Transaxillary Thyroidectomies: A Comparative Learning ... · Transaxillary Thyroidectomies: A...
7
Original Research—Endocrine Surgery Transaxillary Thyroidectomies: A Comparative Learning Experience of Robotic vs Endoscopic Thyroidectomies Otolaryngology– Head and Neck Surgery 2015, Vol. 152(5) 820–826 Ó American Academy of Otolaryngology—Head and Neck Surgery Foundation 2015 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/0194599815573003 http://otojournal.org Kimberley Liqin Kiong, MRCS, MMED 1 , N. Gopalakrishna Iyer, FRCSEd, PhD 2 , Thakshayeni Skanthakumar 2 , Jeremy Chung Fai Ng, FRCSEd 3 , Ngian Chye Tan, FRCSEd 2 ,Hin Ngan Tay, MMED, FAMS 3 *, and Hiang Khoon Tan, FRCSEd, PhD 2 * No sponsorships or competing interests have been disclosed for this article. Abstract Objective. Robotic and endoscopic approaches have become more accepted in thyroid surgery, with current literature documenting the experience of high-volume centers. We adopted both approaches concurrently, and this series pre- sents our initial experience to assess the more practical option for low- to moderate-volume centers starting out with transaxillary thyroidectomies. Study Design. Case series with chart review. Setting. Tertiary academic center. Subjects and Methods. Over a period of 4 years, 101 patients underwent transaxillary thyroidectomies, of whom 48 under- went robotic thyroidectomy and 53 underwent endoscopic thyroidectomy. Data analysis includes patient characteristics, procedure time, thyroid pathology, and postoperative compli- cations. A survey was conducted among surgeons to assess the subjective experience. Results. Endoscopic hemithyroidectomies had a significantly shorter duration of operation (145.8 minutes) vs that of robotic hemithyroidectomies (193.6 minutes), P \.001. The mean time taken for the first 5 hemithyroidectomies vs the last 5 hemithyroidectomies showed a greater drop in the endoscopic group (49.1%) vs the robotic group (18.6%). There were 2 cases of transient recurrent laryngeal nerve injury. In the surgeon survey, the endoscopic technique was perceived to have less need for peripheral support, while the robotic technique was preferred for its shorter learning curve. Conclusion. In terms of outcome, both techniques are compara- ble at least in the initial phase. Based on our early experience, the endoscopic technique may be less intuitive with a longer learning curve, although at steady state, it may be the quicker procedure. This is relevant for low- to moderate-volume cen- ters starting their transaxillary thyroidectomy program. Keywords robotic thyroidectomy, endoscopic thyroidectomy, thyroid surgery Received November 12, 2014; revised December 30, 2014; accepted January 26, 2015. S ince the first endoscopic thyroid lobectomy was per- formed in 1997, 1 many different approaches have been proposed, convergent on the goals of reduced visible scars, while balancing improved surgical outcome with ease of use. 2 Initial experience has highlighted technical issues resulting from inflexible instruments, difficult visualization, and 2-dimensional images. The da Vinci S surgical robotic system (Intuitive Surgical, Sunnyvale, California) is a devel- opment that addresses some of these technical concerns. Highlights of this system include the stereoscopic view, with robot arms that mimic the dexterity of human hands. Multiple studies have been performed to compare the endo- scopic techniques with open thyroidectomies 3-5 and robotic with open thyroidectomies. 6-9 The common thread is that transaxillary techniques are at least as good as open thyroidec- tomies. Several recent reports have focused on comparing robotic with endoscopic thyroidectomies. 10-14 Of note, these studies have been performed in high-volume centers with inherent biases toward one technique or another. Furthermore, all these centers had significant experience in endoscopic thyr- oidectomy before they commenced their robotic thyroidectomy 1 SingHealth, Singapore 2 National Cancer Centre Singapore, SingHealth, Singapore 3 Singapore General Hospital, SingHealth, Singapore * These authors contributed equally to this article. Corresponding Author: Hiang Khoon Tan, FRCSEd, PhD, SingHealth/Duke-NUS Head and Neck Centre, Academia, Level 5, Singapore General Hospital, 20 College Rd, Singapore 169856, Singapore. Email: [email protected] at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015 oto.sagepub.com Downloaded from
Transcript of Transaxillary Thyroidectomies: A Comparative Learning ... · Transaxillary Thyroidectomies: A...

