Trauma and Burns NMS
70
Chapter 21: TRAUMA AND BURNS Canas, Genevieve
-
Upload
genevieve-canas -
Category
Science
-
view
65 -
download
1
Transcript of Trauma and Burns NMS

Chapter 21:TRAUMA AND BURNS
Canas, Genevieve

Trauma
Incidence
– Trauma is the leading cause of death for people 1-44 years of age.
– More than 150,000 people die from trauma every year.
– Half of these deaths result from motor vehicle accidents.

Trauma
The order of priorities in evaluating trauma patients is based on the advanced trauma life support (ATLS) course administered by the American College of Surgeons (ACS).

1. Primary survey.– A - Airway
– B- Breathing (ventilation)
– C- Circulation
– D- Disablility (neurologic deficit)
– E- Exposure/Enviroment

2. The physician or emergency medical technician is urged to:– A- Establish a patent airway
– B- Ensure that both lungs are ventilated
– C- Restore circulating volume and compress external bleeding sites
– D- Check for neurologic deficit
– E- Fully expose (undress) the patient and cover with warmed blankets

3. Diagnosis of immediately life-threatening injuries, followed by rapid treatment
4. Reassessment of the patients' status
5. Secondary survey, complete• history, head-to-toe physical exam, Glasgow Coma Scale (GCS)
6. Definitive treatment, including surgery, prophylactic antibiotics, and tetanus prophylaxis
B Mechanisms of injury
1. Acceleration- deceleration injuries
• caused by falls from heights, blunt trauma, or vehicular accidents.
– Obvious injuries result from direct contact with the landing site (i.e., the ground or the vehicle).
– Subtle injuries result from shearing forces produced by the momentum when heavy organs are suddenly halted or accelerated by a crash.

2. Missile injuriesa. Low-velocity missile injuries include most civilian
gunshot wounds.• Missiles fired from handguns have a velocity in the range of
600- 1,100 ft/second.
• Wounds from this type of missile are generally restricted to the path and the residual cavity created by the missile as it penetrates tissues, such as blood vessels and organs. However, secondary injuries can occur.– External articles (buttons or keys) may be driven into the wound
by the missile.
– Bone fragments, produced when the missile strikes a large bone, can also cause secondary injury.

2. High-velocity missile injuries
– can be recognized by a small entrance wound and a large exit wound with severe underlying tissue damage.
3. Shotgun injuries• Close-range shotgun injuries can be devastating. Large
soft tissue defects are created with widespread damage
• Long-range shotgun injuries consist of multiple low-velocity pellet injuries. These cause widespread penetration but are generally not severe unless the missile happens to strike a major blood vessel or organ.

4. The shocking, knock-down• effect of a missile depends on factors that influence the energy transferred to the victim by the impact.
• Striking energy is directly proportional to the weight of a missile and the square of its velocity.
• Missiles that completely penetrate the victim expend much of their energy on the objects beyond the victim.
• Penetration is diminished when a bullet is used that expands or tumbles after impact.

Treatment
– All missile tracts should be debrided, but missiles need not be removed unless they cause symptoms or are in proximity to a vital structure where body movements or tissue erosion could cause further injury.
C. Management of trauma victims
1. Airwaya. Assessment
• The mouth and upper airway should be inspected for obstruction from foreign bodies (teeth, blood) or maxillofacial instability.
• Stridor or hoarseness implies laryngeal obstruction or injury.
• Examine the neck for asymmetry, cyanosis, subcutaneous emphysema, and fractures.
• The chest should be auscultated for bilateral equal breath sounds.
b. Treatment. Rapid measures are necessary to correct unsatisfactory ventilation.
1. Supplemental oxygen should be administered to all trauma victims until stable.
2. Basic manuevers for relieving obstruction and maintaining ventilation include:– Finger sweep
– Chin lift/jaw thrust
– Oropharyngeal airway
– Nasopharyngeal airway

3. Provide definitive airway.a. Early intubation is important in unstable patients due to the
propensity for apnea and sudden circulatory collapse. Some indications for rapid intubation include:
» Depressed mental status (GCS <8)
» Major head, face, or neck injury
» Impaired ventilation from paralysis
b. Oral tracheal intubation is the most common modality used to provide a definitive airway. Patients are preoxygenated with a bag-valve mask and then intubated with in-line cervical stabilization. Rapid-sequence induction with cricoid pressure should be utilized.
c.Nasotracheal intubation is acceptable only in a spontaneously breathing patient without a suspected basilar skull fracture.

