Traumatic Cerebral Hernia - pdfs.semanticscholar.org · \ Mirror of Hospital Practice TRAUMATIC...
3
Transcript of Traumatic Cerebral Hernia - pdfs.semanticscholar.org · \ Mirror of Hospital Practice TRAUMATIC...
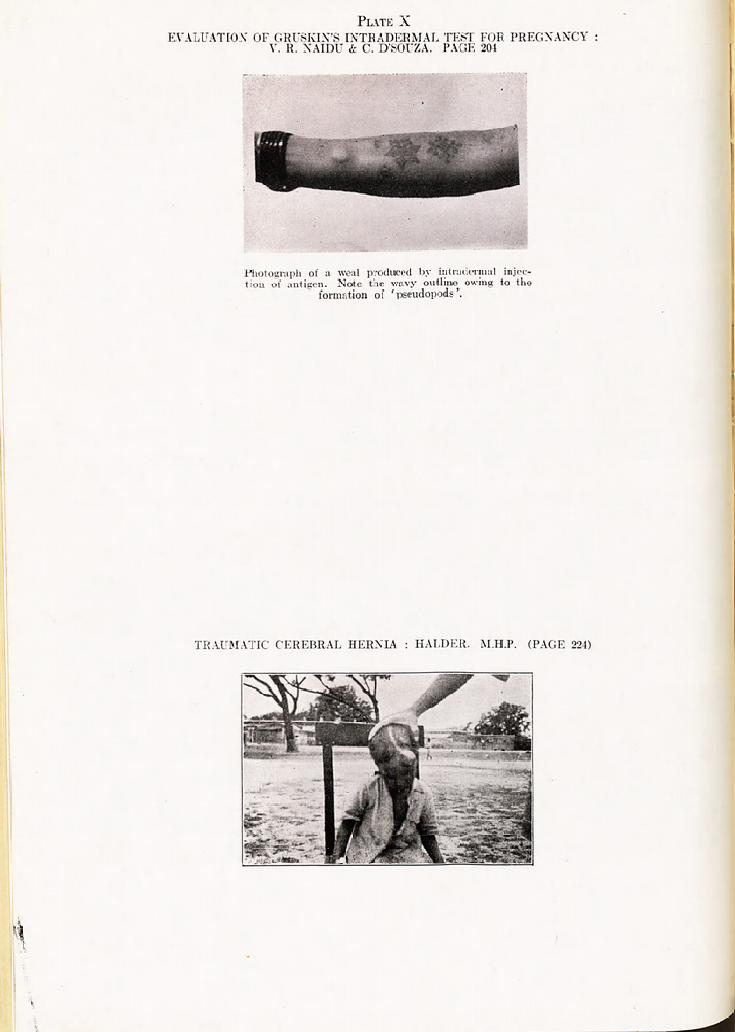
TRAUMATIC CEREBRAL HERNIA : HALDER. M.H.P. (PAGE 224)
\ Mirror of Hospital Practice
TRAUMATIC CEREBRAL HERNIA
By B. HALDER, m.b.
Assistant Surgeon, E. I. Railway Hospital, Jhajha, Bihar
Cerebral hernia, though very rarely met with in civil practice, is almost always a sequel to serious head injury. A compound fracture of the skull, a tear of the membraneous coverings of the brain and an increase of intracranial pressure are the three important causes that are usually responsible for the pathological condi- tion. An injury which gives rise to a localized
May, 1944] VOLVULUS OF THE SIGMOID COLON : SINGH 225
^'eakness of the osseofibrous coverings of the )rain matter leads to the development of such complication. Such injuries lead to a free
(ll'ainage of blood and, due io the natural decom- pression caused by the opening in the skull !J?ne, the symptoms are less severe than the lnJuries would lead one to expect. In fact, grave and alarming symptoms and sequelae are more often seen in closed head injuries than in open ones. Case report.?S., a Mohammedan male, aged
a'}out six years, was brought to the hospital on . nfl July, 1943, in an unconscious state, having een knocked down by a running train,
.-lamination revealed an injury to the vault of 10 skull on the frontal and parietal regions of .e left side. On cleaning, the wound showed
Pjeces of diploe, some lying loose but a few attached to the tissues. The wound was about , belies long and had a Y-shaped end on the left l0ntal angle, where examination revealed a
Portion of brain matter extruded and lacerated; f1 Quantity of cerebrospinal fluid was detected lr! and around the wound; in this area a big Piece of skull bone was missing.
