved Total Improved Total
Sáez-Llorens et al (1998) 3 d Overall 9 9 5 5 ..99Matsubara et al (2009) ,5 d Fever 43 47 5 22 ,.001Kawai et al (2012) 2 d Fever 8 8 6 21 ,.001
Study Time Frame Days of Feverc Days of Feverc
Lu et al (2008) N/A Fever 4.9 6 1.89 5.63 6 2.22 .04
Clinical Improvement at .5 d
Study Time Frame Outcome Treatment (n) Comparator (n) Pb
Improved Total Improved Total
Gendrel et al (1997) 2–18 d Fever 9 9 2 32 ,.001Harris et al (1998) 15–19 d Overall 21 21 9 9 ..99Esposito et al (2005),
study Ad1 m Overall 49 49 88 114 ,.001
Esposito et al (2005),study Bd
6 m Recurrent 26 45 61 109 .86
Bradley et al (2007) 10–17 d Clinical 59 66 15 18 .44a Numbers often extrapolated by the review authors.b Includes P values calculated by the review authors.c Results are mean 6 SD.d Worst-case scenario with all 27 C. pneumoniae patients placed in the treatment improved group and then excluded.
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 1087 by guest on September 8, 2020www.aappublications.org/newsDownloaded from

basic training, found that recruitswith atypical pneumonia more oftenhad serologic evidence ofM. pneumoniaeinfection (identified as Eaton’s agentat the time) than asymptomatic con-trols.35,36 Additionally, in a random-ized, double-blind, placebo-controlledstudy among 300 recruits with atypi-cal pneumonia due toM. pneumoniae,treatment with a tetracycline was foundto decrease the duration of a number ofclinical signs and symptoms faster thanplacebo.37 These seminal studies do not
necessarily represent the typical clini-cal situation encountered by pedia-tricians today, given their young adult,homogenous population, nor can theyaccount for mixed infections or mod-ernized diagnostic testing. Nonetheless,these studies describe principles ofstudy design and conduct in this areathat can serve as a template for pedi-atric investigations.
One of the strengths of meta-analysis isin the process of evaluating the avail-able literature for heterogeneity. It is
often difficult to find a middle groundbetween throwing out all summaryestimates and inappropriately com-bining studies, particularly in pediat-rics, where the paucity of high-qualityRCTs is acute. We provided a summarystatistic for 1 broad study question, butwe noted significant study heteroge-neity that we could not resolve withsubgroup analysis. Therefore, our in-terpretation of the entirety of the sta-tistical testing associated with ourmeta-analysis is that despite multiple
FIGURE 2Meta-analysis of randomized trials comparing spectrum and nonspectrum treatment ofM. pneumoniae in children. Studieswereweighted by size and degreeof heterogeneity. The overall effect (diamond) represents the pooled risk differences of the 5 studies. The confidence interval crosses 0.00, suggesting a lackof statistical significance.
FIGURE 3Funnel plot of standard errors by risk difference for all studies in the second meta-analysis. Publication bias is evident against small studies that showa treatment effect.
1088 BIONDI et al by guest on September 8, 2020www.aappublications.org/newsDownloaded from

studies, a clear treatment effect has notemerged. Furthermore, the study het-erogeneity lends credence to the ideathat a large RCT is necessary to provideguidance to pediatricians on this clin-ical question.
There are several limitations to ourreview,most related to the quality of theavailable data on the topic. First, moststudies contained substantial bias orfinancial conflict of interest. We at-tempted to account for this through in-depth quality assessment and reportingto allow a critical interpretation ofstudy results. In particular, detectionbias was commonly identified in thestudies comparing spectrum withnonspectrum therapy in patients di-agnosed withM. pneumoniae. This biasmost often represented lack of blindingof investigators or participants or lackof a reliable outcome measure (ie, clini-cal improvement). This quality issuecould potentially skew study results to-ward or away from the null hypothesis.
