Transmission of Influenza A Pandemic (H1N1) 2009 Virus in a Long‐Term Care Facility in Ontario,...
4
Transmission of Influenza A Pandemic (H1N1) 2009 Virus in a Long‐Term Care Facility in Ontario, Canada • Author(s): David C. Alexander, PhD; Anne‐Luise Winter, BScN, MHSc; AliReza Eshaghi, PhD; Kathleen Dooling, MD, MPH; Crystal Frenette, BScN; Eileen de Villa, MD, MHSc; Monali Varia, MHSc; Alex Marchand‐Austin, BSc; Frances Jamieson, MD; Jonathan B. Gubbay, MD Source: Infection Control and Hospital Epidemiology, Vol. 31, No. 12 (December 2010), pp. 1300-1302 Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiology of America Stable URL: http://www.jstor.org/stable/10.1086/657337 . Accessed: 15/05/2014 03:00 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. . The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaborating with JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology. http://www.jstor.org This content downloaded from 194.29.185.134 on Thu, 15 May 2014 03:00:05 AM All use subject to JSTOR Terms and Conditions
Transcript of Transmission of Influenza A Pandemic (H1N1) 2009 Virus in a Long‐Term Care Facility in Ontario,...

Transmission of Influenza A Pandemic (H1N1) 2009 Virus in a Long‐Term Care Facility inOntario, Canada • Author(s): David C. Alexander, PhD; Anne‐Luise Winter, BScN, MHSc; AliReza Eshaghi, PhD;Kathleen Dooling, MD, MPH; Crystal Frenette, BScN; Eileen de Villa, MD, MHSc; Monali Varia,MHSc; Alex Marchand‐Austin, BSc; Frances Jamieson, MD; Jonathan B. Gubbay, MDSource: Infection Control and Hospital Epidemiology, Vol. 31, No. 12 (December 2010), pp.1300-1302Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/10.1086/657337 .
Accessed: 15/05/2014 03:00
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org
This content downloaded from 194.29.185.134 on Thu, 15 May 2014 03:00:05 AMAll use subject to JSTOR Terms and Conditions

1300 infection control and hospital epidemiology december 2010, vol. 31, no. 12
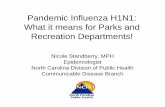
figure 1. Symptom onset dates for cases among long-term carefacility staff (white) and residents (gray) plus the community contact(hatched). Laboratory testing confirmed pH1N1 infection in thecommunity contact and 5 residents (black).
From the Division of Infectious Diseases, Department of Pediatrics,Columbia University (S.J.P., E.R., L.S.), and the Department of InfectionControl and Prevention, New York–Presbyterian Hospital (L.S.), New York,New York; and the Division of Infectious Diseases, Department of InfectionPrevention and Control, the Children’s Hospital of Philadelphia (T.Z., P.P.),and the University of Pennsylvania School of Medicine (T.Z., P.P.),Philadelphia, Pennsylvania.
Address reprint requests to Sameer J. Patel, MD, Division of PediatricInfectious Diseases, Department of Pediatrics, Columbia University, 622 West168th Street, PH 4W-475, New York, NY 10032 ([email protected]).
Received March 31, 2010; accepted June 14, 2010; electronically publishedOctober 21, 2010.� 2010 by The Society for Healthcare Epidemiology of America. All rightsreserved. 0899-823X/2010/3112-0015$15.00. DOI: 10.1086/657334
references
1. Centers for Disease Control and Prevention. 12-step program to preventantimicrobial resistance in health care settings. http://www.cdc.gov/drugresistance/healthcare/ Reviewed September 15, 2005. Accessed December2009.
2. Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians followclinical practice guidelines? A framework for improvement. JAMA 1999;282(15):1458–1465.
3. Wester C, Durairaj L, Evans AT, Schwartz DN, Husain S, Martinez E.Antibiotic resistance: survey of physician perceptions. Arch Intern Med2002;162:2210–2216.
