Treatment of Heart Failure Claire Hunter, MD. Treatment of Heart Failure Goals Improve quality of...
37
Treatment of Heart Failure Claire Hunter, MD
-
Upload
matilda-francis -
Category
Documents
-
view
214 -
download
0
Transcript of Treatment of Heart Failure Claire Hunter, MD. Treatment of Heart Failure Goals Improve quality of...

Treatment of Heart Failure
Claire Hunter, MD


Treatment of Heart Failure
• Goals
• Improve quality of life
• Prolong life
• Ejection fraction most important prognostic factor
• Those with ejection fraction less than 20% have 50% 1-2 year survival

Treatment strategy
• Etiology of heart failure
• Precipitating agents of circumstances
• Evaluation of decompensation
• Nonpharmacologic and pharmacologic treatments

Etiology of Insult to myocardium
• Infarction/Ischemia--loss of myocyte function• Pressure overload• hypertensive heart disease• aortic stenosis• pulmonic stenosis• hypertrophic cardiomyopathy• Volume overload• aortic regurgitation • mitral regurgitation
Etiology continued
• Idiopathic dilated cardiomyopathy (may be viral)• Infiltrative in myocardium or interstitium• sarcoid• iron(hemochromatosis)• amyloid• radiation fibrosis• chemotherapeutic agents (anthracyclines)

Precipitating agents or circumstances
• Ischemia
• Dietary or medication noncompliance (sodium intake)
• Work overload--emotional stress or isometric activity
• Arrhythmias--atrial or ventricular
Evaluation of decompensation
• Dietary review• “Pill count”• Review social circumstances and enlist aid of
social worker if needed• Echocardiography--reassess left ventricular
function, valvular abnormalities• Arrhythmias• Ischemia evaluation (imaging stress or
angiography

Nonpharmacologic treatments
• Dietary reinforcements--2000 mg Na daily
• Rest (not necessarily bed rest)
• Decrease stress
• Assess any added medications that are deleterious
• nonsteroidal antiinflammatory agents

Pharmacologic treatments
• Positive inotropic agents
• digitalis
• catecholamines
• phosphodiesterase inhibitors

Digitalis
• Has not been proven to prolong survival
• Decreases hospitalizations
• Slight increase in arrhythmias
• Improves symptoms of congestion

Catecholamines
• Dobutamine (synthetic)
• Dopamine
• Increase heart rate and myocardial oxygen demand
• Tolerance to effects develops after 72 hours
• Have not been proven long term to improve survival

Phosphodiesterase Inhibitors
• Milrnone, amrinone
• In some trials increase mortality ( oral form and with chronic treatment)
• Short term intravenous treatment decreases pulmonary hypertension and left ventricular filling pressures; but may increase ventricular arrhythmias
Mechanism of heart failure
• Loss of myocardial function triggers
• SYMPATHETIC NERVOUS SYSTEM to compensate
• Cardiac output - heart rate x stroke volume
• Increases constricting and volume expanding hormones

Mechanism continued
• Failing heart down regulates B1 receptors
• Increased filling pressure in ventricle triggers plasma renin angiotensin system
(vasoconstriction and increased afterload)
Afterload reduction
• ACE inhibitors (angiotensin converting enzyme)
• ARB (angiotensin receptor blockers)
• Direct arterial dilators

Angiotensin converting enzyme inhibitors
• Proven to reduce development of overt heart failure in with asymptomatic left ventricular dysfunction
• Proven to prolong survival
• Reduce microalbuminuria in diabetics

Angiotensin Receptor Blockers
• Mortality results have been mixed in studies
• Beneficial symptomatically
• Whether equal to ACE inhibitors remains to be seen
Direct arterial dilators
• Hydralazine best oral example
• Nitroprusside best parenteral example
• Hydralazine used in combination with nitrates proven to prolong survival
• Not as good as ACE inhibitors at reducing mortality

Beta blockers
• Sympathetic activation• Leads to increased circulating catecholamines• By way of the B1 receptor they • Activate the Gs protein which• Activates adenylate cyclase which• Activates cAMP(increases)• Activate protein kinase• Leads to increased intracellular calcium• Leads to improved contractility

Beta receptor down regulation
• Occurs with sympathetic overstimulation
• Receptor uncoupling
• Leads to increased Gi (tonic inhibition)
• Calcium overload (toxic to myocardium)

Beta blockers
• Negative inotropic agents initially
• Restore B1 density and thus lead to
• Ultimate biologic improvement of ejection fraction
• Negate arrhythmogenic effects of catecholamines

Beta blockers
• Improve survival• Selective
• Sustained release metoprolol
• Bisoprolol
• Nonselective • Carvedilol (added value of antioxidant and
alpha effects)

Diuretics
• Treat volume overload
• Relieve symptoms of congestion
• Do not affect survival
• Do not alter remodelling

Diuretics continued
• Thiazides
• Loop diuretics
• Metolozone
Spironolactone
• Improves survival for Class III or IV heart failure
• Most likely due to effects on interstitium, not diuretic effects
• Potassium retention
• Beware of use in those whose creatinine is more than 2.5
Actions of BNP• Hemodynamic
balanced vasodilationcoronary arteries
• Neurohormonaldecreases aldosteronedecreases endothelin
• Renalincreases diuresisincreases natriuresis

