
Transplant Digest - Fall 2010, Issue No. 9 - St. Michael's · Regular readers of the Transplant...
12
Regular readers of the Transplant Digest, will notice that we now have an exciting new layout and design. This change is part of the roll out of renewed St. Michael’s brand. St. Michael’s new image captures its reputation for compassion and caring along with its reality as a modern, sophisticated, and innovative organization. Our new tagline “ Inspired Care. Inspiring Science.” emphasizes equally our three roles – as a hospital providing compassionate care and a teaching and research organization committed to moving knowledge and discovery from the classroom and the lab to the bedside. New Image of Transplant Digest Transplant Digest Fall 2010, Issue No. 9 In this issue ... New Image of Transplant Digest Heart Disease After Kidney Transplantation From the Editor’s Desk Contact Information Kidney Regeneration Post-Transplant Chat Smoking and Kidney Transplantation Coping With Chronic Renal Allograft Failure An Introduction to Diabetes and Kidney Transplant ADVAgraf: A Once Daily Alternative to PROgraf Regular readers of the Transplant Digest, will notice that we now have an exciting new layout and design. This change is part of the roll out of renewed St. Michael’s brand. St. Michael’s new image captures its reputation for compassion and caring along with its reality as a modern, sophisticated, and innovative organization. Our new tagline “ Inspired Care. Inspiring Science.” emphasizes equally our three roles – as a hospital providing compassionate care and a teaching and research organization committed to moving knowledge and discovery from the classroom and the lab to the bedside. New Image of Transplant Digest Transplant Digest Fall , Issue No. In this issue ... New Image of Transplant Digest Heart Disease After Kidney Transplantation From the Editor’s Desk Contact Information Kidney Regeneration Post-Transplant Chat Smoking and Kidney Transplantation Coping With Chronic Renal Allograft Failure An Introduction to Diabetes and Kidney Transplant ADVAgraf: A Once Daily Alternative to PROgraf Cardiovascular disease (CVD), involving such conditions as heart attacks and bypass surgery, is known to decrease dramatically after kidney transplantation. However, CVD is more prevalent in kidney transplant patients than the general population. Even young transplant recipients experience close to a 10-fold increase in CVD. Therefore, CVD is clearly a significant barrier to staying healthy post-transplantation. In order to prevent CVD, doctors attempt to predict which patients are most at risk for developing CVD using the Framingham Risk Score (FRS). The FRS is the most common tool used to determine a patient`s CVD risk. It combines traditional cardiac risk factors (age, sex, total cholesterol, high density lipoprotein, smoking status, diabetes, and blood pressure) to identify high risk patients who would benefit from medications to protect their heart, such as aspirin, blood pressure drugs, and cholesterol-lowering drugs. Unfortunately, the FRS may not be an accurate indicator of risk in kidney transplant patients. In fact, research has shown that the FRS underestimates CVD in kidney transplant patients, especially those patients at the highest risk for developing CVD. This is likely because kidney transplant patients have other important risk factors to consider. These include: • Pre-transplant cardiac and chronic kidney disease • Post-transplant exposure to cardiac risk factors • immunosuppressant medications, acute rejection, and infection At St. Michael`s Hospital (SMH), we are using information on our transplant patients to improve the FRS and identify cardiac risk factors that are specific to kidney transplant patients. We are now studying traditional, novel, and transplant-specific risk factors to determine which factors are most important in kidney transplant patients. Novel risk factors such as C-reactive protein, microalbuminuria, uric acid, vitamin D, and Heart Disease after Kidney Transplantation - Are the Risk Factors the same as the General Population? Dr. Samuel Silver, Resident in Internal Medicine (con’t on page 3) TRANSPLANT DIGEST Fall 2010, Issue No. 9 Transplant Digest Cardiovascular disease (CVD), involving such conditions as heart attacks and bypass surgery, is known to decrease dramatically after kidney transplantation. However, CVD is more prevalent in kidney transplant patients than the general population. Even young transplant recipients experience close to a 10-fold increase in CVD. Therefore, CVD is clearly a significant barrier to staying healthy post-transplantation. In order to prevent CVD, doctors attempt to predict which patients are most at risk for developing CVD using the Framingham Risk Score (FRS). The FRS is the most common tool used to determine a patient`s CVD risk. It combines traditional cardiac risk factors (age, sex, total cholesterol, high density lipoprotein, smoking status, diabetes, and blood pressure) to identify high risk patients who would benefit from medications to protect their heart, such as aspirin, blood pressure drugs, and cholesterol-lowering drugs. Unfortunately, the FRS may not be an accurate indicator of risk in kidney transplant patients. In fact, research has shown that the FRS underestimates CVD in kidney transplant patients, especially those patients at the highest risk for developing CVD. This is likely because kidney transplant patients have other important risk factors to consider. These include: • Pre-transplant cardiac and chronic kidney disease • Post-transplant exposure to cardiac risk factors • Transplant-specific risk factors related to immunosuppressant medications, acute rejection, and infection At St. Michael`s Hospital (SMH), we are using information on our transplant patients to improve the FRS and identify cardiac risk factors that are specific to kidney transplant patients. We are now studying traditional, novel, and transplant-specific risk factors to determine which factors are most important in kidney transplant patients. Novel risk factors such as C-reactive protein, microalbuminuria, uric acid, vitamin D, and Heart Disease after Kidney Transplantation - Are the Risk Factors the same as the General Population? Dr. Samuel Silver, Resident in Internal Medicine (con’t on page 3) TRANSPLANT DIGEST Fall 2010, Issue No. 9
Transcript of Transplant Digest - Fall 2010, Issue No. 9 - St. Michael's · Regular readers of the Transplant...

Regular readers of the Transplant Digest, will notice that we now have an exciting new layout and design. This change is part of the roll out of renewed St. Michael’s brand.
St. Michael’s new image captures its reputation for compassion and caring along with its reality as a modern, sophisticated, and innovative organization.
Our new tagline “ Inspired Care. Inspiring Science.” emphasizes equally our three roles – as a hospital providing compassionate care and a teaching and research organization committed to moving knowledge and discovery from the classroom and the lab to the bedside.
