Transdermal Opoids
6
Transdermal drug delivery: principles and opioid therapy Lyn Margetts FRCA Richard Sawyer FRCA FIPP The applic at ion of medica tio ns to the ski n to ease ailments is a practice that has been utilized by humankind ov er the mi ll enni a and has included the application of poultices, gels, oint- ments, creams, and paste s. These applica tions we re pri mari ly inte nded for a local topi ca l ef fect. The use of adhe si ve skin pa tc hes to deliv er drugs systemi cally is a rela tiv ely new phenomenon. 1 The fir st adhesi ve tr ansdermal delive ry system (TDDS) patch was approved by the Food and Drug Administration in 1979 (scopolamine pat ch for mot ion sic kne ss). Nit rog lyc eri ne patches were approved in 1981. This method of delivery became widely recognized when nico- tine patches for smokin g cessa tion were intro- duced in 1991. TDDS off er pha rma col ogi cal advant age s over the oral route and improved patient accept- abi lit y and compliance. As suc h, the y ha ve been an impor tant area of phar ma ce ut ic al res ear ch and dev elo pme nt over the las t few decades. Conditions for which TDDS are suit- able are detailed in Table 1. Skin structure The skin is the largest organ in the body; it pro- tects against the influx of toxins and the efflux of water and is largely impermeable to the pen- etration of foreign molecules. Human skin con- sists of three main layers: the epidermis, dermis, and hypodermis (Fig. 1). The epidermis, in par- ticul ar the stra tum corneum, acts as the major barrier to drug absorption. The stratum corneum contains only 20% of water and is a highly lipo- philic membrane; it is 10–20 mm thick depend- ing on its state of hydration. The thickness of the epidermis varies from 0.06 mm on eyelids to 0.8 mm on the soles of the feet. An applied drug must traverse these stru c- tural layers, encountering several lipophilic and hydrophilic domains on the way to the dermis where absorption into the systemic circulation is rapid due to the large capillary bed. Removing the str atum cor neum spee ds the diffusion of small water-soluble molecules into the systemic circulation by up to 1000 times. 2 Alternatively, hydrop hil ic compounds can rea ch the dermis via shunt pathways such as hair follicles, sweat gla nds, nerve ending s, and blood and lymph vesse ls. These routes contri bute minimally to steady-state drug flux. The dermis is the thickest layer of the skin (3–5 mm) and possesses hair follicles, sweat glands, nerve endings, and blood and lymph ve sse ls. It ac ts as the sy st emic absorption site for drugs. There are varia tions between individual s in the rate at which drugs are absorbed via the ski n due to fa ctor s such as thic kne ss of the str at um cor neu m, skin hydr ation, unde rlying skin diseases or injuries, ethnic differences, and body temperature. Pharmacokinetics of transdermal drug delivery The dr ug is stored in the TDDS either in a reservoir or impregnated into the fabric of the pa tch. On applyi ng the TDDS to the skin, a drug concen tra tion gradient is deve loped and the dr ug st ar ts to mo ve down the gr adient . A second drug res erv oir is est abl ishe d in the str at um cor neu m. As the drug moves furt her into the skin, it is absorbed into the local capil- lary vasculature and is then transported into the systemic circulation. As a result of this absorption process, there is a dela y between TDDS applicat ion and the deve lopme nt of a desired minimum effec tive concentration (MEC). This delay varies between drugs. There is an initial period in which drug concentrations are hardly measurable. The time to reac h st ead y-s ta te pla sma concentrat ion s varies considerably and may be achieved com- pletely only after two to three patch applications. Thereafter, the steady state is maintained for as lon g as a pa tch is app lie d. The advan ta ge of Key points The transdermal route for drug delivery avoids first pass metabolism and large variations in plasma drug concentrations. The stratum corneum is the greatest barrier to transdermal transport. Drugs suitable for transdermal administra tion