Trauma Healing Initiative: Cambodia Building a culturally appropriate healing network Carol White...
29
Trauma Healing Initiative: Cambodia Building a culturally appropriate healing network Carol White The Center for Victims of Torture Oct. 31, 2007
-
Upload
valerie-jarry -
Category
Documents
-
view
225 -
download
2
Transcript of Trauma Healing Initiative: Cambodia Building a culturally appropriate healing network Carol White...

Trauma Healing Initiative: Cambodia
Building a culturally appropriate healing
network
Carol WhiteThe Center for Victims of Torture
Oct. 31, 2007

Project charge
To address the high levels of trauma in Cambodia
Poverty
Domestic violence
Community violence and exploitation
Depression, alcohol abuse, PTSD

What model to choose?
• Direct services with a training component?
• Training community mental health workers?
• Professional education?
• Support a torture treatment/human rights organization?
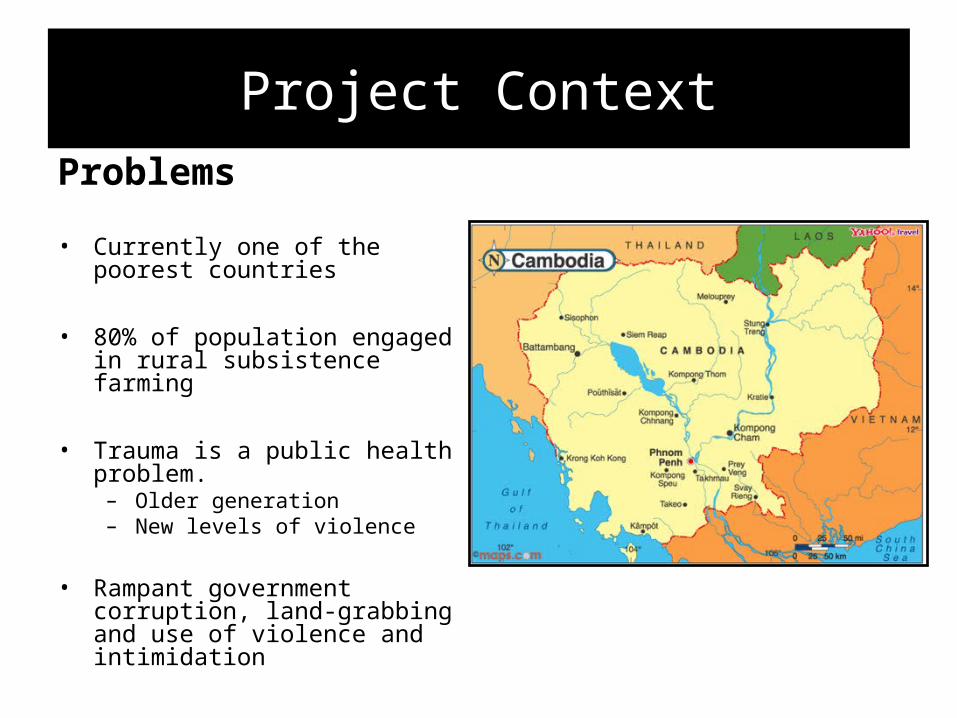
Project ContextProblems
• Currently one of the poorest countries
• 80% of population engaged in rural subsistence farming
• Trauma is a public health problem.– Older generation– New levels of violence
• Rampant government corruption, land-grabbing and use of violence and intimidation

Project Context
Assets• At peace for over 15 years
• Active civil society and many NGOs
• Rapid economic growth • Strong family systems
• A budding mental health infrastructure

A culture of impunity• No legitimate war crimes
trials have been held since Pol Pot times
• No truth and reconciliation process
• Former Khmer Rouge and KR victims live side by side; many local officials are former khmer Rouge
• After 30 years a tribunal has now been authorized, to last 3 years and prosecute up to 6 top leaders, starting in 2007
Exhumed skulls from the “killing fields”

The model we chose

Trauma Healing Initiative Strategy
1. Training of trainers
2. Community outreach & education strategies
3. Training the Network
4. Network model development

Steps in the planning phase

Our first challenge:Setting the stage
• Is it feasible?
• How can we position the project to get the broadest support?
• Who should lead the effort in Cambodia?

