
Trattamento antiaggregante orale precoce nel paziente ... · Trattamento antiaggregante orale...
49
Trattamento antiaggregante orale precoce nel paziente NSTEMI: il trial DUBIUS Giuseppe Musumeci USC Cardiologia Ospedale Santa Croce e Carle Cuneo Como 1 Aprile 2017
Transcript of Trattamento antiaggregante orale precoce nel paziente ... · Trattamento antiaggregante orale...

Trattamento antiaggregante orale precoce nel paziente
NSTEMI: il trial DUBIUS
Giuseppe Musumeci
USC Cardiologia
Ospedale Santa Croce e Carle Cuneo
Como 1 Aprile 2017

➢ Ticagrelor > clopidogrel up (< 10 days) or dowstream (as switch)
➢ D/MI/stroke -2.1% vs -2.5% ARR (-18% RRR)
➢ Major bleeding + 0.4% vs +0.8% ARR (+4% vs +7% RRR)
➢ Non-CABG major bleeding + 0.7% vs +1% (+19% vs +28% RRR)

➢ Prasugrel > clopidogrel only dowstream
➢ D/MI/stroke -2.2% vs -0.1% ARR (-19% vs -2% RRR)
➢ Non-CABG major bleed + 0.6% vs +0.8% (+32% vs +195% RRR)
NSTE-ACS
Coro
MedicalRx
PCI
CABG
MedicalRx
Ho
spital
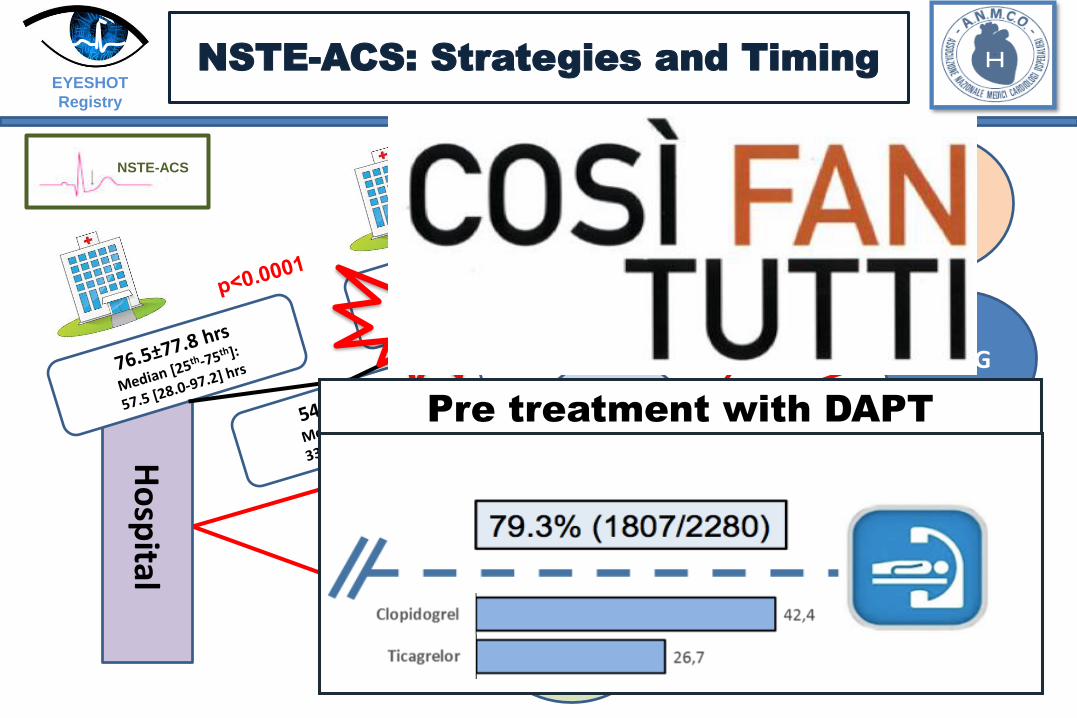
NSTE-ACS: Strategies and Timing
Pre treatment with DAPT
EYESHOT
Registry

* In addition to other standard therapies.
* Patients did not receive open-label thienopyridine before PCI.
Mehta SR et al for the CURE Investigators. Lancet. 2002
Days of follow-up
Composite of MI, urgent revascularization or cardiovascular death at 30 Days
0 5 10 15 20 25 30
0.0
0.02
0.04
0.06
0.08
Cu
mu
lati
ve
Ha
zard
Ra
te
44%Relative Risk
Reduction
p=0.017
(0.35-0.90)
Clopidogrel
pretreated
Placebo
pretreated
Pre-Treatment with Clopidogrel Prior to PCI and Stenting in ACS Patients

CREDO – clopidogrel loading dose timing
and MACE at 28d in per protocol patients (n=1762)
-2
-3
-4
-5
-6305 10 15 20 250
Hours prior to PCI of study drug loading dose
Log odds of death, MI or urgent TVR at 28
daysPlacebo
Clopidogrel
P=0.020for treatment / timing
interaction

Bellemain-Appaix A, et al. JAMA. 201terial2;308
Supplemental material,
Clopidogrel and Pre-Treatment in PCI: A Meta-Analysis
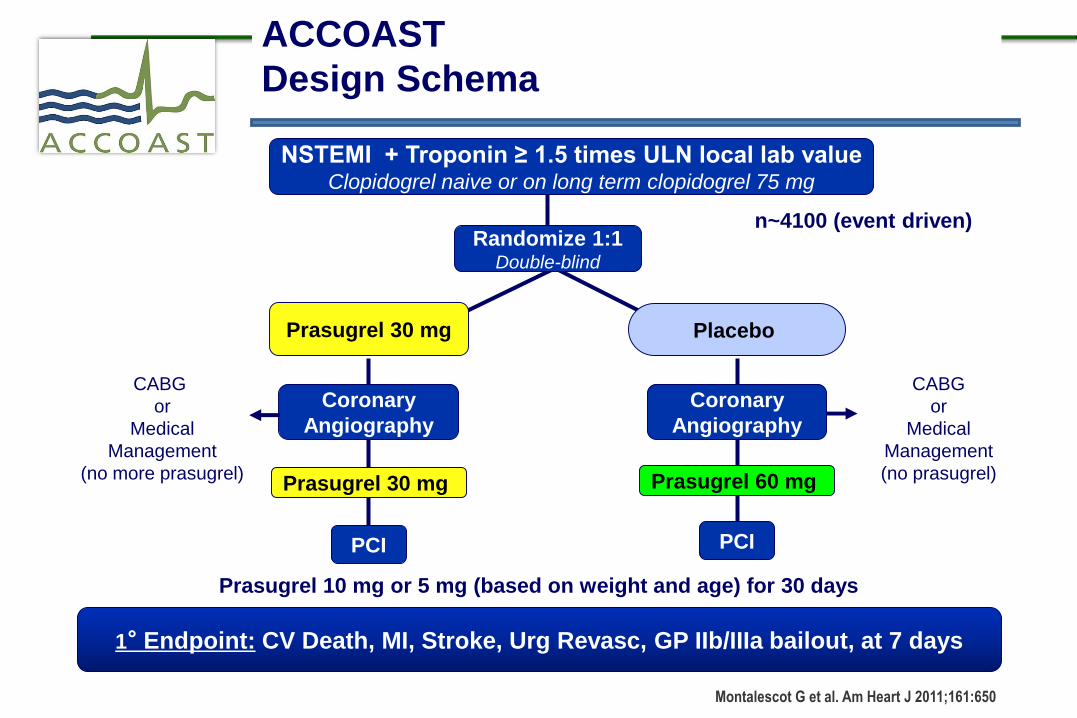
Prasugrel 30 mg
Prasugrel 60 mg Prasugrel 30 mg
Prasugrel 10 mg or 5 mg (based on weight and age) for 30 days
PCI
1° Endpoint: CV Death, MI, Stroke, Urg Revasc, GP IIb/IIIa bailout, at 7 days
Placebo
Coronary
Angiography
n~4100 (event driven)
Coronary
Angiography
PCI
CABG
or
Medical
Management
(no prasugrel)
CABG
or
Medical
Management
(no more prasugrel)
Montalescot G et al. Am Heart J 2011;161:650
Randomize 1:1Double-blind
NSTEMI + Troponin ≥ 1.5 times ULN local lab valueClopidogrel naive or on long term clopidogrel 75 mg
ACCOAST
Design Schema