have a low molecular weight and high lipid solubility. There are two types of patches available: reservoir and matrix systems. Opioid patches are frequently utilized in chronic malignant and non- malignant pain management. Lyn Margetts FRCA Specialist Registrar in Anaesthesia Derriford Hospital Plymouth UK Richard Sawyer FRCA FIPP Consultant in Anaesthesia and Pain Management Eric Angel Pain Clinic Level 7 Derriford Hospital Plymouth PL6 8DH UK Tel: þ44 1752 792525 Fax: þ44 1752 517556 E-mail: [email protected] est.nhs.uk (for correspondence) 171 doi:10.1093/bjaceaccp/mkm033 Continuing Education in Anaesthesia, Critical Care & Pain | Volume 7 Number 5 2007 & The Board of Management and Trustees of the British Journal of Anaesthesia [2007]. All rights reserved. For Permissions, please email: [email protected] b y g u e s t o n A p r i l 6 , 2 0 1 2 h t t p : / / c e a c c p . o x f o r d j o u r a l s . o r g / D o w n l o a d e d f r o m
-
Upload
sau-yee-chow -
Category
Documents
-
view
218 -
download
0
Transcript of Transdermal Opoids

7/31/2019 Transdermal Opoids
http://slidepdf.com/reader/full/transdermal-opoids 1/6
Transdermal drug delivery:principles and opioid therapy
Lyn Margetts FRCA
Richard Sawyer FRCA FIPP
The application of medications to the skin to
ease ailments is a practice that has been utilized
by humankind over the millennia and has
included the application of poultices, gels, oint-
ments, creams, and pastes. These applications
were primarily intended for a local topical
effect. The use of adhesive skin patches to
deliver drugs systemically is a relatively new
phenomenon.1
The first adhesive transdermal delivery
system (TDDS) patch was approved by the Food
and Drug Administration in 1979 (scopolamine
patch for motion sickness). Nitroglycerine
patches were approved in 1981. This method of
delivery became widely recognized when nico-
tine patches for smoking cessation were intro-
duced in 1991.
TDDS offer pharmacological advantages
over the oral route and improved patient accept-
ability and compliance. As such, they have
been an important area of pharmaceutical
research and development over the last few
decades. Conditions for which TDDS are suit-
able are detailed in Table 1.
Skin structure
The skin is the largest organ in the body; it pro-
tects against the influx of toxins and the efflux
of water and is largely impermeable to the pen-
etration of foreign molecules. Human skin con-
sists of three main layers: the epidermis, dermis,
and hypodermis (Fig. 1). The epidermis, in par-
ticular the stratum corneum, acts as the major
barrier to drug absorption. The stratum corneum
contains only 20% of water and is a highly lipo-
philic membrane; it is 10–20 mm thick depend-
ing on its state of hydration. The thickness of
the epidermis varies from 0.06 mm on eyelids to
0.8 mm on the soles of the feet.
An applied drug must traverse these struc-
tural layers, encountering several lipophilic and
hydrophilic domains on the way to the dermis
where absorption into the systemic circulation is
rapid due to the large capillary bed. Removing
the stratum corneum speeds the diffusion of
small water-soluble molecules into the systemic
circulation by up to 1000 times.2
Alternatively,
hydrophilic compounds can reach the dermis
via shunt pathways such as hair follicles, sweat
glands, nerve endings, and blood and lymph
vessels. These routes contribute minimally to
steady-state drug flux. The dermis is the thickest
layer of the skin (3–5 mm) and possesses hair
follicles, sweat glands, nerve endings, and blood
and lymph vessels. It acts as the systemic
absorption site for drugs.
There are variations between individuals in
the rate at which drugs are absorbed via the
skin due to factors such as thickness of the
stratum corneum, skin hydration, underlying
skin diseases or injuries, ethnic differences, and
body temperature.
Pharmacokinetics of transdermal drug delivery
The drug is stored in the TDDS either in a
reservoir or impregnated into the fabric of the
patch. On applying the TDDS to the skin, a
drug concentration gradient is developed and
the drug starts to move down the gradient.
