Trauma Overview Avery B. Nathens MD PhD MPH Division of General Surgery & Trauma St. Michael’s...
110
Trauma Overview Trauma Overview Avery B. Nathens MD PhD Avery B. Nathens MD PhD MPH MPH Division of General Division of General Surgery & Trauma Surgery & Trauma St. Michael’s Hospital St. Michael’s Hospital
-
Upload
abraham-hampton -
Category
Documents
-
view
222 -
download
5
Transcript of Trauma Overview Avery B. Nathens MD PhD MPH Division of General Surgery & Trauma St. Michael’s...

Trauma OverviewTrauma Overview
Avery B. Nathens MD PhD Avery B. Nathens MD PhD MPHMPH
Division of General Surgery Division of General Surgery & Trauma& Trauma
St. Michael’s HospitalSt. Michael’s Hospital

ObjectivesObjectives
Trauma epidemiologyTrauma epidemiology Prehospital carePrehospital care TriageTriage Long term outcomes after Long term outcomes after
injuryinjury

Trauma Trauma EpidemiologyEpidemiology

The Burden of InjuryThe Burden of Injury
Leading cause of death in first 4 decades of Leading cause of death in first 4 decades of lifelife
Third leading cause in all age groupsThird leading cause in all age groups 12% of hospital beds are consumed by injury12% of hospital beds are consumed by injury

0%
2%
4%
6%
8%
10%
12%
1984 1988 1992 1996 2000 2004
Trauma Mortality: 1985-Trauma Mortality: 1985-20032003

Injury mortality rateInjury mortality rate
40
45
50
55
60
65
70
80 82 84 86 88 90 92 94 96 98
Dea
ths
per
100
k p
op
'n
http://www.cdc.gov/ncipc/wisqars/
US, 1998: 53 per 100 000 pop’n

The Burden of InjuryThe Burden of Injury
Nearly ½ of all traumatic incidents Nearly ½ of all traumatic incidents involve the use of alcohol, drugs or involve the use of alcohol, drugs or other substance abuseother substance abuse
60% of all injuries are preventable60% of all injuries are preventable Is predominantly a disease of the Is predominantly a disease of the
young and carries potential for young and carries potential for permanent disabilitypermanent disability

Years of Potential Life Years of Potential Life Lost (YPLL) Before Age Lost (YPLL) Before Age
65 65
0 2 4 6 8 10 12
All Causes
Injury
Cancer
Heart Disease
Perinatal Period
Congenital
HIV
Cerebrovascular
Liver Disease
All Others
http://www.cdc.gov/ncipc/wisqars/
23%
2%
2%
3%
4%
8%
12%
17%
29%
100%

Number of Patients by Age
0
5,000
10,000
15,000
20,000
25,000
30,000
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101 106
Age (years)
Nu
mb
er o
f P
atie
nts
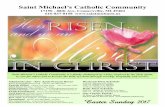
Distribution of injury by Distribution of injury by ageage

Figure 8A
Proportional distribution of patients, grouped by mechanism of injury.
Patients by Mechanism of Injury
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
500,000
Mechanism of Injury
Nu
mb
er o
f P
atie
nts
Motor vehicle traffic
Fall
Struck by, against
Firearm
Transport, other
Cut/pierce
Fire /burn
Pedal cyclis t, other
Other specified andclassifiableMachinery
Mechanism of injuryMechanism of injury

Mechanism of Injury by Age
02,0004,0006,0008,000
10,00012,00014,00016,000
1 8 15 22 29 36 43 50 57 64 71 78 85 92 99 106
Age (years)
Nu
mb
er o
f P
atie
nts Motor Vehicle Traffic
Fall
Struck by
Firearm
Transport, other
Mechanism of injury by Mechanism of injury by ageage

Deaths by Mechanism of Injury
0
5,000
10,000
15,000
20,000
25,000
Mechanism of Injury
Nu
mb
er o
f P
atie
nts
Motor vehicle traffic
Fall
Struck by, against
Firearm
Transport, other
Cut/pierce
Fire/burn
Pedal cyclist, other
Other specified andclassifiableMachinery
Deaths by mechanism of Deaths by mechanism of injuryinjury

Case Fatality by Age
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
Age (years)
Cas
e F
atal
itie
s (%
)
Mortality as a function of Mortality as a function of ageage

Abbreviated Injury Scale (AIS) Abbreviated Injury Scale (AIS) 6 body regions (head, neck, chest, abdomen, 6 body regions (head, neck, chest, abdomen,
pelvis, external)pelvis, external) Each injury coded from 1 to 6Each injury coded from 1 to 6 AIS>=3 is severeAIS>=3 is severe
Injury Severity Score (ISS)Injury Severity Score (ISS) Most common means of classifying injury Most common means of classifying injury
severityseverity Ranges from 1 to 75Ranges from 1 to 75 ISS>=16 – severe multisystem traumaISS>=16 – severe multisystem trauma
Grading Injury SeverityGrading Injury Severity

