
Transpupillary thermotherapy in the management of circumscribed choroidal hemangioma
12
SURVEY OF OPHTHALMOLOGY VOLUME 49 • NUMBER 3 • MAY–JUNE 2004 DIAGNOSTIC AND SURGICAL TECHNIQUES MARCO ZARBIN AND DAVID CHU, EDITORS Transpupillary Thermotherapy in the Management of Circumscribed Choroidal Hemangioma Kaan Gu ¨ndu ¨z, MD Ocular Oncology Service, Department of Ophthalmology, Ankara University Faculty of Medicine, Ankara, Turkey Abstract. Laser photocoagulation and various radiation therapy methods have been used in the treatment of circumscribed choroidal hemangioma that produce visual loss. Recently, transpupillary thermotherapy has been employed in the management of choroidal hemangioma. Thirty-six cases of choroidal hemangioma treated with transpupillary thermotherapy are reviewed. Twenty-eight cases were reported in the literature and 10 cases were managed by the author. Transpupillary thermotherapy has been used as a primary treatment (36 cases) or secondary treatment (2 cases) for choroidal hemangioma. The goal of transpupillary thermotherapy is to achieve resolution of exudative detachment of the fovea and improvement of vision. In all eyes the foveal detachment subsided. In 26 eyes having pretreatment visual acuity 0.05 (20/400), the visual acuity increased in 20 (77%) eyes and remained unchanged in 6 (23%) eyes. After transpupillary thermotherapy, 16 (42%) cases showed complete regression, 20 (53%) demonstrated partial regression, and in 2 (5%) there was no change in tumor thickness at follow-ups ranging from 2 to 44 months. Complications of transpupillary thermotherapy of choroidal hemangioma included cystoid macular edema (3 eyes), preretinal fibrosis (2 eyes), focal iris atrophy (3 eyes), and retinal vascular occlusion (1 eye). Although the follow-up in many studies is limited, transpupillary thermotherapy has not been associated with any significant complications. (Surv Ophthalmol 49:316–327, 2004. 2004 Elsevier Inc. All rights reserved.) Key words. age-related macular degeneration • choroidal hemangioma • choroidal melanoma • cystoid macular edema • epiretinal membrane • laser photocoagulation • photodynamic therapy • radiation therapy • retinal capillary hemangioma • retinoblastoma • transpupillary thermotherapy • visual fields Introduction Choroidal hemangioma is a benign vascular tumor. It is generally believed that the tumor is present at birth or develops by early adulthood. In time, it produces visual symptoms leading to clinical recogni- tion. Choroidal hemangioma can be classified in two forms: a diffuse type and a circumscribed type based on the extent of choroidal involvement. 38,41 The diffuse choroidal hemangioma is associated with 316 2004 by Elsevier Inc. 0039-6257/04/$–see front matter All rights reserved. doi:10.1016/j.survophthal.2004.02.009 Sturge-Weber syndrome. The circumscribed choroi- dal hemangioma (CCH) is usually a sporadic tumor not associated with any systemic manifestations, al- though it can rarely be associated with Sturge-Weber syndrome or its variations, probably representing a limited form of the syndrome. On funduscopy, CCH presents as an orange-red mass. A- and B-mode ultrasonography show that the CCH has a dome shape, medium to high reflectivity,
-
Upload
kaan-guenduez -
Category
Documents
-
view
216 -
download
0
Transcript of Transpupillary thermotherapy in the management of circumscribed choroidal hemangioma

SURVEY OF OPHTHALMOLOGY VOLUME 49 • NUMBER 3 • MAY–JUNE 2004
DIAGNOSTIC AND SURGICAL TECHNIQUESMARCO ZARBIN AND DAVID CHU, EDITORS
Transpupillary Thermotherapy in the Managementof Circumscribed Choroidal HemangiomaKaan Gunduz, MD
Ocular Oncology Service, Department of Ophthalmology, Ankara University Faculty of Medicine, Ankara, Turkey
Abstract. Laser photocoagulation and various radiation therapy methods have been used in thetreatment of circumscribed choroidal hemangioma that produce visual loss. Recently, transpupillarythermotherapy has been employed in the management of choroidal hemangioma. Thirty-six cases ofchoroidal hemangioma treated with transpupillary thermotherapy are reviewed. Twenty-eight caseswere reported in the literature and 10 cases were managed by the author. Transpupillary thermotherapyhas been used as a primary treatment (36 cases) or secondary treatment (2 cases) for choroidalhemangioma. The goal of transpupillary thermotherapy is to achieve resolution of exudative detachmentof the fovea and improvement of vision. In all eyes the foveal detachment subsided. In 26 eyes havingpretreatment visual acuity �0.05 (20/400), the visual acuity increased in 20 (77%) eyes and remainedunchanged in 6 (23%) eyes. After transpupillary thermotherapy, 16 (42%) cases showed completeregression, 20 (53%) demonstrated partial regression, and in 2 (5%) there was no change in tumorthickness at follow-ups ranging from 2 to 44 months. Complications of transpupillary thermotherapyof choroidal hemangioma included cystoid macular edema (3 eyes), preretinal fibrosis (2 eyes), focaliris atrophy (3 eyes), and retinal vascular occlusion (1 eye). Although the follow-up in many studies islimited, transpupillary thermotherapy has not been associated with any significant complications. (SurvOphthalmol 49:316–327, 2004. � 2004 Elsevier Inc. All rights reserved.)
Key words. age-related macular degeneration • choroidal hemangioma • choroidal melanoma •cystoid macular edema • epiretinal membrane • laser photocoagulation • photodynamictherapy • radiation therapy • retinal capillary hemangioma • retinoblastoma • transpupillarythermotherapy • visual fields
IntroductionChoroidal hemangioma is a benign vascular tumor.
It is generally believed that the tumor is presentat birth or develops by early adulthood. In time, itproduces visual symptoms leading to clinical recogni-tion. Choroidal hemangioma can be classified in twoforms: a diffuse type and a circumscribed type basedon the extent of choroidal involvement.38,41 Thediffuse choroidal hemangioma is associated with
Sdntsl
mC
316
� 2004 by Elsevier Inc.All rights reserved.
turge-Weber syndrome. The circumscribed choroi-al hemangioma (CCH) is usually a sporadic tumorot associated with any systemic manifestations, al-
hough it can rarely be associated with Sturge-Weberyndrome or its variations, probably representing aimited form of the syndrome.
