Treating the outpatient with severe IBD: Case studies
48
Treating the outpatient with severe IBD: Case studies Daniel H. Present, MD, MACG Clinical Professor of Medicine The Mount Sinai School of Medicine Russell D. Cohen, MD, FACG, AGAF Professor of Medicine, Pritzker Medical School Co-Director, Inflammatory Bowel Disease Center The University of Chicago Medical Center 1
description
Treating the outpatient with severe IBD: Case studies. Daniel H. Present, MD, MACG Clinical Professor of Medicine The Mount Sinai School of Medicine Russell D. Cohen, MD, FACG , AGAF Professor of Medicine, Pritzker Medical School Co-Director, Inflammatory Bowel Disease Center - PowerPoint PPT Presentation
Transcript of Treating the outpatient with severe IBD: Case studies

Treating the outpatient with severe IBD: Case studies
Daniel H. Present, MD, MACGClinical Professor of Medicine
The Mount Sinai School of Medicine
Russell D. Cohen, MD, FACG, AGAFProfessor of Medicine, Pritzker Medical School
Co-Director, Inflammatory Bowel Disease CenterThe University of Chicago Medical Center
1

Case 1 : Severe Ulcerative Colitis
• Russ Cohen
2

New Patient Visit• 24 yo Black female
• Moved to Chicago from Maryland to pursue career at Boeing.
• 1 month ago: developed painless BRBPR with mucus:– Flexible sigmoidoscopy to 60cm: 10cm of proctitis; normal
proximal. Biopsies of the affected area revealed active proctitis, crypt abscesses, not much chronicity. Proximal biopsies were normal.
3

What Would YOU Do?
1. Any additional workup at this time?a. Full colonoscopy?b. Small bowel imaging?c. Upper endoscopy?
2. Therapeutic Options:a. Mesalamine 1g suppositories qhs?b. Mesalamine 4g enemas qhs?c. Topical steroids instead?d. Oral 5-ASA? e. Oral steroids? 4

Initial Clinical Course
• Starts 5-ASA suppositories• Initially attains remission• Stops suppositories, relapses.• Restart suppositories – not responding, now
worse.– 5 to 6 blood bowel movements, cramping,
diarrhea
5

What Would YOU Do?
1. Restart 5-ASA 1g suppository; see how she does.
2. Start 5-ASA enema?3. Start oral 5-ASA?4. Start oral steroids?5. Check stool specs.6. Start nothing; set up for scope
6

Your Decision…
• She underwent flexible sigmoidoscopy (unprepped) in your office:– Limited to 40cm– Showed moderately
active UC to 30cm with an abrupt cut-off to normal mucosa
7
L Colon: Sharp demarcation line
Rectum: Circumferential, Continuous Inflammation

Next Steps:
• Mesalamine enemas started; patient can’t hold them.
• Oral mesalamine 4.8g started; patient seemed to worsen.
• Oral prednisone (20mg po bid) started; patient still without obvious improvement.
8

Why Aren’t the Steroids Working?
1. ? Too sick2. ? Infected (ie. C diff)3. ? Wrong Diagnosis4. They are working for his colitis; diarrhea is of
other origin.– Celiac?– 5-ASA diarrhea?– IBS?– Dietary
9

Acute, Severe Colitis….
• Typically Abrupt Onset.– Often can identify a “trigger”:
• Infection, antibiotic, major life stress– “Get Over” the acute insult.
• Often Early in Disease Course:– 10% of fulminant colitics – initial presentation.– Median Age early- mid 30’s– Disease Duration: median 4-7 years
Cohen RD et al. Am J Gastroenterol 1999;94:1587-92.Stack WA et al. Aliment Pharmacol Ther 1998;12:973-8Wenzl HH et al. Z Gastroenterol 1998;36:287-93. D’Haens G et al. Gastroenterology 2001;120:1323-9Hyde GM et al. Eur J Gastroenterol Hepatol 1998;10:411-3. 10