INJURY SEVERITY SCORE INJURY SEVERITY SCORE ExampleExample
Abbreviated Abbreviated Injury ScaleInjury Scale
Small subdural haematomaSmall subdural haematoma 44
Parietal lobe swellingParietal lobe swelling 33
Major liver lacerationMajor liver laceration 44
Upper tibial fracture (displaced)Upper tibial fracture (displaced) 33
ISS = 4ISS = 42 + 2 + 442 + 2 + 332 2 = 41= 41

Percentage of Patients and Injury Severity Score (ISS)
0
10
20
30
40
50
60
70
Per
cen
tag
e o
f P
atie
nts
ISS 1 - 9
ISS 10 - 15
ISS16 - 24
ISS > 24
Unknown
Injury severityInjury severity

Case Fatality by Injury Severity Score (ISS)
0
5
10
15
20
25
30
35
Injury Severity Score
Cas
e F
atal
ity
(%) ISS 1 - 9
ISS 10 - 15
ISS 16 - 24
> 24
Unknown
Mortality as a function of Mortality as a function of ISSISS

Unintentional Motor Vehicle Traffic Related Injuries
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
1 8 15 22 29 36 43 50 57 64 71 78 85 92 99
Age (years)
Nu
mb
er
of
Pa
tie
nts Occupant
Motorcyclist
Pedestrian
Pedal Cyclist
Unspecified

American College of Surgeons National Trauma Data Bank ® 2006. Version 6.0
© American College of Surgeons 2006. All Rights Reserved Worldwide
Figure 26A
Proportional distribution of patients, grouped by intent.
Patients by Intent
Unintentional
Assault
Se lf-inflicted
Undeterm ined
Other

American College of Surgeons National Trauma Data Bank ® 2006. Version 6.0
© American College of Surgeons 2006. All Rights Reserved Worldwide
Figure 27A
Proportional distribution of deaths, grouped by intent. Total N = 48,149.
Deaths by Intent
Self-inflicted
Undeterm ined
Other
Assault
Unintentional

Geographic variations in Geographic variations in MVC-mortality: MVC-mortality: Baker et al, Baker et al,
19871987MVC mortality (per 100 000 persons)
2.5
558
Population density (persons/sq mile)
64000
0.2
Esmerelda, NV versus Manhattan, NY

Trimodal Distribution of Trimodal Distribution of Trauma DeathsTrauma Deaths

Epidemiology of Trauma Epidemiology of Trauma DeathsDeaths
*Sauaia et al, J Trauma, 1995
AcuteAcute
( <48 ( <48 hrs)hrs)
EarlyEarly
(48 hr to (48 hr to 7d)7d)
LateLate
(> 7 d)(> 7 d)
CNS CNS injuryinjury
40%40% 64%64% 39%39%
Blood Blood lossloss
55%55% 9%9% 0%0%
MOFSMOFS 1%1% 18%18% 61%61%

Prehospital carePrehospital care

Clinical scenarioClinical scenario
64 yo female running for bus64 yo female running for bus Leg catches on bumperLeg catches on bumper Dragged 20 feetDragged 20 feet
Unconscious with occasional respiratory effortsUnconscious with occasional respiratory efforts Systolic blood pressure – 80Systolic blood pressure – 80 Heart rate 140Heart rate 140 45 minutes from trauma center45 minutes from trauma center

Clinical scenarioClinical scenario

American Civil War: 1861Mortality: 25%Transport time: 72 hrsFactors: +/- ambulance
WW I: 1914Mortality: 8.6%Transport time: 8 hrsFactors: ambulance (motorized)

World War II: 1939 Mortality: 4.5%Transport time: 4 hrsFactors: Ambulance, Medics, Plasma, Antibiotics

Korean War: 1951Mortality: 2.5%Transport time: 1.25 hrsFactors: Helicopter, MASH

Viet Nam War: 1965-1972Mortality 1.9%Transport time: 27 minutesFactors: Helicopter, Medics, Fixed wing

circa 1947

Prehospital transport Prehospital transport timestimes
UrbanUrban Houston - 32.6 minutesHouston - 32.6 minutes Portland ~ 25 minPortland ~ 25 min Chicago - 35 minutesChicago - 35 minutes Tucson - 21 minTucson - 21 min
RuralRural Georgia - 42 minGeorgia - 42 min Northern California - 55 minNorthern California - 55 min WA (Okanogan County) - 49 minWA (Okanogan County) - 49 min
Definitive Care
Any Hospital

Controversies in Controversies in Prehospital Trauma Prehospital Trauma
CareCareALS vs BLS ALS vs BLS Airway managementAirway managementFluid resuscitationFluid resuscitation

ALS vs BLS “packages”ALS vs BLS “packages”
Basic life supportBasic life support Splinting, spine immobilization, Splinting, spine immobilization,
hemorrhage controlhemorrhage control Advanced life supportAdvanced life support
Establish a definitive airwayEstablish a definitive airway Provide intravenous accessProvide intravenous access Administer pharmacologic agentsAdminister pharmacologic agents
““Load and go” or “stay and play”?Load and go” or “stay and play”?

