
Treating Co-occurring PTSD and Chronic Pain
62
Treating Co-occurring PTSD and Chronic Pain using an Acceptance-Based Approach Dr. Pamela L. Holens, C. Psych. University of Manitoba
Transcript of Treating Co-occurring PTSD and Chronic Pain
Treating Co-occurring PTSD and Chronic Pain
using an Acceptance-Based Approach
Dr. Pamela L. Holens, C. Psych.
University of Manitoba
What we know about pain acute vs chronic
What we know about PTSD a chronic “pain” response
The overlap between chronic pain and PTSD
Acceptance-based approaches
Outline
What We Know About Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
Official Definition (International Association for the Study of Pain)
Historical Understandings of the Pain Response
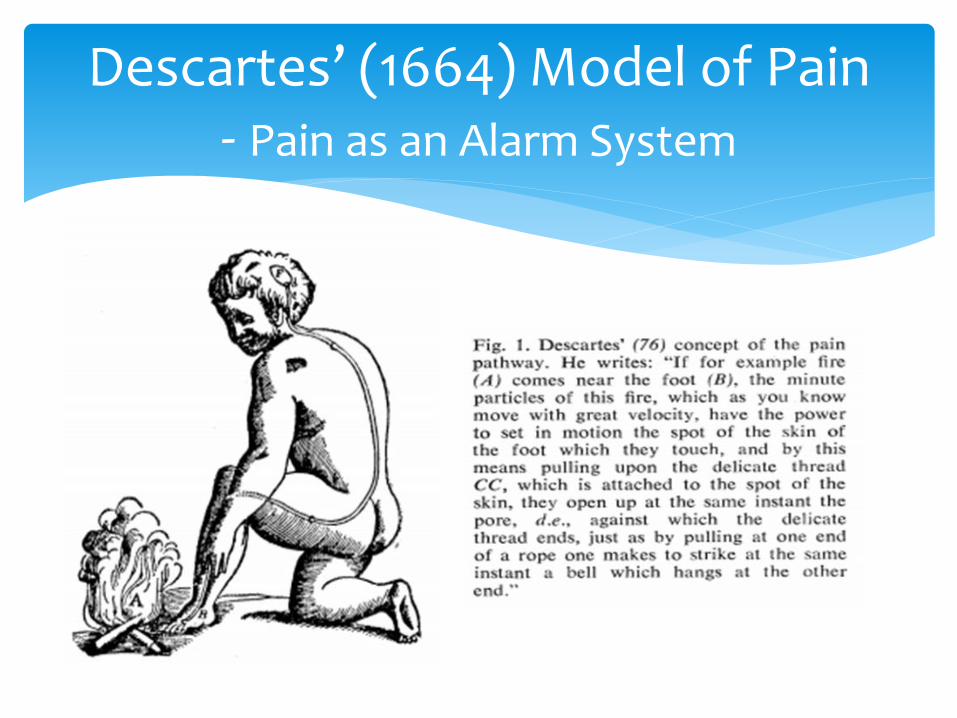
Descartes’ (1664) Model of Pain - Pain as an Alarm System
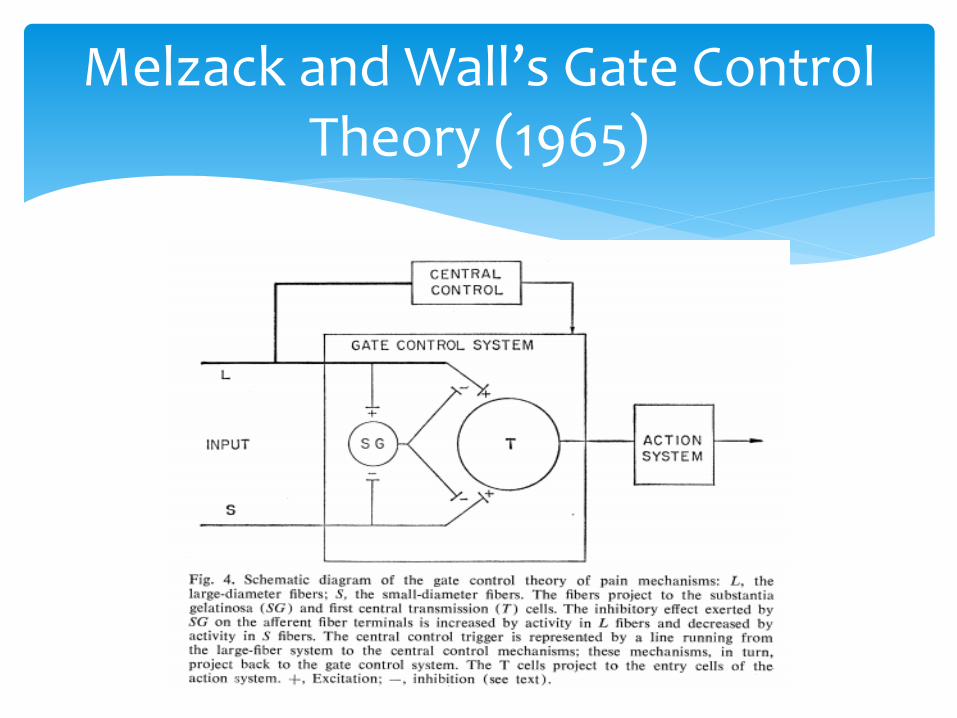
Melzack and Wall’s Gate Control Theory (1965)
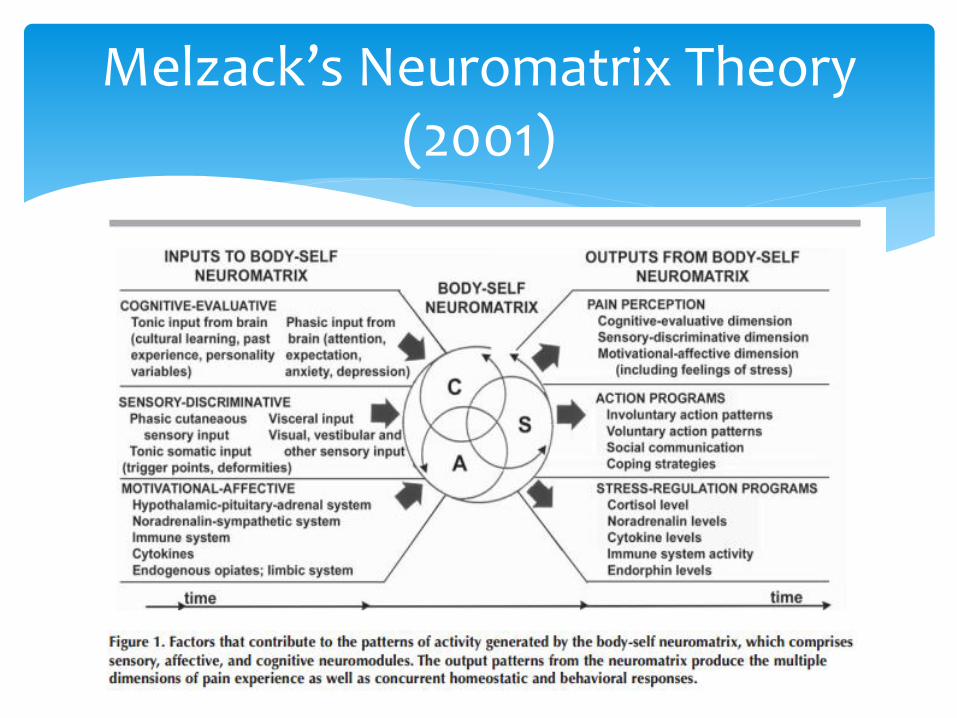
Melzack’s Neuromatrix Theory (2001)
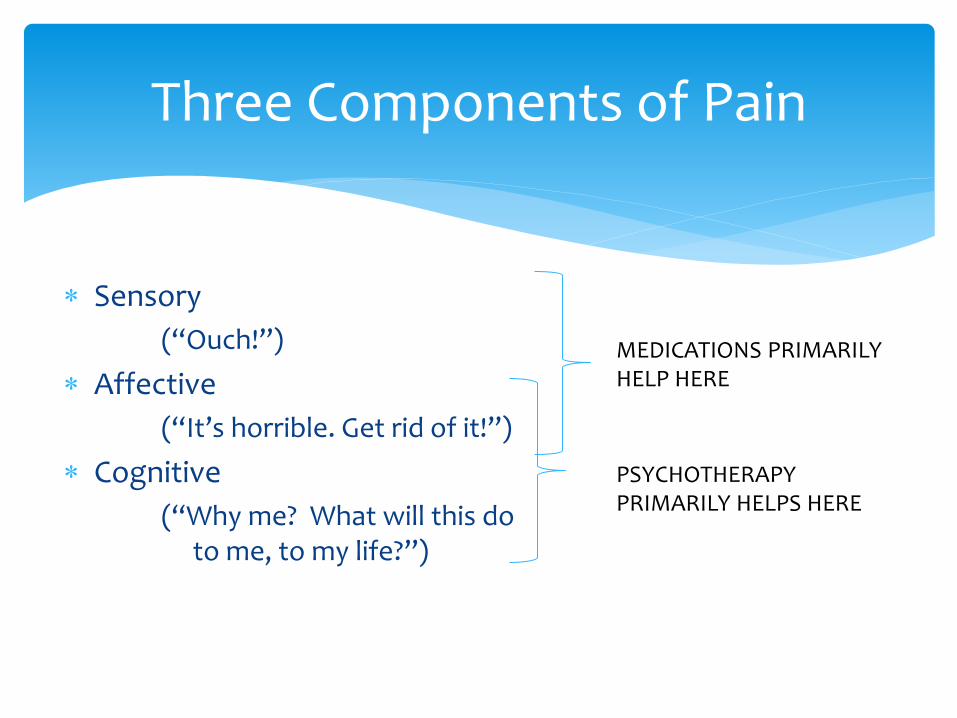
Three Components of Pain