A second drug reservoir is established in the
stratum corneum. As the drug moves further
into the skin, it is absorbed into the local capil-
lary vasculature and is then transported into the
systemic circulation.
As a result of this absorption process, there
is a delay between TDDS application and the
development of a desired minimum effective
concentration (MEC). This delay varies between
drugs. There is an initial period in which drug
concentrations are hardly measurable. The time
to reach steady-state plasma concentrations
varies considerably and may be achieved com-
pletely only after two to three patch applications.
Thereafter, the steady state is maintained for as
long as a patch is applied. The advantage of
Key points
The transdermal route fordrug delivery avoids firstpass metabolism and largevariations in plasma drugconcentrations.
The stratum corneum is the
greatest barrier totransdermal transport.
Drugs suitable fortransdermal administrationhave a low molecular weightand high lipid solubility.
There are two types of patches available: reservoirand matrix systems.
Opioid patches arefrequently utilized inchronic malignant and non-malignant pain management.
Lyn Margetts FRCA
Specialist Registrar in AnaesthesiaDerriford Hospital
PlymouthUK
Richard Sawyer FRCA FIPP
Consultant in Anaesthesia andPain Management
Eric Angel Pain ClinicLevel 7
Derriford HospitalPlymouth PL6 8DH
UK Tel: þ44 1752 792525Fax: þ44 1752 517556
E-mail: [email protected] (for correspondence)
171doi:10.1093/bjaceaccp/mkm033Continuing Education in Anaesthesia, Critical Care & Pain | Volume 7 Number 5 2007
& The Board of Management and Trustees of the British Journal of Anaesthesia [2007].All rights reserved. For Permissions, please email: [email protected]

7/31/2019 Transdermal Opoids
http://slidepdf.com/reader/full/transdermal-opoids 2/6
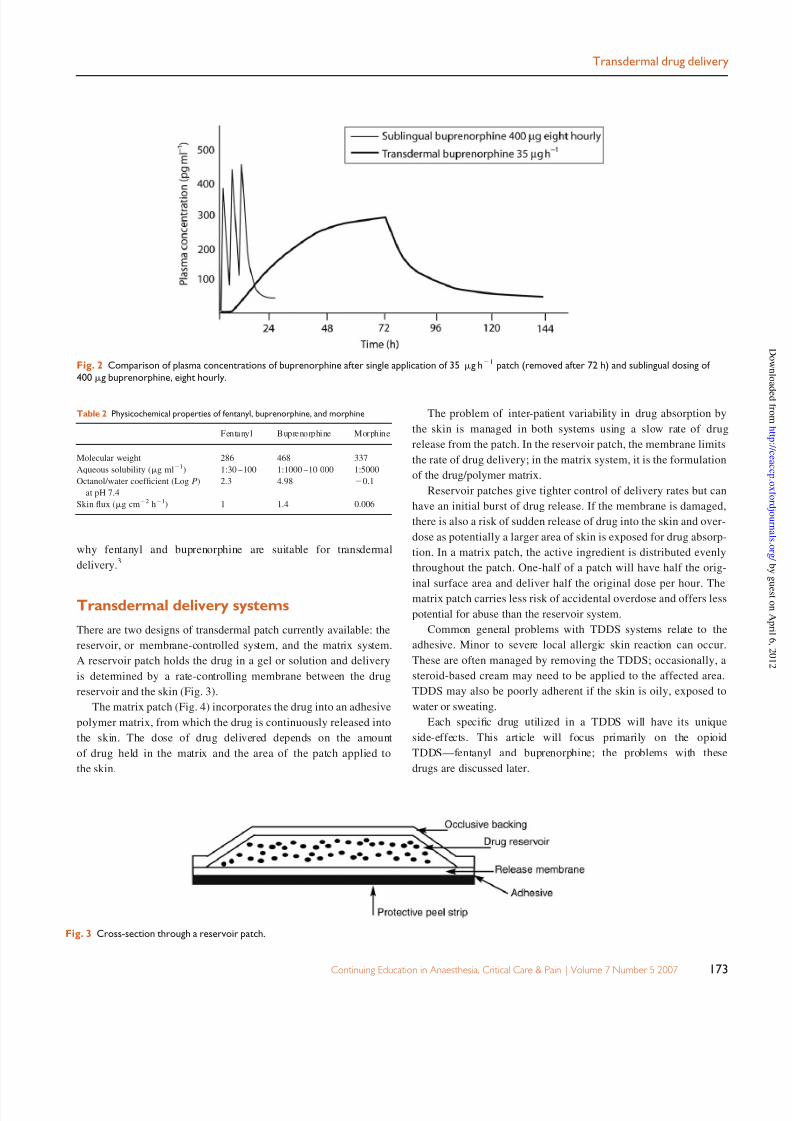
TDDS is that continuous drug delivery is provided with better
patient compliance. Figure 2 shows the difference in plasma con-
centrations of buprenorphine achieved with regular sublingual
dosing and with TDDS application.
After removal of TDDS patches, drug concentrations decrease
gradually. The rate of decline depends on the drug’s context sensi-