Stay and Play:Stay and Play:Pre-hospital care - SAMUPre-hospital care - SAMU
French EMS - SAMU French EMS - SAMU (Service d'Aide Médicale (Service d'Aide Médicale Urgente)Urgente)
Physicians attend to Physicians attend to patient at scenepatient at scene Stabilize at scene, en Stabilize at scene, en
routeroute Identify receiving centerIdentify receiving center

Stay and PlayStay and Play
August 31, 1997August 31, 1997 Mercedes S-280 - 122 mphMercedes S-280 - 122 mph
4 occupants, 2 dead at scene 4 occupants, 2 dead at scene with torn aortaswith torn aortas
SAMU dispatch: 00:26SAMU dispatch: 00:26 SAMU scene arrival: 00:32SAMU scene arrival: 00:32 Extrication complete: 01:00Extrication complete: 01:00 ER arrival, Pitie Salpetriere ER arrival, Pitie Salpetriere
hospital 02:06hospital 02:06 Pronounced dead - 04:30Pronounced dead - 04:30

ALS vs BLS “packages”ALS vs BLS “packages”
No prospective RCT documenting No prospective RCT documenting the effectiveness of ALS in traumathe effectiveness of ALS in trauma
...yet ALS available in 98.5% of the ...yet ALS available in 98.5% of the 200 largest US cities200 largest US cities

ALS vs BLS in trauma: a meta-ALS vs BLS in trauma: a meta-analysisanalysis
Liberman et al, J Trauma, 2000Liberman et al, J Trauma, 2000 Included 15 studies (of 174 pertaining to Included 15 studies (of 174 pertaining to
trauma) that had sufficient data for trauma) that had sufficient data for analysisanalysis
Scene timesScene times ALS: 18.5 minALS: 18.5 min BLS: 13.5 minBLS: 13.5 min

ALS vs BLS in trauma: a meta-ALS vs BLS in trauma: a meta-analysisanalysis
0 1 2 3 4 5 6 7 8 9 10
Winchell, 97
Sampalis, 92
Potter, 88
Cayten, 86
Bickell, 94
Martin, 92
Cayten, 93
Murphy, 93
Cayten, 84
Aprahamian, 83
Ivaturi, 87
Clevenger, 88
Sampalis, 97
Demetriades, 96
Odds of death (ALS vs BLS)
Risk of death ~3 X greater

Multicenter Canadian Multicenter Canadian Study 2003Study 2003
Montreal: MD-ALS; Toronto:PM-ALS;Montreal: MD-ALS; Toronto:PM-ALS; Quebec: EMT-BLSQuebec: EMT-BLS 50% trauma patients in ALS communities 50% trauma patients in ALS communities
had ALS personnel present.had ALS personnel present. Prospective, observational study, Prospective, observational study,
n=9405n=9405 Increased mortality and scene time in Increased mortality and scene time in
MD-ALS group, No difference in MD-ALS group, No difference in mortality for PM-ALS and EMT-BLSmortality for PM-ALS and EMT-BLS
Liberman et al, Annals of Surgery, 2003

Multicenter Canadian Multicenter Canadian Study 2003Study 2003
Conclusion: In urban centers with highly specialized level 1 trauma centers, there is no benefit in having on-site ALS for the prehospital management of trauma patients

Airway Management Airway Management OptionsOptions
Mask ventilationMask ventilation Oral intubationOral intubation Nasal intubationNasal intubation Use of paralytic agentsUse of paralytic agents Surgical airway accessSurgical airway access
Needle Needle cricothyrotomycricothyrotomy
Open cricothyrotomyOpen cricothyrotomyRetrograde Retrograde intubationintubation

Intubation vs. Mask Intubation vs. Mask VentilationVentilation
Gausche et al, JAMA 2000Gausche et al, JAMA 2000 Questions the role of prehospital intubation for Questions the role of prehospital intubation for
pediatric patientspediatric patients 830 pts < age 12 randomized to ETI vs BVM830 pts < age 12 randomized to ETI vs BVM No difference in mortality or neurologic No difference in mortality or neurologic
outcome between the groupsoutcome between the groups Intubation success rate 57%, 14% tubes Intubation success rate 57%, 14% tubes
dislodged, 2% esophageal intubationdislodged, 2% esophageal intubation LimitationsLimitations
No paralytic agentsNo paralytic agents Inexperience paramedicsInexperience paramedics

Oral intubation success Oral intubation success ratesrates
Range 75 to 98% dependent on indications Range 75 to 98% dependent on indications and availability of paralytic agentsand availability of paralytic agents
BEST DATABEST DATA Hedges et al: Thurston County, WA 1983-84: Hedges et al: Thurston County, WA 1983-84:
96%96% Bulger et al: Seattle Fire Dept 1997-1999: 98.4%Bulger et al: Seattle Fire Dept 1997-1999: 98.4% Wayne et al: Bellingham/Whatcom County WA Wayne et al: Bellingham/Whatcom County WA
1999: 95.5%1999: 95.5% WORST DATAWORST DATA
Katz et al: Orlando, FL 1997: 25% of ET tubes Katz et al: Orlando, FL 1997: 25% of ET tubes were malpositioned, 37% for trauma patientswere malpositioned, 37% for trauma patients

