Transthyretin(TTR) amyloidosis
20
Boston Medical Center is the primary teaching affiliate of the Boston University School of Medicine. Transthyretin (TTR) Amyloidosis Frederick L. Ruberg, MD Amyloidosis Center and Section of Cardiovascular Medicine Boston University School of Medicine Boston Medical Center Boston, MA
-
Upload
drucsamal -
Category
Healthcare
-
view
799 -
download
0
Transcript of Transthyretin(TTR) amyloidosis

Boston Medical Center is the primary teaching affiliate
of the Boston University School of Medicine.
Transthyretin (TTR) Amyloidosis
Frederick L. Ruberg, MD
Amyloidosis Center and Section of Cardiovascular Medicine
Boston University School of Medicine
Boston Medical Center
Boston, MA

OVERVIEW OF TTR AMYLOIDOSIS
• Amyloidosis is a disorder of protein folding
• Classification of amyloid type by precursor protein
• Transthyretin (TTR) aka prealbumin 55 k-Da protein
synthesized by liver > 100 known SNPs
• Mutations alter thermodynamic properties of protein to favor
mis-folding and aggregation as amyloid fibrils
– Variant TTR amyloidosis
– Autosomal dominant inheritance pattern (50% likelihood of
transmission)
Connors, Amyloid 2003

KEY POINTS TO REMEMBER 1. Variant TTR amyloidosis results from single nucleotide
polymorphisms (SNPs) that cause nerve, cardiac, and soft tissue amyloid fibril deposition (alone or in combination)
2. Mutations vary by geographic distribution thus ancestry can predict mutation
3. Penetrance is incompletely understood however there are clear gender and age associations with phenotypic expression
4. Clinically it can be difficult to distinguish variant TTR from ATTRwt, but easier to differentiate from AL
5. Novel approaches using TTR stabilization or suppression agents hold great promise to treat variant TTR disease

TTR STRUCTURE AND FIBRIL FORMATION
Bulawa et al. PNAS 2012

CLINICAL MANIFESTATIONS OF VARIANT TTR
AMYLOIDOSIS
Variant TTR amyloidosis
Restrictive Cardiomyopathy
(FAC)
V122I
T60A
Autonomic and peripheral
Neuropathy (FAP) V30M
Mutation

Ruberg, Circulation 2012
FEATURES OF TTR CARDIAC AMYLOIDOSIS

DIAGNOSIS OF VARIANT TTR CARDIAC
AMYLOIDOSIS 1. Clinical suspicion and recognition!
2. Tissue biopsy to identify amyloid by Congo red stain – Abdominal fat aspirate (20-25% sensitive for ATTRwt, 50-75%
sensitive for ATTRvariant)
– Endomyocardial biopsy (virtually 100% sensitive/specific)
3. Typing of amyloid by analysis of biopsy specimen – Immunohistochemistry (problematic high background)
– Mass spectrometry (Mayo Medical Labs send out)
4. Genetic testing to establish TTR genotype – Blood test - PCR
5. Exclusion of plasma cell dyscrasia
Connors Amyloid 2009

CLASSIC ECHO FINDINGS IN VARIANT TTR
AMYLOIDOSIS
Can non-invasive testing conclusively differentiate amyloid type?

ECG IN DIFFERENT AMYLOID TYPES
Rapezzi Circulation 2009

ECHOCARDIOGRAPHY IN DIFFERENT AMYLOID TYPES
Rapezzi Circulation 2009
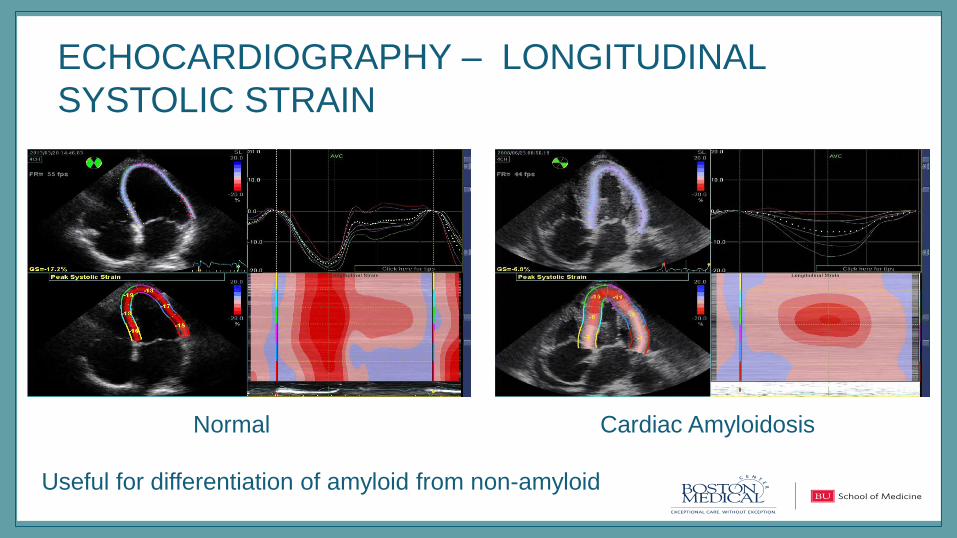
ECHOCARDIOGRAPHY – LONGITUDINAL
SYSTOLIC STRAIN
Normal Cardiac Amyloidosis
Useful for differentiation of amyloid from non-amyloid