Days From First Dose
0 5 10 15 20 25 30
En
dp
oin
t (%
)
0
5
10
15
1996
2037
1788
1821
1775
1809
1769
1802
1762
1797
1752
1791
CV Death, MI, Stroke, UR, GPIIb/IIIa Bailout
1621
1616
No. at Risk, Primary
Efficacy End Point:
No pre-treatment
Pre-treatment
Pre-treatment10.810.0
Pre-treatment
Hazard Ratio, 0.997 (95% 0.83, 1.20)P=0.98P=0.81
(95% 0.84, 1.25) Hazard Ratio, 1.02
No Pre-treatment10.8
9.8No Pre-treatment
1° Efficacy End Point @ 7 + 30 days
(All Patients)
Montalescot G, et al. N Engl J Med 2013;369:999

All TIMI (CABG or non-CABG) Major
Bleeding (All Treated patients)
Days From First Dose
0 5 10 15 20 25 30
En
dp
oin
t (%
)
0
1
2
3
4
5
All TIMI Major Bleeding
Pre-treatment2.9
Pre-treatment2.6
No Pre-treatment1.5
No Pre-treatment1.4
19962037
19471972
13281339
12971310
12881299
12841297
12631280
No. at Risk, All TIMI Major Bleeding:No pre-treatmentPre-treatment
Hazard Ratio, 1.97 (95% 1.26, 3.08)P=0.002
Hazard Ratio, 1.90(95% 1.19, 3.02) P=0.006
Montalescot G, et al. N Engl J Med 2013;369:999

Evidence (NSTEMI) upstream vs
downstream?
Clopigogrel: Upstream flawed superiority UP vs DOWN
Prasugrel: Downstream > Upstream
Ticagrelor: Downstream > Upstream unsettled
“STEMI no overall advantage”
GPI:
I IIa IIb III
AWhen coronary anatomy is
not known.

Antiplatelet in NSTEACS
I IIa IIb III
B
I IIa IIb III
BTicagrelor (180 mg LD, 90 mg bid) is recommended, in the absence of contraindications, for all pts at moderate-to-high risk of ischaemicevents, regardless of initial treatment strategy and including those pretreated with clopidogrel
I IIa IIb III
B
Prasugrel (60 mg LD, 10 mg daily dose) is recommended in patients who are proceeding to PCI if no contraindication
Clopidogrel (300–600 mg LD, 75 mg daily dose) is recommended for pts who cannot receive ticagrelor or prasugrel or who require oral anticoagulation
It is not recommended to administer prasugrel in pts in whom coronary anatomy is not known
ESC guidelines, 2015
I IIa IIb III
B
“…As the optimal timing of ticagrelor or clopidogrel administration in
NSTE-ACS patients scheduled for an invasive strategy has not been
adequately investigated, no recommendation for or against
pretreatment with these agents can be formulated”

Unknown issues
➢ UPSTREAM Tica > DOWNSTREAM Tica?
➢ DOWNSTREAM Tica > DOWNSTREAM Prasugrel?
➢ UPSTREAM Tica > DOWNSTREAM Prasugrel?

RANDOMIZED CONTROLLED TRIAL
Downstream versus Upstream strategy for the
administration of P2Y12 receptor Blockers In
non ST elevated acUte coronary Syndromes
with initial invasive indication.
PI G. Tarantini
Co-PI G. Musumeci
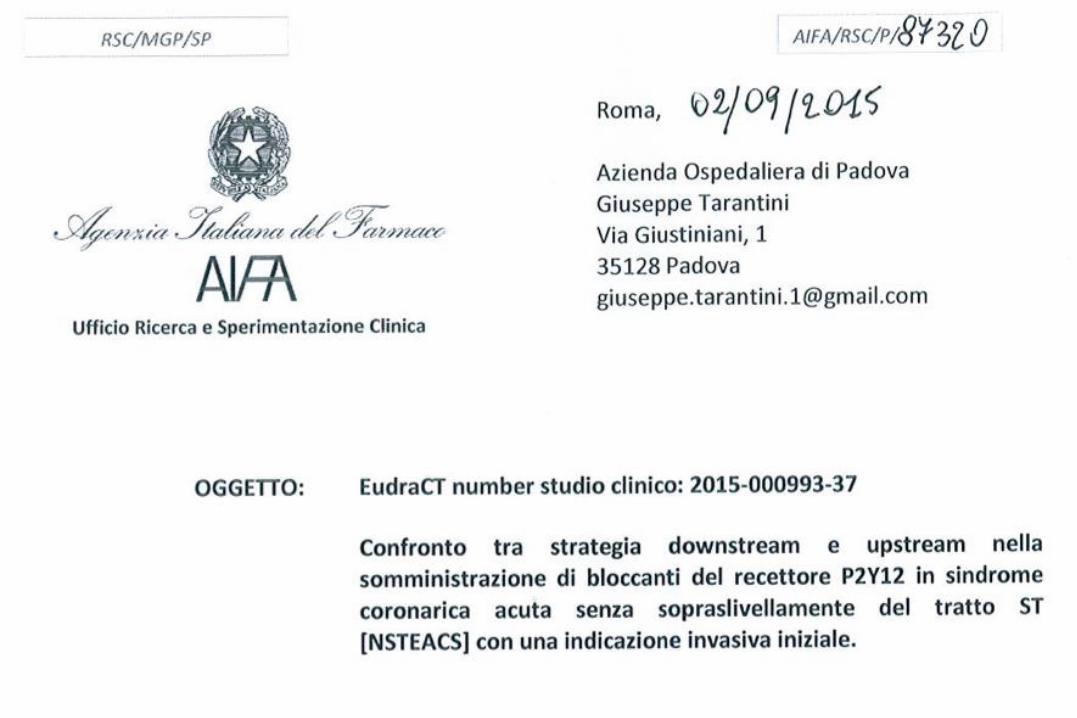