On funduscopy, CCH presents as an orange-redass. A- and B-mode ultrasonography show that theCH has a dome shape, medium to high reflectivity,
0039-6257/04/$–see front matterdoi:10.1016/j.survophthal.2004.02.009

TRANSPUPILLARY THERMOTHERAPY 317
and acoustic solidity.35,38 Fibrous or osseous metapla-sia on the tumor surface, if present, may producehigher reflectivity and may lead to orbital shadow-ing.38 Fluorescein angiography shows early fluores-cence in the prearterial and arterial phase followedby moderate hyperfluorescence in the venous phaseand increasing hyperfluorescence in the late phase.35
There may be leakage into the subretinal space inthe late frames. Indocyanine green angiography dem-onstrates extreme hyperfluorescence in the earlyframe by about 1 minute followed by moderate hyper-fluorescence in the middle and late frames (at ap-proximately 8 and 20 minutes respectively).35 Thisearly hyperfluorescence followed by relative hypoflu-orescence has been referred to as the washout phe-nomenon and is characteristic for CCH.32 Thiswashout phenomenon has not been observed withother intraocular tumors.32
CCH can cause visual loss through a variety ofassociated conditions, including exudative retinal de-tachment, cystoid macular edema, subretinal fibrosis,subfoveal tumor location, and, rarely, neovascularglaucoma.1,41 Asymptomatic CCH not causing visualloss does not require treatment and can be observedperiodically. CCH that produces visual loss due tosubretinal fluid has been treated by transscleral cry-opexy, diathermy, photocoagulation, or radiother-apy. Photocoagulation and radiotherapy havebecome more popular than other modalitiesbecause of their efficacy and ease of applicability.However, these two methods have certain disadvan-tages in the treatment of CCH. As a result, therehas been interest in alternative treatment methods,including photodynamic therapy (PDT)2,11,17,27,29,31
and transpupillary thermotherapy (TTT).7,8,12,20,22,24
Treatment options for diffuse choroidal hemangi-oma producing exudative retinal detachment in-clude laser photocoagulation and external beamradiotherapy. If the exudative retinal detachment isextensive, vitrectomy, gas injection, and endophoto-coagulation may become necessary.16,28,38 Diffusechoroidal hemangioma is not a good candidate forPDT or TTT, which are used for localized lesions.
The purpose of this article is to review the currentstatus of TTT in the management of CCH. Search ofthe Internet library of medicine through the PubMeddatabase revealed six reports published on the sub-ject to date in the English literature.7,8,12,20,22,24 Datafrom the 28 cases reported in these papers are com-bined with data from 10 cases managed by the authorto provide an overview of 38 cases of CCH treatedwith TTT.
Treatment Methods Used forCircumscribed Choroidal HemangiomaLaser photocoagulation is used to eliminate subret-
inal fluid.1,37 It does not cause regression of the
caMcpµaooLisse
c(p(Sle
tlsodmosn
tpeadfu1sw
R
caCimaocl
horoidal hemangioma. In the past, xenon photoco-gulation was used to treat choroidal hemangioma.ore recently, argon laser and diode laser photo-
oagulation have been used.1,13,16 A scatter laserhotocoagulation technique is used with a 200–500m spot size, 0.5–1.0 second duration, and moder-tely intense power to produce a white color changen the tumor. The burns are placed one-half tone burn-width apart over the entire tumor surface.aser photocoagulation should probably not be used
n subfoveal CCH because of the poor visual progno-is associated with treatment at this location.28 Ithould also not be used in CCH associated withxtensive overlying subretinal fluid.Madreperla and coworkers used argon laser photo-
oagulation to treat 13 eyes with CCH.16 In four eyes31%), the visual acuity remained unchanged or im-roved after laser photocoagulation. Three eyes23%) had improved visual acuity by three or morenellen lines at 1 year after treatment. Complete reso-ution of subretinal fluid was noted in six of 13yes (46%).16
Anand and associates reported 64 cases of CCHreated with xenon and laser photocoagulation.1 Fol-owing photocoagulation, the subretinal fluid re-olved in all eyes. Visual acuity improved in 20%f the patients, remained unchanged in 53%, andecreased in 27% at a median follow-up of 46onths, ranging from 6 weeks to 12 years. In 24 out
f 64 eyes in this study, subsequent reaccumulation ofubretinal fluid was noted in 10 eyes (40%), whichecessitated additional laser treatments.1
Multiple laser treatments may result in damageo the retinal structures especially the nerve fibersroducing visual field defects.13 Lanzetta and cowork-rs pointed out that by virtue of its longer wavelengthnd deeper penetration, diode laser may cause lessamage to the inner retinal layers including the nerve
ibers.13 These authors treated two eyes with CCHsing diode laser photocoagulation. At follow-ups of2 and 16 months, exudative retinal detachment re-olved in both eyes. The visual acuity in both eyesere improved by two or more Snellen lines.
ADIATION THERAPY
Various modes of radiation therapy, including epis-leral plaque radiotherapy, external beam irradiation,nd proton beam irradiation, have been used to treatCH.9,15,16,25,28,42 Radiation therapy is generally used
n the presence of extensive, bullous retinal detach-ent, in which laser photocoagulation can not be
pplied. Furthermore, radiation therapy is preferredver laser photocoagulation for subfoveal CCH be-ause of the poor visual prognosis associated withaser photocoagulation treatment at this location.28,42

318 Surv Ophthalmol 49 (3) May–June 2004 GUNDUZ
Episcleral Plaque Radiotherapy
In episcleral plaque radiotherapy (brachytherapy),a radioactive plaque is placed over the tumor. Theplaque is left in place until it delivers the desiredradiation dose to the tumor in the specified timeperiod. Episcleral plaque radiotherapy provides aconvenient means for irradiating the tumor with littleradiation given to the surrounding tissues. Zografosand coworkers treated 39 eyes having CCH and twoeyes having diffuse choroidal hemangioma, usingCobalt-60 episcleral plaque radiotherapy with anapex dose of 40–60 Gy.42 They reported retinal reat-tachment and complete regression of the choroidalhemangioma in all eyes. Mild radiation retinopathyin three eyes (8%) was the only radiation-related sideeffect. Visual acuity equal to or better than 20/200was present in 38 of 41 eyes (93%) at baseline, in 25of 31 eyes (81%) at 2 years, in 14 of 19 eyes (74%)at 5 years, and in 5 of 8 eyes (63%) at 10 years.42
Madreperla and associates treated eight eyes withCCH using either Iodine-125 or Ruthenium-106 epis-cleral plaque radiotherapy with an apex dose of 50Gy.16 They reported retinal reattachment and de-crease in tumor thickness in all eyes. No radiationcomplication was reported. Visual acuity improvedby three or more Snellen lines in five (63%) eyes at1 year. The authors concluded that there was a trendtoward better vision with episcleral plaque radiother-apy than with laser photocoagulation, although thiswas not statistically significant.16
Ritland and associates treated one case of CCHusing Ruthenium-106 episcleral plaque brachyther-apy with an apex dose of 25 Gy.25 This is the lowesttumor apex radiation dose that has been reportedfor plaque radiotherapy of CCH in the literature.Following plaque radiotherapy, the tumor demon-strated decrease in thickness and the visual acuityremained unchanged at a follow-up of 4.3 years.25
External Beam Radiotherapy
External beam radiotherapy has been the firstchoice of treatment for circumscribed and diffusechoroidal hemangioma in many centers. A totaldose of 12–24 Gy is delivered with conventional exter-nal beam radiotherapy25,28 or recently with stereotac-tic irradiation. With stereotactic irradiation, multiplehighly collimated beams converge on the tumor fromdifferent locations around the eye, either concur-rently or subsequently. The treatment can be givenin several fractions or in a single fraction.