Original Research—Endocrine Surgery
Transaxillary Thyroidectomies: AComparative Learning Experience ofRobotic vs Endoscopic Thyroidectomies
Otolaryngology–Head and Neck Surgery2015, Vol. 152(5) 820–826� American Academy ofOtolaryngology—Head and NeckSurgery Foundation 2015Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/0194599815573003http://otojournal.org
Kimberley Liqin Kiong, MRCS, MMED1,N. Gopalakrishna Iyer, FRCSEd, PhD2,Thakshayeni Skanthakumar2, Jeremy Chung Fai Ng, FRCSEd3,Ngian Chye Tan, FRCSEd2, Hin Ngan Tay, MMED, FAMS3*, andHiang Khoon Tan, FRCSEd, PhD2*
No sponsorships or competing interests have been disclosed for this article.
Abstract
Objective. Robotic and endoscopic approaches have becomemore accepted in thyroid surgery, with current literaturedocumenting the experience of high-volume centers. Weadopted both approaches concurrently, and this series pre-sents our initial experience to assess the more practicaloption for low- to moderate-volume centers starting outwith transaxillary thyroidectomies.
Study Design. Case series with chart review.
Setting. Tertiary academic center.
Subjects and Methods. Over a period of 4 years, 101 patientsunderwent transaxillary thyroidectomies, of whom 48 under-went robotic thyroidectomy and 53 underwent endoscopicthyroidectomy. Data analysis includes patient characteristics,procedure time, thyroid pathology, and postoperative compli-cations. A survey was conducted among surgeons to assessthe subjective experience.
Results. Endoscopic hemithyroidectomies had a significantlyshorter duration of operation (145.8 minutes) vs that ofrobotic hemithyroidectomies (193.6 minutes), P \ .001. Themean time taken for the first 5 hemithyroidectomies vs thelast 5 hemithyroidectomies showed a greater drop in theendoscopic group (49.1%) vs the robotic group (18.6%).There were 2 cases of transient recurrent laryngeal nerveinjury. In the surgeon survey, the endoscopic technique wasperceived to have less need for peripheral support, whilethe robotic technique was preferred for its shorter learningcurve.
Conclusion. In terms of outcome, both techniques are compara-ble at least in the initial phase. Based on our early experience,the endoscopic technique may be less intuitive with a longerlearning curve, although at steady state, it may be the quickerprocedure. This is relevant for low- to moderate-volume cen-ters starting their transaxillary thyroidectomy program.
Keywords
robotic thyroidectomy, endoscopic thyroidectomy, thyroidsurgery
Received November 12, 2014; revised December 30, 2014; accepted
January 26, 2015.
Since the first endoscopic thyroid lobectomy was per-
formed in 1997,1 many different approaches have been
proposed, convergent on the goals of reduced visible
scars, while balancing improved surgical outcome with ease
of use.2 Initial experience has highlighted technical issues
resulting from inflexible instruments, difficult visualization,
and 2-dimensional images. The da Vinci S surgical robotic
system (Intuitive Surgical, Sunnyvale, California) is a devel-
opment that addresses some of these technical concerns.
Highlights of this system include the stereoscopic view, with
robot arms that mimic the dexterity of human hands.
Multiple studies have been performed to compare the endo-
scopic techniques with open thyroidectomies3-5 and robotic
with open thyroidectomies.6-9 The common thread is that
transaxillary techniques are at least as good as open thyroidec-
tomies. Several recent reports have focused on comparing
robotic with endoscopic thyroidectomies.10-14 Of note, these
studies have been performed in high-volume centers with
inherent biases toward one technique or another. Furthermore,
all these centers had significant experience in endoscopic thyr-
oidectomy before they commenced their robotic thyroidectomy
1SingHealth, Singapore2National Cancer Centre Singapore, SingHealth, Singapore3Singapore General Hospital, SingHealth, Singapore*These authors contributed equally to this article.
Corresponding Author:
Hiang Khoon Tan, FRCSEd, PhD, SingHealth/Duke-NUS Head and Neck
Centre, Academia, Level 5, Singapore General Hospital, 20 College Rd,
Singapore 169856, Singapore.