4. Hersh AL, Beekmann SE, Polgreen PM, Zaoutis TE, Newland JG. Anti-microbial stewardship programs in pediatrics. Infect Control Hosp Epi-demiol 2009;30:1211–1217.
5. Dellit TH, Owens RC, McGowan JE Jr, et al; Infectious Diseases Societyof America, Society for Healthcare Epidemiology of America. InfectiousDiseases Society of America and the Society for Healthcare Epidemiologyof America guidelines for developing an institutional program to enhanceantimicrobial stewardship. Clin Infect Dis 2007;44:159–177.
Transmission of Influenza A Pandemic(H1N1) 2009 Virus in a Long-Term CareFacility in Ontario, Canada
Outbreaks of respiratory illness are common in long-termcare facilities (LTCFs). In contrast, during the first wave ofthe 2009 influenza pandemic, outbreaks due to the pandemicinfluenza A (H1N1) 2009 strain (pH1N1) were rare in NorthAmerica. As late as August 2009, the US Centers for DiseaseControl and Prevention had reported no pH1N1 cases amongLTCF residents.1 In Ontario, Canada, only 2 such outbreakswere identified.2,3 This report describes the first outbreak,which included pH1N1 transmission within the LTCF.
At the end of May 2009, an increase in cases of respiratoryillness among staff and residents was detected at a moderatelysized LTCF (approximately 180 residents and 220 staff) in PeelRegion, Ontario (population, 1.24 million). Public health au-thorities were notified, and on June 2, a respiratory infectionoutbreak was declared. Control measures were implemented,including isolation of ill residents, restriction of visitors and
social activities, increased facility cleaning, initiation of dropletand contact precautions, and the use of N95 respirators. OnJune 5, testing at the Public Health Laboratories–Toronto ofthe Ontario Agency for Health Protection and Promotion iden-tified pH1N1 in a respiratory specimen obtained from oneLTCF resident. Prophylactic oseltamivir treatment was offeredto all staff and was commenced for all asymptomatic residents.All patients recovered, and none were hospitalized. The out-break was declared over on June 17.
During the outbreak period, a total of 9 residents and 14staff met the criteria for respiratory illness and presented with2 or more of the following new symptoms: runny nose orsneezing, stuffy nose, sore throat or difficulty swallowing, drycough, swollen glands, or fever. Additional symptoms, includ-ing malaise, myalgia, loss of appetite, headache, and chills, werealso considered. Five residents, including 2 who shared a room,had pH1N1 infections confirmed by both real-time polymerasechain reaction (PCR)–based testing and viral culture. Fourother residents tested negative for a standard panel of causativeorganisms. No staff submitted specimens for testing, but acommunity contact, the infant grandchild of a staff member,had been ill with laboratory-confirmed pH1N1 just before theLTCF outbreak began. Symptom onset dates for all patientsare shown in Figure 1.
The mean age of all LTCF residents was 80 years. The 9ill residents had a median age of 70 years, and all had co-morbidities (eg, paraplegia, dementia, and endocrine disor-ders), but there were differences between the 5 patients withlaboratory-confirmed pH1N1 and the 4 with negative testresults. The persons with confirmed cases were younger (me-dian age, 56 vs 87 years) and experienced a longer durationof illness (range, 10–14 days vs 6–10 days). The persons withnegative laboratory test results reported more diverse symp-toms (none had all of the symptoms of fever, cough, andcongestion), whereas all persons with confirmed cases re-
This content downloaded from 194.29.185.134 on Thu, 15 May 2014 03:00:05 AMAll use subject to JSTOR Terms and Conditions

research briefs 1301
ported fever, cough, and congestion. Clinical courses wereuneventful, although 1 resident with confirmed pH1N1 de-veloped chest radiograph–confirmed pneumonia.
Ages for staff members with cases ranged from 23 to 59years, with a median age of 33 years—a decade lower thanthe median age of all staff (43 years). Among 9 staff memberswith available medical histories, only 1 reported the existenceof an underlying medical condition. The duration of illnessranged from 3 to 27 days (median duration, 6 days). No staffexperienced complications.