Schilling and coworkers used external beam radio-therapy with a total dose of 20 Gy to treat 36 eyes withCCH.28 A lateral lens-sparing technique was used. In23 eyes (64%), retinal reattachment was achieved.No radiation complication was noted. Visual acuity
iettaad
uddttsa
epdbGt
P
vtemss1AwtttS
atTaaoptcalich
mproved in 14 eyes (39%), remained stable in 14yes (39%), and decreased in 8 eyes (22%). Tumorhickness did not change after external beam radio-herapy; however, eyes that received supplementalrgon laser photocoagulation to the tumor surfacefter external beam radiotherapy demonstrated aecrease in tumor thickness.28
Ritland and associates treated 8 eyes with CCHsing lens-sparing external beam radiotherapy (totalose 20–24 Gy).25 In all cases, the tumor thicknessecreased with resolution of the exudative retinal de-
achment. Visual acuity improved in all 8 eyes afterreatment. There were no radiation complicationsuch as cataract, retinopathy, and optic neuropathyt follow-up periods ranging from 0.4 to 8.8 years.25
Radiation cataract is a potential complication ofxternal beam radiotherapy. Scott and associates re-orted that cataract developed in 2 of 4 eyes havingiffuse choroidal hemangioma treated with externaleam radiotherapy using an apex dose of 12 to 19y.30 A lens-sparing technique was not employed in
his study.30
roton Beam Radiotherapy
Proton beam (charged particle) radiotherapy pro-ides a homogenous dose of radiation to the entireumor while sparing surrounding structures. Thisffect is based on the principle that protons induceost tissue damage at the tumor level where they
low down (Bragg peak) with relative sparing of theuperficial tissues. Hannouche and associates treated3 eyes having CCH with proton beam irradiation.9
total dose of 30 Cobalt-Gray-Equivalent (CGE)as administered to each eye in four doses. The au-
hors reported retinal reattachment and decrease inumor thickness in all eyes. No radiation complica-ion was seen. Visual acuity improved by two or morenellen lines in 8 eyes (62%).9
Lee and Hungerford treated 3 eyes having macularnd juxtapapillary CCH using proton beam irradia-ion with a dose of 19.8 CGE in four fractions.15
he tumor regressed completely in all patients. Visualcuity improved in only one of three (33%) patientsfter treatment. Two patients developed radiationptic neuropathy and maculopathy, and one had aersistent exudative retinal detachment following
reatment. The high complication rate, which is inontrast to that found in the study of Hannouchend associates,9 was interesting. The authors specu-ated that increased vascularity of CCH may causencreased absorption leading to radiation-relatedomplications or that the dose fractionation may notave been adequate.15

TRANSPUPILLARY THERMOTHERAPY 319
Disadvantages and Side Effectsof Radiation Therapy
The various radiation therapy methods providegood tumor control with no serious radiation compli-cations in the treatment of CCH. However, some ofthese methods have certain disadvantages. First, someof the radiotherapy methods including proton beamradiotherapy and stereotactic irradiation are expen-sive and are not widely available. Second, some radio-therapy methods require surgery. Episcleral plaqueradiotherapy requires two operations, one to insertand the other to remove the radioactive plaque.42
With proton beam irradiation, it is necessary to surgi-cally position the radio-opaque tantalum markers toindicate the tumor position.9 Third, radiation sideeffects such as cataract and retinopathy can occur,although they are rare in the low doses typically usedto treat CCH. Fourth, additional treatment methods,such as argon laser photocoagulation, may becomenecessary at a later date. In five eyes (14%) treatedwith low-dose fractionated lens-sparing externalbeam irradiation (apex dose 20 Gy), additional laserphotocoagulation was required subsequently becauseof recurrent or residual subretinal fluid.28
PHOTODYNAMIC THERAPY
Because of the various disadvantages of argon laserphotocoagulation and radiation therapy in the treat-ment of CCH, there has been interest in the use ofalternative treatment methods. PDT represents onesuch treatment method. PDT allows selective occlu-sion of vascular lesions without damaging the adja-cent retinal structures and causing nerve fiber bundledefects.2,11,17,27,29,31 The photosensitizer binds to low-density lipoproteins (LDL), allowing selective tar-geting of the tumor endothelium, which expresseslarge quantities of LDL receptors. One current disad-vantage of PDT is the expense of the photosensitizerdye used.
In their pioneering study, Barbezotto and Schmidt-Erfurth treated 2 eyes having CCH with PDT usingverteporfin (BPD-MA).2 One eye was treated twiceand the other eye four times to achieve total tumoreradication and complete resolution of the subretinalfluid and cystoid macular edema (CME).2 In a laterreport, Madreperla pointed out that the end-pointof treatment in PDT is not total tumor eradication.17
He indicated that once the tumor stops leaking, fur-ther treatment is unnecessary. Madreperla treated 3eyes having CCH with a single session of PDT usingverteporfin.17 The subretinal fluid resolved com-pletely in all eyes 2 weeks after a single treatment,leading to increase in visual acuity with decreasein tumor thickness compared to baseline.17 Robertsonreported 3 eyes with CCH that were treated with
PerWdade
aw6tRrsShtrn
metlter
T
tbtbcattimaasce
c
PI
d
DT.27 Two eyes received two treatments and oneye was treated once. In all eyes, the subretinal fluidesolved and the tumor regressed completely.27
hereas Barbezotto and Schmidt-Erfurth2 used aose level of 100 J/cm2, Robertson,27 Madreperla17
nd Sheidow and Harbour31 employed the standardose of 50 J/cm2, as in the age-related macular degen-ration study.40
In a recent report on the subject, Schmidt-Erfurthnd associates discussed the results of PDT in 15 eyesith CCH. One to four treatments were applied at-week intervals.29 The authors treated CCHs with aumor thickness ranging from 2.0 mm to 6.2 mm.etreatment was applied when persistent leakage and
esidual tumor were documented clinically and ultra-onographically. A light dose of 100 J/cm2 was used.chmidt-Erfurth and associates indicated that thisigher light dose was more appropriate considering
he increased thickness of the vascular lesion in cho-oidal hemangioma compared with the choroidaleovascular membrane.29
Jurklies and coworkers used PDT as primary treat-ent in 15 eyes and as secondary treatment in 4
yes with CCH.11 PDT was successful in 4 secondarilyreated eyes in which previous treatments includingaser photocoagulation and external beam irradia-ion had failed. This demonstrates that PDT is a pow-rful tool available for tumors not responding toadiotherapy.11
RANSPUPILLARY THERMOTHERAPY
Transpupillary thermotherapy is a relatively newreatment method that uses diode laser with a broadeam and long exposure times. It has been used inhe management of choroidal melanoma,33 retino-lastoma,34 retinal capillary hemangioma,23 andhoroidal neovascularization (occult and classic) inge-related macular degeneration.21 Transpupillaryhermotherapy causes the temperature in the treatedissue to rise to 42–60�C as a result of heat uptaken the retinal pigment epithelial cells and choroidal
elanocytes.10 At the temperature level typicallychieved with TTT, which is lower than with photoco-gulation, cytolysis and ischemic necrosis developecondary to mitochondrial breakdown.6,10 Thesehanges occur both in tumor cells and in vascularndothelium.Recently, TTT has been used to treat CCH, as dis-
ussed below.