d. Surgical airway should be performed if standard intubatingtechniques are unable to be performed or are contraindicated.
» Jet ventilation via a 12- or 14-gauge catheter in the cricothyroid membrane
» Cricothyroidotomy is contraindicated in children less than 12 years of age or in patients with laryngeal fractures.
» Tracheostomy

2. Breathing
a. Assessment
1. Ventilation should be assessed by auscultation of the chest, followed by entidal CO2 monitoring to check for endotracheal tube misplacement. Continuous pulse oximetry and arterial blood gas analysis is also useful.
2. Inspect the thorax for sucking chest wounds, subcutaneous emphysema, tracheal deviation, and diminished breath sounds.

b. Treatment
1. Pneumothorax is diagnosed by absent breath sounds, tracheal deviation away from the affected side, and hypotension.– Needle decompression in the second intercostal space,
midclavicular line
– Chest tube placement
2. Hemothorax (volume replacement and chest tube)
3. Open chest wound (placement of a semiocclusivedressing and chest tube)

3. Circulatory support
a. Assessment of the circulatory status should include appraisal of:
1. Character of the pulse– A rapid, faint pulse suggests profound hypovolemia in most
cases.
– A slow, full pulse may be indicative of severe neurologic injury with increasing intracranial pressure or hypercarbia.
2. Peripheral perfusion, as indicated by level of consciousness, rate of capillary refilling, urine output, and body temperature

3. Tachycardia may be an early compensatory sign of hypovolemia.
4. Blood pressure. The presence of a mild hypotension may be associated with inadequate tissue perfusion. A narrowed pulse pressure with diastolic hypertension is one of the earliest signs of hypovolemia.
5. Stable vital signs with major injury. The condition of patients with major injury and seemingly stable vital signs is dangerous and deceptive.

b. Treatment
1. Venous accessa. Lines should be inserted by a reliable method with which the
physician is comfortable.
» Large-bore peripheral catheters
» Subclavian catheterization
» Subclavian lines and a saphenous
» The saphenous vein

b. Two lines are usually inserted simultaneously.
» It is best to keep one on each side of the diaphragm so that volume replacement is effective in case of vena cavalor subclavian venous trauma.
» Shock patients often require between two to four separate lines for volume replacement to increase the blood pressure to more than 100 mm Hg in less than 10 minutes.
» The first intravenous insertion should include the withdrawal of 20 mL of blood for crossmatching and for laboratory studies, including a type and cross.
» Femoral artery punctures should be performed early for blood gas analyses.

c. All resuscitation lines should be replaced in 12- 24 hours. The urgent insertion of these lines leaves sterility in question, and catheter sepsis can become a serious problem after 24 hours.

2. Volume resuscitation– The initial fluid replacement should be isotonic saline or
lactated Ringer's solutions.
– Once 2 L of crystalloid has been infused, blood transfusion should be strongly considered.
– Unmatched O-positive blood should be used in emergent situations when time is not available for formal blood typing and crossmatching. O negative blood should be used in female patients of childbearing age.
– Fresh frozen plasma, cryoprecipitate and platelets are reserved for known or suspected coagulopathies.
3. Control of hemorrhage must accompany fluid resuscitation.– External bleeding
» Applying direct pressure on bleeding wounds with manually held gauze pads is safe and usually effective.
» Proximal and distal digital compression of bleeding superficial vessels may allow visualization of the bleeding point and accurate clamping.
» Pressure dressings may be used to control diffuse bleeding from abrasions and avulsions that involve large areas.
» Temporary packing of missile tracts and stab wounds can slow the blood flow until surgical exposure is obtained.
» Pneumatic splints and medical antishock trousers (MAST) help in tamponading bleeding and increasing peripheral resistance to increase the blood pressure.
» Tourniquets should be avoided if personnel are available for direct compression.
– Internal bleeding requires early diagnosis and prompt treatment by appropriate surgical intervention
4. Cardiac resuscitationa. Closed chest cardiac massage should be performed while fluid
resuscitation is begun if the patient is asystolic or demonstrates evidence of poor cardiac function.
b. Emergency room thorocotomies for open cardiac massage have few indications and should only be performed by trained surgeons.
c. Indications for emergency room thoracotomy are:
» Hypovolemic cardiac arrest despite vigorous blood volume replacement plus closed chest massage and defibrillation
» Cardiac arrest with penetrating injury to the chest

d. Relative contraindications include:
» Major obvious injuries to the central nervous system (i.e., decapitation, extruding brain tissue)
» Failed external cardiac massage lasting more than 10 minutes
» Major blunt trauma