Head InjuryHead Injury
Winchell, San Diego, 1997 Winchell, San Diego, 1997 Patients with severe head injury: mortality Patients with severe head injury: mortality
decreased from 57% to 36% with decreased from 57% to 36% with intubationintubation
Murray et al, Los Angeles CA, 2000:Murray et al, Los Angeles CA, 2000: Mortality 70% higher in patients with Mortality 70% higher in patients with
severe head injurysevere head injury Davis et al, San Diego, CA 2003:Davis et al, San Diego, CA 2003:
Trial of RSI for head injured patientsTrial of RSI for head injured patients Increased mortality for intubated patients: 33% Increased mortality for intubated patients: 33%
vs 24%vs 24%

Head InjuryHead Injury
Study design and applicability are Study design and applicability are problematicproblematic Retrospective designRetrospective design
Paralytics not allowed in many protocolsParalytics not allowed in many protocols Only the apneic and most unresponsive are intubated Only the apneic and most unresponsive are intubated
– worse prognosis– worse prognosis
In the study where RSI was usedIn the study where RSI was used Significant hyperventilation may have worsened Significant hyperventilation may have worsened
outcomeoutcome Increased pre-hospital timeIncreased pre-hospital time Poor matching (No GCS available in controls)Poor matching (No GCS available in controls)

Penetrating injuryPenetrating injury
Bickell et al, 1994Bickell et al, 1994 Randomized 598 patients with shock following Randomized 598 patients with shock following
penetrating truncal injury in urban Houston: penetrating truncal injury in urban Houston: Immediate fluid resuscitationImmediate fluid resuscitation Delayed fluid resuscitation – postponed until Delayed fluid resuscitation – postponed until
operative interventionoperative intervention Transport times<30 minutesTransport times<30 minutes Fluid administrationFluid administration
Immediate group – 2500 cc’s preoperatively (2/3rd of Immediate group – 2500 cc’s preoperatively (2/3rd of the fluid was given in the ER) the fluid was given in the ER)
Delayed group – 280 cc’s preoperativelyDelayed group – 280 cc’s preoperatively

ResultsResults
Delayed groupDelayed group Slightly improved survival – 62% vs Slightly improved survival – 62% vs
70%70% Shorter hospital LOSShorter hospital LOS Fewer complicationsFewer complications
CaveatsCaveats Young patientsYoung patients Short transport timesShort transport times Penetrating injuryPenetrating injury

High speed High speed rolloverrollover
35 yo 35 yo restrained restrained driverdriver

Epigastric Epigastric stab stab woundwound
StableStable

50 yo male50 yo male Had been drinkingHad been drinking Falls down flight of Falls down flight of
stairsstairs Transient LOCTransient LOC Now awake, alert, Now awake, alert,
GCS 15GCS 15

Triage of the Triage of the Major Trauma Major Trauma
PatientPatient

Triage: Triage: the sorting out and the sorting out and classification of casualties of war or classification of casualties of war or other disaster, to determine priority other disaster, to determine priority of need and proper place of treatmentof need and proper place of treatment
“Get the right patient to the right place at the right time”

A tale of two countiesA tale of two countiesWest & Trunkey, 1979West & Trunkey, 1979
Orange CountyOrange County Trauma patients transported to Trauma patients transported to
nearest of 39 facilitiesnearest of 39 facilities
San Francisco CountySan Francisco County Trauma patients transported to 1 Trauma patients transported to 1
centrally located trauma facilitycentrally located trauma facility
Preventable deaths: 43%
Preventable deaths: 1%

National Evaluation of the National Evaluation of the Effect of Trauma Center Care Effect of Trauma Center Care
on Mortalityon MortalityN Engl J Med, 2006N Engl J Med, 2006
25% lower risk of death at one year in trauma centers
0
2
4
6
8
10
12
14
In hospital 30 d 90 d 365 d
Time from injury
Mor
talit
y (%
)
NTCTC
N=15,000 patients


Ideal TriageIdeal Triage
Direct patients with serious injuries Direct patients with serious injuries to centers with available resources to centers with available resources and personneland personnel
Direct those with less serious Direct those with less serious injuries to all other centers within injuries to all other centers within same geographic areasame geographic area

Field triage goals – a Field triage goals – a balancebalance
Undertriage – major trauma patient Undertriage – major trauma patient triaged to center with inadequate triaged to center with inadequate resourcesresources Patient incurs riskPatient incurs risk
Overtriage – minimally injured trauma Overtriage – minimally injured trauma patient triaged to regional trauma patient triaged to regional trauma centercenter System incurs riskSystem incurs risk
Utilization of limited material, financial and Utilization of limited material, financial and human resourceshuman resources
Inconveniences family/patientInconveniences family/patient

Field Triage Tools - Field Triage Tools - OverviewOverview
Physiologic criteriaPhysiologic criteria
Anatomic criteriaAnatomic criteria
Mechanism of injuryMechanism of injury
ModifiersModifiers