DUBIUS TRIAL
Downstream versus Upstream strategy for the administration of P2Y12 receptor Blockers In non ST elevated acUte coronary Syndromes with initial invasive indication
HYPOTHESES:1. Superiority of downstream vs upstream strategy2. Non inferiority of Prasugrel vs Ticagrelor
CO-PRIMARY (powered) HYPOTHESES
1. Superiority of the downstream administration strategy for P2Y12 receptor blockers over the upstream administration strategy (ticagrelor only) in terms of NACE at 30 days
2. Non inferiority of Prasugrel vs Ticagrelor in the PCI group of the downstream strategy arm in terms of NACE at 30 days.

PRIMARY ENDPOINT: NACE
Net Adverse Cardiac Events (NACE):
Death from vascular causes (cardiovascular or cerebrovascular, without another known cause)
non fatal MI
non fatal stroke
BARC major bleedings (type 3, 4 and 5)
SECONDARY ENDPOINTS
• Death from vascular causes
• MI
• Stroke
• TIA
• Severe recurrent ischemia
• Recurrent ischemia or other arterial thrombotic event
• Death from any cause.
• Stent thrombosis (possible, probable, or definite).
• Target vessel revascularization (TVR).
• Target lesion revascularization (TLR).
• NACE occurred between admission and revascularization
• BARC type 2, 3, 4 and 5 bleeding
• All TIMI major, major-life-threatening, and minor bleeding
• STEEPLE major and minor bleedings
• Compliance to mandated antiplatelet therapy

INCLUSION CRITERIA
1. Age ≥ 18
2. Non ST elevated acute coronary syndrome (unstable angina, non ST elevated myocardial infarction), with an onset of symptoms during the previous 72 hours.
3. An initial invasive strategy is chosen (the patient is expected to undergo coronary angiography within 72 h from admission).
4. Subject is able to start therapy with a new P2Y12 inhibitor (prasugrel or ticagrelor) OR is on a maintenance dose of clopidogrel or ticlopidine and is able to switch to a new P2Y12 inhibitor (prasugrel or ticagrelor).
3. Patient agrees to comply with follow-up evaluations.
MAIN EXCLUSION CRITERIA (1)1. Known hypersensitivity/contraindication to aspirin, clopidogrel, prasugrel, ticagrelor,
heparin or bivalirudin, or sensitivity to contrast media, which can't be adequately pre-medicated.
2. Platelet count <100,000 cells/mm³ or >700,000 cells/mm³, or a white blood cell (WBC) count <3,000 cells/mm³ within 7 days prior to index procedure.
3. Fibrinolytic therapy within 24 hours before randomization.
4. Concomitant therapy with a strong cytochrome P-4503A inhibitor or inducer.
5. Serum creatinine level >170 micromol/L within 7 days prior to index procedure.
6. Subject is receiving chronic anticoagulation therapy.
7. Subject is already receiving ticagrelor or prasugrel.
8. Shock.
MAIN EXCLUSION CRITERIA (2)
9. History of stroke or TIA
10. Active peptic ulcer or upper gastrointestinal bleeding within prior 6 months.
11. History of bleeding diathesis or coagulopathy or will refuse blood transfusions.
12. Planned elective surgery within 12 months after the procedure requiring discontinuation of any antiplatelet drugs.
13. Pregnant or nursing subjects
14. Other medical illness (e.g., cancer or congestive heart failure) or known history of substance abuse (alcohol, cocaine, heroin etc.)
15. Subject is belonging to a vulnerable population
16. Currently participating in investigational drug or device trial
FOLLOW UP
30 ± 7 days: office visit✓ Adverse events with related laboratory tests results, ECGs, details of any subsequent repeat
coronary angiography and results of such, if applicable.✓ Compliance to protocol required anti-platelet medications✓ Use and changes in chronic anti-platelet medications
12 months ± 30 days: office visit✓ Adverse events with related laboratory tests results, ECGs, details of any subsequent repeat
coronary angiography and results of such, if applicable.✓ Compliance to protocol required anti-platelet medications.✓ Use and changes in chronic anti-platelet medications.