Options for Severe Colitis
• If responsive to oral steroids:– Immunomodulators (aza, 6MP) with gradual
taper of steroids– Infliximab– Adalimumab
11

Azathioprine or 6-MP in UC
AZA
Placebo
AZA/6-MP
Steroid-Dependent Active UCMaintenance of Remission in UC
Res
pons
e R
ate
Rel
apse
Rat
e
Placebo
1)Jewell DP, Truelove SC. Br Med J. 1974;4:627-630. 2) Hawthorne AB, et al. Br Med J. 1992;305:20-22. 3) Ardizzone S, et al. Gut. 2006;55:47-53. 4) Mantzaris et al. Am J Gastroenterol. 2004;99:1122-1128.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1.5-2.0 mg/kg/d1 100 mg/d2
0%
10%
20%
30%
40%
50%
60%
70%
80%
100 mg/d2 2.0 mg/kg/d3 2.2mg/k/d4
AZA: azathioprine.
6-MP: 6-mercaptopurine

UC – Maintenance Therapy n=83
George J et al. Amer J Gastroenterol 1996; 91:1711
Prob
abili
ty o
f Rem
issi
onM
aint
enan
ce
Months
1.0
.8
.6
.4
.2
00 20 40 60
6-MP Maintenance in UC

611
34
2628
36
05
10152025303540
8 Weeks 30 Weeks
Perc
ent o
f Pat
ient
s
Placebo IFX 5 mg/kg IFX 10 mg/kg
Infliximab in UC: Clinical Remission
15 16
393432
37
05
1015202530354045
8 Weeks 30 Weeks
Perc
ent o
f Pat
ient
s
Placebo IFX 5 mg/kg IFX 10 mg/kg†
†
†
†P.002 vs placebo‡P.003 vs placebo
†
‡
‡
‡
‡
ACT 1 ACT 2
Rutgeerts P et al. N Engl J Med. 2005;353:2462-2476.

Infliximab in UC: Mucosal Healing
3425
62
5059
49
0
10
20
30
40
50
60
70
8 Weeks 30 Weeks
Perc
ent o
f Pat
ient
s
Placebo IFX 5 mg/kg IFX 10 mg/kg†
†
† †
†P<.001 vs placebo‡P.009 vs placebo
31 30
60
46
6257
0
10
20
30
40
50
60
70
8 Weeks 30 Weeks
Perc
ent o
f Pat
ient
s
Placebo IFX 5 mg/kg IFX 10 mg/kgACT 1 ACT 2
‡
‡‡
‡
Mucosal healing = endoscopic subscore of 0 or 1
Rutgeerts P et al. N Engl J Med. 2005;353:2462-2476.

Infliximab in UC Corticosteroid Discontinuation
at Week 30
10
24
19
0
5
10
15
20
25
30
Perc
ent o
f Pat
ient
s
Placebo IFX 5 mg/kg IFX 10 mg/kg
†
†P=.030 vs placebo‡P.010 vs placebo
3
18
27
0
5
10
15
20
25
30
Perc
ent o
f Pat
ient
s
Placebo IFX 5 mg/kg IFX 10 mg/kg
‡
‡
ACT 1 ACT 2
Rutgeerts P et al. N Engl J Med. 2005;353:2462-2476.

Infliximab, Azathioprine, or Infliximab + Azathioprine for the Treatment of Moderate to Severe Ulcerative Colitis:
“UC SUCCESS Trial”
Panaccione et al. DDW 2011 Abstract #835
Possible escape* (blinded)
IFX (5 mg/kg) + PBO(n=78)
AZA + PBO(2.5 mg/kg) (n=79)
IFX+AZA(n=80)
Randomization of Patients
VisitsWeek 0
Week 2
Week 6
Primary Evaluation
Infusions
Week 16
Week 14
*Subjects not achieving ≥1 point improvement in partial Mayo score
Week 8
ABSTRACT ONLY

