Traumatic Brachial Plexus Injury: Assessment and Management Mohamed Khalid MCh.Orth, FRCS.Orth,...
72
Traumatic Brachial Plexus Injury: Assessment and Management Mohamed Khalid MCh.Orth, FRCS.Orth, Diplomate European Board of Hand Surgery With inputs from Dominic Power, Peripheral Nerve Surgeon, Queen Elizabeth Hospital, Birmingham.
-
Upload
samuel-bradford -
Category
Documents
-
view
259 -
download
1
Transcript of Traumatic Brachial Plexus Injury: Assessment and Management Mohamed Khalid MCh.Orth, FRCS.Orth,...

Traumatic Brachial Plexus Injury:Assessment and Management
Mohamed Khalid MCh.Orth, FRCS.Orth, Diplomate European Board of Hand Surgery
With inputs from Dominic Power, Peripheral Nerve Surgeon, Queen Elizabeth Hospital, Birmingham.

Objectives• Anatomy• Pathomechanics • Pathoanatomy• Pathophysiology• Common clinical patterns• BPI Classification• Key examination points• BPI investigation• Early management• Timing of surgery• Reconstruction priorities• Reconstruction ladder• Evolution of modern techniques• Reconstruction algorithm• Additional procedures• Results• Prognosis in BPI• Research areas• Clinical cases

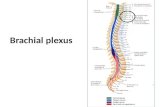
Brachial Plexus Anatomy
• Anterior primary rami of C5-T1• Phrenic nerve C3/4/5• 3 important nerves originate
above the clavicle– C5 root-dorsal scapular– C5/6/7 roots-long thoracic
nerve (Bell)– C5/6 upper trunk-
suprascapular nerve• T1 contributes preganglionic
sympathetic fibres to stellate ganglion

Pathomechanics of BPI


Pathoanatomy

Pathophysiology• Seddon 1943
– Neuropraxia • Focal demyelination• Axonal continuity
– Axonotomesis• Axonal loss • Wallerian degeneration
– Neurotmesis • Transection of a nerve
• Complex spectrum with several patho-physiological processes co-existing:– Focal ischaemia and oedema– Demyelination– Intraneural bleeding– Axonal loss– Nerve avulsions (post-
ganglionic)– Root avulsions (pre-ganglionic)– Spinal cord oedema and
haemorrhage– Intra- and peri-neural fibrosis– Anterior horn cell death

Common Clinical Patterns• Supraclavicular lesions
– Preganglionic or postganglionic– Myotome / dermatome
distribution• Infraclavicular lesions
– Postganglionic– Proximal peripheral nerve
distribution• Upper, Intermediate, Lower or
TBPI– Upper roots injured most
frequently– 80% patients are likely to have
at least some complete injury
• Upper roots (C5/C6) often postganglionic– Branches and interscalene
ligaments protect roots from avulsion• 60% ruptures• 40% avulsions
• Lower roots (C8/T1) usually preganglionic– Direct line of pull to spinal
cord• 85% avulsions• 15% ruptures

Upper Plexus - C5/6• “Bad shoulder, good hand”• Affects shoulder girdle muscles
– “Waiters tip” – Erb’s palsy – Adducted and internally rotated shoulder
• Root lesion– Serratus anterior, Rhomboids, Suprapsinatus, Infraspinatus,
Deltoid, Biceps brachii, Brachialis, Brachioradialis• More distal lesion
– Rhomboids spared (dorsal scapular nerve)– Serratus anterior spared (long thoracic nerve)

Intermediate Plexus - C7
• Rare in isolation– Tumour– Iatrogenic injury
• Co-exists with upper and lower plexus injuries– C5/6/7– C7/8/T1
• Minor impact– Weakness of wrist extensors– Can be used as ipsilateral intraplexal donor or
contralateral donor for reconstruction

Lower Plexus – C8/T1
• “Good shoulder, bad hand”– Klumpke’s palsy • Weakness FCU, FDP to ulnar digits• Loss of hand intrinsics • Loss of EIP• Loss of EPL• Medial forearm and hand sensory loss• Horner’s syndrome (loss of sympathetic outflow)