tive half-time and whether a reservoir has been formed in the skin.
Effect of drug characteristics
The properties of a drug that enable good penetration through the
stratum corneum can be deduced from the equation for steady-state
flux.2 When the cumulative mass of a diffusant, m, passing per
unit area through a membrane is plotted, after time t , the graph
approaches linearity and the slope yields the steady flux dm /dt ,
dm
dt ¼ DC oK
h
where D is the diffusion coefficient, C o the constant concentration
of drug in donor solution, K the partition coefficient of solute
between membrane and bathing solution, and h the thickness of
the membrane.
Therefore, for a drug to penetrate well, it should have low mole-
cular mass (high D), adequate solubility in oil (high C o), and a
moderately high partition coefficient. All of the drugs currently
available in patch formulation share three features that enable
administration through a convenient area of skin: molecular mass
,500 Da; high lipophilicity; and low required daily dose
(,2 mg). The comparison of the physicochemical properties of
fentanyl, buprenorphine, and morphine (Table 2) demonstrates
Fig. 1 Cross-section through the skin.
Table 1 Transdermal patches licensed in the UK and conditions for which they are
indicated
Active ingredient Indication
Buprenorphine Analgesia
Clonidine Hypertension
Oestradiol Hormone replacement
Oestradiol and progesterone Hormone replacement
Ethinyloestradiol, Norelgestromin Contraception
Fentanyl Analgesia
Glyceryl trinitrate Angina
Hyoscine Motion sickness
Lisuride Parkinson’s disease/restless legs syndrome
Nicotine Smoking cessation
Testosterone Hypogonadism
Transdermal drug delivery
172 Continuing Education in Anaesthesia, Critical Care & Pain j Volume 7 Number 5 2007
7/31/2019 Transdermal Opoids
http://slidepdf.com/reader/full/transdermal-opoids 3/6
why fentanyl and buprenorphine are suitable for transdermal
delivery.3
Transdermal delivery systems
There are two designs of transdermal patch currently available: the
reservoir, or membrane-controlled system, and the matrix system.
A reservoir patch holds the drug in a gel or solution and delivery
is determined by a rate-controlling membrane between the drug
reservoir and the skin (Fig. 3).