STUDY CONDUCTION
SCTB@DCTV (Service of Clinical Trials and Biometrics)Dept. of Cardiac, Thoracic and Vascular Sciences, University of Padova
Randomization and e-CRF service (Red-Cap and Open-Clinica based)Study design and sample size calculationAssistance for regulatory aspects and ethical committee submission processStatistical plan (SAP), analysis and reporting (R and SAS)Risk-based monitoring
Public, University-level no-profit serviceResearch- and innovation-oriented approachLinked with advanced teaching (clinical epidemiologists, clinical researchers, research nurses, advanced biostatisticians)Master I level (Biostatistics for medical writing)Master II level (Advanced topis in biostatistics for clinical trials)
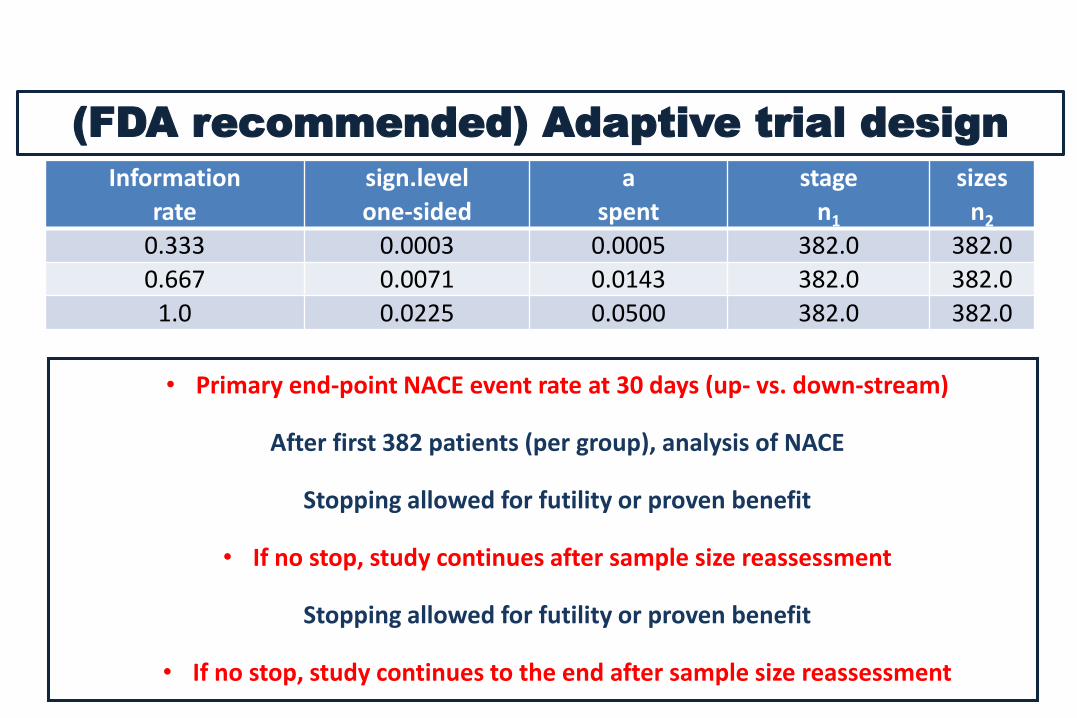
Information
rate
sign.level
one-sided
a
spent
stage
n1
sizes
n2
0.333 0.0003 0.0005 382.0 382.0
0.667 0.0071 0.0143 382.0 382.0
1.0 0.0225 0.0500 382.0 382.0
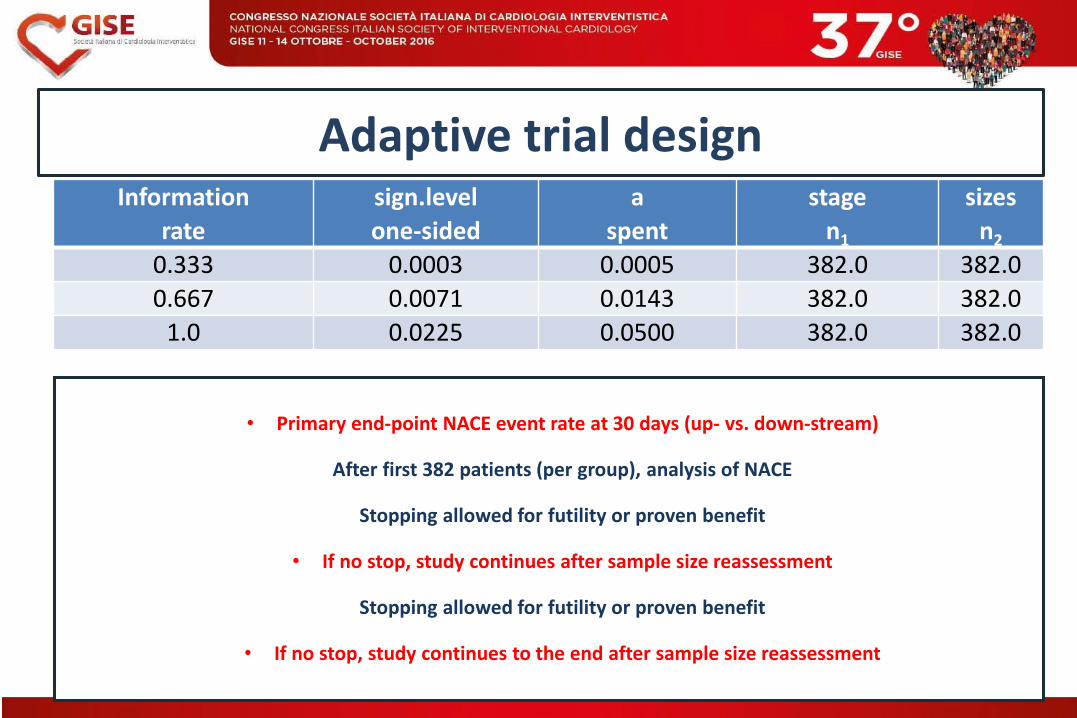
(FDA recommended) Adaptive trial design
• Primary end-point NACE event rate at 30 days (up- vs. down-stream)
After first 382 patients (per group), analysis of NACE
Stopping allowed for futility or proven benefit
• If no stop, study continues after sample size reassessment
Stopping allowed for futility or proven benefit
• If no stop, study continues to the end after sample size reassessment

LOMBARDIA
- A.O. di Desio e Vimercate
- A.O. Papa Giovanni XXIII
- A.O. Treviglio
- Centro Cardiologico Monzino
- A.O. Fatebenefratelli
- Policlinico San Matteo -
Fondazione IRCCS
- Ospedale Bassini
- Ospedale Niguarda Ca'
Granda
- Policlinico San Marco
ZIngonia
- A.O.S. Antonio Abate
- Humanitas
- Ospedale di Vimercate
- Istituto Scientifico Ospedale
San Luca
- Ospedale San Gerardo
- Ospedale Maggiore
- San Donato
PIEMONTE
- Ospedale degli Infermi
- Ospedale Maria Vittoria
- S.Giovanni Bosco
- Ospedale Maggiore
della Carità
- AO Ordine Mauriziano
di Torino
- P.O. Domodossola e
Verbania
LIGURIA
- Ospedale Galliera
- Ospedale San Paolo - ASL 2
Savonese
EMILIA ROMAGNA
- Policlinico S. Orsola –
Malpighi
- Ospedale G.B. Morgagni -
L. Pierantoni
- Ospedale Infermi – Rimini
- AOU Ferrara
- AO-IRCCS Santa Maria
Nuova
CAMPANIA
- A.O.S.G.Moscati
- A.O. Monaldi
- AO Universitaria Federico II
- Ospedale Cardarelli
TOSCANA
- A.O. Senese
- Azienda USL 9
- Azienda USL 4
- Ospedale del Cuore
- Azienda USL 6
- Azienda Ospedaliero-
Universitaria PisanaABRUZZO
- Ospedale Spirito Santo
CALABRIA
- A.O. di Cosenza
- AO Mater Domini di
Catanzaro
- S. Anna Hospital
PUGLIA
- Ospedale Civile Lorenzo
Bonomo
- Ospedale Casa Sollievo
Della Sofferenza
- San Paolo
LAZIO
- Ospedale Sandro Pertini
- Policlinico Casilino
- Ospedale S. Andrea
- Ospedale S. Spirito
VENETO
- Azienda ULSS 9 Treviso
- Azienda ULSS 13 Mirano
- Ospedale San Giacomo
- Ospedale Civile Santa Maria
della Misericordia
- Azienda ULSS 17 Schiavonia
- Casa di Cura Dott.
Pederzoli
SICILIA
- A.O. Universitaria Gaetano
Martino
- Ospedale 'Civile Maria
Paternò Arezzo
- P.S. S.Elia
- A.R.N.A.S. Ospedali Civico
- San Giovanni – ASP 1
SARDEGNA
- Ospedale San Francesco
- Ospedale Sirai
MARCHE
- Ospedale Civile di Macerata
TRENTINO
-Ospedale S.Maria del Carmine
ABRUZZO
-ASL 1 Avezzano – Sulmona –
L’Aquila – P.O. S. Filippo e Nicola
FRIULI
-Ospedali Riuniti Di Trieste
Coordinating Center:
PADOVA
711
5
3
4
2
41
16
526
3
16 Centri aderenti: 67
(+25 da GISE 2015)