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination
• Obstetric• Adult

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination
• Traumatic– Traction, avulsion, penetrating wounds
• Infective– Cervical amyotrophy– Parsonage-Turner (viral brachial neuritis)
• Radiation induced• Malignant
– Pancoast tumour of the lung– Primary nerve tumours
• Iatrogenic– CVLs– Invasive angiography– Neck dissection

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination
• Supraclavicular• Infraclavicular

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination
• Preganglionic• Postganglionic

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination
• Upper plexus– C5/6– C5/6/7
• Lower plexus– C8/T1
• Panplexus– C5-T1

Classification of Brachial Plexus Palsy
• Age• Pathological• Anatomical• Combination
• Leffert– I open– II closed
• IIA Supra-clavicular– Pre-, Post-ganglionic
• IIB Infra-clavicular
– III radiation– IV obstetric
• IVA Erb’s• IVB Klumpke’s• IVC Mixed

Key Examination Points• ATLS
– Serial clinical examination• Flaccid paralysis of involved limb• Associated fractures and dislocations
– First rib, clavicle, cervical transverse processes, ipselateral limb fractures– Shoulder, ACJ , SCJ and scapulo-thoracic dislocations
• De-afferentiation pain• Long tract signs in lower limbs
– Asymmetry of reflexes, clonus, up-going plantar• Horner’s syndrome
– Miosis, ptosis, anhydrosis, enopthalmos• Phrenic nerve palsy• Loss of dorsal scapular nerve• Cervical plexus involvement
– Sensory loss proximal to clavicles– Paralysis of strap muscles– Cervical scoliosis

BPI Investigation– Imaging
• CXR, C spine, shoulder radiographs• MRI• Myelography + CT
– Neurophysiology tests• Somatosensory Evoked Potentials• NCS
– 6/52 neuropraxia resolution– Normal SNCVs and absent MNCVs in preganglionic lesions– Absent SNCVs and MNVCs in postganglionic lesions
• EMG– Fibrillation potentials– Spontaneous muscle depolarisations due to ACh receptor upregulation in
target muscles– Histamine Test
• Is it pre-ganglionic?• Historical interest only

CXR: Phrenic Nerve Palsy

CT Myelogram: C5/6 root avulsions

Early Management of BPI• Open injury:
– Early exploration– Debridement– Nerve repair, graft and transfers
• Closed injury:– Physiotherapy
• Shoulder abduction• Shoulder external rotation• Elbow ROM• ROM fingers
– Occupational therapy• Wrist splints• Resting intrinsic plus splints• Skin care for trophic areas• Education
– Regular clinical reassessment• Advancing Tinel test for regeneration in zones of axonotmesis• Deep muscle pain for early sign of reinnervation

Early Management of BPI• Open injury:
– Early exploration– Debridement– Nerve repair, graft and transfers
• Closed injury:– Physiotherapy
• Shoulder abduction• Shoulder external rotation• Elbow ROM• ROM fingers
– Occupational therapy• Wrist splints• Resting intrinsic plus splints• Skin care for trophic areas• Education
– Regular clinical reassessment• Advancing Tinel test for regeneration in zones of axonotmesis• Deep muscle pain for early sign of reinnervation

Case 1: Open root avulsions

Case 1: Open root avulsions

Case 2: Stab injury C5/C6

Case 2: Stab injury C5/C6

Case 2: Stab injury C5/C6

Case 2: Stab injury C5/C6

Early Management of BPI• Open injury:
– Early exploration– Debridement– Nerve repair, graft and transfers
• Closed injury:– Physiotherapy
• Shoulder abduction• Shoulder external rotation• Elbow ROM• ROM fingers
– Occupational therapy• Wrist splints• Resting intrinsic plus splints• Skin care for trophic areas• Education
– Regular clinical reassessment• Advancing Tinel test for regeneration in zones of axonotmesis• Deep muscle pain for early sign of reinnervation

Early Management of BPI• Open injury:
– Early exploration– Debridement– Nerve repair, graft and transfers
• Closed injury:– Physiotherapy
• Shoulder abduction• Shoulder external rotation• Elbow ROM• ROM fingers
– Occupational therapy• Wrist splints• Resting intrinsic plus splints• Skin care for trophic areas• Education
– Regular clinical reassessment• Advancing Tinel test for regeneration in zones of axonotmesis• Deep muscle pain for early sign of reinnervation