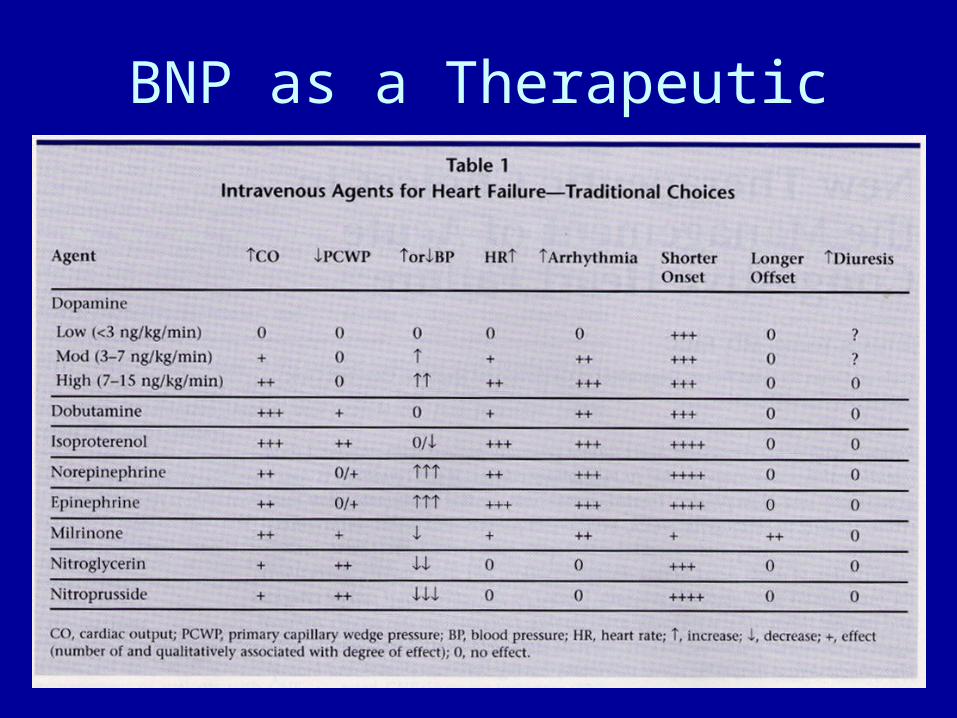
BNP as a Therapeutic




Disease Management
• Telemonitoring
• Weekly educational mailings
• Medical claims declined by $1100 per patient in treatment group
• Claims increased $9600 in non-treatment group

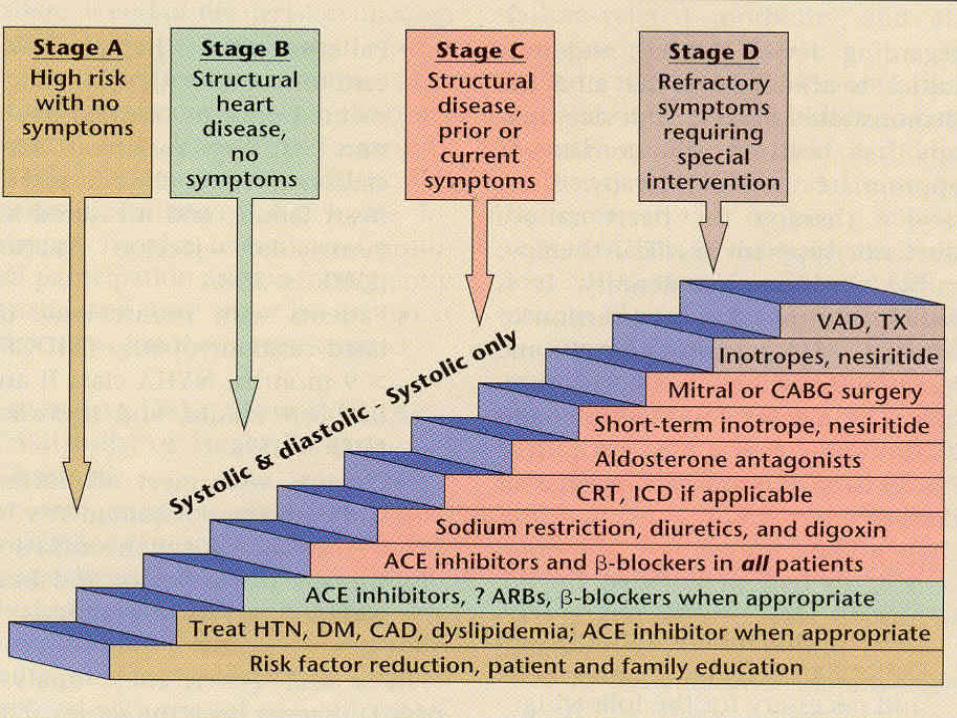
Goals of Treatment
• Improve cardiac function and survival with• ACE inhibitors• Beta blockers• Diuretics if needed for symptoms• Spironolactone for Class III or IV

Accomplish these goals
• Decreasing sympathetic drive and its toxic effects on the myocardium
• Decreasing the constricting hormones that increase afterload and increase the work for the heart
• Positively impact remodelling so the heart can be more efficient