Whole-genome sequencing of pH1N1 isolates from the 6patients with confirmed cases was performed with a modifiedversion of the published World Health Organization pro-tocol.4 In brief, virus was cultured in Madin-Darby caninekidney cells. Total RNA was extracted with a NucliSENSeasyMAG system (bioMerieux), and cDNA was generatedwith the SuperScript III One-Step RT-PCR System (Invitro-gen) using 46 oligonucleotide pairs containing universal M13primer sequences. The BigDye Terminator v3.1 Cycle Se-quencing kit (Applied Biosystems) and a 3730XL DNA An-alyzer (Applied Biosystems) were used for sequencing. Nu-cleotide data was assembled with Vector NTI Advance 11(Invitrogen). For each strain, a 13,166-nt semantide was gen-erated by concatenating data from all 8 genomic segments.
Sequencing revealed extensive nucleotide homology amongthe LTCF isolates. Two were identical, 1 contained a singlesynonymous nucleotide substitution, and the remaining 2exhibited distinct, nonsynonymous substitutions in theirpolymerase segments. The community contact strain was dif-ferent and exhibited 17 nucleotide changes, including 8 non-synonymous substitutions.
Between April 20 and June 12, 2009, there were 75 out-breaks of respiratory infection reported by LTCFs in Ontario.2
Although there was extensive community spread of pH1N1during this period, resident cases of pH1N1 were confirmedin only 2 LTCF outbreaks.2,3 Enterovirus and/or rhinovirus(26 of 75 outbreaks), parainfluenza (23 of 75), and meta-pneumovirus (16 or 75) were responsible for the majority ofrespiratory infections. LTCF residents are typically elderlyand/or possess underlying medical conditions that put themat risk for numerous illnesses, yet emerging evidence suggeststhat elderly individuals are less likely to acquire pH1N1.5-7
Consistent with this, 3 of the 5 pH1N1-positive residents inthis outbreak were less than 60 years of age, and only 1 wasolder than 80 years of age (the median age of all LTCFresidents).
The epidemic curve and case investigation data suggestedthat the outbreak originated with the grandchild of a staffmember. Whole-genome sequencing data confirmed that theresident isolates were genetically homogenous, which is con-sistent with the introduction of pH1N1 from a commonsource and transmission of a single strain within the LTCF.However, sequencing also revealed that the isolate from thecommunity contact was genetically distinct from the LTCFstrains and was thus not responsible for the outbreak. These
findings highlight the power of molecular epidemiology tech-niques to complement traditional outbreak investigationmethods.
acknowledgments
We thank the LTCF staff and residents and acknowledge the efforts of thecommunicable disease investigation and surveillance staff at Peel PublicHealth and the Virus Isolation and Molecular Diagnostics staff at the OntarioAgency for Heath Protection and Promotion, Public Health Laboratories-Toronto.
Financial support. Genome sequencing work was supported by the On-tario Ministry of Health and Long-Term Care funding for “Severe RespiratoryIllness.”
Potential conflicts of interest. All authors report no conflicts of interestrelevant to this article.
David C. Alexander, PhD;Anne-Luise Winter, BScN, MHSc; AliReza Eshaghi, PhD;
Kathleen Dooling, MD, MPH; Crystal Frenette, BScN;Eileen de Villa, MD, MHSc; Monali Varia, MHSc;
Alex Marchand-Austin, BSc; Frances Jamieson, MD;Jonathan B. Gubbay, MD
From the Public Health Laboratories-Toronto, Ontario Agency for HealthProtection and Promotion (D.C.A., A.-L.W., A.E., F.J., J.B.G.), and NationalMicrobiology Laboratory, Public Health Agency of Canada, Toronto (A.M.-A.), and Peel Public Health, Brampton (K.D., C.F., E.d.V., M.V.), Ontario,Canada.