Physiologic criteria - ACS Physiologic criteria - ACS field triagefield triage
GCS<14GCS<14 SBP<90SBP<90 RR<10 or >29RR<10 or >29
ProsPros Objective, Objective,
quantifiablequantifiable Easily assessedEasily assessed Predictive of deathPredictive of death
ConsCons Time dependentTime dependent

Anatomic criteria - ACS Anatomic criteria - ACS field triagefield triage
Penetrating injury Penetrating injury proximal to elbow or kneeproximal to elbow or knee
Flail ChestFlail Chest Trauma with burnsTrauma with burns >>2 proximal long-bone #2 proximal long-bone # Pelvic #Pelvic # Open & depressed skull Open & depressed skull
## ParalysisParalysis Amputation proximal to Amputation proximal to
wrist or anklewrist or ankle Major burnsMajor burns
ProsPros Accurate if injury obviousAccurate if injury obvious
ConsCons Physical exam not Physical exam not
predictive of injuriespredictive of injuries Time consuming examTime consuming exam

Mechanism of injury - Mechanism of injury - ACS field triageACS field triage
Falls >20 ftFalls >20 ft High risk crashHigh risk crash
EjectionEjection Death in same Death in same
compartmentcompartment Intrusion > 12 in Intrusion > 12 in
occupant compartmentoccupant compartment Intrusion > 18 in Intrusion > 18 in
anywhereanywhere Auto-pedestrian/cyclist Auto-pedestrian/cyclist
>20 mph>20 mph MCC > 20mphMCC > 20mph
ProsPros Estimate of type, Estimate of type,
amount, direction of amount, direction of force appliedforce applied
Readily assessed by Readily assessed by EMS personnelEMS personnel
ConsCons Estimate of potential, Estimate of potential,
not actual injurynot actual injury Limited value when Limited value when
used aloneused alone

Modifiers: permissive Modifiers: permissive criteria -criteria -
ACS field triageACS field triage Age <5 or >55Age <5 or >55 AnticoagulationAnticoagulation BurnsBurns PregnancyPregnancy
ProsPros Good predictor of Good predictor of
adverse outcomesadverse outcomes
ConsCons Cannot be ascertained Cannot be ascertained
in fieldin field UnderutilizedUnderutilized

Mechanism
Transport to highest level of trauma care available: alert trauma team
Field Triage Decision Scheme:Field Triage Decision Scheme:ACS COT, Resources for ACS COT, Resources for
Optimal Care, 2007Optimal Care, 2007Physiologic
criteria
Anatomic criteria
Consider transport to a trauma center
Modifiers(Permissive)

Predictors of undertriagePredictors of undertriage
Advanced age - single most important Advanced age - single most important predictor of undertriagepredictor of undertriage Zimmer-Gembeck, J Trauma, 1995Zimmer-Gembeck, J Trauma, 1995

Toronto Field Trauma Toronto Field Trauma Triage GuidelinesTriage Guidelines
Directs injured patients to trauma Directs injured patients to trauma centrescentres
CriteriaCriteria PhysiologicPhysiologic AnatomicAnatomic MechanismMechanism

Toronto Field Trauma Toronto Field Trauma Triage Guidelines: Triage Guidelines: Physiologic criteriaPhysiologic criteria
GCS<=10 GCS<=10 OROR Two or more ofTwo or more of
AnyAny alteration in level of consciousness. alteration in level of consciousness. A pulse rate less than 50 or more than A pulse rate less than 50 or more than
120.120. A blood pressure less than 80 or an A blood pressure less than 80 or an
absent radial pulseabsent radial pulse A respiratory rate less than 10 or greater A respiratory rate less than 10 or greater
than 24than 24

Toronto Field Trauma Toronto Field Trauma Triage GuidelinesTriage Guidelines
AnatomicAnatomic Spinal Cord injury with paraplegia or Spinal Cord injury with paraplegia or
quadriplegia.quadriplegia. Penetrating injury to head, neck, trunk or Penetrating injury to head, neck, trunk or
groin, ORgroin, OR Amputation above the wrist or ankleAmputation above the wrist or ankle

Toronto Field Triage Toronto Field Triage CriteriaCriteria
Diversion to closest Diversion to closest hospitalhospital Divert if anticipate won’t surviveDivert if anticipate won’t survive
Complete airway obstructionComplete airway obstruction Absence of spontaneous respirationsAbsence of spontaneous respirations Absence of a palpable carotid pulseAbsence of a palpable carotid pulse
Estimated transport time>30 minutesEstimated transport time>30 minutes


Organized Systems of Organized Systems of Trauma CareTrauma Care
Trauma Center•Most severely injured
Rehabilitation
Interfacility
Transfer
Non-Trauma Center•Other injured persons
Prehospital•Notification/EMS Access•EMS response•Triage•Transport
Ongoing•Prevention•Training•Evaluation