5. Monitoring circulating blood volume and resuscitative therapy is based on the signs and symptoms of shock. – Urine output measured hourly is an important guideline to
the accuracy of fluid resuscitation. Output exceeding 30 cc/hour implies adequate perfusion to all vital organs.
– CVP can be useful when its trend is observed over time and in patients with significant preexisting cardiac and pulmonary disfunction. Pulmonary artery (Swan-Ganz) catheter monitoring may be more appropriate in these patients.

5. Assessment of neurologic injury
a. Head trauma
1. Assessment– Loss of consciousness signifies a head injury until such an
injury has been ruled out.
– Intracranial trauma cannot be adequately assessed while the patient is in shock.
– If hypotension is present in a patient with a head injury, it is rarely secondary to the head trauma, and the physician must look for another cause of the hypotension.

d. The neurologic evaluation should assess the following factors rapidly:
» Level of consciousness
» Motor activity and tactile sensation
» Obvious head trauma, such as a depressed skull fracture, gunshot wound, or leaking cerebrospinal fluid
» Pupil size and response to light
» Oculocephalic (doll's eye•) reflex. Because testing involves rotating the patient's head, it should only be done after spinal cord injury has been ruled out.
e. Evolving hypertension and bradycardia (Cushing's phenomenon) indicate increasing intracranial pressure and a worsening neurologic problem.

2. Treatment– Initial management includes the following considerations:
» Sterile saline-soaked gauze should be placed over open injuries.
» Mannitol and other drugs to lower intracranial pressure should be given
» Hypotension and hypoventilation seriously injure brain cells. It is, therefore, important to assess adequately fluid requirements and ventilation.
» Overhydration increases intracranial pressure and should be avoided once fluid requirements have been met and the patient is stable.

b. Spinal cord trauma
• Assessment– Until proven otherwise, the spine should be considered
unstable and the cord, therefore, liable to injury in all patients with major blunt trauma.
– The cervical spine should be considered unstable in:
» Every unconscious patient
» Every patient with face and head contusions or vertebral tenderness
» Every patient with decreased mentation, which precludes adequate neurologic examination

c. Radiographic films showing all seven cervical vertebrae intact should be obtained before allowing the patient's neck to be extended for any reason.
d. Evidence of injury to the spinal cord should be sought.
» It should be recognized that the cord may not yet be injured although the spine is unstable.
» Appropriate spinal stabilization must be performed until proper studies have been done.
» Findings, such as absence of motor or sensory function below the injury, loss of muscle tone, and loss of anal sphincter tone, should be sought.
» Hypotension may be present if there is a loss of vascular tone (arterial and venous) within the affected region.

6. Exposurea. Assessment.
All patients should be removed of clothing from head to toe. This allows for complete visualization of the entire body surface, which helps to limit missed injuries.
b. Treatment.
Hypothermia must be addressed rapidly to avoid complicating the patient's hemodynamic status. Heated blankets, warmed IV fluids, and raising the ambient room temperature are excellent ways to limit hypothermia.

7. Secondary surveya. Head and neck.– Pupil size and character, tympanic membranes, and
facial stability should all be assessed.– Fractures should be evaluated for airway
compromise. – Rhinorrhea and otorrhea should be suspected with
clear drainage. – Raccoon eyes and Battle's sign indicate a base of
skull fracture. – Computed tomography (CT) is the imaging of choice
for these injuries.

b. Thorax
Tension pnuemothorax and massive hemothorax are often diagnosed and treated on the primary survey. Pulmonary contusion, rib fractures, small effusions, and small pneumothoraxes are found on chest radiographs, which should be performed early on during the resuscitation.
1. Tamponade is decreased cardiac output secondary to poor right ventricular filling that is impaired by fluid (blood) around the heart.– Echocardiography
– Pericardial window is a surgical procedure where the pericardium is directly visualized from a subxyphoid approach.
– Pericardial centesis should only be used to decompress a tamponade that is awaiting surgery.