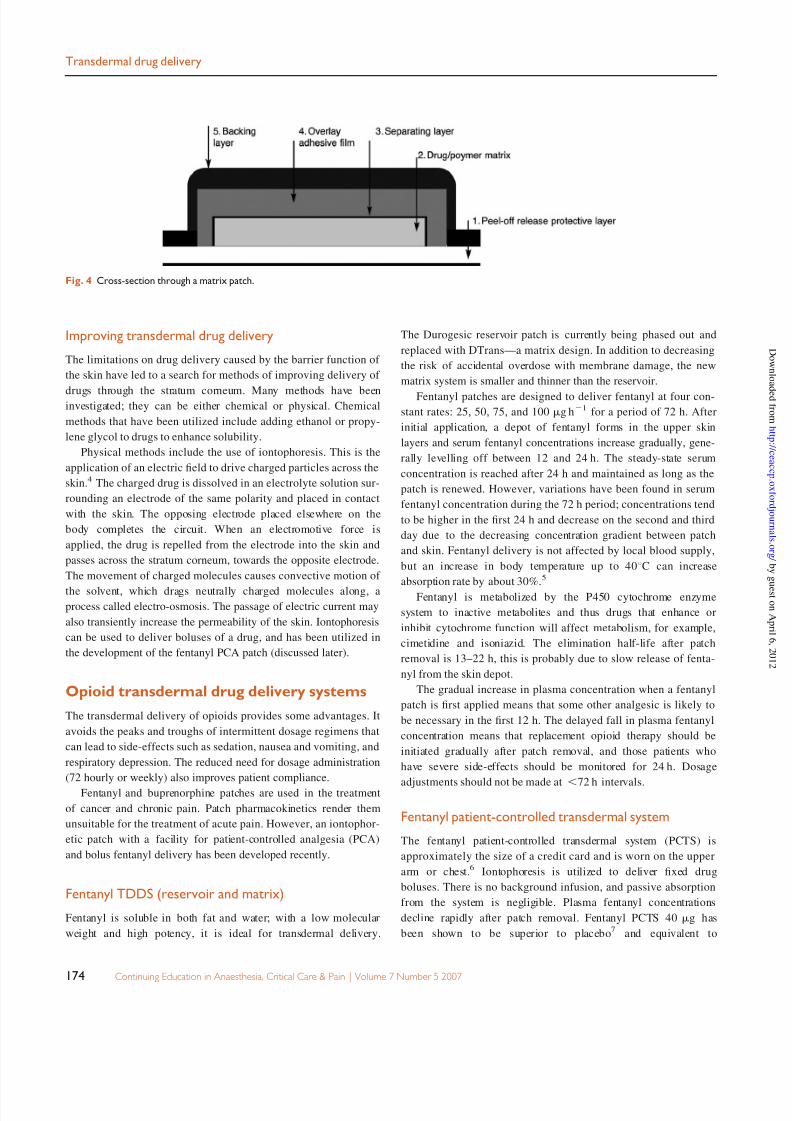
The matrix patch (Fig. 4) incorporates the drug into an adhesive
polymer matrix, from which the drug is continuously released into
the skin. The dose of drug delivered depends on the amount
of drug held in the matrix and the area of the patch applied to
the skin.
The problem of inter-patient variability in drug absorption by
the skin is managed in both systems using a slow rate of drug
release from the patch. In the reservoir patch, the membrane limits
the rate of drug delivery; in the matrix system, it is the formulation
of the drug/polymer matrix.
Reservoir patches give tighter control of delivery rates but can
have an initial burst of drug release. If the membrane is damaged,
there is also a risk of sudden release of drug into the skin and over-
dose as potentially a larger area of skin is exposed for drug absorp-
tion. In a matrix patch, the active ingredient is distributed evenly
throughout the patch. One-half of a patch will have half the orig-
inal surface area and deliver half the original dose per hour. The
matrix patch carries less risk of accidental overdose and offers less
potential for abuse than the reservoir system.
Common general problems with TDDS systems relate to the
adhesive. Minor to severe local allergic skin reaction can occur.
These are often managed by removing the TDDS; occasionally, a
steroid-based cream may need to be applied to the affected area.
TDDS may also be poorly adherent if the skin is oily, exposed to
water or sweating.