Feasibility assessment
• Met with 20 organizations
• 30 key informants
• Explained project concept

Mapping networks of support and healing for communities affected by torture
Trauma survivor, family &
communitiesTraditional
healers
Community leaders &
community support
Schools
Human Rights NGOs
Public clinics & hospitals
International health NGOs
Training institutions
Spiritual healers
Media for public education
Ministry of health
War crimes tribunal
War crimes documentation
Human rightsenvironment
Local health NGOs &
village health workers
Get National Program for Mental Health congruence & blessing
• Dr. Ka Sunbaunet, Director
• 20-year mental health plan
• Interest in participating
• Congruent with plan

Assess relevance to upcoming Khmer Rouge trials (ECCC)
• Royal Government of Cambodia task force
• Helen Jarvis, special advisor

Choose implementing partner
• TPO Cambodia– MOU/subgrant– scope of work– Hire coordinator
And the partner chooses us.

Bring potential core group agency leaders together for the “call”

Our next challenge:Engaging partners in the project
• Engage individual clinicians
• Get buy-in from agencies
• Build knowledge & trust in CVT and among individuals

Engagement tactics
• International training events
• Start regular meetings to share cases and decide training topics
• Help review project plan
• Social time

A core group of clinicians begins to meet monthly from 9 organizations
• Trafficking victims• Human rights/torture clients• Extreme domestic violence/rape clients• Government psychiatry• University psychology department• Children’s mental health• Community mental health/training/trauma
treatment• Khmer Rouge anti-impunity and
documentation• Cambodian returnees from the U.S.

Progress in the implementing phase

The next challenge: How to train the Core Group of Clinicians

Expert trauma training consultant living in-country for one year
• In-depth training in psychotherapy(150 hours to date)
• Case consultation and observation
• Agency consults as requested
• Pilot curricula for future manualization

The next challenge: How to sustain and deepen the learning ?
• Create treatment and training manuals
• Continue expatriate consultancy as long as possible
• Incent organizational experimentation & service enhancement
• Encourage collaboration among partner agencies

Examples of collaboration among partners
• Department of psychology
• National Program for Mental Health
• NGO requests for assistance
• 5 requests for service enhancement subgrants

By the end of four years, THI hopes to have:
• Trauma treatment and training manuals
• Piloted public education strategies
• A core group of multi-disciplinary Cambodian clinicians who can train others
• Piloted innovations in ongoing clinical supervision and training
• A trauma clinic functioning in Phnom Penh that cares for torture survivors and serves as a training site

By the end of four years, THI plans to have:
• A functioning network of agencies and individuals in one urban and one rural area.
• Ongoing relationships between clinical providers serving torture/trauma survivors and human rights organizations
• A means of tracking and evaluating the level of impact the network is having on reaching and serving the target population.

Overall challenges with this model of capacity-building
• Low control vs. buy-in and low cost
• Potential for high impact & sustainability—but
• High risk for failure
• How can technology help in low resource/tech savvy
environment?
• Is there a “tipping point” when local agents continue to collaborate and train on trauma treatment ?

Opportunities:
a brighter future for Cambodia !

SummaryInternational Services International Capacity
BuildingTrauma Healing
Initiative
Context
The model chosen must fit the country context: culture, resources, potential for local control & broader impact
Scope
Training & direct services: Local scale
Training & OD: One indigenous institution with torture/human rights focus
Training only: Potential for reaching many agencies & governmt health structure
Control High Low Low-medium
Culturally appropriate
Direct long term supervision makes
adaptation of western therapy models to indigenous culture
easier
Run by local professionals Professional core group is consulted, but lack of
direct services makes ing this difficult
Cost High Low Low
Evaluation High control & direct
services makes evaluation easier
Self report & consultant monitoring
Classroom evaluation & some work observation
Local buy-in
Indigenous staff of CVT One institution Implementing partner, partner agencies, core
group of clinicians
Sustainability
Hard, because of cost & INGO model
Medium: Need to find other funders
High potential: Depends on buy-in &
appropriateness of training