-The whole wound was cleaned and stitched ter apposing the scalp margins and putting
Sw?e sulphonamide powder into the wound, but j.^culty was experienced at the junction of the inibs of the Y-shaped wound as the margins or le
scalp could not be apposed even after
Raping away a portion of the cerebral sub-
stance that had already been expelled out or le skull cavity and was lying on the anterior l)art of the wound. On the second day the chilcl
brought with retention of urine and faeces which was relieved by an enema. The wouncl ^ as not opened but the superficial dressings. onv Uere changed as they were soaked with blood
cerebrospinal fluid. The patient c'0lnatose?no temperature. ,
. Gradually the general condition of the cnil(
lnaproved, and he began to respond to questions ^ite normally. ,
()n the eighth day the wound was opened and 'e stitches were removed. All the stitches too
Perfectly, leaving a raw area on the front part 'ere the brain was exposed, and from where
J>0l'ebrospinal fluid was still oozing and soaking le dressings daily. ..
As days passed, this part began to swell up ^dually till the whole swelling came up to tlic sAZe of a ping-pong ball, and this tumour was Ulagnosed to be one of cerebral hernia.
4 y*?1 . ? Pulsation was noticed, and cerebrospinal fluid
> still oozing freely from the lower part oi the [V^our. Within a few days the child had a
JlSh temperature which lasted for four days, an 693 was freely administered as the fever
Was thought to be due to infection of the cerebro- spinal fluid. The fever was checked, and tiie
fUlnour was dressed every day with acriflavine |?tion. The illustration shows the size or tne
tumour about one month after the accident (see Plate X).
In accordance with the usual textbook treat- ment, the application of formalin soaked in a piece of gauze was started, with occasional dress- ings of absolute alcohol, as the child was
developing conjunctivitis due to daily applica- tions of formalin (the tumour being close to the left eye and the vapour of formalin irritating the eye). After a few days' application, a hard black crust began to form on the wound, and the cerebrospinal fluid leakage began to get less and less' till it stopped. An ulcer also
gradually began to form at the base of the tumour, on a level with the adjacent scar tissue, which gradually began to cut the tumour off the scalp till eventually in a month's time the whole tumour, which looked like a thick scab, separated from the scalp leaving a small ulcer. It took another fortnight for the ulcer to heal completely and for the skin to grow over it. A distinct gap with sharp margins can now be felt in the skull at the site of the scar. This part of the scalp is very thin and soft, and throbbing, though less prominent than before, is visible at that area. No deficiency in the mental outlook is noticed, and no neurological symptom is complained of by the patient.
Points to note :? 1. Such a serious injury with laceration and
expression of the brain substance does not
necessarily mean death or serious neurological deficiency symptoms as is commonly supposed.
2. Cerebral hernia developed at the site of
the deficiency in the skull bone where the
meninges were also torn. 3. Infection of the cerebrospinal fluid is a
complication which was efficiently checked by the prompt administration of sulphapyridine (M&B 693).
4. Spontaneous cure of the hernia with
medicinal applications occurred without thorough plastic operation and the attendant complica- tion and difficulties.
5. The case was treated in the out-patient department throughout.
6. Injury to the left frontal lobe of the brain does not lead to appreciable motor or sensory loss or late neurological sequel?. Memory and
intellect are apt to be affected as a late, after- effect.