New Image of Transplant Digest
Transplant Digest
Fall 2010, Issue No. 9
In this issue ...New Image of Transplant Digest
Heart Disease After Kidney Transplantation
From the Editor’s Desk
Contact Information
Kidney Regeneration
Post-Transplant Chat
Smoking and Kidney Transplantation
Coping With Chronic Renal Allograft Failure
An Introduction to Diabetes and Kidney Transplant
ADvAgraf: A Once Daily Alternative to PROgraf
Regular readers of the Transplant Digest, will notice that
we now have an exciting new layout and design. This
change is part of the roll out of renewed St. Michael’s
brand.St. Michael’s new image captures its reputation for
compassion and caring along with its reality as a
modern, sophisticated, and innovative organization.
Our new tagline “ Inspired Care. Inspiring Science.”
emphasizes equally our three roles – as a hospital
providing compassionate care and a teaching
and research organization committed to moving
knowledge and discovery from the classroom and the lab to the
bedside.
New Image of Transplant Digest
Transplant DigestFall , Issue No.
In this issue ...New Image of Transplant DigestHeart Disease After Kidney TransplantationFrom the Editor’s Desk
Contact InformationKidney Regeneration
Post-Transplant ChatSmoking and Kidney Transplantation
Coping With Chronic Renal Allograft FailureAn Introduction to Diabetes and Kidney Transplant
ADVAgraf: A Once Daily Alternative to PROgraf
Cardiovascular disease (CVD), involving such conditions
as heart attacks and bypass surgery, is known to decrease
dramatically after kidney transplantation. However, CVD
is more prevalent in kidney transplant patients than the
general population. Even young transplant recipients
experience close to a 10-fold increase in CVD. Therefore,
CVD is clearly a significant barrier to staying healthy
post-transplantation. In order to prevent CVD, doctors attempt to predict
which patients are most at risk for developing CVD
using the Framingham Risk Score (FRS). The FRS is the
most common tool used to determine a patient`s CVD
risk. It combines traditional cardiac risk factors (age,
sex, total cholesterol, high density lipoprotein, smoking
status, diabetes, and blood pressure) to identify high risk
patients who would benefit from medications to protect
their heart, such as aspirin, blood pressure drugs, and
cholesterol-lowering drugs. Unfortunately, the FRS may
not be an accurate indicator of risk in kidney transplant
patients.
In fact, research has shown that the FRS underestimates
CVD in kidney transplant patients, especially those
patients at the highest risk for developing CVD. This
is likely because kidney transplant patients have other
important risk factors to consider. These include:
• Pre-transplant cardiac and chronic kidney disease
• Post-transplant exposure to cardiac risk factors
• immunosuppressant medications, acute rejection, and
infection At St. Michael`s Hospital (SMH), we are using
information on our transplant patients to improve the
FRS and identify cardiac risk factors that are specific
to kidney transplant patients. We are now studying
traditional, novel, and transplant-specific risk factors to
determine which factors are most important in kidney
transplant patients. Novel risk factors such as C-reactive
protein, microalbuminuria, uric acid, vitamin D, and
Heart Disease after Kidney Transplantation -
Are the Risk Factors the same as the General Population?
Dr. Samuel Silver, Resident in Internal Medicine
(con’t on page 3)
TRANSPLANT DIGESTFall 2010, Issue No. 9
Regular readers of the Transplant Digest, will notice that
we now have an exciting new layout and design. This
change is part of the roll out of renewed St. Michael’s
brand.St. Michael’s new image captures its reputation for
compassion and caring along with its reality as a
modern, sophisticated, and innovative organization.
Our new tagline “ Inspired Care. Inspiring Science.”
emphasizes equally our three roles – as a hospital
providing compassionate care and a teaching
and research organization committed to moving
knowledge and discovery from the classroom and the lab to the
bedside.
New Image of Transplant Digest
Transplant DigestFall
, Issue No.
In this issue ...New Image of Transplant Digest
Heart Disease After Kidney
TransplantationFrom the Editor’s DeskContact InformationKidney RegenerationPost-Transplant ChatSmoking and Kidney TransplantationCoping With Chronic Renal
Allograft FailureAn Introduction to Diabetes and
Kidney TransplantADVAgraf: A Once Daily
Alternative to PROgraf
Cardiovascular disease (CVD), involving such conditions
as heart attacks and bypass surgery, is known to decrease
dramatically after kidney transplantation. However, CVD
is more prevalent in kidney transplant patients than the
general population. Even young transplant recipients
experience close to a 10-fold increase in CVD. Therefore,
CVD is clearly a significant barrier to staying healthy
post-transplantation. In order to prevent CVD, doctors attempt to predict
which patients are most at risk for developing CVD
using the Framingham Risk Score (FRS). The FRS is the
most common tool used to determine a patient`s CVD
risk. It combines traditional cardiac risk factors (age,
sex, total cholesterol, high density lipoprotein, smoking
status, diabetes, and blood pressure) to identify high risk
patients who would benefit from medications to protect
their heart, such as aspirin, blood pressure drugs, and
cholesterol-lowering drugs. Unfortunately, the FRS may
not be an accurate indicator of risk in kidney transplant
patients.
In fact, research has shown that the FRS underestimates
CVD in kidney transplant patients, especially those
patients at the highest risk for developing CVD. This
is likely because kidney transplant patients have other
important risk factors to consider. These include:
• Pre-transplant cardiac and chronic kidney disease
• Post-transplant exposure to cardiac risk factors
• immunosuppressant medications, acute rejection, and
infection At St. Michael`s Hospital (SMH), we are using
information on our transplant patients to improve the
FRS and identify cardiac risk factors that are specific
to kidney transplant patients. We are now studying
traditional, novel, and transplant-specific risk factors to
determine which factors are most important in kidney
transplant patients. Novel risk factors such as C-reactive
protein, microalbuminuria, uric acid, vitamin D, and
Heart Disease after Kidney Transplantation -
Are the Risk Factors the same as the General Population?
Dr. Samuel Silver, Resident in Internal Medicine
(con’t on page 3)
TRANSPLANT DIGESTFall 2010
Regular readers of the Transplant Digest, will notice that
we now have an exciting new layout and design. This
change is part of the roll out of renewed St. Michael’s
brand.St. Michael’s new image captures its reputation for
compassion and caring along with its reality as a
modern, sophisticated, and innovative organization.