Effect of legislative Effect of legislative initiatives on MVC-initiatives on MVC-
mortalitymortalityNathens et al, JAMA, 2000Nathens et al, JAMA, 2000
LegislationLegislation Effect on crash mortalityEffect on crash mortality
Primary restraint lawsPrimary restraint laws 13% (11-16)13% (11-16)
State trauma systemState trauma system 9% (6-11)9% (6-11)
Secondary restraint lawsSecondary restraint laws 3% (0-5)3% (0-5)
65 mph (vs 55 mph) speed limit65 mph (vs 55 mph) speed limit
Administrative revocation lawsAdministrative revocation laws
7% (3-10)7% (3-10)
5% (3-7)5% (3-7)

Access time & trauma-Access time & trauma-mortality ratesmortality rates

3486 deaths
Field deaths54% (1882)
Reached hospital 46% (1604)
ED deaths 21% (732)
OR deaths4% (139)
Other in hospital22% (733)
ED 45%
OR 8%
Other 47%

Patient KLPatient KL 34 yo male truck 34 yo male truck
driver/moverdriver/mover High speed MVCHigh speed MVC
Mild traumatic brain injuryMild traumatic brain injury Liver laceration, splenectomyLiver laceration, splenectomy Bad pelvic fracture, femur Bad pelvic fracture, femur
fracturefracture Acetabular fractureAcetabular fracture
Angioembolization for Angioembolization for pelvic fracture bleedingpelvic fracture bleeding
ICU stay ~7 daysICU stay ~7 days

What will happen to KL What will happen to KL in 1 yearin 1 year
A) Working at full capacityA) Working at full capacityB) Desk jobB) Desk jobC) Not working, milling about the house on C) Not working, milling about the house on
disability compensation, driving his wife disability compensation, driving his wife crazycrazy
D) Not working, in chronic painD) Not working, in chronic painD) Nursing homeD) Nursing home

Why can’t he return to Why can’t he return to normal function normal function
A) Brain injuryA) Brain injury
B) Liver injury and lack of a spleenB) Liver injury and lack of a spleen
C) Acetabular/femur and pelvic C) Acetabular/femur and pelvic fracturefracture
D) Bad dreamsD) Bad dreams

What is his chance of re-What is his chance of re-injuryinjury
A) Less than the average person, he is A) Less than the average person, he is a more careful driver nowa more careful driver now
B) His injuries put him at slightly B) His injuries put him at slightly greater than average riskgreater than average risk
C) He is accident prone – he’ll likely C) He is accident prone – he’ll likely get himself into troubleget himself into trouble

Functional Outcomes Functional Outcomes After InjuryAfter Injury
Multisystem traumaMultisystem trauma
Specific injuriesSpecific injuries Traumatic brain injuryTraumatic brain injury Severe extremity injuriesSevere extremity injuries
Post traumatic stress Post traumatic stress disorder & functional disorder & functional outcomesoutcomes

Employment OutcomesEmployment Outcomes Brenneman, J Trauma, Brenneman, J Trauma,
19971997 N=195, ISS>10N=195, ISS>10
Sampling bias – too well and too sick excludedSampling bias – too well and too sick excluded 52% back at work at 1 year52% back at work at 1 year
Pre-injuryPre-injury % employed at 1 year% employed at 1 year
White collarWhite collar 8282
Blue collarBlue collar 4343

Employment & Financial Employment & Financial OutcomesOutcomes
Michaels, J Trauma, 2000 Michaels, J Trauma, 2000 Outcomes at 1 year (n=247)Outcomes at 1 year (n=247)
Excluded head injury, SCIExcluded head injury, SCI
EmploymentEmployment 64% had returned to work64% had returned to work 23% workers’ comp/disability23% workers’ comp/disability
FinancialFinancial 30% reported a decline income30% reported a decline income

Functional limitations & Functional limitations & DisabilityDisability
Enabling America: IOM, Enabling America: IOM, 19971997
Pathology
Osteoarthritis of the hip post acetabular
fracture
Impairment
Limited range of motion
Functional limitation
Unable to climb stairs
Disability
Cannot continue employ as mover

Functional limitations Functional limitations following multiple traumafollowing multiple trauma
Mackenzie, Qual Life Res, 2002Mackenzie, Qual Life Res, 2002 Prospective cohort study: n=1240, 1 yr Prospective cohort study: n=1240, 1 yr
follow upfollow up
Functional capacity index (FCI)Functional capacity index (FCI) Physical & cognitive function onlyPhysical & cognitive function only Focuses on tasks necessary for ADLFocuses on tasks necessary for ADL
Insensitive to socially defined roles “role Insensitive to socially defined roles “role performance”performance”
Less sensitive to personal/environmental influencesLess sensitive to personal/environmental influences Sensitive to specific medical interventionsSensitive to specific medical interventions

Limitation in functions by Limitation in functions by FCI dimensionFCI dimension
FCI FCI dimensiondimension
% with % with limitationlimitation
Bending/Bending/liftinglifting
6363
AmbulationAmbulation 6161
Cognitive Cognitive functionfunction
2727
Hand/arm Hand/arm functionfunction
2525
Sexual Sexual functionfunction
1818
FCI FCI dimensiondimension
% with % with limitationlimitation
VisionVision 1818
Excretory Excretory functionfunction
88
HearingHearing 55
EatingEating 44
SpeechSpeech 22