Transpupillary Thermotherapy forCircumscribed Choroidal Hemangioma
ROPOSED MECHANISM OF ACTION OF TTTN CCH
Transpupillary thermotherapy produces heat-in-uced sclerosis of the vascular channels in CCH,

320 Surv Ophthalmol 49 (3) May–June 2004 GUNDUZ
leading to tumor regression and resolution of theassociated subretinal fluid.22 Although previous stud-ies shed some light on the histopathologic effects ofTTT,6,10 mechanisms of TTT-induced vasculardamage and occlusion are not fully understood.
HISTOPATHOLOGIC EFFECTS OF TTT
There are no histopathologic samples of eyeshaving CCH treated with TTT. The determinationof the histopathologic effects of TTT is made fromstudies on eyes with choroidal melanoma. Histopa-thologically, TTT-treated melanomas demonstrateextensive thrombosis of tumor vessels.10 This throm-bosis, in addition to cytolysis of tumor cells and vascu-lar endothelium (as discussed above), contributes totumor necrosis. In a histopathologic study, tissue ne-crosis up to a depth of 3.9 mm from the surface ofthe tumor has been reported to develop after TTTof choroidal melanoma.10
The retina is vulnerable to the damaging effects ofhyperthermia. Singh and associates reported that ir-reparable rhegmatogenous retinal detachment de-veloped in one case of choroidal melanoma due tocomplete atrophy of the retina after TTT.39 Connollyand coworkers studied the effect of TTT on thenormal human retina in three eyes enucleated forlarge choroidal melanoma.4 Considering theTTT4CNV trial power/spot diameter ratio of 267mW/mm, they applied power settings of 430 mW,530 mW, and 630 mW (low, medium, and high doses,respectively) with a 2 mm spot size. The authors foundthat TTT produces mild or no change on the outersensory retina in most low or medium-dose TTT ap-plications. Sensory retinal damage is more likely tooccur with high-dose TTT applications or when thefundus is heavily pigmented (either naturally orpathologically as with a choroidal melanoma).4
In contrast to the retina and choroid, the sclerais known to be resistant to the effects of hyperther-mia.39 Although complete regression of the choroidalmelanoma is achieved with TTT, melanoma cellshidden in the posterior intrascleral emissary canals orscleral lamellae may activate causing intraocular orextraocular tumor recurrence.39
ANGIOGRAPHIC CHANGES AFTER TTT
Lanzetta and coworkers studied the vascularchanges induced by TTT on subfoveal choroidalneovascularization and choroidal vasculature in 64eyes, using fluorescein angiography and indocyaninegreen angiography.14 The authors observed in-creased leakage of choroidal neovascularization andchoroidal vessels within 1 hour after TTT.14 Follow-up at 1 and 2 weeks showed hypofluorescence andabsence of leakage on angiography. At 4 weeks after
Thtatdolpiltaardhadsianiooe
paeswstsotussTe
iwawriAacaTp
TT, fluorescein angiography demonstrated mottledypofluorescence-hyperfluorescence of the TTT-
reated areas and absence of leakage. Based on thesengiographic findings, the authors hypothesized thathe mechanism leading to vessel closure begins withamage to endothelial cells during the hyperthermiaf target tissue. Endothelial cell damage leads to re-
ease of vasoactive molecules and increase in vascularermeability.14 Hypofluorescence at 1 and 2 weeks
s due to hypoperfusion of the choroidal neovascu-arization and choriocapillaris. It could also be dueo extensive thrombosis or exudate in the treatedreas, as reported previously by Journee-de Korvernd coworkers.10 However, at 4 weeks, vascularemodeling and reperfusion of choriocapillaris pre-ominates, presenting a mottled hypofluorescence-yperfluorescence appearance on fluoresceinngiography. Retinal vessels did not show dye leakageue to a breakdown of the vascular barrier at anytage. These results show that TTT first leads to anncrease in vascular permeability, then to closure ofbnormal choroidal neovascularization, as well asormal choroicapillaris in the treated area.14 This
s followed by vascular remodeling and reperfusionf the normal choriocapillaris. This mottled patternf hypofluorescence and hyperfluorescence is alsovident in CCH after TTT (Fig. 1, bottom left).Currie and associates, using fluorescein angiogra-
hy, described retinal and choroidal vascular changesssociated with TTT for choroidal melanoma in 29yes.5 The authors demonstrated that choroidal ves-els within the margins of the choroidal melanomaere destroyed after TTT.5 However, choroidal ves-
els beyond the edges of the tumor but within thereatment margins were still present. This findingupports the results from the histopathologic studyf Connolly and associates that heavy fundus pigmen-ation (as with a choroidal melanoma) increases theptake of heat during hyperthermia.4 Currie and as-ociates found a high rate of retinal vascular occlu-ion: 83% arterial and 69% venous occlusion afterTT for choroidal melanoma. They also found that 4yes (14%) developed choroidal neovascularization.Midena and coworkers reported fluorescein and
ndocyanine green angiographic findings in 45 eyesith choroidal melanoma after TTT.19 Using indocy-nine green angiography, patent choroidal vesselsere found in 76% of the cases, choroidal vascularemodeling in 42%, and retinochoroidal anastomosisn 11%. Four eyes (9%) had melanoma recurrence.ll recurrent cases demonstrated retinochoroidalnastomosis.5 The authors emphasized the signifi-ance of indocyanine green angiography in the evalu-tion of the impact of TTT on choroidal circulation.hey pointed out that indocyanine green angiogra-hy is necessary to confirm that fluorescein leakage

TRANSPUPILLARY THERMOTHERAPY 321
Fig. 1. Top left: Fundus photograph shows the choroidal hemangioma (arrows) measuring 6.0 × 6.0 mm in base diameter.Top right: Late venous phase fluorescein angiogram depicts the marked hyperfluorescence in the tumor. Middle left: B-mode ultrasonogram demonstrates the 2.0 mm thick choroidal hemangioma with acoustic solidity. Middle right: Fundusphotograph demonstrates the complete regression of choroidal hemangioma 3 months after a single session of TTT.Bottom left: Late venous phase fluorescein angiogram shows the complete disappearance of choroidal hemangioma 3months after a single session of TTT. Note the mottled hyperfluorescence-hypofluorescence pattern of the choroid.Bottom right: B-mode ultrasonogram depicts the complete disappearance of the choroidal hemangioma 3 months after asingle session of TTT.