Our new tagline “ Inspired Care. Inspiring Science.”
emphasizes equally our three roles – as a hospital
providing compassionate care and a teaching
and research organization committed to moving
knowledge and discovery from the classroom and the lab to the
bedside.
New Image of Transplant Digest
Transplant Digest
Fall , Issue No.
In this issue ...New Image of Transplant Digest
Heart Disease After Kidney
TransplantationFrom the Editor’s DeskContact InformationKidney RegenerationPost-Transplant ChatSmoking and Kidney
TransplantationCoping With Chronic Renal
Allograft FailureAn Introduction to Diabetes and
Kidney TransplantADVAgraf: A Once Daily
Alternative to PROgraf
Cardiovascular disease (CVD), involving such conditions
as heart attacks and bypass surgery, is known to decrease
dramatically after kidney transplantation. However, CVD
is more prevalent in kidney transplant patients than the
general population. Even young transplant recipients
experience close to a 10-fold increase in CVD. Therefore,
CVD is clearly a significant barrier to staying healthy
post-transplantation.
In order to prevent CVD, doctors attempt to predict
which patients are most at risk for developing CVD
using the Framingham Risk Score (FRS). The FRS is the
most common tool used to determine a patient`s CVD
risk. It combines traditional cardiac risk factors (age,
sex, total cholesterol, high density lipoprotein, smoking
status, diabetes, and blood pressure) to identify high risk
patients who would benefit from medications to protect
their heart, such as aspirin, blood pressure drugs, and
cholesterol-lowering drugs. Unfortunately, the FRS may
not be an accurate indicator of risk in kidney transplant
patients.
In fact, research has shown that the FRS underestimates
CVD in kidney transplant patients, especially those
patients at the highest risk for developing CVD. This
is likely because kidney transplant patients have other
important risk factors to consider. These include:
• Pre-transplant cardiac and chronic kidney disease
• Post-transplant exposure to cardiac risk factors
• immunosuppressant medications, acute rejection, and
infection At St. Michael`s Hospital (SMH), we are using
information on our transplant patients to improve the
FRS and identify cardiac risk factors that are specific
to kidney transplant patients. We are now studying
traditional, novel, and transplant-specific risk factors to
determine which factors are most important in kidney
transplant patients. Novel risk factors such as C-reactive
protein, microalbuminuria, uric acid, vitamin D, and
Heart Disease after Kidney Transplantation -
Are the Risk Factors the same as the General Population?
Dr. Samuel Silver, Resident in Internal Medicine
(con’t on page 3)
TRANSPLANT DIGESTFall 2010
Cardiovascular disease (CVD), involving such conditions as heart attacks and bypass surgery, is known to decrease dramatically after kidney transplantation. However, CVD is more prevalent in kidney transplant patients than the general population. Even young transplant recipients experience close to a 10-fold increase in CVD. Therefore, CVD is clearly a significant barrier to staying healthy post-transplantation.
In order to prevent CVD, doctors attempt to predict which patients are most at risk for developing CVD using the Framingham Risk Score (FRS). The FRS is the most common tool used to determine a patient`s CVD risk. It combines traditional cardiac risk factors (age, sex, total cholesterol, high density lipoprotein, smoking status, diabetes, and blood pressure) to identify high risk patients who would benefit from medications to protect their heart, such as aspirin, blood pressure drugs, and cholesterol-lowering drugs. Unfortunately, the FRS may not be an accurate indicator of risk in kidney transplant patients.
In fact, research has shown that the FRS underestimates CVD in kidney transplant patients, especially those patients at the highest risk for developing CVD. This is likely because kidney transplant patients have other important risk factors to consider. These include:
• Pre-transplant cardiac and chronic kidney disease
• Post-transplant exposure to cardiac risk factors
• Transplant-specific risk factors related to immunosuppressant medications, acute rejection, and infection
At St. Michael`s Hospital (SMH), we are using information on our transplant patients to improve the FRS and identify cardiac risk factors that are specific to kidney transplant patients. We are now studying traditional, novel, and transplant-specific risk factors to determine which factors are most important in kidney transplant patients. Novel risk factors such as C-reactive protein, microalbuminuria, uric acid, vitamin D, and
Heart Disease after Kidney Transplantation - Are the Risk Factors the same as the General Population?Dr. Samuel Silver, Resident in Internal Medicine
(con’t on page 3)
TRANSPLANT DIGESTFall 2010, Issue No. 9
2
St. Michael’s HospitalRenal Transplant Program(across the hospital)61 Queen Street 9th Floor Toronto, Ontario, M5C 2T2 Phone: (416) 867-3665
Please send your comments or sugges-tions of topics for future publication to:[email protected]
Disclaimer Note:Views presented in this newsletter are those of the writers and do not necessarily reflect those of St. Michael’s Hospital or the University of Toronto. Subject matter should not be construed as specific medical advice and may not be relevant to individual patient circumstances. For all questions related to your own health please contact your health care provider.
Contact InformationDr. Ramesh Prasad – EditorMeriam Jayoma-Austria, RN, CNeph(C) – Newsletter Coordinator
An important goal of Transplant Digest is to impart kidney transplant-related information to both patients and health care providers in a readable, understandable form that will not become outdated anytime soon. To this end, we have strived to cover the spectrum of important problems that transplant recipients may come across over a number of Digest issues, meant therefore to be kept together in one place. In keeping with this quest for originality, this edition carries new articles on a broad variety of topics, a few of which
From the Editor’s Deskwill interest everybody, and all of which will interest many.
Our medical trainees, the doctors of tomorrow, obliged our request to provide you with their insights in to the risks for heart disease after transplantation, particularly smoking. For the smokers among our patients, may be these articles will finally convince you to quit. We also get many questions about growing new kidneys in a test tube as an alternative to transplant, for which we have provided an article written just for you by one of our senior trainees. We
have a detailed explanation about tacrolimus formulations from our pharmacist, and an article about coping with transplant failure from social work. References are provided for many articles for those desiring further information. Our nurses’ ever-popular post-transplant chat covers the all-pervading problem of anemia. All the authors and staff will find your comments and suggestions about Transplant Digest to be most welcome.
Dr. Ramesh Prasad, Editor
Thank You Josie! All the best! Jozenine Mislang covered Meriam’s one year maternity leave.
3
Kidney regeneration has been a goal nephrologists have been striving for over many years. Recent advances in bioengineering techniques and our understanding of stem cells has brought this goal closer to reality.