Address reprint requests to David C. Alexander, PhD, Ontario Agency forHealth Protection and Promotion, 101 Resources Road, Room B04, Toronto,Ontario, Canada, M9P 3T1 ([email protected]).
Received May 27, 2010; accepted June 16, 2010; electronically publishedOctober 28, 2010.� 2010 by The Society for Healthcare Epidemiology of America. All rightsreserved. 0899-823X/2010/3112-0016$15.00. DOI: 10.1086/657337
references
1. National Center for Immunization and Respiratory Diseases, Centers forDisease Control and Prevention. Use of influenza A (H1N1) 2009 mono-valent vaccine recommendations of the Advisory Committee on Immu-nization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2009;58:1–8.
2. Marchand-Austin A, Farrell DJ, Jamieson FB, et al. Respiratory infectionin institutions during early stages of pandemic (H1N1) 2009, Canada.Emerg Infect Dis 2009;15:2001–2003.
3. Ontario Ministry of Health and Long-Term Care. Ontario influenzabulletin 2008–2009 season, surveillance week 24 (June 14, 2009–June20, 2009). 2009. http://www.health.gov.on.ca/english/providers/program/pubhealth/flu/flu_08/bulletins/flu_bul_01_20090620.pdf. Accessed Oc-tober 13, 2010.
4. World Health Organization. Global Alert and Response. Sequencingprimers and protocol. Global Alert and Response Information resources.2009. http://www.who.int/csr/resources/publications/swineflu/sequencing_primers/en/index.html. Accessed April 20, 2010.
5. Tuite AR, Greer AL, Whelan M et al. Estimated epidemiologic parametersand morbidity associated with pandemic H1N1 influenza. CMAJ 2010;182:131–136.
6. Writing Committee of the World Health Organization Consultation onClinical Aspects of Pandemic (H1N1) 2009 Influenza. Clinical aspects ofpandemic 2009 influenza A (H1N1) virus infection. N Engl J Med 2010;362:1708–1719.
This content downloaded from 194.29.185.134 on Thu, 15 May 2014 03:00:05 AMAll use subject to JSTOR Terms and Conditions

1302 infection control and hospital epidemiology december 2010, vol. 31, no. 12
table 1. Molecular Characteristics of Methicillin-Resistant Staphylococcus aureus Isolates Recovered from Healthcare Workers and fromEnvironment Samples in a Hospital
Source Ward SCCmec spa MLST pvl sea sec seg sei seh agrMIC of
oxacillin, mg/mL
Clothes-changing room Dermatology III t037 ST239 � � � � � � I 1256Medical doctor Neurosurgery V t458 ST573 � � � � � � II 1.5Staff nurse General surgery IVc t664 ST72 � � � � � � I 1.5Staff nurse Neurosurgery IV t548 ST1178 � � � � � � II 2Sink Dermatology V t127 ST1 � � � � � � III 8Resuscitation trolley Neurosurgery III t421 ST239 � � � � � � I 1256Bed rails Neurosurgery III t037 ST239 � � � � � � I 1256
note. MIC, minimum inhibitory concentration; MLST, multilocus sequence typing; pvl, Panton-Valentine leukocidin gene; SCCmec, staphylococcalcassette chromosome mec; sea, staphylococcal enterotoxin A; sec, staphylococcal enterotoxin C; seg, staphylococcal enterotoxin G; seh, staphylococcal enterotoxinH; sei, staphylococcal enterotoxin I; �, positive; �, negative.
7. Miller E, Hoschler K, Hardelid P, et al. Incidence of 2009 pandemicinfluenza A H1N1 infection in England: a cross-sectional serological study.Lancet 2010;375:1100–1108.