322 Surv Ophthalmol 49 (3) May–June 2004 GUNDUZ
seen on fluorescein angiography is due to choroidalneovascularization instead of simulating conditionssuch as choroidal vascular remodeling.19
INDICATIONS FOR TTT
Transpupillary thermotherapy can be used as aprimary treatment7,8,12,20 or secondary treatment22,24
for CCH (Table 1). Of the 38 cases of CCH reviewed,36 had TTT as primary treatment. Transpupillarythermotherapy was used as secondary treatment intwo cases of CCH after subretinal fluid failed to re-solve with laser photocoagulation.22,24
The indication for performing TTT on a CCHis the presence of exudative detachment of the fovealeading to a decrease in visual acuity. CCHs eligiblefor TTT are those with anterior tumor margin pos-terior to the equator of the eye, largest tumor base�10 mm, tumor thickness �4 mm, and shallow su-bretinal fluid overlying the tumor. Table 2 showsthe largest tumor base diameter and tumor thicknessfrom the published studies7,8,12,20,22,24 and the au-thor’s current series. Among the reported series, onlyFuchs and coworkers used TTT for CCH up to 5.1mm in thickness.7
CCHs with a largest base diameter �10 mm andthickness �4 mm associated with extensive, bullousretinal detachment are not generally treated withTTT. Extensive subretinal fluid overlying the tumormay hinder effective visualization of the tumor andprevent accurate focusing of the laser beam. Radia-tion therapy has classically been used in the treatmentof medium to large CCH with bullous retinal de-tachment.9,28
Another important feature to consider is tumor-touching of the optic disk for three reasons. First,proper treatment of the tumor margin touching the
otuti(StitotosatTTf
qmbaetprwmabssrc
TABLE 1
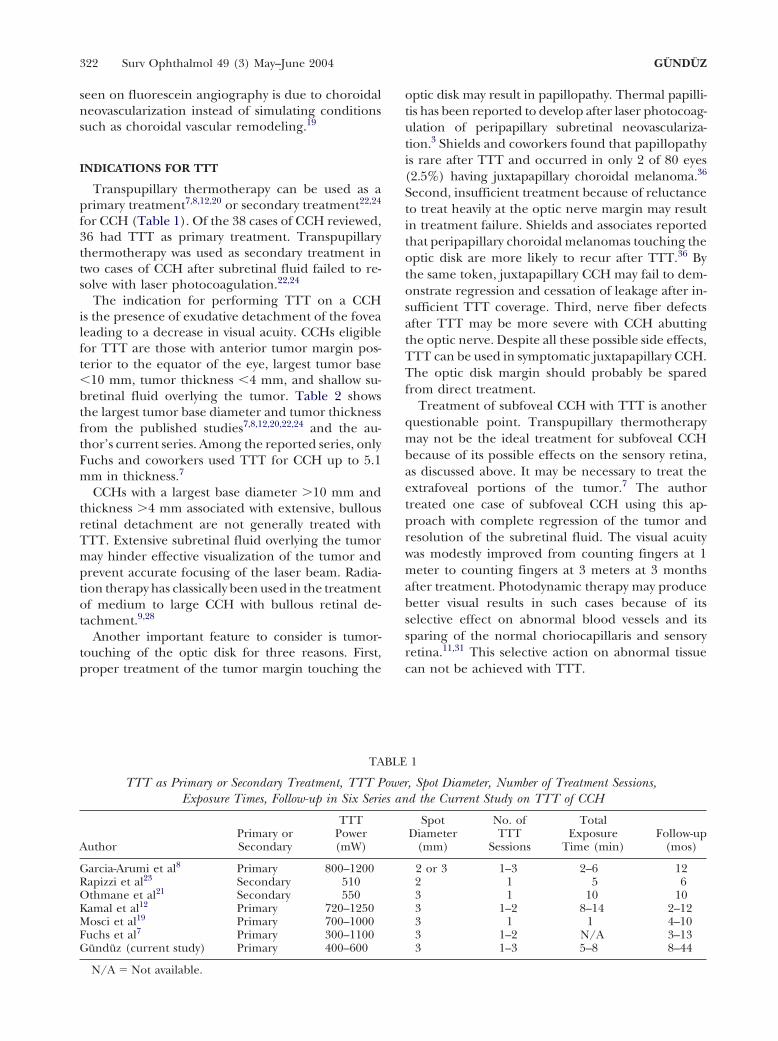
TTT as Primary or Secondary Treatment, TTT Power, Spot Diameter, Number of Treatment Sessions,Exposure Times, Follow-up in Six Series and the Current Study on TTT of CCH
TTT Spot No. of TotalPrimary or Power Diameter TTT Exposure Follow-up
Author Secondary (mW) (mm) Sessions Time (min) (mos)
Garcia-Arumi et al8 Primary 800–1200 2 or 3 1–3 2–6 12Rapizzi et al23 Secondary 510 2 1 5 6Othmane et al21 Secondary 550 3 1 10 10Kamal et al12 Primary 720–1250 3 1–2 8–14 2–12Mosci et al19 Primary 700–1000 3 1 1 4–10Fuchs et al7 Primary 300–1100 3 1–2 N/A 3–13Gunduz (current study) Primary 400–600 3 1–3 5–8 8–44
N/A � Not available.
an not be achieved with TTT.
ptic disk may result in papillopathy. Thermal papilli-is has been reported to develop after laser photocoag-lation of peripapillary subretinal neovasculariza-ion.3 Shields and coworkers found that papillopathys rare after TTT and occurred in only 2 of 80 eyes2.5%) having juxtapapillary choroidal melanoma.36
econd, insufficient treatment because of reluctanceo treat heavily at the optic nerve margin may resultn treatment failure. Shields and associates reportedhat peripapillary choroidal melanomas touching theptic disk are more likely to recur after TTT.36 Byhe same token, juxtapapillary CCH may fail to dem-nstrate regression and cessation of leakage after in-ufficient TTT coverage. Third, nerve fiber defectsfter TTT may be more severe with CCH abuttinghe optic nerve. Despite all these possible side effects,TT can be used in symptomatic juxtapapillary CCH.he optic disk margin should probably be spared
rom direct treatment.Treatment of subfoveal CCH with TTT is another
uestionable point. Transpupillary thermotherapyay not be the ideal treatment for subfoveal CCH
ecause of its possible effects on the sensory retina,s discussed above. It may be necessary to treat thextrafoveal portions of the tumor.7 The authorreated one case of subfoveal CCH using this ap-roach with complete regression of the tumor andesolution of the subretinal fluid. The visual acuityas modestly improved from counting fingers at 1eter to counting fingers at 3 meters at 3 months
fter treatment. Photodynamic therapy may produceetter visual results in such cases because of itselective effect on abnormal blood vessels and itsparing of the normal choriocapillaris and sensoryetina.11,31 This selective action on abnormal tissue

TRANSPUPILLARY THERMOTHERAPY 323
TTT TECHNIQUE, PARAMETERS, AND FOLLOW-UP
Transpupillary thermotherapy is performed withdiode laser emitting at 810 nm with a slit-lamp biomi-croscope delivery system. After pupillary dilation, aretrobulbar injection of local anesthetic is given. TTTis performed using a contact lens with coupling agentand topical anesthesia. The panfunduscope (Roden-stock or Volk) or the Mainster contact lenses arecommonly used. With the panfunduscope and theMainster lenses, the actual retinal spot size is 41%and 5% greater than the thermotherapy spot sizesetting, respectively.18
The TTT parameters used in the published stud-ies7,8,12,20,22,24 and the current series are listed inTable 1. A 2 or 3 mm spot diameter can be chosen. Theinitial power is generally set at 200–300 mW andthe power is increased in 50–100 mW incrementsuntil a light gray color change is observed on thetumor surface during the second half of the oneminute application period. A whitish color change onthe tumor surface is not desirable, as it indicatesoverexposure. The powers used range from 300 to1200 mW (Table 1).