Bioengineering a scaffold for a new organ
One of the critical challenges for regeneration of any organ has been how to organize the many different types of cells that make up an organ into a functioning system. Organs such as the kidney are complex networks of various cell types that interact with one another in very specific ways. While researchers have for years been able to grow different kidney cells in culture dishes, they have had difficulty organizing these cells into functioning kidneys. Recently, however, researchers in the United States have reported the ability to create “scaffolds” that help organize cells into proper locations by removing the cells from organs supplied by animal or deceased
human donors. Using the heart1, liver2, and lung3 as examples, these researchers were able to remove all the original donor cells, and then seed the leftover protein skeleton with new cells from potential recipients. The new organs were able to perform basic functions. The importance of this advance is that it allows doctors to potentially generate organs that are made up of cells from the proposed recipient, meaning that theoretically we will not need to use immune suppressing drugs to prevent organ rejection. Interestingly, the first such tissue-engineered transplantation occurred in Spain in 2008, where a woman received a new airway seeded with her own cells.4 While this technique has yet to be applied to the kidney, the above reports suggest that bioengineering kidneys is likely something to expect in the not too distant future.
Stem cells: a new source of kidney cells
Another major challenge has been generating sufficient kidney cells to
regenerate kidney tissue (or to form an entire new kidney). Classically, it has been thought that most adult cells, including many in the kidney, are not able to grow and regenerate new cells in large numbers. As we understand biology better, we now recognize that there are populations of adult stem cells that possess the ability to regenerate cells in the kidney and other organs. Interestingly, the bone marrow has recently been shown to harbour a number of cell types that can help protect and/or regenerate damaged tissue in the kidney.5 Work done at St. Michael’s Hospital, in fact, has shown that special cells from the bone marrow appear to protect the injured kidney from further damage in experimental animal models.6
Together, these exciting advances bring the hope of protecting and regenerating kidney tissue closer to reality. Research into these areas is intensive and ongoing, and hopefully will bear fruit in the near future.
Kidney Regeneration: A New Approach to Chronic Kidney DiseaseDarren Yuen, MD FRCPC
1. Ott, H.C., et al. Perfusion-decellularized matrix: using nature’s platform to engineer a bioartificial heart. Nat Med 14, 213-221 (2008). 2. Uygun, B.E., et al. Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix. Nat Med 16, 814-820. 3. Ott, H.C., et al. Regeneration and orthotopic transplantation of a bioartificial lung. Nat Med 16, 927-933. 4. Macchiarini, P., et al. Clinical transplantation of a tissue-engineered airway. Lancet 372, 2023-2030 (2008). 5. Rookmaaker, M.B., et al. Bone-marrow-derived cells contribute to glomerular endothelial repair in experimental glomerulonephritis. Am J Pathol 163, 553-562 (2003). 6. Yuen, D.A., et al. Culture-Modified Bone Marrow Cells Attenuate Cardiac and Renal Injury in a Chronic Kidney Disease Rat Model via a Novel Antifibrotic
Mechanism. PLoS ONE 5, e9543.
parathyroid hormone are of particular significance, as they have gathered increased attention in the general population, but have not been studied extensively in kidney transplant patients. By routinely measuring these values in kidney transplant patients at SMH, we are in an excellent position to determine if novel risk factors can help improve our ability to predict CVD.
Thus far, we have found that the traditional risk factors, especially diabetes and smoking, which partly make up the FRS remain important in kidney transplant patients. Other important cardiac risk factors include:
• Pre-transplant CVD
• South Asian ethnicity
• Acute rejection
• Delayed graft function
• Estimated glomerular filtration rate (eGFR)
We are currently trying to determine if any of the above risk factors can improve
the FRS. Our hope is that one day we might have a tool for kidney transplant patients to accurately predict which patients are at low
risk, moderate risk, and high risk of developing CVD.
We would like to thank all kidney transplant recipients who participated in
research at SMH in order to help current and future patients.
(con’t from page 1)
Post-Transplant ChatThelma Carino, RN, Jennie Huckle, RN and Fernanda Shamy, RN
1. What is anemia? Is it bad?
Anemia is defined as a hemoglobin level less than 135 g/L in men and 120 g/L in women, on the basis of blood testing. It is not a single disease, but rather an effect from one or more of a number of processes. Anemia is bad because it can cause fatigue and breathlessness, and can cause heart damage. Patients with major illnesses who also have anemia tend to do worse than those without anemia.
2. How can you tell if I have anemia?
You may feel very tired or weak, feel your heart beating faster, and feel breathless or cold. Your nails may lose their natural pinkness, and your mucous membranes (especially the inner part of your lower eyelid) may look very pale. Most commonly anemia is detected by blood testing, before and after your transplant. Usually the compete blood count (CBC) in a lavender-top blood tube is checked regularly, but sometimes blood iron stores, folate and vitamin B12 are also ordered.
3. Why do I have anemia?
Almost all patients with chronic kidney disease have anemia, because a hormone called erythropoietin normally made by the kidneys which tells the bone marrow to make blood, is no longer produced. If your kidney transplant also does not make enough of this hormone you may have anemia. Unfortunately some of your anti-rejection drugs and blood pressure lowering drugs which you need can also contribute. You may be deficient in essential nutrients like iron, folic acid, and vitamin B12. You could also have an infection which makes it difficult for your body to use these nutrients properly. Another important cause is blood loss, such as from heavy menstrual bleeding or bleeding from your stomach or bowels. Sometimes diseases in other organs like the liver or thyroid can also cause anemia. Rarely, you may be breaking down blood cells in your bloodstream as a result of certain diseases or drug reactions. Routine blood testing, even if frequent, is not usually a cause. Anemia is normal and to be expected in pregnancy. It is usually hard to find a single explanation for anemia.
4. I used to have anemia on dialysis. Will I still have it after my transplant?
Some patients continue to have anemia after their transplant due to one or more of the causes listed above. More commonly however it corrects on its own if the transplant is working well. This may take a few months.
5. Will fixing anemia solve all my problems?
No, unless your symptoms were strictly due to anemia. This is rarely the case. Years of chronic kidney disease take their toll on the body, so while fixing anemia may solve some aspects of your health situation, it certainly does not solve everything.