2. Blunt aortic tears and penetrating great vessel injury– Chest x-ray. Widened mediastinum, deviation of nasogastric
(NG) tube, depressed left mainstem bronchus, pleural cap, blurring of aortic knob, and first and second rib fractures all could indicate great vessel injury
– Transesophageal echocardiography
– Angiography is the gold standard. May be replaced eventually with CT or magnetic resonance (MR) angiography.
3. Esophageal perforation must be evaluated with esophagoscopy and contrast swallow.
c. Abdomen
• Diagnostic peritoneal lavage– is an invasive test in which a surgeon places a catheter in the
peritoneal cavity and irrigates with 1 L of saline.
– The test is considered positive if the fluid cell count is greater than 100,000 red blood cells or greater than 500 white blood cells or if vegetative matter or bacteria is present. The lavageis sensitive but not specific to the organ injured.

• Ultrasound
• CT scan is a noninvasive test with excellent sensitivity and specificity. The exam is also the only modality that evaluates the retroperitonium.
• Surgery. Once ongoing bleeding or perforation is diagnosed, prompt laparotomy should be performed.

d. Genitourinary injuries
• Urethral injury– Blood at the meatus is an indication for retrograde
urethrography. Even gentle insertion of a Foley catheter can disrupt a partially divided urethra.
– Major injuries should be repaired surgically.
• Bladder injuries usually heal spontaneously if adequate urinary drainage is established.

• Kidneys are commonly injured organs.– Most renal injuries can be managed nonoperatively; however,
renal pedicle disruption or major parenchymal damage with hemorrhage are the primary indications for surgery.
– Intravenous pyelography provides a good test of renal function, but it is not adequate for determining anatomic continuity of the organ

e. Soft tissue injuries
1. Debridement is the key to avoiding infection and promoting rapid healing.– All devitalized tissue must be removed during debridement.
– The degree of injury often depends on the density of the tissue and its water content.
» The lung tends to receive relatively minor degrees of damage remote from the missile tract.
» By contrast, muscle or liver, because of their greater density and water content, develop large temporary cavities and require extensive debridement beyond the apparent missile tract.
2. Muscle– Wide areas of devitalized tissue occur in high-velocity wounds
and require debridement.
– Viable muscle tissue visibly contracts when touched with an electrosurgical instrument set on a low power. It also contracts when gently pinched with forceps.
– Muscle that does not react must be removed, although weakness and deformity will result.

3. Arteries– Palpable pulses do not rule out arterial injury.
– Grossly injured vascular areas that exhibit intramural bleeding or disruption require removal.
– Repair should be done with autogenous material, if at all possible.
– Fasciotomies are almost always required in conjunction with vascular repair if there has been prolonged ischemia or concominant venous injury.
– Stab wounds and missile tracts in proximity to major vascular structures require either surgical exploration or, at a minimum, emergency arteriography.

4. Major veins should be repaired when injured.
5. Nerves. It is not necessary to debride nerves that are injured. Exposed nerves should be covered with normal muscle or fat, leaving definitive repair for a future time.
6. Bone. Contaminated small pieces of bone that are not attached to soft tissue may be removed.
7. Lung tissue is usually resistant to remote damage. Because of its spongy nature, the lung absorbs shock without injury, so a missile tract generally contains all of the injury.

8. Parenchymal organs, such as the liver and kidney– Bleeding is the major problem. Devitalized tissue should be
removed with as much functional tissue left as possible.
– An effort should be made to salvage an injured spleen, particularly in a child. There is evidence that a small spleen slice, reimplanted in the omentum, will grow and provide some splenic function.
9 . Genitalia. Very conservative debridement is indicated. Exposed testicular tissue should be covered with scrotal skin or reimplanted under attached skin, if possible.

f. Fractures
1. A fracture is seldom a major priority in the presence of other life-threatening injuries.– Hemorrhage or vascular compromise associated with a
fracture gives it a higher priority, as does a threat to the viability of an extremity.
– Bleeding associated with a fracture can account for a large portion of a patient's circulating blood volume, and hypovolemic shock is commonly associated with bilateral femoral fractures.