Environmental Contaminationin the Hospital as a Possible Sourcefor Nosocomial Infection with Methicillin-Resistant Staphylococcus aureus
Methicillin-resistant Staphylococcus aureus (MRSA) ranks topamong the clinically most relevant nosocomial pathogens.During our earlier clinical study of MRSA epidemiology inthe largest public hospital in Malaysia, we found a high prev-alence of sequence type (ST) 239–staphylococcal cassette chro-mosome mec (SCCmec) III/IIIA MRSA (1,877 [44.1%] of 4,280isolates) harbored in 360 (92.5%) of all 389 case patients.1 Totrace the source of nosocomial MRSA transmission, we inves-tigated the impact of healthcare workers (HCWs) and the hos-pital environment. We assessed the prevalence and the molec-ular characteristics of MRSA strains isolated from the studysources and compared these with clinical isolates obtainedpreviously.
A total of 500 samples (40 environmental specimens and460 nasal swab specimens) were obtained from HCWs (11medical specialists [2.4%], 82 general physicians [17.8%], 11pharmacists [2.4%], 16 physiotherapists [3.5%], and 340 staffnurses [74%]) in the wards with the highest rates of MRSAcolonization and infection (ie, general medicine, urology/neph-rology, surgery, and dermatology) during November–Decem-ber 2009. All samples were subjected to S. aureus– and MRSA-specific isolation procedures, in accordance with standardguidelines.1 MRSA isolates were tested by polymerase chainreaction for the mecA gene and were subjected to staphylococcalprotein A gene (spa) sequencing (http://spaserver.ridom.de),pulsed-field gel electrophoresis (PFGE), SCCmec typing, andmultilocus sequence typing.1,2 All isolates were screened for the
presence of the virulence genes pvl (Panton-Valentine leuko-cidin); fnb (fibronectin-binding protein); cna (collagen adhe-sin gene); sea, seb, sec, sed, see, seg, seh and sei (staphylococcalenterotoxins A–I, respectively); tsst (toxic shock syndrome tox-in); and eta and etb (exfoliative toxins a and b, respectively).1
Of the 460 HCWs, 94 were nasally colonized with S. aureus,including 2 medical specialists, 17 medical doctors, 1 phar-macist, 3 physiotherapists, and 71 staff nurses. Three HCWs(0.65%) tested positive for MRSA, with spa type t664-ST72-SCCmec IVc, t458-ST 573-SCCmec IV, and t548-ST1178-SCCmec V in the isolates from 1 HCW each. Among the 40environmental samples, 4 (10%) were found to be MRSApositive. Two isolates (50%), which were recovered frombed rails and the clothes-changing room, were t037/ST239-SCCmec III. One strain (25%), which was isolated from theresuscitation trolley, had type t421/ST239-SCCmec III. Final-ly, 1 t127/ST1-SCCmecV strain (25%) was cultured from thesink in the dermatology ward. Virulence profile investigationshowed that all strains were positive for adhesion genes, suchas fnbA, cna, and the biofilm-related genes icaA and icaD.Among the superantigen genes tested, sea was the most prev-alent and was detected in all environmental strains (ST239and ST1). A sec, seg, and sei gene cluster was found onlyamong the strains from HCWs (ST548, ST573, and ST1178),whereas seh and pvl were isolated from a single environmentalstrain (ST1). None of the other superantigenic toxin genes(eg, seb, sed, tsst, eta, and etb) were detected in any of theisolates. Typing for agr grouped 4 isolates as agr I (ST239and ST72), 2 strains as agr II (ST573 and ST1178), and 1strain (ST1) as agr III (Table 1). A dendrogram based onPFGE revealed that the MRSA strains were genotypically dis-tinct, except for strains 489 and 496 (ST239), which werehighly similar. Antibiotic susceptibility profiles and results ofthe Etest (AB Biodisk) illustrated that MRSA strains fromHCWs were susceptible to oxacillin, with a low minimuminhibitory concentration (ie, less than 2 mg/L), and wereresistant to erythromycin. ST239 and ST1 environmentalstrains were multidrug resistant, with minimum inhibitoryconcentrations of oxacillin of more than 256 mg/L and 8 mg/L, respectively.3
This content downloaded from 194.29.185.134 on Thu, 15 May 2014 03:00:05 AMAll use subject to JSTOR Terms and Conditions