6. Can anemia be improved by diet? How about a multivitamin?
It certainly helps to eat nutritious food. Your body normally absorbs about 10% of the 10-15 mg of iron present in a normal diet, and keeps iron balance by losing and absorbing 1 mg per day. Iron rich foods include liver
POST-TRANSPLANT ANEMIA
4
and lean red meats, seafood, various kinds of beans including soybeans, iron-fortified whole grains including cereals, pasta, and breads, spinach and green leafy vegetables, broccoli, asparagus, and Brussels sprouts. If you are vegetarian, you do not have to become a meat-eater to get more iron!
Good sources of folic acid include dark green, leafy vegetables, whole wheat bread, beans, peas, nuts and seeds, sprouts, oranges, liver and other organ meats, and fortified cereals. Vitamin B12 is richly present in meat and seafood, cheese and eggs. Those who consume no meat or dairy products probably need to take a supplement. Please check with the transplant clinic before taking any multivitamins.
7. Are there medications which can be used to treat anemia?
Sometimes medication becomes necessary. If you are taking an iron supplement, do not stop it without discussing this at a clinic visit, because your hemoglobin may suddenly “crash”. If you have stomach upset from an iron tablet, check with our pharmacist who may be able to find another formulation more suited to you. Do not take iron at the same time as calcium. Do not panic if your stool becomes black with an iron supplement. Sometimes taking vitamin C along with iron allows it to be absorbed better. Very rarely, intravenous iron can be given in the hospital. If you have been prescribed folate tablets or vitamin B12 injections, please do not stop taking them on your own. Rarely, your transplant doctor may decide to change or adjust your transplant drugs or blood pressure drugs to try to help your body correct the anemia. Finally, you may be asked to take injections of erythropoietin or darbopoeitin.
8. I have been told to take injections for my anemia. I am nervous about this.
If you took these injections by yourself before the transplant, it will be no different afterwards. If this is your first time, bring the injection with you back to the transplant clinic as soon as you have filled the prescription and one of the staff will show you how to inject under the skin. Get a family member involved if needed. Remember, you can fill your injection only at one pharmacy because it involves special paperwork. Always keep the syringes stored at the proper temperature so the medication does not get spoiled.
9. Why isn’t my hemoglobin coming back to normal even though I am taking medication for this?
Whenever you start an injection or have the dose changed, your hemoglobin should be repeated in 2 weeks. Often medication adjustment is all that is needed to achieve correction in a few months. Make sure that you are taking your other medications properly, and are eating a proper diet. If the anemia persists, your doctor may choose to refer you to another specialist, such as a hematologist or gastroenterologist. Every attempt is made to avoid blood transfusions. Remember, with injections your target hemoglobin is only 110-120 g/L. Overcorrecting this into what is the “normal” range for normal people may actually be very harmful.
10. I have been told that my hemoglobin is high. This is not anemia, is it?
This rare but we do see this. It is called erythrocytosis. The hemoglobin may go up to as high as 200 g/L. No one knows for sure why this happens but it may be related in some way to the transplant drugs. If this is the case, you may have to come to the clinic so that some blood can be removed (it is useless for donation purposes). Some blood pressure drugs like ACE inhibitors or angiotensin II receptor anatagonists, which can sometimes contribute to anemia, may actually be very useful in this situation.
5

6
“patients who smoked cigarettes had a 51% increased relative risk of graft failure, a 45%
increased risk of mortality, and a 24% increased risk of acute rejection compared
to non-smoker recipients”
Cigarette smoking is an addiction that affects many people worldwide. Unfortunately, many patients with advanced kidney disease or already on dialysis and awaiting kidney transplant are smokers as well as a significant proportion, around 20% of kidney transplant recipients smoke regularly.
The relationships of smoking with hypertension, cardiovascular disease and cancer are well known in the general population. Because of this evidence, smoking is usually highly discouraged by every health professional.
If you happen to be a smoker who is awaiting a kidney transplant or already a lucky recipient with a working graft, or even if you are not affected but just curious, you might want to know: Are there any special considerations with cigarette smoking in kidney transplant patients?
Certainly, there are. According to a study of 4000 kidney recipients in the US, patients who smoked cigarettes had a 51% increased relative risk of graft failure, a 45% increased risk of mortality, and a 24% increased risk of acute rejection compared to non-smoker recipients.
Increased risk of cardiovascular disease and deathYou might have heard about it, that if you have severe kidney insufficiency or are already on dialysis, your risk of cardiovascular disease is much higher (even 10-50-fold higher!) compared to others without kidney disease. Although somewhat less, your risk is still high as a kidney transplant recipient. There is no doubt about the association between smoking and cardiovascular events in the general population. This relationship is more pronounced in kidney transplant recipients and the already very high risk of any cardiac or cerebral event is
amplified by smoking. A study of elderly kidney recipients in Quebec showed that smoking was the greatest modifiable risk factor of death after transplantation. These findings were later confirmed for younger recipients as well. The likelihood of an acute cardiac event within the first two years after transplantation was 3.5-fold higher in smokers compared to non-smokers. Not only cardiac events but also peripheral vascular disease is more common and more severe in smokers.
Increased the risk of early rejectionIf you are a smoker awaiting transplantation, unfortunately, your risk of acute rejection early after transplantation is higher. Smokers had poor early transplant function and worse graft function one year after transplantation. The mechanism how smoking impacts the risk of acute rejection is not clear, but a few studies suggest that it might directly affect the immune system leading to rejection.
Smoking accelerates loss of graft functionIt has been shown that smoking is a risk factor of worsening renal function in different renal diseases, such as diabetes, lupus, IgA nephropathy or polycystic kidney disease. After transplantation, smoking is a risk factor for progressive loss of graft function regardless of your original kidney disease. According to an earlier study, patients who smoked before transplantation had 2.3 fold higher risk of losing the kidney graft compared to non-smokers. In another report, patients who were smokers at the time of transplantation had inferior graft survival rates to patients who were non-smokers: 65% at 5 years and only 48% at 10 years had functioning graft whereas those numbers were 78% and 62% in non-smokers, respectively.
The good news is that there seems to be a benefit to quitting, since patients who no longer smoke at the time of transplantation do better than current smokers: an earlier study showed that patients who quit smoking were not at higher risk of transplant loss compared to whose who never smoked. I should mention that donors’ smoking history also may affect graft function and survival.