Second, we were unable to extract dataon outcomes for all studies, reducingthe number of articles that could beincluded in the meta-analysis and po-tentially causing publication bias. This
limitation should be balanced againstthe fact that we abstracted quantitativedata from more studies than previousmeta-analyses on this subject.
Third, our assessment of treatmenteffect was limited primarily to sub-jective outcome measures such assymptomatic improvement or resolu-tion. This limitation is inevitable giventhe primary endpoints used in the in-cluded studies, but our bias assess-ment specifically addresses thesubjective nature of the data.
Fourth, M. pneumoniae testing modal-ities have changed dramatically overtime, with variable testing character-istics and lack of overall consistency.This limits the uniformity of the patientpopulation included in our review. Fur-thermore, coinfectionwith a pathogen inaddition to M. pneumoniae is commonbut rarely identified via clinical testing,making it difficult to draw specific con-clusions about therapeutic effects.9,38
Finally, no study included inouranalysistook into account the duration of illnessbefore the start of antibiotic therapy. Itis possible that the timing of in-tervention relative to the start ofsymptoms is related to the outcome.
CONCLUSIONS
Our systematic review provides in-sufficient evidence to support con-clusions about the efficacy ofmacrolidetreatment of CA-LRTI due to M. pneu-moniae in children. Fever duration maybe decreased, but the clinical impact ofthis effect is unclear, and we identifiedfew high-quality studies to support it.Our review represents the most com-prehensive evaluation of treating M.pneumoniae in children with CA-LRTI todate. The findings from this reviewhighlight the need for high-quality,prospective studies to assess the im-pact of antibiotic therapy to treat CA-LRTI causedbyM.pneumoniae in children.These studies should specifically ad-dress the potential for confoundingmixed infections, timing of interventionrelative to symptom onset, and testingmodalities that include a combinationof serology and polymerase chain re-action assays.
ACKNOWLEDGMENTSThe authors thank Dr Swati Murthy forher help with data collection and Dr JillHalterman for her review of the finalmanuscript.
REFERENCES
1. Pati S, Lorch SA, Lee GE, Sheffler-Collins S,Shah SS. Health insurance and length ofstay for children hospitalized with community-acquired pneumonia. J Hosp Med. 2012;7(4):304–310
2. Ambroggio L, Taylor JA, Tabb LP, NewschafferCJ, Evans AA, Shah SS. Comparative ef-fectiveness of empiric b-lactam mono-therapy and b-lactam–macrolide combinationtherapy in children hospitalized withcommunity-acquired pneumonia. J Pediatr.2012;161(6):1097–1103
3. Bradley JS, Byington CL, Shah SS, et al. Themanagement of community-acquired pneu-monia in infants and children older than 3months of age: clinical practice guidelinesby the Pediatric Infectious Diseases Societyand the Infectious Diseases Society ofAmerica. Clin Infect Dis. 2011;53(7):e25–76
4. Shah SS, Test M, Sheffler-Collins S, Weiss AK,Hall M. Macrolide therapy and outcomesin a multicenter cohort of children hos-pitalized with Mycoplasma pneumoniaepneumonia. J Hosp Med. 2012;7(4):311–317
5. Lu YJ, Chen TH, Lin LH, Shen CM, Huang CH.Macrolide use shortens fever duration inMycoplasma pneumoniae infection in chil-dren: a 2-year experience. J Microbiol Immu-nol Infect. 2008;41(4):307–310
6. Defilippi A, Silvestri M, Tacchella A, et al.Epidemiology and clinical features of My-coplasma pneumoniae infection in chil-dren. Respir Med. 2008;102(12):1762–1768
7. Sakurai N, Nagayama Y, Honda A, MakutaM, Yamamoto K, Kojima S. Mycoplasmapneumoniae and other pathogens in theaetiology of lower respiratory tract infections
among Japanese children. J Infect. 1988;16(3):253–261
8. Waites KB. New concepts of Mycoplasmapneumoniae infections in children. PediatrPulmonol. 2003;36(4):267–278