Each spot is maintained for 1 minute on the tumorsurface to ensure that TTT achieves the necessarytemperature raise in the treated tissue. The exposuretime is adjusted to cover the entire tumor surface inan overlapping fashion, with larger tumors requiringlonger exposure times. In the published series, expo-sure times ranged from 2 to 14 minutes, dependingon the tumor size (Table 1).
According to the results of the histopathologicstudy of Connolly and associates,4 undesirable sen-sory retinal damage is unlikely to occur with low- tomedium-dose TTT power levels (power/spot diame-ter ratio �267 mW/mm) in light to moderately pig-mented eyes. Furthermore, the subretinal fluidoverlying a choroidal hemangioma may help to
n
A
sdcs(ttbc
fpau
C
tcartrse(dt
tdmip
TABLE 2
Number of Eyes, Largest Tumor Base Diameter, andTumor Thickness in 6 Series and the Current
Study on TTT of CCH
Largest TumorNo. of Tumor Base Thickness
Author Eyes Diameter (mm) (mm)
Garcia-Arumi et al8 8 4.1–7.3 1.8–3.4Rapizzi et al23 1 6.1 1.6Othmane et al21 1 6.0 3.5Kamal et al12 6 6.5–9.0 2.0–4.5Mosci et al19 2 N/A 1.5–2.6Fuchs et al7 10 2.3–7.5 1.2–5.1Gunduz 10 3.0–8.0 1.5–3.1
(current study)
N/A � Not available.
relm
eftvst
eiTdr
educe the effect of heat on the sensory retina. How-ver, it may be prudent to use lower power levels (20%ess according to the above study) in patients with
ore heavily pigmented eyes.The end point of TTT in CCH is the resolution of
xudative detachment of the fovea. If the subretinalluid fails to resolve after one treatment, second andhird treatments can be given at 2- to 3-month inter-als. The end point of treatment is not total tumor de-truction, and further treatment is not necessary ifhe tumor stops leaking.
Kamal and associates used indocyanine green dyenhancement in TTT of CCH.12 They reasoned thatndocyanine green dye injected 20 seconds prior toTT may increase the uptake of heat in CCH, as itoes in amelanotic choroidal melanoma. In othereports on TTT of choroidal hemangioma, indocya-ine green dye enhancement was not used.7,8,20,22,24
NATOMIC RESULTS
Of the 38 CCHs reviewed herein, all tumorstopped leaking after TTT and the exudative retinaletachment resolved. Sixteen CCHs (42%) showedomplete regression (Fig. 1), 20 CCHs (53%) demon-trated partial regression by at least 10%, and 2 CCHs5%) displayed no change after TTT on the basis ofumor thickness (Table 3). Transpupillary thermo-herapy produces early resolution of subretinal fluidut slower tumor shrinkage, with tumor regressionontinuing for many months after treatment.
CCHs with increased tumor thickness or subretinalibrosis and those treated previously with argon laserhotocoagulation may not show complete regressionfter TTT.7,22 These factors may prevent effectiveptake of heat by the tumor.
OMPLICATIONS
Among the 28 cases of CCH reported in the litera-ure (Table 3),7,8,12,20,22,24 the treatment compli-ations were branch retinal vein occlusion in one eyend transient CME in one eye.12 The transient CMEesponded well to oral nonsteroidal anti-inflamma-ory medication.12 Complications after TTT of cho-oidal hemangioma in the ten eyes in the author’series included CME and preretinal fibrosis (twoyes [Fig. 2, top and middle]) and focal iris atrophythree eyes [Fig. 3]). These complications were evi-ent at the first follow-up visit 3 months afterreatment.
Preretinal fibrosis may be due to heat-induced con-raction of the internal limiting membrane. Capillaryamage after TTT may also contribute to the develop-ent of preretinal fibrosis. Cystoid macular edema
s probably due to heat-induced inflammation of theerifoveal vascular bed leading to capillary damage.

324 Surv Ophthalmol 49 (3) May–June 2004 GUNDUZ
TABLE 3
Tumor Status, Treatment Complications and Best-corrected Visual Acuity Change afterTTT in Six Series and the Current Study on TTT of CCH
BCVA ChangebTumor Treatment
Author Statusa Complications Increased Unchanged Decreased
Garcia-Arumi et al8 PR (8) - 4 2 -Rapizzi et al23 TR - 1 - (1)Othmane et al21 PR - 1 - (1)Kamal et al12 TR (5), PR (1) BRVO (1), Worsening 3 2 -
CME (1)Mosci et al19 TR (2) - 2 - -Fuchs et al7 PR (8), NC (2) - 4 2 -Gunduz (current study) TR (8), PR (2) CME (2), preretinal 5 - -
fibrosis (2), IA (3)
BCVA � best corrected visual acuity; TR � total regression; PR � partial regression; NC � no change; BRVO � branchretinal vein obstruction; CME � cystoid macular edema; IA � iris atrophy.
a Refers to change in tumor thickness.b Refers to �2 Snellen lines of visual acuity change in patients having pretreatment visual acuities �0.05. Patients
with pretreatment visual acuity �0.05 were not included.
The preretinal fibrosis itself may also increase theCME. Topical nonsteroidal anti-inflammatory andsteroidal medication can be tried in the managementof CME. However, in some cases, CME can be persis-tent. In both of the author’s cases, a tapering doseof oral prednisone (1 mg/kg/day) was required forresolution of CME (Fig. 2, bottom), that did notrespond to a 3-month topical steroid treatment.
Focal iris atrophy develops because of the broadlaser beam’s inadvertently touching the partially di-lated pupil (Fig. 3). It is important that pupils befully dilated before TTT to minimize the risk of iriscomplications. Should the pupil become mioticduring TTT, the application should be stopped andpupillary dilation should be re-established.