How does smoking affect the kidney?Graft loss over the long term is a result of chronic changes in the kidney due to both immunological and non-immune factors. Those processes partly lead to changes of the blood vessels, resulting in stiffer and narrower blood vessels in the transplanted kidney. Similar damage to the blood vessels is caused by smoking and it clearly accelerates the process and contributes to the earlier decline of graft function. In addition, many other structures in the kidney changes in regular smokers.
There are several other mechanisms underlying the adverse effects of smoking and the mechanisms are not yet fully understood. More than 4000 chemicals have been identified in smoke in the form of particles or gases; many of those can accumulate in the kidney (such as lead, cadmium, mercury, and silica) and those are toxic even in small quantities.
In addition, nicotine has a great effect on the circulation increasing blood pressure and the resistance of peripheral blood vessels. It also has the ability to blunt the beneficial effect of certain blood pressure medication, even in the very short term after smoking only one cigarette. The blood flow inside the kidney is also greatly impacted by nicotine, letting it exposed to higher blood pressure and blood flow that can be detrimental over the long term.
Increased risk of malignancy, infection and other consequencesCancer is a well known complication of transplantation, the risk of malignancy is 3-5 fold higher compared to the general population and cancers are usually
Smoking and kidney transplantation: Don’t let your kidney go up in smoke!Csaba Ambrus, M.D., Ph.D

7
more aggressive. Age, sun exposure and smoking history are the most important predictors of cancer development. Various cancer types have been associated with smoking after transplantation, especially lung and lip cancer.
Smoking will damage lung structure and also inhibit the natural clearance mechanisms of the airways. As a consequence, it puts you at greater risk for lung infections, bronchitis and pneumonia. Smoking also increases the acid production in your stomach and this will delay the healing any ulcers you may develop. It also impairs the ability of red cells to carry oxygen, so less oxygen will reach the tissues in the body and this decreases the ability to heal. All these effects are more severe if you take immunosuppressive medications. Furthermore, there are studies suggesting that smoking is also a risk factor for development of diabetes after transplantation.
Is it worth quitting even if someone has been smoking for many years?We do not have much evidence about the effect of smoking cessation on kidney function. However, as studies showed in the general population, the risk of any event related to smoking will decrease after quitting. As I earlier mentioned, patient who quit few years before transplantation had better graft function and their graft last longer compared to those who continued smoking. So it is never late to quit!
How can I get help to quit smoking?Weaning from smoking is a difficult process that needs the cooperation of both patient and health personal. It requires regular counselling and often drug support such as nicotine patch or other medication. Ask your doctor for help!
I can give you few tips to help you quit:
• Avoid beverages that contain caffeine! Caffeine, found in coffee, tea, and many soft drinks, can stimulate your urge to smoke again.
• Drink more liquids and eat fruits during the first three non-smoking days, provided your kidney function allows you to do so (!!). Body fluids of smokers have high concentrations of nicotine; as these concentrations decrease nicotine cravings increase. Extra liquid can act as an alternative to cigarettes and help nicotine pass out of your body.
• Use deep breathing! When the craving to smoke strikes, you should take slow, deep breaths. This will help you relax long enough to consciously decide not to smoke. It will also help supply your brain and the rest of the body with oxygen. Take in a deep breath with your mouth wide open, bend at the waist, and breathe out; repeat two or three times. Stop if you begin to feel dizzy.
• Take your vitamins! Taking a B vitamin may help diminish the nervousness and mood swings that can occur when one tries to stop smoking. Take vitamin C if
you are unable to eat fruit. Remember to consult your doctor before taking vitamins.
• Exercise regularly! An aerobic workout, such as walking briskly, can improve lung capacity and vascular tone, and help prevent depression. Consult with your doctor or physiotherapist before beginning any exercise program.
• Join a smoking cessation group! These groups can be helpful for discussing feelings and learning from others in the same situation. Check the Yellow Pages or your local heart, lung, or cancer society chapter to find a convenient group.
It is not easy to give up smoking. You may become anxious or irritable. You may develop headaches, nervousness, dizziness, muscle cramps, fatigue, sleepiness, increased sweating, as well as difficulty focusing your attention, a loss of appetite, increased craving for food, or an intense craving to smoke. However, if you stick to your decision not to smoke, you will be breaking a habit that is harming your health and, in time, the “withdrawal” symptoms will diminish and you’ll feel better than ever before.
Your ability to choose not to smoke grows stronger each time you repeat the choice. Instead of thinking about how much you want to smoke, remind yourself of smoking’s harmful effects and the health benefits that will be yours without smoking.
References1. Tips to quit smoking were taken from the homepage of the Columbia University, with minor modifications and without the author’s permission: http://www.cumc.columbia.edu/dept/cs/pat/kidneypancreastx/life.html
2. Cosio, F. G., Falkenhain, M. E., Pesavento, T. E., Yim, S., Alamir, a., Henry, M. L., et al. (1999). Patient survival after renal transplantation: II. The impact of smoking. Clinical transplantation, 13(4), 336-41.
3. Dantal, J., & Pohanka, E. (2007). Malignancies in renal transplantation: an unmet medical need. NDT, 22 Suppl 1, i4-10.4. Gallagher, M. P., Kelly, P. J., Jardine, M., Perkovic, V., Cass, A., Craig, J. C., et al. (2010). Long-term cancer risk of immunosuppressive regimens after kidney
transplantation. JASN, 21(5), 852-8.5. Kasiske, B. L., & Klinger, D. (2000). Cigarette smoking in renal transplant recipients. JASN, 11(4), 753-9.6. Nogueira, J. M., Haririan, A., Jacobs, S. C., Cooper, M., & Weir, M. R. (2010). Cigarette smoking, kidney function, and mortality after live donor kidney
transplant. AJKD, 55(5), 907-15.7. Orth, S. R., & Hallan, S. I. (2008). Smoking: a risk factor for progression of chronic kidney disease and for cardiovascular morbidity and mortality in renal
patients--absence of evidence or evidence of absence? CJASN, 3(1), 226-36.8. Sezer, S., Bilgic, a., Uyar, M., Arat, Z., Ozdemir, F. N., Haberal, M., et al. (2006). Risk factors for development of posttransplant diabetes mellitus in renal
transplant recipients. Transplantation proceedings, 38(2), 529-32.9. Sung, R. S., Althoen, M., Howell, T. a., Ojo, a. O., & Merion, R. M. (2001). Excess risk of renal allograft loss associated with cigarette smoking.