CMR: DIFFERENTIATION OF TTR VS. AL
Dungu JACC Img 2014
ICC = 0.66 (only fair agreement)
QALE score sensitivity 87%, specificity 96%

CMR: NATIVE (NON-CONTRAST) T1 MAPPING
Fontana JACC Img 2014

NUCLEAR IMAGING: SELECTIVE FOR TTR • Tc-99m Bone avid compounds
– Pyrophosphate (PYP) and DPD
– May preferentially identify TTR amyloid cardiomyopathy
Rapezzi Eur J Nuc Med Mol Imag 2011, JACC Img 2011: Banypersad, JAHA 2012
Bokhari Circ CV Imaging 2013: Longhi JACC Img 2014

PROGNOSIS: VARIANT TTR DUE TO V122I
• Mutation seen in 4% African Americans
– 1 million African Americans with mutation
– Approximately 100,000 over age 65y at risk
• Increased risk of CHF in cohort studies
• Median survival is 24-27 months following diagnosis
– Prospective multi-center TRACS (Transthyretin Amyloidosis Cardiac Study)
Jacobson NEJM 1997: Buxbaum AHJ 2010: Connors AHJ 2009: Ruberg AHJ 2012

LONGITUDINAL ASSESSMENT OFV122I ALLELE
STATUS, SURVIVAL AND HEART FAILURE • ARIC study of roughly 3850 African Americans
• V122I found in 3%, carriers vs. non-carriers compared after
25 years for survival, heart failure, and echo findings
Quarta et al, NEJM 2015
CHF curves diverge at 70 years
Limited # of older male carriers

MANAGEMENT OF VARIANT TTR AMYLOID • Medical treatments for heart failure
– Midodrine for orthostasis from autonomic neuropathy
• Liver transplant alone in TTR variant amyloid cardiomyopathy
is ineffective owing to continued progression despite wild-type
TTR
• Emerging medical treatments for TTR amyloid
– Stabilization
– Suppression

MANAGEMENT OF TTR AMYLOID: DIFLUNISAL • Currently available, FDA approved, but off-label usage
• Non-steroidal, inexpensive, oral, reversible inhibitor of TTR aggregation
• Efficacy dramatically demonstrated in neuropathic symptoms in TTR polyneuropathy, data regarding efficacy in TTR cardiomyopathy not yet reported
• Can be safely administered in patients with TTR (wt and variant) cardiomyopathy
• Limited by GI bleeding risk, heart failure risk, and nephrotoxicity
Berk et al, JAMA 2013: Castano, Congest Heart Fail 2012

INVESTIGATIONAL THERAPEUTICS FOR
VARIANT TTR AMYLOID CARDIOMYOPATHY Agent Mechanism Trial Identifier Design Endpoint Comments
Tafamidis stabilization ATTR-
ACT/Pfizer
NCT
01994889
20 mg vs. 80
mg vs.
placebo
All-cause
mortality +
cardiovasc.
hospitalization
PO daily for
30 months
Revusiran Suppression
(RNAi)
ENDEAVOR/A
lnylam
NCT
02319005
500 mg vs.
placebo
6 min walk
duration
SC weekly for
18 months
Patisiran Suppression
(RNAi)
APOLLO/Alnyl
am
NCT
01960348
Active drug
vs. placebo
NIS+7 score IV weekly for
18 months
ISIS-TTR-Rx Suppression
(Antisense
ODN)
ISIS NCT
01737398
300 mg vs.
placebo
NIS+7 score SC weekly for
65 weeks
SUMMARY • While sharing precursor protein with TTRwt, variant TTR
amyloidosis has a dramatically different and variable
phenotypic expression (heart/nerve) and disease course
– V122I may substantively contribute to heart failure in African
Americans
• Medical treatments overlap and may be equally effective
• Diagnosis involves genetic testing AND tissue identification,
though robustness of PYP/DPD nuclear scan data is altering
perception
– Biomarker discovery ongoing