FCI & Return to WorkFCI & Return to Work
0%
5%
10%
15%
20%
25%
Pat
ien
ts (
%)
0-0.2 0.21-0.4 0.41-0.6 0.61-0.8 0.81-0.99
1
FCI
18% 65% 82%Return to work
Bad Good

Functional outcomes Functional outcomes following traumatic brain following traumatic brain
injuryinjury Dikmen, Arch Phys Med Rehabil, 2003Dikmen, Arch Phys Med Rehabil, 2003
N=261, 80% followup at 3-5 yearsN=261, 80% followup at 3-5 years Moderate to severe TBIModerate to severe TBI
Functional status examinationFunctional status examination Physical, social, psychologic assessmentPhysical, social, psychologic assessment

Functional Status in TBIFunctional Status in TBI Glasgow Outcome Scale Glasgow Outcome Scale
Moderate-severe disability in 24%Moderate-severe disability in 24%
Majority not institutionalized: 92%Majority not institutionalized: 92%
Return to work after injury: 84%Return to work after injury: 84% Only 58% still working by 3-5 yearsOnly 58% still working by 3-5 years
What percent are you “back to normal:” What percent are you “back to normal:” 80%80%

Functional Status in TBI: Functional Status in TBI: Partial/complete Partial/complete
dependencydependency
0 10 20 30 40 50 60
% of patients
Personal care
Ambulation
Standard of living
Home management
Travel
Financial independence
Cognitive competency
Social integration
Major activity
Leisure/recreation

Functional impact of Functional impact of Orthopedic InjuriesOrthopedic Injuries
Michaels, J Trauma, 2000Michaels, J Trauma, 2000
0
10
20
30
40
50
60
70
80
90
100
Phys fn
Role P
hys
Pain
Gen h
ealth
Vitalit
y
Social
funct
ioni
ng
Role e
motio
nal
Men
tal h
ealth
BaselineNon-orthopedicOrthopedic
Physical well being Mental well being

Functional impact of Orthopedic InjuriesFunctional impact of Orthopedic InjuriesMichaels, J Trauma, 2000Michaels, J Trauma, 2000
0
10
20
30
40
50
60
70
80
90
100
Phys fn
Role P
hysPai
n
Gen h
ealth
Vitalit
y
Social
funct
ionin
g
Role e
motio
nal
Men
tal h
ealth
BaselineNon-orthopedicOrthopedic
Physical well being Mental well beingPhysical well being Mental well being

Reconstruction or Reconstruction or amputation of limb amputation of limb
threatening injuries?threatening injuries?Bosse, NEJM, 2002Bosse, NEJM, 2002
Prospective cohort studyProspective cohort study 545 high energy trauma below the femur545 high energy trauma below the femur Baseline, 3, 6, 12, 24 mo assessmentBaseline, 3, 6, 12, 24 mo assessment 84% f/u at 24 mos84% f/u at 24 mos
Functional outcome measure: Sickness Functional outcome measure: Sickness Impact ProfileImpact Profile

Sickness Impact ProfileSickness Impact Profile
Measure of self reported health statusMeasure of self reported health status 12 categories of function12 categories of function 2 major dimensions: physical health, psychosocial 2 major dimensions: physical health, psychosocial
healthhealth
Score: 0-100Score: 0-100 Population norms: 2-3Population norms: 2-3 Differences of 2-3 are meaningfulDifferences of 2-3 are meaningful Severe disability: >10Severe disability: >10

Outcomes: Outcomes: Reconstruction vs Reconstruction vs
amputationamputation12 months12 months 24 months24 months
ReconstruReconstructct
AmputatAmputatee
ReconstruReconstructct
AmputaAmputatete
OverallOverall 1515 1414 1212 1313
PhysicalPhysical 1313 1212 1010 1010
PsychosociaPsychosociall
1212 1212 1010 1111
Work (%)Work (%) 4141 4242 3636 3939
• Amputation equivalent to reconstruction • Consider when determining care priorities in the critically ill injured patient

Factors associated with poor Factors associated with poor outcomeoutcome
Bosse, NEJM, 2002Bosse, NEJM, 2002
Low educational levelLow educational level NonwhiteNonwhite PovertyPoverty
Lack of private health Lack of private health insuranceinsurance
SmokingSmoking Disability Disability
compensation compensation litigationlitigation
Focus should be on non clinical interventions and psychosocial/vocational rehabilitation

Outcomes following Pelvic Outcomes following Pelvic FractureFracture
Wright, J Urol 2006Wright, J Urol 2006 Pelvic fractures associated with neurovascular and Pelvic fractures associated with neurovascular and
ligamentous injuryligamentous injury Impact on genitourinary, anorectal and sexual function Impact on genitourinary, anorectal and sexual function
never evaluatednever evaluated
Prospective cohort studyProspective cohort study 298 patients with pelvic fracture; 862 without298 patients with pelvic fracture; 862 without
Excluded patients with overt injuries known to Excluded patients with overt injuries known to impact on genitourinary, anorectal or sexual impact on genitourinary, anorectal or sexual dysfunctiondysfunction GU injuries Anorectal injuries Spinal cord injury with deficit