Timing of Surgery• Acute closed BPI <6/52
– CT myelography 3-6/52 post injury• Pseudomeningocoeles, myelomalacia and root avulsions
– Unequivocal total BPI (C5-T1 avulsion) • Explore 1-2/12
– All others repeated clinical assessment• Consider EMG and NCS at 6-8/52 • Planned exploration at 3/12 for grafting and nerve transfers
• Delayed presentation <6/12• Consider NCS /EMG / CT myelography• Explore for neurolysis, grafting and nerve transfers
• Delayed presentation >6/12• Consider NCS /EMG / CT myelography• Consider selective distal neurotisations , arthrodeses, tendon transfers and
functioning free muscle transfers

Reconstruction Priorities
• Shoulder and elbow control to enable positioning of a sensate hand for prehension– Shoulder abduction SSN (AxN)– Elbow flexion MCN– Sensate hand (MN / lateral cord)– Finger flexion (MN)– Elbow extension (RN)– Release (RN / PIN)– (Intrinsic function)

Reconstruction Priorities
• Shoulder and elbow control to enable positioning of a sensate hand for prehension– Shoulder abduction SSN (AxN)– Elbow flexion MCN– Sensate hand (MN / lateral cord)– Finger flexion (MN)– Elbow extension (RN)– Release (RN / PIN)– (Intrinsic function)

Reconstruction Ladder in BPI• Neurolysis
• External / internal• Nerve grafts
• Sural, LCNF, MCNF• Plexo-plexal (anatomic)
• Neurotisation • Reinnervation of a denervated motor or sensory end organ• Extraplexal donors for specific functions
• Nerve transfers• Ipselateral C7 or contralateral hemi C7 transfer to median nerve using a
vascularised ulnar nerve graft (in cases of preganglionic C8/T1 lesions) based on superior ulnar collateral vessels
• Arthrodeses• Osteotomies• Tendon transfers• Amputations• Functioning Free Muscle Transfers

Evolution of modern techniques 1• Early exploration <6/52
• Haemorrhage is often problematic• Potential for early recovery of neuropraxic injury• Unreliable intra-operative nerve stimulation
• Poor historical results of late exploration (>6/12) • Distal reinnervation is unsatisfactory
• Long grafts• End plate response diminishes with time
• Move towards earlier exploration in closed injuries (6/52-3/12)– Referrals are often delayed
• Associated injuries (eg IPPV for HI)• BPI is frequently missed • Trauma surgeon education• Supra-regional referrals

Evolution of modern techniques 2• Neurotise rather than plexo-plexal grafting
– “One nerve, one function”– Uncertain condition of root (SSEPs poor predictors)– Co-contraction of reinnervated antagonists
• Importance of reinnervation of the deltoid– Leechavenvongs: Long Head Triceps to anterior axillary nerve
• Distally based transfers more rapid and reliable recovery– Oberlin 1 and Oberlin 2 transfers for elbow flexion– FCR, PL, redundant FDS branches to ECRB, PIN and PT
• Avoid grafts– Longer reinnervation times and less predictable outcomes
• End to side techniques (“Something for nothing”)• FFM transfer when >6/12 since injury
– Muscle reinnervation MRC 3+ not possible after 12/12• Contralateral C7 to provide sensation
– Hemi C7 transfer minimises donor morbidity– Poor motor reinnervation, reasonable sensory to median nerve
• Selective use of osteotomies, arthrodeses, tendon and muscle transfers

Selective neurotisation: Phrenic to SSN

Selective neurotisation: XI to SSN

Selective neurotisation: XI to MCN

Selective neurotisation: ICNs to MCN

Leechavengvongs: Triceps branch to axillary transfer

Leechavengvongs: Triceps branch to axillary transfer

Oberlin 1: Selective distal neurotisation for elbow flexion

Oberlin 1 and 2: Selective distal neurotisations for elbow flexion

Oberlin 1 and 2: Selective distal neurotisations for elbow flexion

Doi: Functioning free gracilis for elbow flexion and finger extension

Contralateral Hemi C7 Transfer

Osteotomy
• TBPI• Some C5/6/7 recovery• No wrist extension• Supinated forearm• Poor cosmesis and
function

Osteotomy
• TBPI• Some C5/6/7 recovery• No wrist extension• Supinated forearm• Poor cosmesis and
function

Osteotomy
• Plan– Derotation osteotomy of
forearm– Wrist fusion– Wrist flexor to digital
extensor transfer