9. Korppi M, Heiskanen-Kosma T, Kleemola M.Incidence of community-acquired pneumoniain children caused by Mycoplasmapneumoniae: serological results of a pro-spective, population-based study in primaryhealth care. Respirology. 2004;9(1):109–114
10. Mulholland S, Gavranich JB, Gillies MB,Chang AB. Antibiotics for community-acquired lower respiratory tract infec-tions secondary to Mycoplasma pneumoniaein children. Cochrane Database Syst Rev.2012;9:CD004875
11. Aurangzeb B, Hameed A. Comparative effi-cacy of amoxicillin, cefuroxime and
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 6, June 2014 1089 by guest on September 8, 2020www.aappublications.org/newsDownloaded from

clarithromycin in the treatment ofcommunity-acquired pneumonia in chil-dren. J Coll Physicians Surg Pak. 2003;13(12):704–707
12. Ferwerda A, Moll HA, Hop WC, et al. Efficacy,safety and tolerability of 3 day azithromycinversus 10 day co-amoxiclav in the treat-ment of children with acute lower re-spiratory tract infections. J AntimicrobChemother. 2001;47(4):441–446
13. Harris JA, Kolokathis A, Campbell M, CassellGH, Hammerschlag MR. Safety and efficacyof azithromycin in the treatment of community-acquired pneumonia in children. PediatrInfect Dis J. 1998;17(10):865–871
14. Toltzis P. Determining the best regimen forchildren hospitalized with CAP. J Pediatr.2012;161(6):A1–A2
15. Hersh AL, Shapiro DJ, Pavia AT, Shah SS.Antibiotic prescribing in ambulatory pedi-atrics in the United States. Pediatrics. 2011;128(6):1053–1061
16. Bradley JS, Arguedas A, Blumer JL, Sáez-LlorensX, Melkote R, Noel GJ. Comparative study oflevofloxacin in the treatment of children withcommunity-acquired pneumonia. Pediatr In-fect Dis J. 2007;26(10):868–878
17. Sterner G, Fransén H, Tunevall G, SvedmyrA. A comparative trial of cephaloridine anderythromycin in hospitalized pneumonicpatients. Postgrad Med J. 1967;43(Suppl43):43–, 53–54
18. Oxford Centre for Evidence-Based Medicine.The Oxford levels of evidence 2. 2013.Available at: www.cebm.net/index.aspx?o=5653. Accessed August 29, 2013
19. Viswanathan M, Ansari MT, Berkman ND,et al. Assessing the Risk of Bias of In-dividual Studies in Systematic Reviews ofHealth Care Interventions. Rockville, MD:Methods Guide for Effectiveness and Com-parative Effectiveness Reviews; 2008
20. Esposito S, Bosis S, Faelli N, et al. Role ofatypical bacteria and azithromycin therapyfor children with recurrent respiratory
tract infections. Pediatr Infect Dis J. 2005;24(5):438–444
21. Garo B, Garré M, Quiot JJ, et al. Myco-plasma pneumoniae infections. A multi-center retrospective study of 182 cases [inFrench]. Presse Med. 1988;17(29):1475–1478
22. Gendrel D, Raymond J, Moulin F, et al Eti-ology and response to antibiotic therapy ofcommunity-acquired pneumonia in Frenchchildren. Eur J Clin Microbiol Infect Dis.1997;16(5):388–391
23. Sáez-Llorens X, Castaño E, Wubbel L, et al.Importance of Mycoplasma pneumoniaeand Chlamydia pneumoniae in childrenwith community-acquired pneumonia [inSpanish]. Rev Med Panama. 1998;23(2):27–33
24. Wubbel L, Muniz L, Ahmed A, et al. Etiologyand treatment of community-acquiredpneumonia in ambulatory children.Pediatr Infect Dis J. 1999;18(2):98–104
25. Principi N, Esposito S, Blasi F, Allegra L;Mowgli Study Group. Role of Mycoplasmapneumoniae and Chlamydia pneumoniae inchildren with community-acquired lowerrespiratory tract infections. Clin Infect Dis.2001;32(9):1281–1289
26. Kogan R, Martínez MA, Rubilar L, et al.Comparative randomized trial of azi-thromycin versus erythromycin and amox-icillin for treatment of community-acquiredpneumonia in children. Pediatr Pulmonol.2003;35(2):91–98
27. Matsubara K, Morozumi M, Okada T, et al Acomparative clinical study of macrolide-sensitive and macrolide-resistant Myco-plasma pneumoniae infections in pediatricpatients. J Infect Chemother. 2009;15(6):380–383.