Aza (n=76) IFX (n=77) Both (n=78)0%
10%
20%
30%
40%
50%
24% 22%
40%
Week 16 Steroid Free Remission*
* Total Mayo score < 2, no subscore >1, no steroids.
P = 0.032 vs. AZAP = 0.017 vs. IFX
Infliximab, Azathioprine, or Infliximab + Azathioprine for the Treatment of Moderate to Severe Ulcerative Colitis:
“UC SUCCESS Trial”
Panaccione et al. DDW 2011 Abstract #835ABSTRACT
ONLY

Co-administration of Immunosuppressants: Dramatically
Lower anti-Infliximab antibody rates• “SONIC” Crohn’s Disease Trial:
• Infliximab alone: 14% anti-Infix antibodies• Infliximab + Aza: 1% anti-Infix antibodies
• “UC-Success” Ulcerative Colitis Trial:• Infliximab alone: 14% anti-Infix antibodies• Infliximab + Aza: 1% anti-Infix antibodies

Adalimumab in Moderate to Severe UC
Placebo Adalimumab 80/40 Adalimumab 160/800%
4%
8%
12%
16%
20%
9.2% 10.0%
18.5%
• 8 week trial: Doses given weeks 0,2,6.• Primary endpoint: Clinical Remission (Mayo score < 2; no subscore >1).• * p=0.031 vs. placebo. • SAE: 7.6%, 3.8%, 4.0% respectively. 2 malignancies: both in placebo (basal cell;
breast)
*
Reinisch W et al. Gut ;2011 (online Jan 5, 2011: 10.1136/gut.2010.221127)

Adalimumab: Induction of Clinical Remission in Moderate to Severe UC (DDW 2011)
• 8 week endpoint (52 week trial): Doses given weeks 0,2,6.• 494 Patients: moderate to severe UC• Primary endpoints: Clinical Remission at weeks 8 and 52.• Response rates: 34.6% placebo vs. 50.4% ADA (p<0.001)
Clin
ical
Rem
issi
on
* p=0.019 vs. placebo.
Sandborn W et al. DDW 2011, abstract #744. ABSTRACT ONLY
Week 8: Remission

Adalimumab: Mucosal Healing in Moderate to Severe UC (DDW 2011)
• 8 week endpoint (52 week trial): Doses given weeks 0,2,6.• 494 Patients: moderate to severe UC• Primary endpoints: Clinical Remission at weeks 8 and 52.
Clin
ical
Rem
issi
on
* p=0.032
Sandborn W et al. DDW 2011, abstract #744.ABSTRACT
ONLY
Week 8

Back to the case:
• Patient started on infliximab and azathioprine.
• Initially also on topical therapies.• Steady response; steroids successfully
tapered.• Subsequent colonoscopy revealed no active
disease, although chronic mucosal changes and pseudopolyps characterized rectum – to –distal L colon. 23

Case #2: Severe Crohn’s Disease
• Dan Present
24

New Patient Appointment• 30 yo W Male
• 10- yr history of vague crampy abd pain, intermittent but became more persistent.
• Recalls going to the local ER about 8 years ago while in college and subsequently having “intestine xrays where I had to drink barium” which suggested possible Crohn’s disease. Thinks he had a colonoscopy and “didn’t show anything” but didn’t know if the ileum was intubated. 25

Current Symptoms
• Post-prandial watery bowel movements.• Admits that he has lost about 20lbs in the
past few months due to “it hurts when I eat too much.”
• Fatigued. • Vague joint pains.• Asks if he can step outside to smoke a
cigarrette…26

WHAT WOULD YOU DO?
1. Order a colonoscopy?2. Order small bowel imaging?
a. If so, which one?3. Start mesalamine 4g4. Start metronidazole 500mg tid?5. Start anti-TNF?
27

Diagnostic Workup• SBFT: Multiple strictures of the distal jejunum,
mid- and distal ileum, with normal intervening mucosa. Active inflammation. No proximal dilation.
• Colonoscopy: colon normal; ileum: narrowed; some ulcerations.
• Bx: Ileum: Ileitis c/w Crohn’s. Colon: normal• Diagnosed with “Crohn’s disease”
28

