Transfusion - indications, contraindications, technique...What to do before transfusion - physician...
52
Transfusion - indications, contraindications, technique Emoke Šteňová Eva Kováčová Jozef Bulas
Transcript of Transfusion - indications, contraindications, technique...What to do before transfusion - physician...

Transfusion - indications, contraindications, technique
Emoke ŠteňováEva Kováčová
Jozef Bulas

Function and Properties of Blood
• A vehicular organ that perfuses all other organs
• Delivers nutrients to cells and removes wastes
• Hemostatic governors are carried to and from appropriate sites
• Regulation - pH, heat, osmolality
• Protection – blood clot, WBC attack microbes, antibodies -immunity

Fluid Compartments

Definition
• Blood transfusion is defined as a process of receivingblood products into one´s circulation intravenously.
• Usually life saving maneuver
• The transfusion therapy is given in the situation when there is not the possibility to manage the clinical status of patient by medicamentous (drug) therapy.
• Types – autologous, allogenic

Aim of Tranfusion
•The aim of transfusion therapy is not to achieve
- normal hemoglobin value,
- blood cell count,
- or level of clotting factors,
but the management or prevention of clinical
complications in patients.

What to do before transfusion -physician
He/she is obliged to:
• inform the patient about planned administration of transfusion medicine
and possible risks.
• obtaine informed consent from patient and/or his relatives with the
suggested transfusion therapy.
• write this information into the medical record,
• sign it legibly and to mark these notes by the doctor‘s personal stamp.
• select the most appropriate type and amount of transfusion product.
• indicate the administration of transfusion, must clearly write into patient´s
medical record the reason for administration of transfusion.
• check the identity of patient, correctly fill in the formular for transfusion
request and to fill in the record of transfusion

The blood is a living tissue
➢ The transfusion of blood or its cellular componentsfrom the donnor to recipient is a kind of transplantation with its biological consequences.
➢ The aim of hemotherapy is to achieve the optimal therapeutic efficacy with the least threatening of the patient by the side-effects, potentially connected with hemotherapy.
➢ The missing blood component needs to be replaced by transfusion product with the minimal admixture of other components.

Side effects of hemotherapy
• Risk of posttransfusion event.
• Allommunization in group systems of
erythrocytes, thrombocytes and leukocytes,
and rarely also the serum antibodies.
• Hemosiderosis after many transfusions
• Transmission of infection diseases: HBV, HCV,
CMV, AIDS, syphilis, malaria, tularemia,

Transfusion Preparation

Banked Whole Blood
• Ery, Leu, Tro in plasma
• Can be stored for 5 ww
• Rarely required
• Acute blood loss > 15% (car accident f.e.)
• ↑ of lactic acid, K+
• refrigerater

Packed Red Cells
Diluted with plasma to a hematocrit cca 50 - 75% Volume is cca 300mlStoring for 42 days – just above freezing (+2...+6oC)
a) standard / fresh or stored/
b) specially prepared from fresh blood - leucocyte-reduced• Filtered / prevention of anti-Le antibody production/
•Washed / repeated centrifugation after adding physiologicalsolution is used to remove plasma, mainly complement –ndication in hemolytic anemias/

Indications - anaemia
acute
• massive bleeding or hemorhagic shock- loss ofmore than 25% ofcirculating volume
• Whole blood or Ery
• Massive bleeding is the onlyindication for administrationof whole blood; it correctsanemia and hypovolemia.
chronic
• If symptoms of hypoxia are present
• If quick increaing of Hblevel is needed (beforesurgery)
• Correction of anemia with erythrocytes
CAVE! In chronic anemias which can by treated causally e.g. by vit. B12, folicacid, iron transfusions are not indicated!