Each specific drug utilized in a TDDS will have its unique
side-effects. This article will focus primarily on the opioid
TDDS—fentanyl and buprenorphine; the problems with these
drugs are discussed later.
Fig. 3 Cross-section through a reservoir patch.
Fig. 2 Comparison of plasma concentrations of buprenorphine after single application of 35 mg h21 patch (removed after 72 h) and sublingual dosing of
400 mg buprenorphine, eight hourly.
Table 2 Physicochemical properties of fentanyl, buprenorphine, and morphine
Fentanyl Buprenorphine Morphine
Molecular weight 286 468 337
Aqueous solubility (mg ml21
) 1:30 –100 1:1000 –10 000 1:5000
Octanol/water coefficient (Log P)
at pH 7.4
2.3 4.98 20.1
Skin flux (mg cm22 h21) 1 1.4 0.006
Transdermal drug delivery
Continuing Education in Anaesthesia, Critical Care & Pain j Volume 7 Number 5 2007 173
7/31/2019 Transdermal Opoids
http://slidepdf.com/reader/full/transdermal-opoids 4/6
Improving transdermal drug delivery
The limitations on drug delivery caused by the barrier function of
the skin have led to a search for methods of improving delivery of
drugs through the stratum corneum. Many methods have beeninvestigated; they can be either chemical or physical. Chemical
methods that have been utilized include adding ethanol or propy-
lene glycol to drugs to enhance solubility.
Physical methods include the use of iontophoresis. This is the
application of an electric field to drive charged particles across the
skin.4 The charged drug is dissolved in an electrolyte solution sur-
rounding an electrode of the same polarity and placed in contact
with the skin. The opposing electrode placed elsewhere on the
body completes the circuit. When an electromotive force is
applied, the drug is repelled from the electrode into the skin and
passes across the stratum corneum, towards the opposite electrode.
The movement of charged molecules causes convective motion of
the solvent, which drags neutrally charged molecules along, aprocess called electro-osmosis. The passage of electric current may
also transiently increase the permeability of the skin. Iontophoresis
can be used to deliver boluses of a drug, and has been utilized in
the development of the fentanyl PCA patch (discussed later).
Opioid transdermal drug delivery systems
The transdermal delivery of opioids provides some advantages. It
avoids the peaks and troughs of intermittent dosage regimens that
can lead to side-effects such as sedation, nausea and vomiting, and
respiratory depression. The reduced need for dosage administration
(72 hourly or weekly) also improves patient compliance.
Fentanyl and buprenorphine patches are used in the treatment
of cancer and chronic pain. Patch pharmacokinetics render them
unsuitable for the treatment of acute pain. However, an iontophor-
etic patch with a facility for patient-controlled analgesia (PCA)
and bolus fentanyl delivery has been developed recently.
Fentanyl TDDS (reservoir and matrix)
Fentanyl is soluble in both fat and water; with a low molecular
weight and high potency, it is ideal for transdermal delivery.
The Durogesic reservoir patch is currently being phased out and
replaced with DTrans—a matrix design. In addition to decreasing
the risk of accidental overdose with membrane damage, the new
matrix system is smaller and thinner than the reservoir.
Fentanyl patches are designed to deliver fentanyl at four con-
stant rates: 25, 50, 75, and 100 mg h21 for a period of 72 h. After
initial application, a depot of fentanyl forms in the upper skin
layers and serum fentanyl concentrations increase gradually, gene-
rally levelling off between 12 and 24 h. The steady-state serum
concentration is reached after 24 h and maintained as long as the
patch is renewed. However, variations have been found in serum
fentanyl concentration during the 72 h period; concentrations tend
to be higher in the first 24 h and decrease on the second and third
day due to the decreasing concentration gradient between patch
and skin. Fentanyl delivery is not affected by local blood supply,
but an increase in body temperature up to 408C can increase
absorption rate by about 30%.5
Fentanyl is metabolized by the P450 cytochrome enzyme
system to inactive metabolites and thus drugs that enhance or
inhibit cytochrome function will affect metabolism, for example,
cimetidine and isoniazid. The elimination half-life after patch
removal is 13–22 h, this is probably due to slow release of fenta-
nyl from the skin depot.