Transplantation, 71(12), 1752-7.10. van Leeuwen, M. T., Grulich, A. E., McDonald, S. P., McCredie, M. R., Amin, J., Stewart, J. H., et al. (2009). Immunosuppression and other risk factors for
lip cancer after kidney transplantation. Cancer epidemiology, biomarkers & prevention, 18(2), 561-9.11. van Walraven, C., Austin, P. C., & Knoll, G. (2010). Predicting potential survival benefit of renal transplantation in patients with chronic kidney disease.
CMAJ, 182(7), 666-72.12. Yavuz, a., Tuncer, M., Gürkan, a., Demirbas, a., Süleymanlar, G., Ersoy, F., et al. (2004). Cigarette smoking in renal transplant recipients. Transplantation
proceedings, 36(1), 108-10.
8
Coping With Chronic Renal Allograft FailureCarmen Morris, MSW DCCP/Nephrology
Allograft failure often causes distress for patients for whom kidney transplant represented a source of hope. While explanation for this distress vary from person to person. The processes used to talk about loss, bereavement, grief, and mourning, may be used account for your emotional reactions to allograft failure.
Bereavement is the state where a person experiences feelings of sadness and loneliness after having suffered a loss that is either physical or symbolic. From this perspective, you experience sadness not only because you have lost the kidney, but also because of the unfulfilled dreams and wishes you have associated with having a successful transplant. The length of time for bereavement varies from person to person.
Grief is the normal reaction to loss that may manifests itself in physical, social, or emotional forms. Physical reactions may include changes in sleep or appetite, and tiredness. Emotional reactions may include anger, guilt, and anxiety. Social reactions may include both positive and negative feelings about roles in the family or employment. As with bereavement, your grief will depend on the situation surrounding the loss of the allograft.
Mourning is the conscious or unconscious cultural reaction to a loss. It is the ongoing process of incorporating the loss into your ongoing life and is influenced by customs
and rituals and by society’s guidelines for coping with loss. You may experience mourning in three phases, shock and disbelief that the kidney is failing, disorganization and sadness, and followed by reorganization.
Tips for Coping with Chronic Allograft Failure
The stage of reorganization is difficult to achieve at times. You may find that you are still having difficulty coping on your own; as your emotions may result in feelings of more distress. Take steps to find coping support. You may find ‘grief work’ helpful, by way of easing emotional distress. Patients report that it enhances their ability to move beyond the news of chronic graft failure.
‘Grief work’ entails a series of steps you need to finish to enable you to overcome your loss. These steps include the process of accepting your losses, experiencing your pain, adjusting to your new situation, and ultimately reinvesting your emotional energy into the process of moving forward. Successful ‘grief work’ require you to ‘engage’ with a caring health professional, who is there to guide you through the number of steps, and reassure you that your emotions are natural coping reactions.
In addition, initiate talks with your medical team about what your treatment options are for the future. The possibility of another transplant is often a source of hope and optimism for patients. The fact is; a failed transplant does not necessarily preclude you from having a successful transplant in the future.
Finally, strengthen your support system, and seek help to access community resources. There is evidence to suggest that you will begin to feel that you have regained control over your life and better able to transition successfully to possible dialysis or re-transplantation; with the right supports in place.
Cited From:
Clara D Neyhart, The patient with progressive renal insufficiency and a failing transplant, Nephrology Nursing Journal (June, 2002);
Gill, Paul, Lowes, Lesley, Kidney Transplant Failure experience: a Longitudinal Study, Nephrology Nursing Journal, (June, 2002);
“Bereavement, Mourning, and Grief”, the National Cancer Institute (June, 2010).

9
Approximately 1.8 million adult Canadians are living with diabetes mellitus. The Canadian Diabetes Association defines diabetes as a metabolic disorder characterized by high blood sugar due to a problem with insulin secretion, insulin action or both. Diabetes is associated with complications affecting various organs in the body-particularly the kidneys, eyes, nerves, heart and blood vessels to the feet and brain.
About 50% of people with diabetes have chronic kidney disease (CKD). CKD is when the kidneys are damaged and are unable to function properly. Diabetes is the one of the leading causes of CKD. When kidney disease worsens, it may eventually lead to kidney failure requiring dialysis or transplant to maintain life.
Blood Sugar control and Kidney Failure
It may become difficult to control blood sugars when the kidneys fail to work properly especially when taking insulin or diabetes pills. Insulin and some diabetes pills are normally metabolized or broken down by the kidney. However, when the kidneys are no longer working, the action of insulin is much longer because of the kidney’s inability to properly break it down. This also happens with certain diabetes pills, which can result in higher than normal levels of the medication in the blood. This can increase one’s risk for hypoglycemia or low blood sugar. Therefore, when kidney failure occurs, a significant reduction in the dose of insulin or diabetes pills is often necessary to avoid low blood sugar. As a result, sometimes people with diabetes and kidney failure can manage their blood sugars without any medication. This can be misleading as people may believe their diabetes has been cured.
Blood Sugar control and Kidney Transplant
Controlling blood sugars after kidney transplant in someone with diabetes can also be challenging for a few reasons. Firstly, some of the usual transplant medications raise blood sugar levels, namely, prednisone, tacrolimus, cyclosporine and possibly sirolimus. Secondly, a healthy transplanted kidney is now able to metabolize or break down insulin and diabetes pills normally. Therefore, the requirements of these medications to control blood sugar often are much more than before transplant. Also, the physical stress of surgery can cause high blood sugars particularly in persons with diabetes. Improved appetite and weight gain following kidney transplantation may also contribute to higher blood sugars.
Diabetes Management after Kidney Transplant
Close monitoring of blood sugar is very important after kidney transplant. Blood sugar is routinely checked with other lab tests. Also, self-monitoring of blood sugar at home is encouraged especially if taking insulin or diabetes pills. Monitoring blood sugar informs us if changes to the diabetes regimen are necessary. High blood sugars can lead to dehydration if not treated appropriately. Dehydration can be stressful to the new transplanted kidney.