Clinical Indications for RBC Transfusion
• Surgery - Hgb < 80g/l or Ht < 0,26
• Active, clinically significant bleeding
• Anemia with clinical symptoms
• Anemia without clinical symptoms in patientwith preexisting cardiopulmonary or cerebrovascular diseases
• Severe myelosupression - if limited evidencefor maintaining Hgb greater > 100g/l

Platelet concentrates - types
• pooled PTL (approx. from 6 donors)
• PTL from apheresis (single donor, there ispossibility to keep compatibility in HLA system)
• Leucocyte-reduced PLT concentrate
- stored in room T – only 5 days
Cave! Compatibility in AB0 and D antigen.

Clinical Indications for RBC Transfusion
Prophylactic use
• Reversible bone marrowfailure with PLT < 10G/l (not chronic!!!)
• In presence of risk factorsfor bleeding (sepsis f.e.)
• Pre-procedure – epiduralanaesthesia
• Pre- and postoperativeperiod
• In case of hypoproduction
Therapeutic use
• PLT < 50G/l with bleeding
• When massive blood loss
have occured
• AITP- only in life-threatiningbleeding
CAVE! Contraindication – TTP and HIT

Threshold for Thrombocyte transfusion

Leukocytes
• Rare indication
•
• Severe neutropenia ANC < 0,5 G/l due the
cong or aq bone marrow failure
• Severe sepsis- fungal /bacterial
unresponsible to ATB Th

PlasmaFresh frozen plasma
• Freshly donated blood
• Source of vitamin K-
dependent clotting factors
• Only source of f. V.
Indication:
Coagulopathy
Deficient clotting factors
Cryoprecipitated antihemophilicfactor
• Antihemophilic concentrate
• Rich in clotting factors
• Indication:
• Hemophilia, von Willebrand ´s disease
CAVE!
Do not use hot water for thawing of plasma (30-35oC)Do not refreeze after thawing
Compatibility in AB0 is need.
Rh(D) negative girls anf women in fertile age - Rh(D) negative plasma

Clinical Indications for Frozen PlasmaTransfusion
• Prothrombine time (Pt) prologation by more than4sec, - INR 1,4. a aPTT ba more than 10 sec, dueto combined defect of clotting factors eventuallywith the symptoms of bleeding.
• Preparation to operation
• Postoperative period
• Thrombocytic thrombocytopenic purpura
• Rapid reversal of adverse effect of coumarinedrug
• Part of substitution during exchange transfusion.

Others
• Concentrate of f. II, VII, X, IX,
• human albumin
• Fibrinogen
• Immunoglobulines
• AT III

Principles of transfusion productsadministration (1)
• Units of fresh frozen plasma should be administered within 4 hours after thawing.
• Units of irradiated RBC is necessary to administer till 28th day from the collection data .
• Into transfusion products should not be added any drugs or infusion solutions.
• Department must return unused transfusion product back to blood bank with the accompanying protocol indicating the reason of non administration, for destroying the unused transfusion

Principles of transfusion productsadministration (2)
• Each transfusion preparation accepted at department should be registered in the Transfusion Diary, even when not used (withtime of receipt written in the diary of the department).
• For administration of each unit of transfusion medicine (except of platelet transfusions from whole blood) must be used the new kit.

Principles of transfusion productsadministration (3)
• In transfusion of Erythrocytes or full blood there is necessary to keep strictly the same blood group in AB0 system and in D antigen between the donor and transfusion recipient.
• In vital indication there is possibility to transfuse the 0 Rhnegative group
• old transfusions have increased content of K+,
• in massive transfusions -citrate toxicity - =decreased Ca2+

Compatibility procedures in laboratory
• Accurate A,B,0 , Rh typing of the patient and donor
• Screening for anti-RBC antibodies in the donors´and recipients serum (ABO, Rh, Duffy, Kell...)
• Crossmatching – donors ´ RBC and recipients sera(major)