Arruolati 312 pazienti
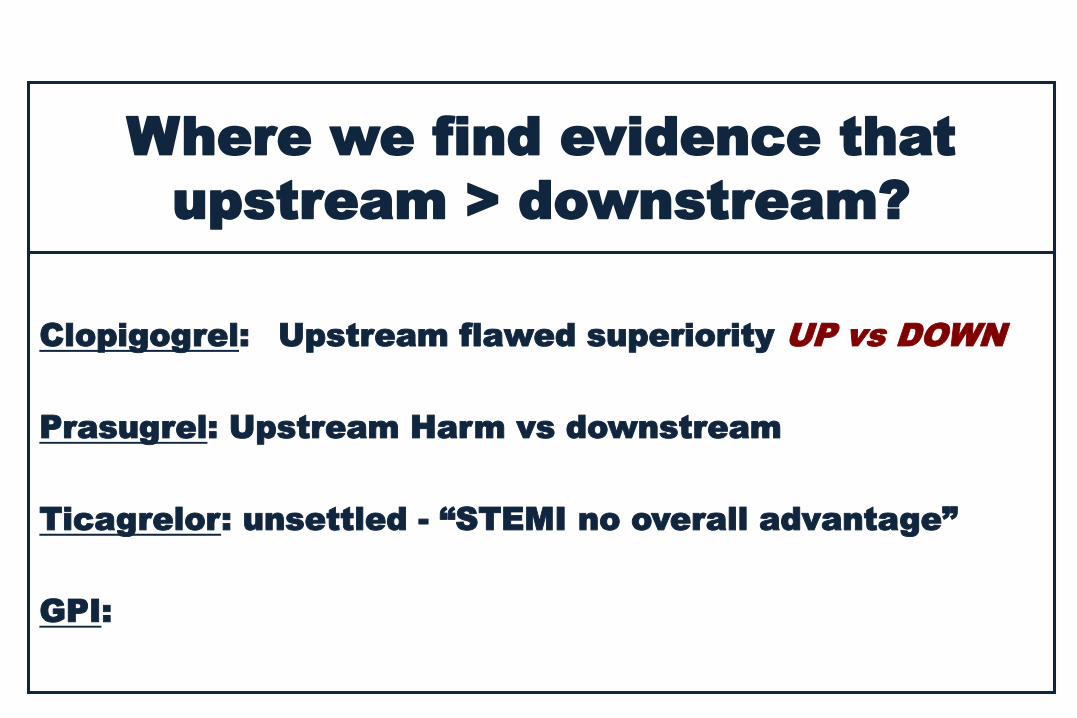
Where we find evidence that
upstream > downstream?
Clopigogrel: Upstream flawed superiority UP vs DOWN
Prasugrel: Upstream Harm vs downstream
Ticagrelor: unsettled - “STEMI no overall advantage”
GPI:

Study logistics
Randomization via dedicatedrandomization interface (PC and
mobile)
Data collection via on-line Red-Cap platform
Pt Rand (1) at first contact
to upstream vs downstream
Pt in downstream Rand (2) when decision is taken on PTCA
Discharge
30 days follow-up
1-year follow-up
Risk-based monitoring via centralizeddata flow-analysis and feedbacks to
centers
Adaptive ad-interim analysis (3 stages)

42
32
30 0 0 0 0 0
ARRUOLAMENTO ATTIVO
CENTRI APPROVATI (n=19)
Messina, G. Andò
Gallarate, S.I. Caico
Milano - Monzino, D. Trabattoni
Ragusa, A. Nicosia
Roma - Casilino, R. Della Bona
Roma - Pertini, S. Rigattieri
Cinisello Balsamo, S. Pierini
Mirano, C. Penzo
Treviglio, P. Sganzerla
Nuoro, G. Casu
ATTIVAZIONE IN CORSO
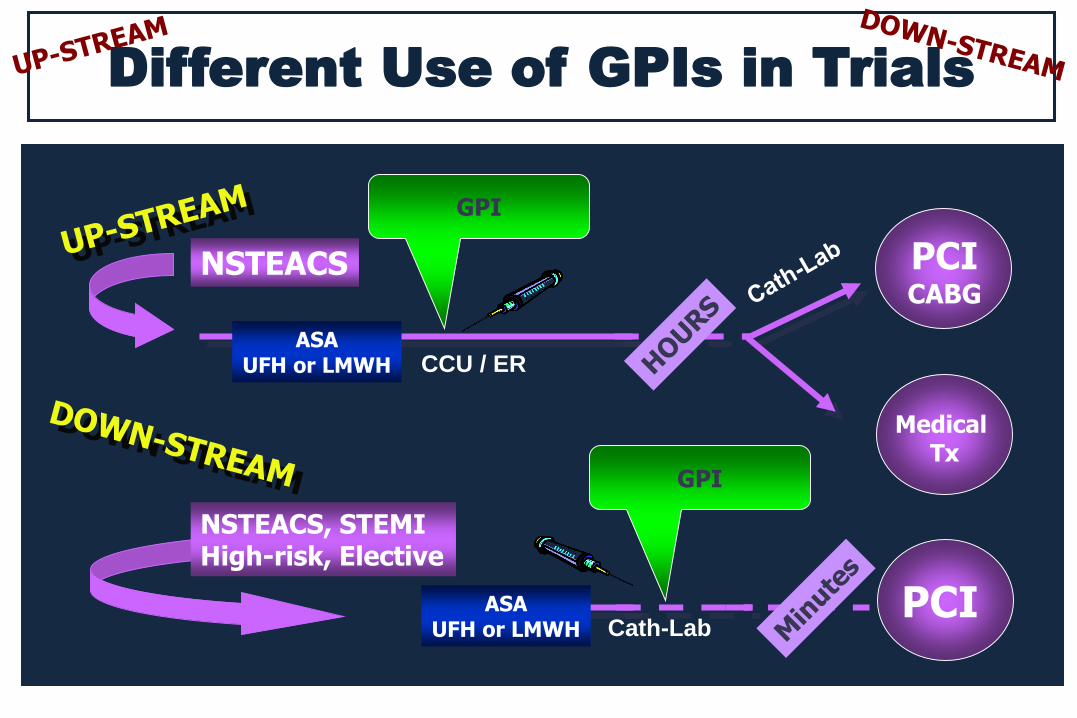
Different Use of GPIs in Trials
NSTEACS
ASAUFH or LMWH
GPI
PCICABG
Medical Tx
GPI
PCIASAUFH or LMWH
NSTEACS, STEMIHigh-risk, Elective
Cath-Lab
CCU / ER