Outcomes following Pelvic Outcomes following Pelvic FractureFracture
Symphysis
Sacrum

Adjusted Risk of Male Adjusted Risk of Male Sexual & Excretory Sexual & Excretory
DysfunctionDysfunctionFracture configuration
Sexual dysfunctionRR (95% CI)
Excretory dysfunction
RR (95% CI)
Fracture involving the SI joints
3.6 (1.7-7.8) 2.4 (0.5-12.3)
Open pelvic fracture 2.0 (1.1-3.8) 4.6 (1.7-13)
Symphyseal fracture 1.2 (0.5-2.9) 4.3 (1.1-17)
Closed pelvic fracture 1.7 (0.4-6.9) 3.1 (0.4-23)

Adjusted Risk of Female Adjusted Risk of Female Sexual & Excretory Sexual & Excretory
DysfunctionDysfunctionSexual
dysfunctionRR (95% CI)
Excretory dysfunction
RR (95% CI)
Fracture involving the SI joints
0.6 (0.1-3.4)0.6 (0.1-3.4) 1.3 (0.2-6.6)1.3 (0.2-6.6)
Open pelvic fracture 0.8 (0.2-2.8)0.8 (0.2-2.8) N/AN/A
Symphyseal fracture 2.4 (0.6-8.7)2.4 (0.6-8.7) 6.2 (1.7-22)6.2 (1.7-22)
Closed pelvic fracture 1.3 (0.3-6.81.3 (0.3-6.8 N/AN/A

Post-Traumatic Stress Post-Traumatic Stress DisorderDisorder
PTSD symptomsPTSD symptoms Intrusive: flashbacks, memories, Intrusive: flashbacks, memories,
nightmaresnightmares Avoidant: emotional detachment, Avoidant: emotional detachment,
restricted emotion, avoidance of remindersrestricted emotion, avoidance of reminders Arousal: insomnia, irritability, vigilanceArousal: insomnia, irritability, vigilance
Common following traumatic injuryCommon following traumatic injury 10-40% of all patients admitted following 10-40% of all patients admitted following
injuryinjury

“The PTSD Demon”

Predictors of PTSDPredictors of PTSDZatzick, Am J Psych 2002Zatzick, Am J Psych 2002
Longitudinal study (1 year)Longitudinal study (1 year) PTSD in 30-40% at 1, 4, or 12 mo post injuryPTSD in 30-40% at 1, 4, or 12 mo post injury
PredictorsPredictors PTSD symptoms at baselinePTSD symptoms at baseline Greater prior traumaGreater prior trauma +ve toxicology screen for stimulants+ve toxicology screen for stimulants FemaleFemale
Notable negatives Notable negatives Injury severity or type, pre-event functioning, Injury severity or type, pre-event functioning,
income, educationincome, education

0102030405060708090
Physic
al fn
Role p
hysic
al
Role e
motio
nalPai
n
Gener
al h
ealth
Vitalit
y
Social
fn
Men
tal h
ealth
No PTSD PTSD
PTSD & Functional PTSD & Functional outcomesoutcomes
Zatzick, Arch Surg, 2002Zatzick, Arch Surg, 2002PTSD : strongest predictor of poor functional outcome
Physical well being Mental well being

Screening and Intervention Screening and Intervention for PTSDfor PTSD
Zatzick et al, Arch Gen Zatzick et al, Arch Gen Psychiatry, 2004Psychiatry, 2004
10
15
20
25
30
35
0 1 3 6 12Time (months)
% P
TS
D
Control
Intervention

National Evaluation of the National Evaluation of the Effect of Trauma Center Care Effect of Trauma Center Care
on Mortalityon MortalityN Engl J Med, 2006N Engl J Med, 2006
25% lower risk of death at one year in trauma centers
0
2
4
6
8
10
12
14
In hospital 30 d 90 d 365 d
Time from injury
Mor
talit
y (%
)
N=15,000 patients
No real difference in functional outcome

Injury RecividismInjury RecividismWorrel & Nathens, J Trauma, Worrel & Nathens, J Trauma,
20062006
Increasing ageMaleAlcohol abuse

SummarySummary Mortality is the tip of the icebergMortality is the tip of the iceberg
Gross underestimate of the personal and Gross underestimate of the personal and societal burden of injurysocietal burden of injury Only 50% employed at 1 yearOnly 50% employed at 1 year
Functional limitations dominated by Functional limitations dominated by orthopedic and head injuriesorthopedic and head injuries
PTSDPTSD Likely a major contributor to adverse functional Likely a major contributor to adverse functional
outcomesoutcomes

Where should efforts be Where should efforts be directed?directed?
Vocational & psychosocial Vocational & psychosocial rehabilitationrehabilitation
Screening and intervention for PTSDScreening and intervention for PTSD
Prevention of recurrent injuryPrevention of recurrent injury Brief interventions for alcohol abuseBrief interventions for alcohol abuse