Bedside test• Patient ´s name, DOB• Patient´s informed consent• In patients with cold-antibodies transfusion should be pre-heated for 2 hours in
an incubator at 37 °C• Verify the blood type, donor number, component name• Verify the product is not outdated• Sign the Transfusion Record Form before blood transfusion is initiated, date, time• Verification of the AB0 blood group- RBC, PLT, plasma• Pre-transfusion vital sign documentation - T, BP, HR and urine chemical analysis• Biological test (3x 10-20 ml of blood fast, á 3 min) - monitor the patient
especially the first 15 minutes after beginning of transfusion;• than nurse monitors the patient throughout the treatment period,• adverse reaction - stop the transfusion immediately, securing venipuncture, alert
a doctor and provide the necessary information. • During transfusion do not prick the bag or remove air bubbles from tubing.• After the end of transfusion, nurse should desinfy the needle and transfusion bag
store in refrigerator for next 48 h. • Post-transfusion vital sign documentation - T, BP, HR and urine chemical analysis

Transfusion reactions
• Haemolytic – acute, delayed
• Allergic
• Febrile
• Bacterial Contamination
• Circulatory Overload

Haemolytic Reaction - acute
• Incompatibility in system AB0
• 1:30 -60,000; fatal 1: 600,000)
• Manifestation: dyspnoe, anxiety, unrest, feeling of chestpressure, lumbar pain, nausea, sweating, tachycardia, hypotension, shock, DIC,acute phase develops within 1 hour (free hemoglobin presentin plasma and urine, bilirubin is increased.)
• Therapy: interruption of transfusion (Secure i.v. line!),
• 20% Mannitol dose to 100 g / 24h, corticosteroids, Bicarbonate,therapy of shock, Hemodialysis in anuria
• Prevention: careful preparation and checking of transfusionunit, and Transfusion procedure,

Pyretic Reaction
• = febrile nonhemolytic- reaction - 1 in 200 ; 1 in300• Is determined by the presence of pyrogens in preparation and
/ or anti -Le antibodies (in previously alloimmunizedrecipients). It is a benign reaction without severe consequence
• FNHTR is caused by white blood cell–derived cytokines, such as IL-1, IL-6, IL-8, and TNF in RBC pack of donor ´s blood. Theirconcentration is directly related to the duration of storage of the blood products.
• Manifestations: temperature rise > 1° C, fever, chills, headache. Dg: after exclusion of another causes: bacter. contamination, acute hemolytic reaction
• Therapy: antipyretics, sedatives, steroids• Prevention: Administration of leucyte reduced preparations
(filtered, washed). Pretreatment with antipyretic drugs(acetaminophen)

Allergic Reaction
• 1:30 to 1:100, different severity.
• Manifestation: urticaria, pruritus, dizziness, angioneuroticedema, anaphylactic reaction (1: 150,000)
•Therapy antihistamines, corticosteroids
•Prevention: prophylactically administered antihistaminesbefore the transfusion

Circulatory Overload
• cardiovascular reaction
• Manifestation: hypervolemia, heart failure
• Therapy: slowing the rate of transfusion, Furosemide

Bacterial - toxic reaction
• Contaminated blood transfusion. eg G- bacteries
• Manifestation: occuring of endotoxin shock, activation of DIC
•Therapy: antibiotics, therapy of shock, treatmentof DIC
• Prevention: compliance with the measures forthe collection, storage and administration oftransfusion

Late complications
• Hemosiderosis -Iron overload (after 80-100 units)
• transmission of infection diseases

Posttransfusion reaction
• Interruption of transfusion.
• Venepunction is secured ! by isotonic salineinf.
• Patients blood sample 5-7 ml -for laboratory tests
• The transfusion pack is sent to laboratory - withaccompanying report.
• Examination: Anti -Erythrocyte antibodies, anti-leucocyte antibodies, anti-Thrombocyteantibodies, microbiological examination

Case Report

Medical History 1
• Chief Compliant: A 47-year-old woman presented to the Emergency Department complaining of fevers, back pain, and dark urine.
• Present Illness: On the day before admission – fever, chills, dark urine, minimal lower back pain. 11 days before she was hospitalised for short time because of severe anemia, fatigue and breathlessness - Hgb 70 g/L. She received 2 units of packed red blood cells and was discharged home. The gynecological surgery (hysterectomy) was planned in near future.
• She denied headache, sore throat, cough, shortness of breath, or gastrointestinal, genitourinary or dermatologic symptoms.