Redefining GP IIb/IIA issues
NSTEACSGPI
GPI
EARLY ACS TIMACS

Bellemain-Appaix A, et al. JAMA. 2012;308:2507
Clopidogrel and Pre-Treatment in PCI: A Meta-Analysis
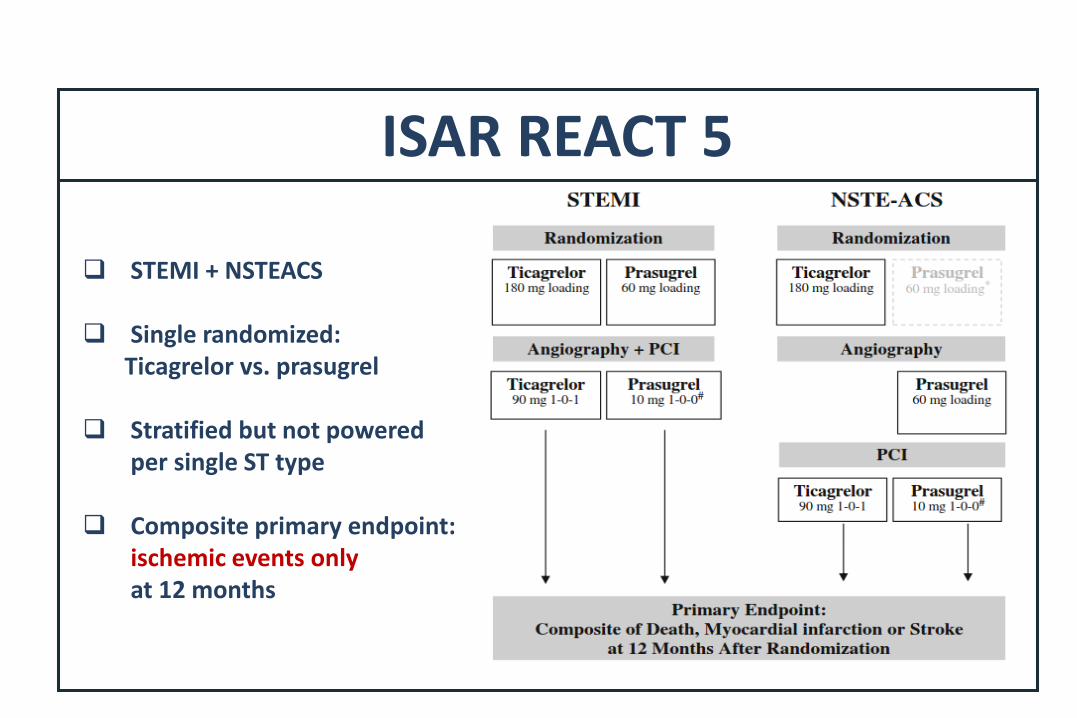
ISAR REACT 5
STEMI + NSTEACS
Single randomized:Ticagrelor vs. prasugrel
Stratified but not powered per single ST type
Composite primary endpoint:ischemic events onlyat 12 months

ESC 2015 UA/ NSTEACS guidelines
“UP versus Down -stream” strategy
ESC guidelines, 2015
“NO recommendation for or against pretreatment
with TICA or Clopidogrel can be formulated”
When upstream is selected
“optimal timing of TICA or CLOP administration in
NSTE-ACS patients scheduled for an invasive
strategy has not been adequately investigated”
Where we find evidence that
upstream > downstream?
Clopigogrel: Upstream flawed superiority UP vs DOWN
Prasugrel: Upstream Harm vs downstream
Ticagrelor: unsettled - “STEMI no overall advantage”
GPI: Upstream harm vs downstream

I IIa IIb III
A
I IIa IIb III
CGPIIb/IIIa inhibitors during PCI should be considered for bailout situations or thrombotic complications.
It is not recommended to administer GPIIb/IIIa inhibitors in patients in whom coronary anatomy is not known.
ESC guidelines, 2014 and 2015
GP IIb/IIIa in NSTEACS
GP IIb/IIIa in STEMI
I IIa IIb III
B
I IIa IIb III
CGP IIb/IIIa inhibitors should be considered for bail-out or evidence of no-reflow or a thrombotic complication.
Upstream use of a GP IIb/IIIa inhibitor (vs. in-lab use) may be considered in high-risk patients undergoing transfer for primary PCI.
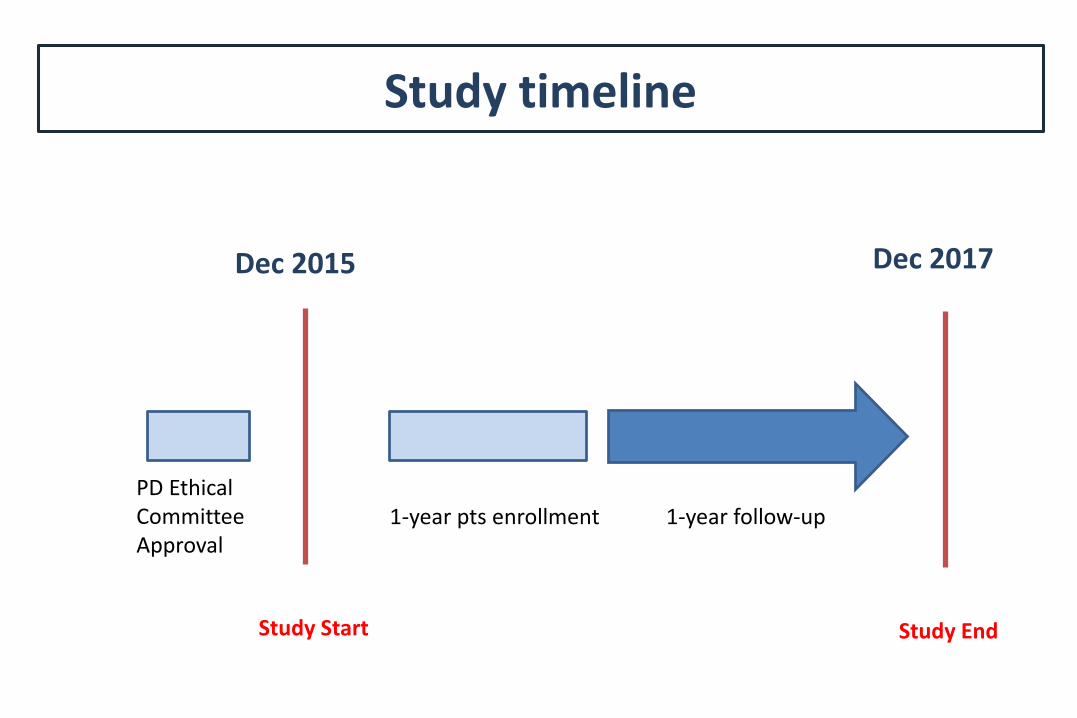
Study timeline
PD Ethical Committee Approval
Study Start
1-year pts enrollment 1-year follow-up
Dec 2015
Study End
Dec 2017
Information
rate
sign.level
one-sided
a
spent
stage
n1
sizes
n2
0.333 0.0003 0.0005 382.0 382.0
0.667 0.0071 0.0143 382.0 382.0
1.0 0.0225 0.0500 382.0 382.0
Adaptive trial design
• Primary end-point NACE event rate at 30 days (up- vs. down-stream)
After first 382 patients (per group), analysis of NACE
Stopping allowed for futility or proven benefit
• If no stop, study continues after sample size reassessment
Stopping allowed for futility or proven benefit
• If no stop, study continues to the end after sample size reassessment