Sensory
(“Ouch!”)
Affective
(“It’s horrible. Get rid of it!”)
Cognitive
(“Why me? What will this do to me, to my life?”)
MEDICATIONS PRIMARILY HELP HERE
PSYCHOTHERAPY PRIMARILY HELPS HERE

The actual, physical pain sensation is an adaptive reflex. It serves the function of alerting us to danger, tissue damage, or threats of such damage.
The noxious sensation of pain is critical for our survival.
The Pain Sensation

Signals injury or disease and produces actions to stop it or treat the causes, eg. Chest pains may signal heart disease and may force us to seek medical help
Memories of earlier pain and suffering warn us to avoid potentially dangerous situations
After serious injury or disease, pain makes us rest, promoting the body’s healing processes
Survival Functions of Pain (Melzack, 2005)

What is the value of phantom limb pain?
Many aches and pains (backaches, headaches, muscle pains, nerve pains, pelvic pains, facial pains) serve no discernible purpose, are difficult to treat, and are horrendous for the people who suffer them.
Chronic pain is not a warning to prevent physical injury or disease. It is the disease – the result of neural mechanisms gone awry.
Pain is valuable, but . . . . (Melzack, 2005)
Chronic Pain (AKA persistent pain):
Pain that persists beyond the usual course of an acute illness or healing time of an injury (usually beyond three to six months), associated with a pattern or recurrence over months or years or associated with a chronic pathological process. It is often accompanied by emotional (depressive) symptoms but objective physiological signs are sometimes absent (p. 3).
Pain Assessment and Management Clinical Practice Guidelines (WRHA, April 2012)
An alarm system working overtime
Chronic Pain is . . .
Causal and maintaining factors may be unclear
Efforts to reduce or eliminate the pain may be unsuccessful
Continuing attempts to control pain may be maladaptive, especially if they cause unwanted side effects or prevent participation in valued activities such as those involving work, family, or community
When pain is chronic . . . (McCracken et al., 2004).