Medical History 2
• Past History: long-standing history of anemia and menorrhagia caused by uterine myomata. Till this timeshe refused suggested hysterectomy. Art. Hypertension
• Current Medication: Indapamid 2,5mg/d
• Allergies: 0
• Substance Abuse: 0
• Gynecol Hist: 2 children,
• Social History: married, clerk
• Family History: 0

Physical Examination
• General observation: 168cm/65kg, T 37.7oC, BP 110/64 mm Hg, HR 89/min, breathing 16 times/min, O2sat 99%, eupnoic.
• Skin well- hydrated, pale pink colour skin, no skin lesions, and no focal neurologic deficits. Her pupils were equal and reactive to light, and her sclerae were anicteric. Her oropharynx was clear, her neck was supple, and there was no lymphadenopathy or thyromegaly. The lungs were clear to auscultation. The cardiovascular examination demonstrated a normal rate and regular rhythm, a normal S1and S2, and no murmurs. abdomen was soft, nontender, nondistended, and without masses or organomegaly. There was no lower extremity edema.

Laboratory Results 1pt. results ref.values commentary
Blood CountLe (WBC) 11.1 x109 3.8 - 10 ↑Hemoglobin 90 g/l 120 - 160 ↓hematocrit 28.0% 34 - 46 ↓MCV 86 fl, 82 - 98 nTrombocytes (Plt) 89 x109 150 - 400 ↓
HemostasisThrombin Time 14.5 s < 21 s aPTT 24.5 sec, 23.4 – 35.1 INR 1.2 0.8 - 1.2
UrinalysisClour: dark, cloudy urine unusualSpecific gravity 1.025, Hemoglobin ++ negat. ↑WBC 5 - 10 per HPF < 15 nRBC 3 - 10 per HPF, < 10 nHyaline casts 3 - 5 perHPF 0 - 2 ↑
pt. results ref.values commentary
Biochemistry
Na 137 mmol/L, 132 - 146
K 3.5 mmol/L, 3.5 - 5.5
Chloride 100 mmol/L, 99 - 109
bicarbonate 24 mmol/L 22 - 26
Urea 12 mmol/l 2 - 6.7 ↑
Creatinin 125 umol/l 44 - 80 ↑
ALP 2.1ukat/l 0.58 -1.74 ↑
AST 1.6 ukat/l 0.17- 0,85 ↑
ALT 0.66 ukat/l 0.2 - 0.6 ↑
CK 1.41 ukat/l 0.4 - 2.8

Question # 1
How can be explained the hemoglobinuria with–ve RBC in urine?
1. Free hemoglobin in urine as a consequence ofhemolysis.
2. Free myoglobin in urine as a consequence ofrhabdomyolysis.

Answer
1. Free hemoglobin in urine as a consequence of hemolysis. –correct. Hemolysis may release free hemoglobin into the blood; hemoglobin is then filtered by the kidneys and excreted in the urine. Standard urinalysis detects this hemoglobin, whereas microscopic analysis does not reveal red blood cells.
2. Free myoglobin in urine as a consequence of rhabdomyolysis –wrong. The patient has no risk factors for rhabdomyolysis (such as seizures, trauma, or prolonged immobility), and the creatine kinase level is not elevated, as would be expected if rhabdomyolysis were present.

Question # 2
Which laboratory tests are most valuable to diagnose hemolysis?

Question # 2
parameter Pt ´s result Ref. range
Total bilirubin 28umol/l ↑ 0,4-17,1
LDH 19,9ukat/l↑ 1,8-3,4
Haptoglobin 0,15g/l ↓ 0,3-2,0
reticulocytes 2,4%↑ 0,5-1,5
Which laboratory tests are most valuable to diagnose hemolysis?