28. Kawai Y, Miyashita N, Yamaguchi T, et al.Clinical efficacy of macrolide antibioticsagainst genetically determined macrolide-resistant Mycoplasma pneumoniae pneu-monia in paediatric patients. Respirology.2012;17(2):354–362
29. Ruhrmann H, Blenk H. Erythromycin versusamoxicillin for the treatment of pneumoniain children (author’s transl) [in German].Infection. 1982;10(Suppl 2):S86–S91
30. Gomez Campdera JA, Navarro Gomez ML,Hernandez Sampelayo T, Merello Godino C,Sanchez Sanchez C. Azithromycin in thetreatment of ambulatory pneumonia inchildren. Acta Pediatr Esp. 1996;54(8):554–562
31. Leyenaar JK, Shieh MS, Lagu T, Pekow PS,Lindenauer PK. Comparative effectivenessof ceftriaxone in combination with a mac-rolide compared with ceftriaxone alone forpediatric patients hospitalized with com-munity acquired pneumonia [publishedonline ahead of print]. Pediatr Infect Dis J.2013
32. Carbon C, Isturiz R. Narrow versus broadspectrum antibacterials: factors in the se-lection of pneumococcal resistance to beta-lactams. Drugs. 2002;62(9):1289–1294
33. Davey P, Brown E, Charani E, et al. Inter-ventions to improve antibiotic prescribingpractices for hospital inpatients. CochraneDatabase Syst Rev. 2013;4:CD003543
34. Walker E, Hernandez AV, Kattan MW. Meta-analysis: its strengths and limitations.Cleve Clin J Med. 2008;75(6):431–439
35. Forsyth BR, Bloom HH, Johnson KM, ChanockRM. Etiology of primary atypical pneumoniain a military population. JAMA. 1965;191:364–368
36. Chanock RM, Mufson MA, Bloom HH, JamesWD, Fox HH, Kingston JR. Eaton agentpneumonia. JAMA. 1961;175:213–220
37. Kingston JR, Chanock RM, Mufson MA, et al.Eaton agent pneumonia. JAMA. 1961;176:118–123
38. Michelow IC, Olsen K, Lozano J, Duffy LB,McCracken GH, Hardy RD. Diagnostic utilityand clinical significance of naso- and oro-pharyngeal samples used in a PCR assay todiagnoseMycoplasma pneumoniae infection inchildren with community-acquired pneumonia.J Clin Microbiol. 2004;42(7):3339–3341
1090 BIONDI et al by guest on September 8, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-3729 originally published online May 26, 2014; 2014;133;1081Pediatrics
Shawn RalstonEric Biondi, Russell McCulloh, Brian Alverson, Andrew Klein, Angela Dixon and
Treatment of Mycoplasma Pneumonia: A Systematic Review
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/133/6/1081including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/133/6/1081#BIBLThis article cites 36 articles, 3 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on September 8, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-3729 originally published online May 26, 2014; 2014;133;1081Pediatrics
Shawn RalstonEric Biondi, Russell McCulloh, Brian Alverson, Andrew Klein, Angela Dixon and
Treatment of Mycoplasma Pneumonia: A Systematic Review
http://pediatrics.aappublications.org/content/133/6/1081located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2014/05/20/peds.2013-3729.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2014has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on September 8, 2020www.aappublications.org/newsDownloaded from