Now, What Would YOU Do?
1. Mesalamine 4g2. Budesonide CIR 9mg3. Prednisone 40mg4. 6MP initiation5. Anti-TNF6. Natalizumab7. Surgery
29

Clinical Course
• Budesonide 9mg started– Plan is to decrease by 3mg every 3 weeks.
• 6MP 75mg started (pt weight 75kg)– Increased to 100mg after 2-3 weeks.– (TPMT genotype was wildtype)
• Although pt felt better on 9mg budesonide, he could not decrease the dose to 6mg without relapse
30

At this point
• WBC 3,500 Polys: 80%, Bands 2%• Hgb 12.5• Platelet count: 200,000• LFT’s: normal
• 6TG: 325 6MMP 5,000
31

What Would YOU Do?
1. Switch from budesonide to prednisone 40mg
2. 6MP dose increase3. Anti-TNF4. Natalizumab5. Surgery
32

You start an anti-TNF:
1. And stop the 6-MP?2. And decrease dose of the 6-MP?3. With same dose of 6-MP?
33

P<0.001 vs. azaP=0.055 vs. ifx
P<0.001 vs. azaP=0.022 vs. ifx
Columbel JF et al. N Engl J Med 2010;362:1383-95.
Combination Therapy Increases Efficacy

Minimal Improvement
• Is seen on the infliximab• Suspecting a need for surgery, you order at
CT enterography: inflammation, – Still a substantial amount of SB activity,
multiple strictures but none are obviously obstructive.
35

What Would YOU Do?
1. Switch from budesonide to prednisone 40mg
2. 6MP dose increase3. Switch Anti-TNF4. Natalizumab5. Surgery
36

Decide to try Natalizumab
• JC virus antibody status: negative• Patient stops 6MP• Starts natalizumab 300mg IV q 28 days• Able to slowly wean off of Entocort over 3
months• 6 months out: well on natalizumab
37

Case 3: Severe Fistulous Crohn’s Disease
• Russ Cohen and Dan Present
38

Presentation To Your Office
• 45 yo W M with fistulous Crohn’s disease to the perineal area for 10 years.
• Colonoscopies to the ileum have always showed normal TI, normal colon, other than the distal rectum, which has some small ulcerations, and a anorectal stricture.
• Now with increased fistula discharge and increased difficulty in passing BM
39

Medications
• Prednisone 25mg po qd• Mesalamine 4.8 g qd• Previously on short-term antibiotics• Had previous fistulotomy 6-years ago
40

Physical Exam
• Abdominal exam: all normal• Perianal exam- multiple draining perianal
fistulas with mild fluctuance; previous fistula sites seen, as well as previous fistulotomy site.
• Attempted rectal examination – stricture too tight to allow introduction of finger-tip.
41

When do you call…
The surgeon?– Trial of antibiotics
first?– Trial of
immunomodulators first?
– Trial of anti-TNF first?
42

When do you order…
• Imaging?
CT?
MRI?
Dynamic proctography?
43
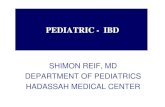
from: radiologyassistant.nl

Start antibiotics, sent to surgeon
• Orders MRI Pelvis to determine if fistulas connected to main cavity.
• Examination under anesthesia– Dilation of the stricture (Hegar)– Flex sig to 25cm: only distal rectal disease.– Multiple fistulas emanating from a single
fistula orifice on each side of the dentate line.• Fistulectomy x2, seton placed x2
44

Patient now sits in front of you..
• With 2 setons coming out their bottom• Wanting to know, “What ya gonna do?”
45

What You Gonna Do?
1. Continue 5-ASA ?2. Continue Steroids ?3. Start antibiotics?4. Start 6MP/ Azathioprine?5. Start MTX?6. Start anti-TNF?7. Start natalizumab?
46

What you did…
• Patient started on azathioprine and infliximab.
• Visits back to the surgeon after each induction dose of infliximab to evaluate need for setons (eventually removed).
• Patient well on azathioprine and infliximab
47

When do you stop therapy?
48