Transpupillary thermotherapy can cause branchretinal artery or vein occlusion because of the heat-induced ischemic necrosis of vascular endothelium.Thrombosis in the vascular lumina may also contrib-ute to vascular occlusion.10 Shields and coworkersreported that branch retinal vascular occlusions arefairly common following TTT of choroidal mela-noma (12–41%).36 Currie and associates found thatretinal vascular occlusions involving small vessels oc-curred in a higher proportion of eyes undergoingTTT for choroidal melanoma (69–83%).5 In mostcases, retinal vascular occlusion does not have signifi-cant consequences.36 However, retinal vein occlusionmay lead to retinal ischemia and neovasculariza-tion in about 6% of the treated eyes.36,39
Another potential complication of TTT in CCHis the development of visual field defects. In studieswith choroidal melanoma, TTT has been shown tocause wedge-shaped visual field defects.26 Althoughsubretinal fluid separating the sensory retina from
tpv
V
2V2rdlApcp
ooiiwtobeti
nma
he retinal pigment epithelium may provide a certainrotection for the retina, visual field defects may de-elop in eyes with CCH after TTT.
ISUAL RESULTS
Among the 38 eyes treated with TTT (Table 3),6 had pretreatment visual acuity �0.05 (20/400).isual acuity increased by 2 or more Snellen lines in0 of 26 eyes (77%), and remained unchanged in theemaining 6 eyes (23%). Decrease in visual acuityid not occur in any of the treated eyes having base-
ine visual acuities �0.05. Two patients in Garcia-rumi series,8 one patient in Kamal series,12 fouratients in Fuchs series,7 and five patients in theurrent series were excluded because they hadretreatment visual acuities �0.05.The visual outcome in CCH depends on a number
f factors. The presence of subfoveal tumor, CME,r subretinal fibrosis may preclude marked increase
n visual acuity after treatment. Shields and associates,n a review of 200 CCHs, reported that visual acuityas 0.1 (20/200) or less in 60% of the eyes despite
reatment with various modalities.35 Shorter durationf symptoms before treatment was associated with aetter visual outcome. The authors concluded thatarly treatment should be instituted in vision-hreatening choroidal hemangiomas before irrevers-ble changes take place.35
Summary and ConclusionsTranspupillary thermotherapy without indocya-
ine green dye enhancement seems to be an effectiveethod to treat CCH. The goal of treatment is to
chieve resolution of exudative detachment of the

TRANSPUPILLARY THERMOTHERAPY 325
Fig. 2. Top left: Fundus photograph shows the choroidalhemangioma (arrows) measuring 8.0 × 6.0 mm in base diam-eter and 2.5 mm in thickness (by ultrasonography). Top right:Early venous phase fundus fluorescein angiogram depictsthe patchy hyperfluorescence in the choroidal hemangioma,pigment epithelial changes temporal and superior to thetumor suggestive of subretinal fluid, and absence of pre-treat-ment cystoid macular edema. Middle left: Fundus photographshows the completely regressed choroidal hemangioma(arrows) 3 months following TTT. The macular epiretinalmembrane extending from the tumor base to the optic discis hardly visible in this photograph. Middle right: Late phasefundus fluorescein angiogram demonstrates completeregression of the choroidal hemangioma 3 months followingTTT. Note the presence of cystoid macular edema andthe staining of the retina in the area of the epiretinalmembrane between the optic disk and the treatment scar.Bottom: Late phase fundus fluorescein angiogram shows theresolution of cystoid macular edema following oral cortico-steroid treatment.
fovea and improvement of vision. Transpupillarythermotherapy can lead to total or partial regressionof CCH. In subfoveal CCH, the extrafoveal portions ofthe tumor may be treated. Complications of TTTof CCH include CME, preretinal fibrosis, focal irisatrophy, and retinal vascular occlusion. Althoughmost of the reported studies on TTT of CCH had
la
d
imited follow-up, TTT has not been associated withny significant complications.
Methods of Literature SearchA search of the PubMed database to 2003 was con-
ucted using various combinations of the key words

326 Surv Ophthalmol 49 (3) May–June 2004 GUNDUZ
Fig. 3. Iris atrophy (arrows) following TTT of choroidalhemangioma. This complication develops from the laserbeam inadvertently touching the mid-dilated pupil.
1
1
1
1
1
1
1
choroidal hemangioma, cystoid macular edema, preretinalfibrosis, laser photocoagulation, photodynamic therapy, ra-diation therapy, transpupillary thermotherapy, visual fields,choroidal melanoma, retinal capillary hemangioma, age-related macular degeneration, and retinoblastoma. Articlesin all languages were considered provided that theEnglish abstracts were included in non-English arti-cles. Relevant articles that were cited in the referencelists of the retrieved articles were also included. Allreports related to the use of TTT for circumscribedchoroidal hemangiomas were included. Selected re-ports of the use TTT for other types of tumors andreports of other types of treatment for choroidal hem-angiomas were included for purposes of comparison.