Diagnosis
• A delayed hemolytic transfusion reaction

Treatment and other tests
• The patient received aggressive hydration.
• Peripheral blood smear - a very few schistocytes and spherocytes.
• Testing of the patient’s blood revealed the presence of an antibody against the Jk(a) antigen that had not been detected at the time of transfusion 11 days previously.
• Additional testing for posttransfusion purpura was negative.
• She was discharged.
• Follow up 1 week later – Hgb 94 g/L, S- Cr 86 umol/l.

Delayed hemolytic transfusion reaction
• Delayed hemolytic transfusion reactions are more common but much less serious as acute hemolytic transfusion reactions.
• Febrile hemolytic transfusions result from an anamnestic antibody response to a foreign red blood cell antigen, commonly of the Rh or Kidd group, to which the recipient has been previously exposed.
• Important risk factors for development of a febrile hemolytic transfusion include prior transfusion, pregnancy, and organ transplantation.
• Febrile hemolytic transfusion reactions typically occur between 3 and 21 days after transfusion and cause mild to moderate hemolysis accompanied by fever, hemoglobinuria and an increased serum bilirubin.
• In the peripheral blood smear may be mild spherocytosis. • Diagnosis requires demonstration of a newly positive direct
antibody (Coombs) test along with evidence of hemolysis.

Diagnosis
• Haemolytic anaemia is evident.
• Spherocytosis is present as a result of red cell damage.
• Direct antiglobulin test is positive, with either IgG alone (67%), IgGand complement (20%) or complement alone (13%) being found on the surface of the red cells.
• Autoantibodies may have specificity for the Rh blood group system(e.g. for the e antigen).
• Autoimmune thrombocytopenia and/or neutropenia may also bepresent.

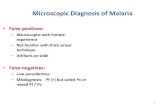
IgG anti–red cell autoantibodies. A, Structure of an IgG molecule demonstrating its variable and constant regions and the heavy and light chains. B, Agglutination of red cells by pentameric IgM antibodies, which can join the cells into a lattice. C, Coating of red cells by IgG antibodies. The antibodies are unable to agglutinate the cells. D, Agglutination of IgG-coated red cells by an anti-IgG antibody.

The direct test detects patients' cells sensitized in vivo (i.e.: in pt´s blood)-adding anti-human globulin to such erythrocytes causes visible agglutination=positiveThe indirect test: detects if the patients serum containes anti-erythrocyte antibodies: 1st step: tested Erythrocytes are added to patients serum;2nd step: adding human antiglobulin into such suspension: agglutination=positive test
adding
INDIRECT test:Testing, if antibodies against Erythrocytes are present in pt.serum
(two steps)
DIRECT test:Testing, if antibodies against Ery are already binded on them (one step)
Antiglobulin (Coombs') tests

Extravascular haemolysis is due to interaction of antibody-coated cells with cells in the reticuloendothelial system, predominantly in the spleen.
(a) Spherocytosis results from partial phagocytosis.(b) Complete phagocytosis if there is complement as well as antibody on the cell surface. (c) Cells coated with complement only are ineffectively removed and circulate with C3d
or C3b on their surface.

Acute haemolytic transfusion reaction
• In contrast to delayed hemolytic transfusion, an acute hemolytic transfusion reaction is an extremely rare but life-threateningcomplication of blood product transfusion.
• These reactions most commonly result from ABO incompatibility, generally due to transfusion of a group O recipient with non-group O red blood cells, but they may also be caused by acquired antibodies directed against Rh group or other red blood cell antigens.
• This process promotes a rapid intravascular hemolysis that may lead to disseminated intravascular coagulation (DIC), acute renal failure due to pigment-induced acute tubular necrosis, and frank shock.
• The presence of fever, chills, evidence of hemolysis or DIC, flank pain, and hemoglobinuria should all raise suspicion for an acute hemolytic transfusion reaction.

Delayed serologic transfusion reaction
• In the absence of hemolysis, a patient with a newly positive direct antibody test and antibodyscreen is considered to have manifested adelayed serologic transfusion reaction.

Thank You for Your Attention