The gradual increase in plasma concentration when a fentanyl
patch is first applied means that some other analgesic is likely to
be necessary in the first 12 h. The delayed fall in plasma fentanyl
concentration means that replacement opioid therapy should be
initiated gradually after patch removal, and those patients who
have severe side-effects should be monitored for 24 h. Dosage
adjustments should not be made at,
72 h intervals.
Fentanyl patient-controlled transdermal system
The fentanyl patient-controlled transdermal system (PCTS) is
approximately the size of a credit card and is worn on the upper
arm or chest.6
Iontophoresis is utilized to deliver fixed drug
boluses. There is no background infusion, and passive absorption
from the system is negligible. Plasma fentanyl concentrations
decline rapidly after patch removal. Fentanyl PCTS 40 mg has
been shown to be superior to placebo7
and equivalent to
Fig. 4 Cross-section through a matrix patch.
Transdermal drug delivery
174 Continuing Education in Anaesthesia, Critical Care & Pain j Volume 7 Number 5 2007

7/31/2019 Transdermal Opoids
http://slidepdf.com/reader/full/transdermal-opoids 5/6
i.v. morphine PCA for the treatment of acute postoperative pain.8
The fentanyl PCTS has the advantage of being less cumbersome
than i.v. systems but a potential disadvantage is the pre-
programmed fixed dose; although this eliminates the possibility of
programming errors, it means that the device will be unsuitable forthose patients with higher opioid requirements.
Buprenorphine TDDS (matrix)
Buprenorphine is a partial agonist at m-receptors; it is 60 times
more potent than morphine. A ceiling effect is reached at doses of
.16 mg day21. This does not happen in clinical practice as the
patches are designed to deliver 35, 52.5, or 70 mg h21
and the
maximum dose is 3.36 mg day21 (two 70 mg h
21 patches).
Effective plasma concentrations are reached within 12–24 h of
patch application. As with fentanyl, metabolism is by the CYP
3A4 system, but offset after patch removal is slower due to the
high affinity of buprenorphine for opioid receptors. Patients withsevere side-effects should be observed for 30 h after removal of
the patch. A recent development is the release of a 7 day buprenor-
phine patch. This buprenorphine patch is a matrix system, available
in three sizes, delivering 5, 10, or 20mg h21 of buprenor-
phine over 7 days, and licensed for the treatment of moderate to
severe pain.
Clinical efficacy of opioid TDDS
Opioid TDDS have proven to be efficacious in the long-term man-
agement of chronic malignant and non-malignant pain.9,10
Transdermal opioids have found applications in managing patients
suffering with chronic low back pain and chronic musculoskeletal
disorders. In both groups, patient satisfaction is greater with prefer-
ence for transdermal drug delivery as this is associated with less
side-effects (e.g. constipation) and is more convenient. Improve-
ments in measures of quality of life have also been reported in
cancer pain patients receiving opioid TDDS.
Transdermal patches are open to abuse, sometimes with fatal
consequences. There are reports of fentanyl being extracted from
patches for i.v. injection. This was a particular problem with the
reservoir patch. Respiratory depression and cognitive dysfunction
are important side-effects of opioid patches. Patients should be
clearly educated about the potential adverse effects and cautioned
against using alcohol or other sedative medication concurrently
with opioid patches. Because of the unique pharmacokinetics of
the TDDS systems, the depressive effects are not immediately
reversed by patch removal; in emergency situations, i.v. naloxone
may be required to reverse this sedative effect. Patients and carers
must be clearly educated about this. Cognitive dysfunction can
present with a wide range of neuropsychological side-effects,
including mental dullness, euphoria, and reduced attention, con-
centration, and memory. Ability to drive motor vehicles has been
investigated; there was no significant difference in performance
measures between patients with fentanyl patches and controls.