References1. Anand R, Augsburger JJ, Shields JA: Circumscribed choroidal
hemangiomas. Arch Ophthalmol 107:1338–42, 19892. Barbazetto I, Schmidt-Erfurth U: Photodynamic therapy of
choroidal hemangioma: two case reports. Graefe’s Arch ClinExp Ophthalmol 238:214–21, 2000
3. Bloom SM: Thermal papillitis after dye red photocoagulationof a peripapillary choroidal neovascular membrane. Retina10:261–4, 1990
4. Connolly BP, Regillo CD, Eagle RC Jr, et al: The histopatho-logic effects of transpupillary thermotherapy in human eyes.Ophthalmology 110:415–20, 2003
5. Currie ZI, Rennie IG, Talbot JF: Retinal vascular changesassociated with transpupillary thermotherapy for choroidalmelanomas. Retina 20:620–6, 2000
6. Diaz CE, Capone A, Grossniklaus HE: Clinicopathologic find-ings in recurrent choroidal melanoma after transpupillarythermotherapy. Ophthalmology 105:1419–24, 1998
7. Fuchs AV, Mueller AJ, Grueterich M, Ulbig MW: Transpupil-lary thermotherapy (TTT) in circumscribed choroidal hem-angioma. Graefes Arch Clin Exp Ophthalmol 240:7–11, 2002
8. Garcia-Arumi J, Ramsay LS, Guraya BC: Transpupillary ther-motherapy for circumscribed choroidal hemangiomas. Oph-thalmology 107:351–6, 2000
9. Hannouche D, Frau E, Desjardins L, et al: Efficacy of protontherapy in circumscribed choroidal hemangiomas associatedwith serous retinal detachment. Ophthalmology 104:1780–4, 1997
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
0. Journee-de Korver JG, Oosterhius JA, de Wolff-RouendaalD, Kemme H: Histopathological findings in human choroidalmelanomas after transpupillary thermotherapy. Br J Oph-thalmol 81:234–9, 1997
1. Jurklies B, Anastassiou G, Ortmans S, et al: Photodynamictherapy using verteporfin in circumscribed choroidal heman-gioma. Br J Ophthalmol 87:84–9, 2003
2. Kamal A, Watts AR, Rennie IG: Indocyanine green enhancedtranspupillary thermotherapy of circumscribed choroidalhemangioma. Eye 14:701–5, 2000
3. Lanzetta P, Virgili G, Ferrari E, Menchini U: Diode laserphotocoagulation of choroidal hemangioma. Int Ophthal-mol 19:239–47, 1996
4. Lanzetta P, Michieletto P, Pirracchio A, Bandello F: Earlyvascular changes induced by transpupillary thermotherapy ofchoroidal neovascularization. Ophthalmology 109:1098–104, 2002
5. Lee V, Hungerford JL: Proton beam therapy for posteriorpole circumscribed choroidal hemangioma. Eye 12:925–8,1998
6. Madreperla SA, Hungerford JL, Plowman PN, et al: Choroidalhemangiomas: visual and anatomic results of treatment byphotocoagulation or radiation therapy. Ophthalmology 104:1773–9, 1997
7. Madreperla SA: Choroidal hemangioma treated with photo-dynamic therapy using verteporfin. Arch Ophthalmol 119:1606–10, 2001
8. Mainster MA, Crossman JL, Erickson PJ, Heacock GL: Retinallaser lenses: magnification, spot size, and field of view. Br JOphthalmol 74:177–9, 1990
9. Midena E, Pilotto E, DeBelvis V, et al: Choroidal vascularchanges after transpupillary thermotherapy for choroidalmelanoma. Ophthalmology 110:2216–22, 2003
0. Mosci C, Polizzi A, Zingirian M: Transpupillary thermother-apy for circumscribed choroidal hemangiomas: first choicein therapy. Eur J Ophthalmol 11:316–8, 2001
1. Newsom RS, McAlister JC, Saeed M, McHugh JD: Transpupil-lary thermotherapy (TTT) for the treatment of choroidalneovascularisation. Br J Ophthalmol 85:173–8, 2001
2. Othmane IS, Shields CL, Shields JA, et al: Circumscribed cho-roidal hemangioma managed by transpupillary thermother-apy. Arch Ophthalmol 117:136–7, 1999
3. Parmar DN, Mireskandari K, McHugh D: Transpupillary ther-motherapy for retinal capillary hemangioma in von Hippel-Lindau disease. Ophthalmic Surg Lasers 31:334–6, 2000
4. Rapizzi E, Grizzard WS, Capone A Jr: Transpupillary thermo-therapy in the management of circumscribed choroidal hem-angioma. Am J Ophthalmol 127:481–2, 1999
5. Ritland JS, Eide N, Tausjo J: External beam irradiation ther-apy for choroidal hemangiomas. Visual and anatomic resultsafter a dose of 20 to 25 Gy. Acta Ophthalmol Scand 79:184–6, 2001
6. Robertson DM, Buettner H, Bennett SR: Transpupillary ther-motherapy as primary treatment of small choroidal melano-mas. Arch Ophthalmol 117:1512–9, 1999
7. Robertson DM: Photodynamic therapy for choroidal heman-gioma associated with serous retinal detachment. Arch Oph-thalmol 120:1155–61, 2002
8. Schilling H, Sauerwein W, Lommatzsch A, et al: Long termresults after low dose ocular irradiation for choroidal hae-mangiomas. Br J Ophthalmol 81:267–73, 1997
9. Schmidt-Erfurth UM, Michels S, Kusserow C, et al: Photody-namic therapy for symptomatic choroidal hemangioma.Visual and anatomic results. Ophthalmology 109:2284–94,2002
0. Scott TA, Augsburger JJ, Brady LW, et al: Low dose irradiationfor diffuse choroidal hemangiomas associated with bullousnonrhegmatogenous retinal detachment. Retina 11:389–93, 1991
1. Sheidow TG, Harbour JW: Photodynamic therapy for circum-scribed choroidal hemangioma. Can J Ophthalmol 37:314–7, 2002
2. Shields CL, Shields JA, DePotter P: Patterns of indocyaninegreen videoangiography of choroidal tumors. Br J Ophthal-mol 79:237–45, 1995

TRANSPUPILLARY THERMOTHERAPY 327
33. Shields CL, Shields JA, Cater J, et al: Transpupillary thermo-therapy for choroidal melanoma: tumor control and visualresults in 100 consecutive cases. Ophthalmology 105:581–90, 1998
34. Shields CL, Santos MCM, Diniz W, et al: Thermotherapy forretinoblastoma. Arch Ophthalmol 117:885–93, 1999
35. Shields CL, Honavar SG, Shields JA, et al: Circumscribedchoroidal hemangioma: clinical manifestations and factorspredictive of visual outcome in 200 consecutive cases. Oph-thalmology 108:2237–48, 2001
36. Shields CL, Shields JA, Perez N, et al: Primary transpupillarythermotherapy for small choroidal melanoma in 256 consec-utive cases. Outcomes and limitations. Ophthalmology 109:225–34, 2002
37. Shields JA: The expanding role of laser photocoagulation forintraocular tumors: the 1993 H. Christian Zweng MemorialLecture. Retina 14:310–22, 1994
38. Shields JA, Shields CL: Intraocular Tumors. A Text andAtlas. Philadelphia, Saunders, 1992, pp 239–59
39. Singh AD, Eagle RC Jr, Shields CL, Shields JA: Enucleationfollowing transpupillary thermotherapy of choroidal mela-noma: clinicopathologic correlations. Arch Ophthalmol121:397–400, 2003
4
4
4
C2
d
tF
0. Verteporfin in Photodynamic Therapy Study Group : Vertep-orfin therapy of subfoveal choroidal neovascularization inage-related macular degeneration: two-year results of arandomized clinical trial including lesions with occult withno classic neovascularization-vertoporfin in photodynamictherapy report 2. Am J Ophthalmol 131:541–60, 2001
1. Witschel H, Font RL: Hemangioma of the choroid. A clinico-pathologic study of 71 cases and a review of the literature.Surv Ophthalmol 20:415–31, 1976
2. Zografos L, Bercher L, Chamot L, et al: Cobalt-60 treatmentof choroidal hemangiomas. Am J Ophthalmol 121:190–9,1996
Presented in part as a scientific poster at the Xth Internationalongress of Ocular Oncology, Amsterdam, the Netherlands, 17–1 June 2001.The author has no proprietary interest in any concept or product
iscussed in this article.Reprint address: Kaan Gunduz MD, Associate Professor of Oph-
halmology, G.M.K.Bulvari116/3, Maltepe 06570, Ankara, Turkey.ax: 90-312-2291812. E-mail: [email protected]


