The targets for good blood sugar control are:
• Fasting blood sugar and before meals: 4-7 mmol/L
• Blood sugar 2 hours after a meal: 5-10 mmol/L
It is not uncommon for a person with diabetes on diabetes pills to require insulin therapy to control blood sugars after kidney transplant, especially when receiving high doses of prednisone. Insulin therapy may be temporary in some cases, and sometimes is needed indefinitely to keep blood sugars well controlled.
Following a healthy diet after transplant is part of the overall management of diabetes. A registered dietitian can help with this.
Lastly, incorporating regular exercise is important for diabetes management as it helps to lower blood sugar, promotes weight loss and improves overall health, including heart health.
An Introduction to Diabetes and Kidney TransplantTess Montada-Atin, NP MN CDE
10
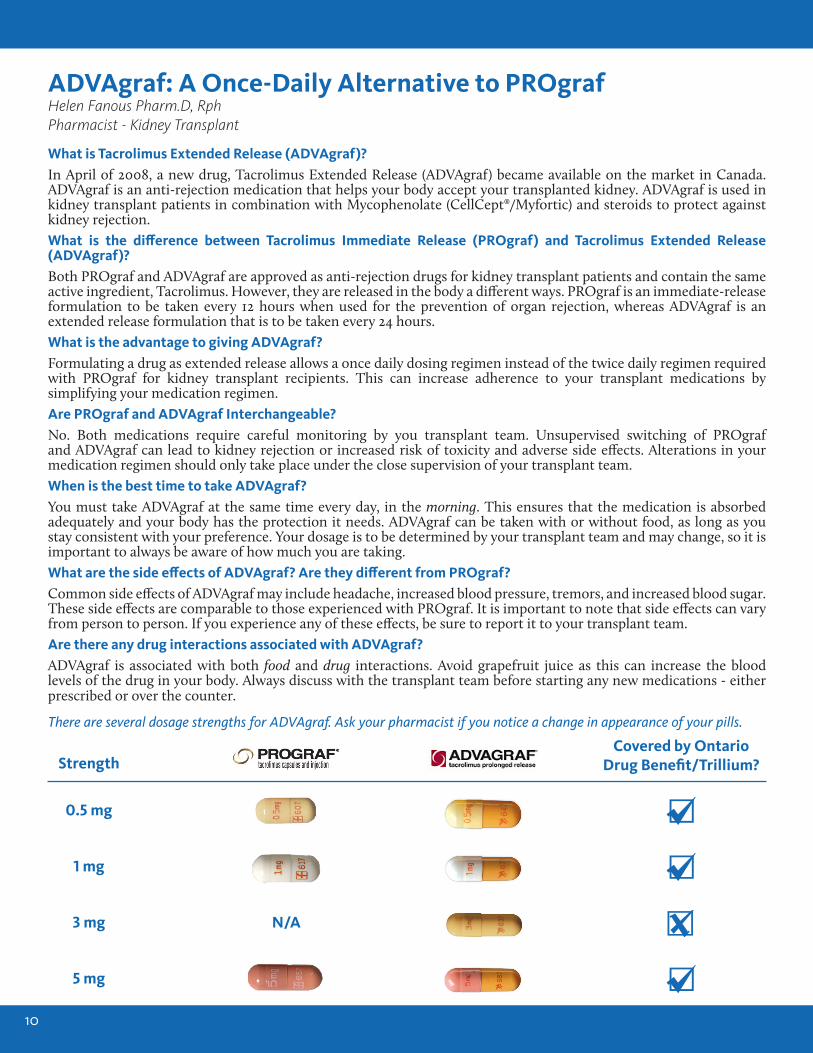
What is Tacrolimus Extended Release (ADVAgraf)?In April of 2008, a new drug, Tacrolimus Extended Release (ADVAgraf) became available on the market in Canada. ADVAgraf is an anti-rejection medication that helps your body accept your transplanted kidney. ADVAgraf is used in kidney transplant patients in combination with Mycophenolate (CellCept®/Myfortic) and steroids to protect against kidney rejection. What is the difference between Tacrolimus Immediate Release (PROgraf) and Tacrolimus Extended Release (ADVAgraf)?Both PROgraf and ADVAgraf are approved as anti-rejection drugs for kidney transplant patients and contain the same active ingredient, Tacrolimus. However, they are released in the body a different ways. PROgraf is an immediate-release formulation to be taken every 12 hours when used for the prevention of organ rejection, whereas ADVAgraf is an extended release formulation that is to be taken every 24 hours.What is the advantage to giving ADVAgraf?Formulating a drug as extended release allows a once daily dosing regimen instead of the twice daily regimen required with PROgraf for kidney transplant recipients. This can increase adherence to your transplant medications by simplifying your medication regimen.Are PROgraf and ADVAgraf Interchangeable?No. Both medications require careful monitoring by you transplant team. Unsupervised switching of PROgraf and ADVAgraf can lead to kidney rejection or increased risk of toxicity and adverse side effects. Alterations in your medication regimen should only take place under the close supervision of your transplant team. When is the best time to take ADVAgraf?You must take ADVAgraf at the same time every day, in the morning. This ensures that the medication is absorbed adequately and your body has the protection it needs. ADVAgraf can be taken with or without food, as long as you stay consistent with your preference. Your dosage is to be determined by your transplant team and may change, so it is important to always be aware of how much you are taking. What are the side effects of ADVAgraf? Are they different from PROgraf?Common side effects of ADVAgraf may include headache, increased blood pressure, tremors, and increased blood sugar. These side effects are comparable to those experienced with PROgraf. It is important to note that side effects can vary from person to person. If you experience any of these effects, be sure to report it to your transplant team.Are there any drug interactions associated with ADVAgraf?ADVAgraf is associated with both food and drug interactions. Avoid grapefruit juice as this can increase the blood levels of the drug in your body. Always discuss with the transplant team before starting any new medications - either prescribed or over the counter.
ADVAgraf: A Once-Daily Alternative to PROgrafHelen Fanous Pharm.D, RphPharmacist - Kidney Transplant
StrengthCovered by Ontario
Drug Benefit/Trillium?
1 mg
0.5 mg
3 mg N/A
5 mg
There are several dosage strengths for ADVAgraf. Ask your pharmacist if you notice a change in appearance of your pills.
NOTES
Funding for this publication provided by Hoffmann-La Roche Limited


