However, it is probably wise to advise patients to abstain from
driving if their opioid dose is being changed or if they are experi-
encing any neuropsychological side-effects.
Unintended exposure is also a real but rare complication.
Children can be exposed to the drug by patches being inadvertentlytransferred onto the child after hugging an adult with a patch on. It
is very important to avoid children coming into contact with
opioid patches; fatal consequences have been reported.
Perioperative pain management of patientsusing opioid patches
There is little evidence-base to guide the most appropriate manage-
ment of acute pain in patients on long-term opioid medication. As
a general principle, the patient’s usual pre-admission regimen
should be maintained where possible and additional analgesia
given to cover the acute painful stimulus. The following are
general guidelines.
† Involve the hospital acute pain team early.
† Cover the patient’s baseline opioid requirement, the options
are to leave the TDDS on or to change to an equivalent
opioid dose via i.v. infusion. Where possible, continue the
usual TDDS regimen to cover the chronic pain element.
† Remember to use multi-modal analgesia; regional blocks,
NSAIDs, acetaminophen.
† If using strong opioids for postoperative analgesia, higher
than usual bolus doses will be needed.
† Cessation or reduction of the patient’s usual opioid dose will
lead to withdrawal symptoms.
† The opioid dose given via TDDS must never be adjusted inan attempt to control the acute pain.
† Ensure that everyone involved in the care of the patient is
aware of the TDDS and the strategy for pain management.
References
1. Prausnitz MR, Mitragotri S, Langer R. Current status and future potentialof transdermal drug delivery. Nat Rev 2004; 3: 115–24
2. Barry BW. Novel mechanisms and devices to enable successful transder-
mal drug delivery. Eur J Pharm Sci 2001; 14: 101–14
3. Lehmann KA, Zech D. Transdermal fentanyl: clinical pharmacology. J Pain
Symptom Manage 1992; 7: S8–164. Wang Y, Thakur R, Fan Q, Michniak B. Transdermal iontophoresis: com-
bination strategies to improve transdermal iontophoretic drug delivery.
Eur J Pharm Biopharm 2005; 60: 179–91
5. Muijsers RBR, Wagstaff AJ. Transdermal fentanyl. An updated review of
its pharmacological properties and therapeutic efficacy in chronic cancer
pain control. Drugs 2001; 61: 2289–307
6. Sinatra R. The fentanyl HCl patient-controlled transdermal system: an
emerging option for the management of acute postoperative pain. Clin
Pharmacokinet 2005; 44: 1–32
7. Chelly JE, Grass J, Houseman TW, Minkowitz H, Pue A. The safety and
efficacy of a fentanyl patient-controlled transdermal system for acute
Transdermal drug delivery
Continuing Education in Anaesthesia, Critical Care & Pain j Volume 7 Number 5 2007 175

7/31/2019 Transdermal Opoids
http://slidepdf.com/reader/full/transdermal-opoids 6/6
postoperative analgesia: a multicenter, placebo-controlled trial. Anesth
Analg 2004; 98: 427–33
8. Viscuzi ER, Reynolds L, Chung F, Atkinson LE, Khanna S.Patient-controlled transdermal fentanyl hydrochloride vs. intravenous
morphine pump for postoperative pain. JAMA 2004; 291: 1333–41
9. Donner B, Zenz M, Strumpf M, Raber M. Long-term management of cancer
pain with transdermal fentanyl. J Pain Symptom Manage 1998; 15: 168–75
10. Milligan K, Lanteri-Minet M, Borchert K et al. Evaluation of long termefficacy and safety of transdermal fentanyl in the treatment of chronic
noncancer pain. J Pain 2001; 2: 197–204
Transdermal drug delivery
176 Continuing Education in Anaesthesia, Critical Care & Pain j Volume 7 Number 5 2007