NSTE-ACS
EYESHOT
Registry
Coro
MedicalRx
PCI
CABG
MedicalRx
Ho
spital
Pre treatment with DAPT
NSTE-ACS: Strategies and Timing

ACCOAST trial
Time to TX - Outcomes
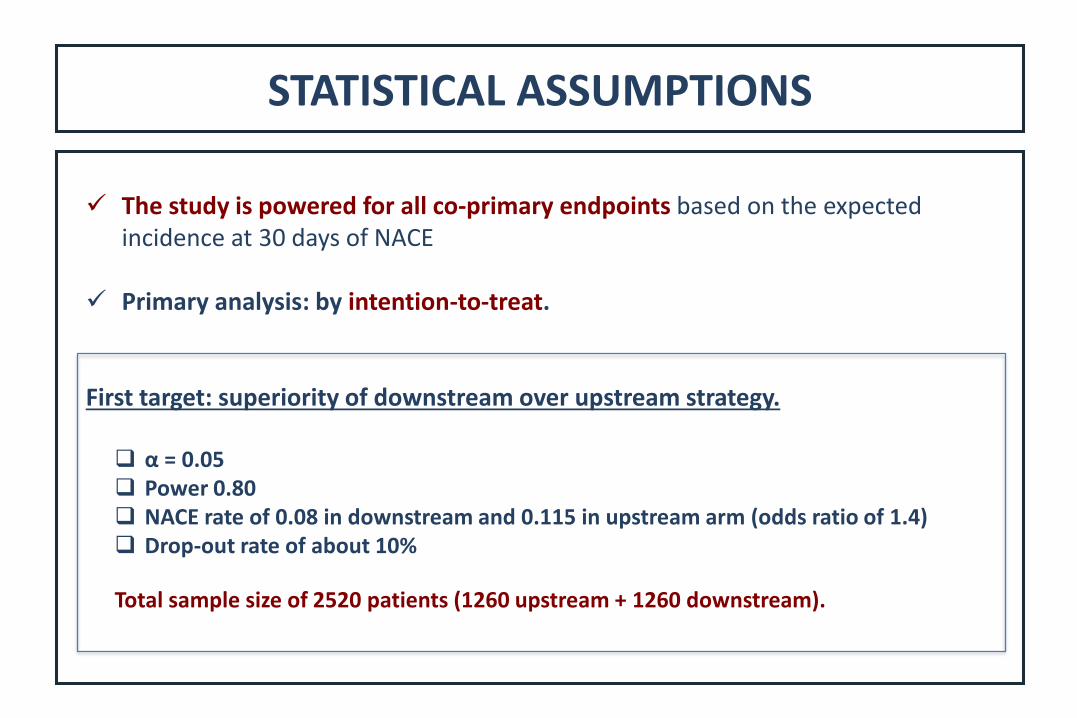
STATISTICAL ASSUMPTIONS
✓ The study is powered for all co-primary endpoints based on the expectedincidence at 30 days of NACE
✓ Primary analysis: by intention-to-treat.
First target: superiority of downstream over upstream strategy.
α = 0.05 Power 0.80 NACE rate of 0.08 in downstream and 0.115 in upstream arm (odds ratio of 1.4) Drop-out rate of about 10%
Total sample size of 2520 patients (1260 upstream + 1260 downstream).
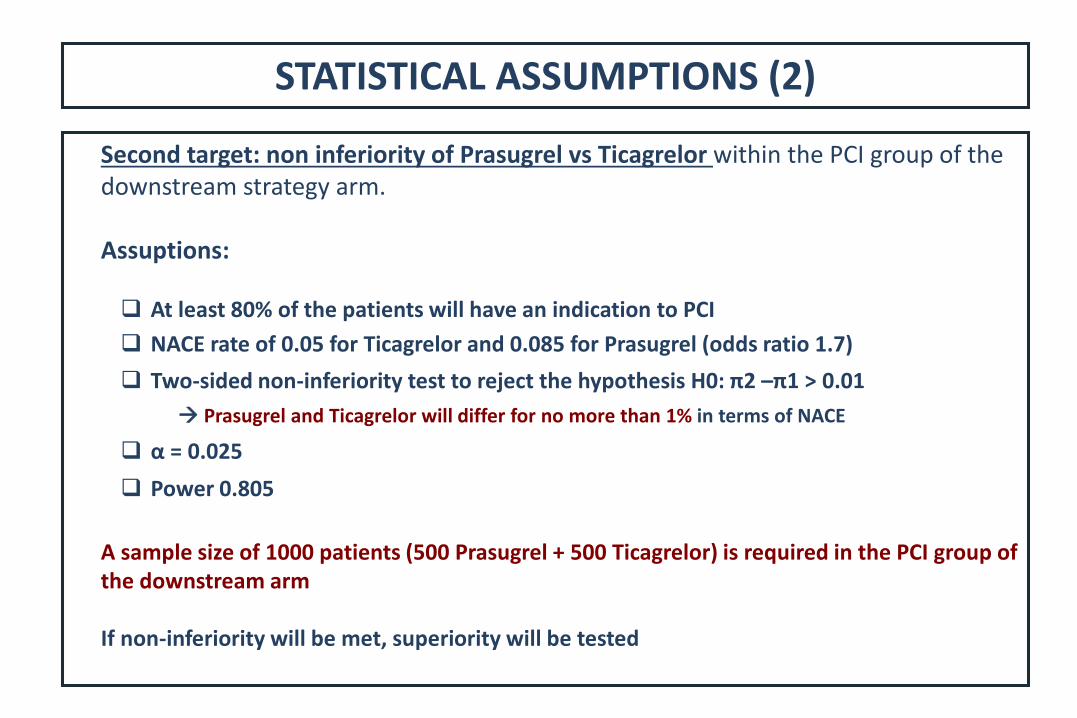
STATISTICAL ASSUMPTIONS (2)
Second target: non inferiority of Prasugrel vs Ticagrelor within the PCI group of the downstream strategy arm.
Assuptions:
At least 80% of the patients will have an indication to PCI
NACE rate of 0.05 for Ticagrelor and 0.085 for Prasugrel (odds ratio 1.7)
Two-sided non-inferiority test to reject the hypothesis H0: π2 –π1 > 0.01
Prasugrel and Ticagrelor will differ for no more than 1% in terms of NACE
α = 0.025
Power 0.805
A sample size of 1000 patients (500 Prasugrel + 500 Ticagrelor) is required in the PCI group of the downstream arm
If non-inferiority will be met, superiority will be tested
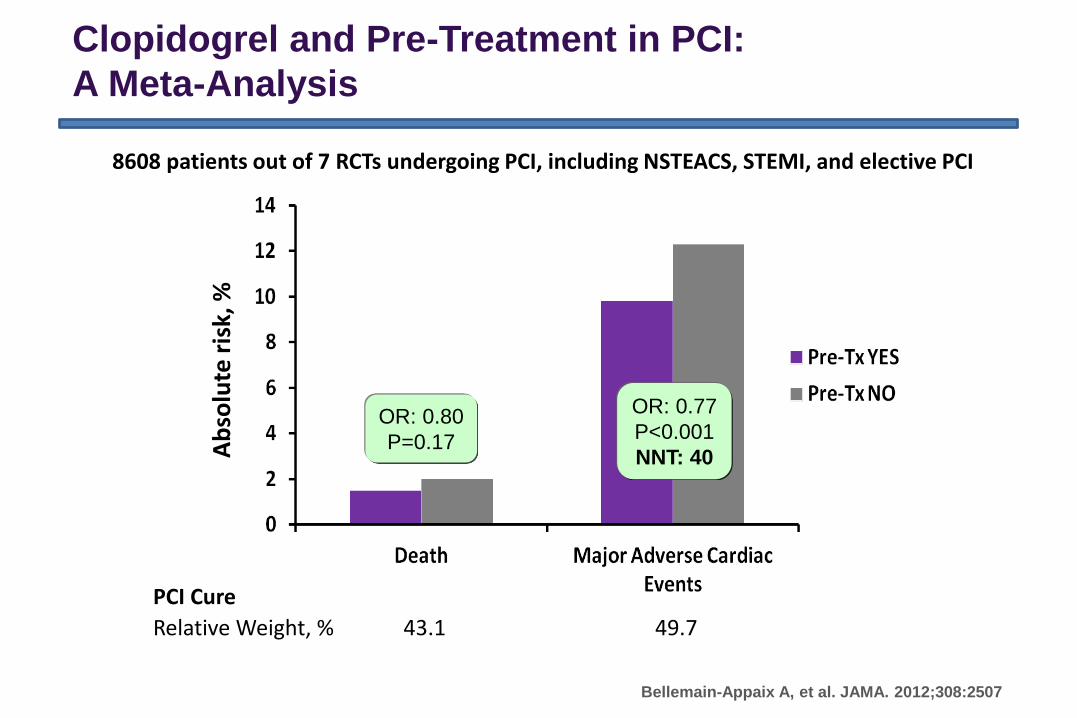
Clopidogrel and Pre-Treatment in PCI:
A Meta-Analysis
8608 patients out of 7 RCTs undergoing PCI, including NSTEACS, STEMI, and elective PCI
PCI Cure
Relative Weight, % 43.1 49.7
Bellemain-Appaix A, et al. JAMA. 2012;308:2507
Ab
solu
te r
isk,
%
OR: 0.80
P=0.17
OR: 0.77
P<0.001
NNT: 40