Recommendation 17: Opioids (p. 12)
Opioids are not indicated in all chronic pain conditions, and medication alone is often insufficient to manage chronic pain. Other effective pharmacologic and non-pharmacologic treatments should also be considered.
Chronic Pain and Opioids (WRHA, 2012)
Non-Pharmacological Management (Recommendation 24: p. 16)
Superficial heat and cold
Massage
Relaxation
Imagery
Prayer/spiritual practices
Pressure/vibration
Music
Cognitive Behavioural Therapy (CBT)
Child/infant specific practices
Selection of non-pharmacological methods should be based on individual preference, and may include strategies such as:
Pain Catastrophizing (Turner & Aaron, 2001)
Fear Avoidance (Vlaeyen & Linton , 2000)
Low self-efficacy and Lack of perceived control (Arnstein et al., 1999; Litt, 1988)
Passive Pain Coping (McCracken & Eccleston, 2003) These factors are addressed in Cognitive Behavioural Therapy (CBT) for chronic pain
Psychological Factors Associated with Pain Severity and Disability
The development of avoidant behaviours motivated by fear of feeling pain.
Fear Avoidance
Excessive pain behaviours* in the service of decreasing physical activity and leading to physical deconditioning and increased risk for the development of worsening pain and other medical comorbidities (e.g., obesity) (Verbunt et al., 2003).
• e.g., grunting, sighing, frequently talking about
the pain, facial expressions, guarded movements,
restriction of movements
Disuse Syndrome
What We Know about PTSD
1) Exposure to a threat to well-being (traumatic event)
2) Symptoms, for longer than one month, of:
i) Re-experiencing
ii) Avoidance
iii) Hyperarousal
Posttraumatic Stress Disorder (PTSD)
An alarm system working overtime
Posttraumatic Stress Disorder is . . .
Avoidance of trauma-related thoughts and situations may work in the short-run, but in the long-run it prolongs posttrauma reactions and prevents individuals from getting over their trauma-related difficulties.
(Rothbaum, Foa, Hembree, 2007)
Avoidance maintains PTSD symptoms
“The world is an extremely dangerous place”
“I am incompetent/unable to cope”
Unhelpful thoughts and beliefs maintain PTSD symptoms
Combination of the following techniques:
1. Psychoeducation
2. Anxiety management
3. Cognitive restructuring
4. Exposure exercises
Recommended therapeutic strategies for treating PTSD
Foa, 1999
Demystify symptoms
Normalize and validate reactions
Reinforce personal effectiveness and hope
Psychoeducation
Relaxation Techniques are taught:
Slow breathing
Muscle relaxation
Anxiety management
Assumptions:
It’s not the situation itself that creates distress, but one’s perception of the situation
The most effective way to diminish/modify emotions is to change one’s perception
Cognitive restructuring
Clients are helped to confront safe but anxiety-arousing situations in order to decrease their excessive fear and anxiety.
Clients learn that they can tolerate these situations and that nothing bad happens to them.
(Rothbaum, Foa, Hembree, 2007)
Exposure Therapy
The Overlap Between Chronic Pain and PTSD
CHRONIC PAIN
PTSD BOTH
The co-morbid experience of chronic pain and PTSD appears to be associated with more severe presenting symptomatology than either condition alone (Geisser, Roth, Bachman et al., 1996)
Research on Chronic Pain and PTSD
CHRONIC PAIN
PTSD BOTH
Chronic Pain and PTSD frequently co-occur, and similar mechanisms, such as fear avoidance, anxiety sensitivity, and catastrophizing, may exist for maintaining both conditions (Otis, Keane, & Kerns, 2003) .