2. Early fractures that are open can be treated in accordance with the associated soft tissue injury.– Debridement, vascular repair, and other soft tissue surgery
should be performed before stabilization of the fracture.
– However, adequate splinting and stabilization should be accomplished because it decreases the risk of fat embolism syndrome.
– Internal fixation devices are generally hazardous in the presence of extensive soft tissue injury and should be avoided, if possible.

g. Tendon injuries require conservative debridement only. Tendons should be covered with normal tissue; otherwise, they become devitalized and useless.
h. Special situations• Pediatrics. Young children have different injury patterns due
to their pliable skeletons and head-to-body ratio.
• Pregnancy. Assessment and treatment is directed toward the mother, as her health is primarily important to the fetus. Early obstetrical input as well as fetal ultrasounds and monitoring are vital. Emergent cesarean section for fetaldeterioration is performed in conjuction with the trauma surgeons

BURNS

Burns
1. Depth of burns
a. First-degree burns (involvement of epidermis only). Clinical findings are limited to erythema.
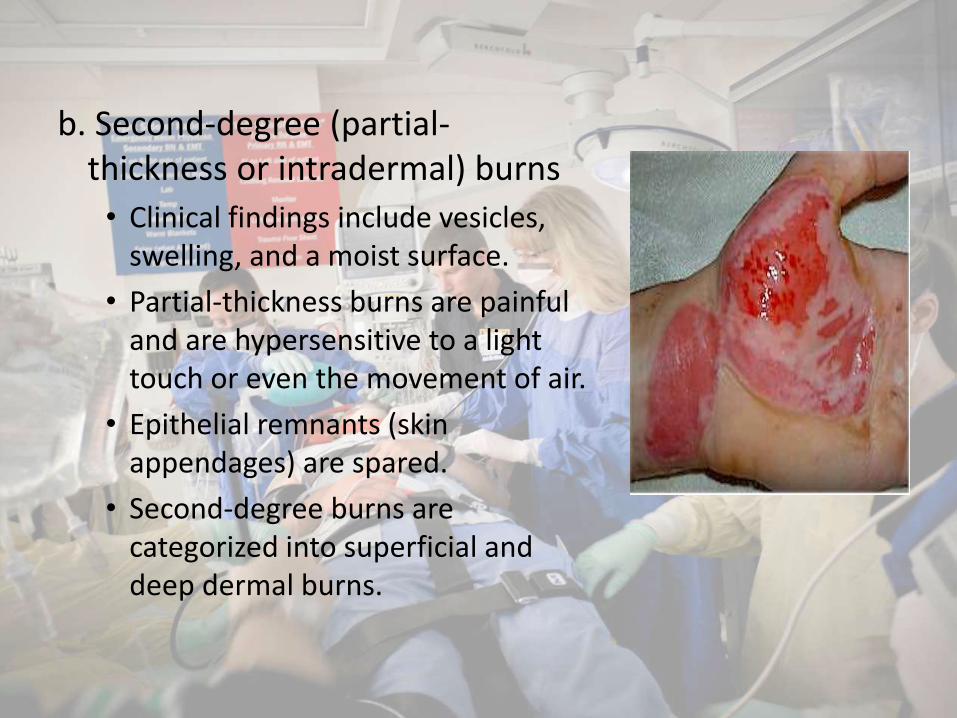
b. Second-degree (partial-thickness or intradermal) burns
• Clinical findings include vesicles, swelling, and a moist surface.
• Partial-thickness burns are painful and are hypersensitive to a light touch or even the movement of air.
• Epithelial remnants (skin appendages) are spared.
• Second-degree burns are categorized into superficial and deep dermal burns.

c. Third-degree (full-thickness, entire depth of dermis) burns• These burns have a
charred, waxen, or leathery appearance and may be white or grayish in color. They usually appear dry. Thrombosed vessels may be evident.
• The burn surface is pain free and is anesthetic to a pinprick or to touch.

• Extent of burns. This is determined by the rule of nines– Inpatient treatment is required for a patient with
either:• Full-thickness burns extending over 2% or more of the
body surface area (BSA)
• Partial-thickness burns extending over 10% or more of the BSA
• Intravenous fluid resuscitation is required for all partial-or full-thickness burns extending over 20% or more of the BSA


3. Location of burns
– Inpatient treatment is required for second- or third-degree burns of the face, hands, feet, or genitalia.
– Second- or third-degree burns involving major flexion creases usually require hospital treatment to minimize contractures and other late problems.
– Second and third-degree burns exceeding 20% BSA.