0.4 0.6 0.8 1.0 1.2
Hazard Ratio (95% CI)
RRR: –13.4%
p=0.60
RRR: 38.6%
p=0.05
RRR: 18.5%
P=.23CREDO Overall
Steinhubl SR, et al. JAMA. 2002;288:2411
CREDO Study: Timing of
Loading Dose and 28-Day Endpoint
Timing N Pretreat No Pretreat
3–<6 h 893 7.9 7.0
≥6–24h 851 5.8 9.4
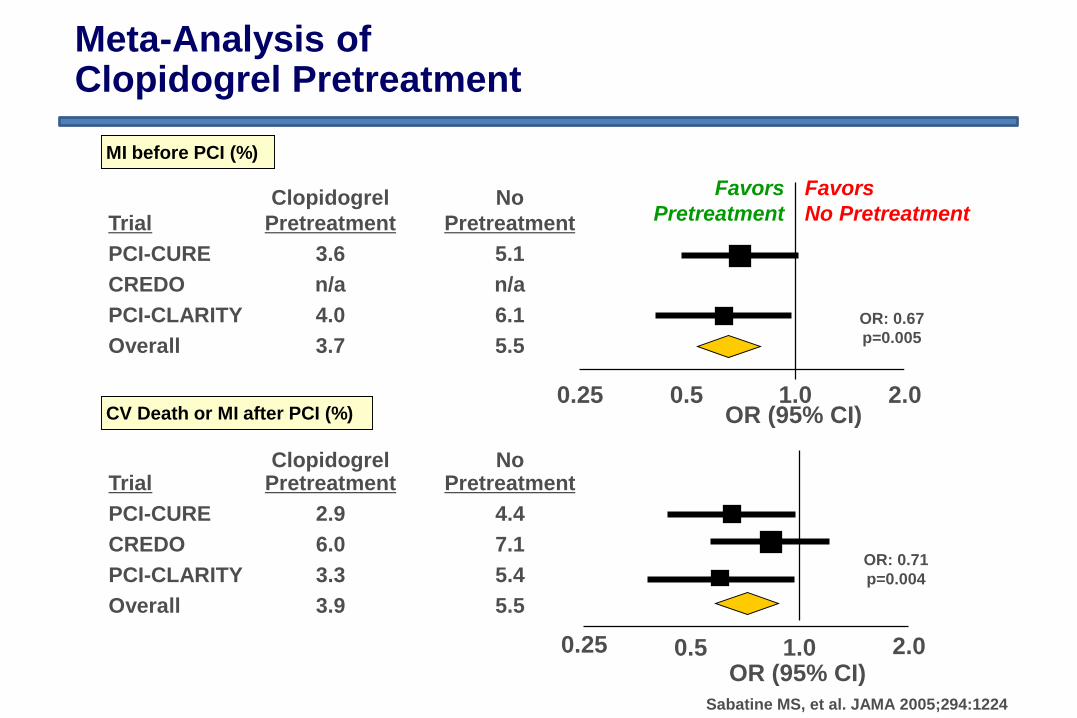
Clopidogrel No
Trial Pretreatment Pretreatment
PCI-CURE 3.6 5.1
CREDO n/a n/a
PCI-CLARITY 4.0 6.1
Overall 3.7 5.5
Meta-Analysis of Clopidogrel Pretreatment
CV Death or MI after PCI (%)
MI before PCI (%)
1.00.25 2.00.5
1.00.25 2.00.5OR (95% CI)
OR (95% CI)
OR: 0.67
p=0.005
Favors
Pretreatment
Favors
No Pretreatment
OR: 0.71
p=0.004
Sabatine MS, et al. JAMA 2005;294:1224
Clopidogrel NoTrial Pretreatment Pretreatment
PCI-CURE 2.9 4.4
CREDO 6.0 7.1
PCI-CLARITY 3.3 5.4
Overall 3.9 5.5

Bellemain-Appaix A, et al. JAMA. 2012;308:2507
Clopidogrel and Pre-Treatment in PCI:
A Meta-Analysis
STABLE
ACS


