Research on Chronic Pain and PTSD
Among individuals utilizing an online chronic pain support group:
Fully 50% of participants met criteria for PTSD
For those with PTSD, more severe symptoms were related to lower levels of chronic pain acceptance
Conclusions-> Avoidance may be a mutually maintaining mechanism in chronic pain and PTSD
->Acceptance should be studied as a potential treatment link between the two disorders
Research on Chronic Pain and PTSD
Thomas (2012)
Factors that maintain both chronic pain and PTSD:
1) Attentional biases
2) Anxiety sensitivity
3) Pain acting as a reminder of the traumatic event
4) Avoidance is used for coping
5) Fatigue/lethargy/depression contribute
6) General anxiety contributes
7) Cognitive demands limit use of adaptive coping
The Mutual Maintenance Model Sharp & Harvey, 2001

Acceptance-Based Approaches
When “pain” is “unacceptable”:
Patients are likely to attempt to avoid it at all costs
Patients are likely to seek readily available interventions to reduce or eliminate it
-> These efforts may not be in their best interest if the consequences include no reductions in pain and many missed opportunities for satisfying and productive functioning
Why acceptance? (Kerns, Sellinger & Goodin, 2011)
Some patients may achieve better overall adjustment to chronic pain if they reduce their avoidance and other attempts to control chronic pain, increase their levels of acceptance, and direct their efforts toward goals they can achieve
Why acceptance? (Kerns, Sellinger, Goodin, 2011)
Pain is seen as an inevitable part of living that can be accepted, whereas struggling to avoid inescapable pain causes more suffering.
The more an individual struggles to escape the pain, the more he or she suffers.
An acceptance-based stance
Reports of lower pain intensity
Less pain-related anxiety and avoidance
Less depression
Less physical and psychosocial disability
Greater physical and social ability
Better work status (McCracken, 1998; McCracken & Velleman, 2010; McCracken & Zhao-O’Brien, 2010; Vowles & McCracken, 2008).
Greater acceptance of pain is associated with . . .
Acceptance of pain was found to be a significant predictor of adjustment on several measures of patient function, independent of perceived pain intensity (McCracken, 1998).
Level of acceptance of pain has been shown to be independent of pain intensity (i.e., it is not simply those with less pain who are more willing to accept pain) (McCracken et al., 2004).
Also . . .
With clinical and non-clinical populations alike, acceptance techniques (e.g., observing and accepting thoughts and feelings as they are) produce greater tolerance of acute pain and discomfort than do more traditional techniques of pain control, such as distraction and cognitive restructuring (Gutierrez et al, 2004; Levitt et al., 2004).
Laboratory studies have shown
ACT is a form of CBT that uses acceptance and mindfulness processes, as well as commitment and behaviour change processes, to produce greater psychological flexibility.
This is the treatment approach that we have chosen to use with our clients who have comorbid PTSD and chronic pain
Acceptance and Commitment Therapy (ACT)
ACT is a form of CBT, but it differs from traditional CBT in that rather than trying to teach people to better control their thoughts, feelings, sensations, and memories, ACT emphasizes observing thoughts, feelings, sensations, and memories as they are, without trying to change them, and behaving in ways consistent with valued goals and life direction.
ACT versus traditional CBT
While pain indeed hurts, it is an individual’s struggle with pain that causes suffering (Dahl & Lundgren, 2006).
ACT philosophy as applied to Chronic Pain
Experiential avoidance/Experiential control
Cognitive fusion
Lack of contact with the present moment
Problematic Processes addressed by ACT
Attempts to control, alter, or avoid the following: thoughts, feelings, sensations, or memories
Experiential Avoidance/ Experiential Control
Cognitive Fusion
Lack of contact with the present moment
Acceptance
Defusion
Self as Context
Contact with the Present Moment
Values
Committed Action
Six Core Therapeutic Processes of ACT
Acceptance: an alternative to experiential avoidance
Pain is ruining
my life
Cognitive Defusion
PAIN
Cognitive Defusion

Present Moment Awareness
Chronic Pain and PTSD . . . alarm systems working overtime
Quieting the alarm system
Mindfulness Meditation
Self as Context
Defining Valued Directions
Committed Action
Chronic pain and PTSD frequently co-occur
Both can be viewed as involving an overactive alarm system
Avoidance contributes to the maintenance and worsening of both conditions
Acceptance-based interventions assist with calming the alarm system and reducing avoidance, thereby improving overall functioning and Quality of Life.
In Summary . . .