Airway control and ventilation
1. Airway obstruction may develop rapidly after inhalation injury or may be delayed. The possibility should be suspected if any of the following conditions are present:– A history of being burned in a confined space
– A facial burn or singed facial hair
– Charring or carbon particles in the oropharynx
– Carbonaceous sputum
– Circumferential burns of the trunk, especially those with a thick eschar (which may require emergency excision

2. Measurement of arterial blood gases is indicated as well as measurement of carbon monoxide level (carboxyhemoglobin value over 10% is significant)
3. Endotracheal intubation should be performed before the patient develops respiratory problems.

Circulatory support and fluid resuscitation
• Major burns those involving 20% or more of the BSA call for fluid resuscitation.
1. Intravenous fluids should be administered through a 14- or 16-gauge intravenous catheter.– The catheter may be placed through the burn
wound, if required.
– Intravenous fluids should not be given via a lower extremity because the site is prone to sepsis and its increased mortality risk.

2. Fluid resuscitation should begin with lactated Ringer's solution.a. The volume to be given is calculated as follows:
• For adults: % BSA burned — kg body weight — 2-4 mLelectrolyte solution
• For children: % BSA burned — kg body weight — 3 mLelectrolyte solution
• The percentage of the BSA that is burned is estimated by the rule of nines
b. Half of the calculated amount of fluid is given in the first 8 hours, and the remaining half is distributed over the succeeding 16 hours.

c. The volume and rate of fluid administration should be varied• Optimal urine output is 30- 50 mL/hour in adults and 1
mL/kg of body weight/hour in children.• To aid urine flow and to allow monitoring of output, an
indwelling urethral catheter should be inserted early, even in children.
d. Evaporative hypotonic fluid loss is evident after the first 24 hours.• Intravenous fluids at a rate to maintain serum sodium
concentration at 140 mEq/L• Colloid (controversial) at a rate of 0.3-0.5 mL plasma/kg body
weight/% burn
Burn wound care
1. Cold compresses may be applied to relieve the pain of partial-thickness burns if the burns cover less than 10% of the BSA.
2. Maintenance of body temperature is important, especially in children, who have a high evaporative heat loss and may rapidly become hypothermic.
3. Shielding the burn from air movement by covering it with a clean, warm linen dressing will help to relieve the pain of partial-thickness burns.

4. Topical antimicrobial treatment with agents such as silver nitrate solution is usually recommended for deep second-degree and third-degree burns.
5. Debridement and escharectomy are best performed in specialized centers; however, escharotomy may be urgently required in circumferential extremity wounds, causing distal circulatory impairment, and in circumferential trunk or neck wounds, causing respiratory impairment.

Other considerations
1. NG intubation is indicated for any patient with nausea or vomiting and for most patients with burns covering 25% or more of the BSA.
2. Analgesia should be confined to conservative use of intravenous narcotics in small, frequent doses.
3. Systemic antibiotics are usually not indicated. However, in some situations, particularly in the early treatment of patients with partial-thickness burns, prophylaxis is warranted.
4. Tetanus toxoid with or without hyperimmunehuman globulin should be given if the patient's immunization status is not current

5. Chemical burns
– Alkali burns are generally deeper and more serious than acid burns.
– All chemical burns should be treated by flushing with neutral solutions.
• Immediate drenching in a shower or with a hose is helpful.
• Burns of the eye require extensive flushing over an 8-hour period.
6. Electrical burns are usually deeper and more severe than indicated by the surface appearance.a. Muscle and soft tissue injury
• Muscle involvement may be markedly underestimated by attention to the surface wounds alone (e.g., fluid requirements are about 50% higher than estimated by surface wounds).– Brawny edema is characteristic.– Early escharotomy, fasciotomy, and debridement are often
necessary, and repeated explorations at 24-48 hours may be needed.
– Serious soft tissue injury results from high-voltage electrical burns (generally considered more than 1,000 volts); low-voltage electrical burns (household outlets) cause less soft tissue injury but may cause asystole and apnea.

b. Surface burns occur at both the entrance and exit points of the current.
c. Oliguria is common, as is acidosis.
• Urine output should be maintained at high levels at least 100 mL/hour in adults. Mannitol administration is usually needed to maintain this level and is mandatory in the presence of myoglobinuria.
• Arterial blood pH should be monitored and maintained with intravenous bicarbonate, given as 50 mEq every half hour until the pH reaches normal levels.

d. Myocardial infarction (immediate or delayed) is well-described postinjury, thus making continuous cardiac monitoring essential in all patients with electrical burns.
e. Transverse myelitis and cataracts are long-term sequelae.


