Arthrodeses
• Glenohumeral fusion• Wrist fusion• CMCJ fusion to thumb

Glenohumeral Arthrodesis 1
• TBPI post XI to SSN and ICNs to MCN
• Poor shoulder recovery• GHJ instability with
“pistoning” with elbow flexion
• Shoulder internal rotation with elbow flexion

Glenohumeral Arthrodesis 2

Glenohumeral Arthrodesis 3

Glenohumeral Arthrodesis 4
• GHJ plate fusion • 30-30-30 positioning

Tendon and Muscle Transfers
• Trapezius to greater tuberosity• Latissimus dorsi to infraspinatus• Latissimus dorsi to Biceps• Pectoralis major rotationplasty to Biceps• Steindler flexorplasty for assisted elbow flexion• Pedicled Latissimus dorsi to finger flexors

Pectoralis to Biceps 1

Amputation: Scapulothoracic dissociation

Additional Procedures
• Weak elbow flexion– If co-contraction biceps and triceps consider triceps to
biceps transfer– If weak post Oberlin consider Steindler flexorplasty
• Supination deformity after Biceps reinnervation– Derotation forearm osteotomy
• Weak finger extension– Wrist arthrodesis and wrist flexor to finger extensor
transfers

Prognosis in BPI
• Improved if young (<30 years)• Distal injuries do better (“Time Distance”)• Incomplete motor loss suggests a focal injury – Some neuropraxia likely
• Partial plexus injury better than flaccid paralysis of whole arm
• Pre-ganglionic signs do worse• Associated vascular injuries do worse

Research Areas in BPI• Surgical– Re-plantation of pre-ganglionic avulsions to the CNS
• May reduce brachialgia– (Sciatic conduit to conus medullaris has been used to re-
innervate glutei in paraplegics)• Molecular– Neural transmitters– Nerve growth factors– Neural tubes and neurotropism (Lundborg)
• Rehabilitation– Sensory re-education– Neural plasticity– “Acoustic glove” Lundborg (Sweden)

Case1: Preganglionic C5/C6
• Phrenic to MCN• XI to SSN

Case1: Preganglionic C5/C6
• Phrenic to MCN• XI to SSN• Shoulder abduction 70• Biceps MRC 4• Returned to work as a
soldier

Case1: Preganglionic C5/C6
• Phrenic to MCN• XI to SSN• Shoulder abduction 70• Biceps MRC 4• Returned to work as a
soldier• But scapular winging
due to long thoracic palsy

Case 2: C5-T1 Avulsions
• Poor results of shoulder & elbow neurotisations
• >6/12 at presentation

Pediatric Brachial Plexus Palsy• Incidence 0.38 to 1.56 per 1000 LB• Perinatal risk factors:
- Macrosomia- Maternal diabetes- Multiparous pregnancy- Previous deliveries resulting in PBPP- Prolonged labor- Breech delivery- Shoulder dystocia- Assisted and difficult deliveries

Pattern
• Most commonly involves the upper trunk (C5/6)• Rarest is insolated lower trunk• Upper trunk Extra-foraminal most common with
vertex delivery and shoulder dystocia• Right upper limb involved most often because of most
common LOA position in vertex delivery• C5-6 root avulsions most common with Breech
delivery and at times bilateral• Mecahnical cause most common

Diagnosis• Clinical diagnosis most
important• Horner’s syndrome bad
prognostic sign• Serial examinations over
the first few weeks to months
• Observation of spontaneous movements, neonatal reflexes, motor stimulation

Naraka’s Classification
• I Classic Erb’s palsy. 46% cases. Successful spontaneous recovery in 90%
• II Extended upper trunk (C5-7). Waiter’s tip. 29% cases
• III Flail Extremity without Horner’s syndrome• IV Flail Extremity with Horner’s syndrome. May
have associated phrenic nerve palsy and elevated hemi-diaphragm. Limited spontaneous recovery

Prognostic Indicators
• Infants who recover anti-gravity biceps strength by 2-3 months have a complete recovery in 1-2 years
• Infants who do not recover antigravity biceps strength by 5-6 months should undergo micro-surgical reconstruction
• Infants with partial recovery of C5-7 anti-gravity strength will have permanent progressive limitations requiring extensive rehab and salvage surgery