Email: [email protected]
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from

program. At our center, we started our transaxillary robotic
and endoscopic thyroidectomy program at the same time and
collected data prospectively during the initial phase of the pro-
cess. The objective of this study is to present our comparative
experience and the learning process for these 2 techniques.
Our center has a relatively low volume of cases that are eligi-
ble for and interested in transaxillary thyroidectomies. As
such, our learning process and results have shown some differ-
ences from the available literature. We believe our experience
can be valuable and realistic for low- to moderate-volume cen-
ters that are looking to embark on either or both of these tech-
niques without any prior experience.
Patients and Methods
All patients undergoing either robotic (n = 48) or endoscopic
(n = 53) approach thyroidectomy from February 2010 through
August 2014 were included in this study. These represent our
first 101 cases at our institutions. Clinicopathologic, procedure-
related, and outcome data were prospectively recorded. The
study was approved by the SingHealth Centralized Institutional
Review Board (CIRB).
Routine preoperative assessment included a physical exami-
nation, ultrasound scan, and fine-needle aspiration cytology
(FNAC). Inclusion criteria for either of the transaxillary options
were benign nodule up to 5 cm and differentiated thyroid
cancer (DTC) up to 2 cm. Exclusion criteria were previous neck
surgery, evidence of severe thyroiditis, definite extrathyroidal
invasion, and lateral lymph node metastases. These criteria are
similar to those set by Kang et al9 and Lee et al.11 All patients
who satisfied the inclusion/exclusion criteria were then offered
and counseled on the open, transaxillary endoscopic or transaxil-
lary robotic approaches and allowed to choose freely with the
knowledge that the robotic option would cost SGD$7000 more
than either the open or endoscopic approach.
All operations were performed by 5 specialized head and
neck surgeons at the National Cancer Centre Singapore and
Singapore General Hospital. Thyroidectomy extent and man-
agement was based on the American Thyroid Association
(ATA) guidelines.15
Postoperatively, all patients had at least a 6-month follow-up
period. Drain volumes were measured daily until the drains
were removed, when the output decreased to less than 30 mL
over 24 hours. Complications of hematoma, seroma, chyle leak,
and tracheal injury were assessed, while routine calcium and
parathyroid hormone (PTH) levels were measured in patients
undergoing total thyroidectomy. Hypocalcemia was defined as a
corrected serum calcium level \2.1 mmol/L, requiring calcium
replacement, and permanence was defined as replacement
requirements persisting beyond 6 months. Abnormal intact PTH
(iPTH) levels were taken to be \0.9 pmol/L. Any postoperative
hoarseness was assessed by flexible fiber-optic laryngoscopy to
check vocal cord mobility with subsequent follow-up. Transient
recurrent laryngeal nerve (RLN) injury was defined as paresis
lasting less than 6 months.
To assess the subjective experience with each technique,
each surgeon independently completed a 5-question survey.
A sample of the survey is shown in Figure 1. These
questions aim to compare various aspects of the surgical
technique that may lead a surgeon to prefer one technique
over the other.
Operative Methods
Endoscopic thyroidectomy. This technique was done using a
unilateral axillo-breast approach with gas insufflation.
Patients were placed with one arm in full extension and the
neck in slight extension. One incision was made at the apex
of the axilla and another at the ipsilateral areolar junction
for the insertion of 5-mm instrument ports. A further inci-
sion was made midway between these 2 points at the ante-
rior axillary line for the insertion of a 12-mm camera port.
Subsequently, carbon dioxide gas was insufflated to a pres-
sure of 10 to 12 mm Hg to create a working space. Using
suction or a Maryland dissector and L hook instrument, a
flap was created over the pectoralis major muscle and clavi-
cle up to the thyroid notch. Dissection was carried out along
the medial border of the sternocleidomastoid muscle (SCM)
until the superior belly of the omohyoid. This was then dis-
sected to allow upward and lateral retraction. The ster-
nothyroid muscles were split longitudinally to expose the
thyroid lobe. The superior pole was then taken down with
the Harmonic (Johnson & Johnson Medical, Cincinnati,
Ohio) shears. Further capsular dissection was carried out
from the lateral approach with the Harmonic shears. The
RLN and parathyroid glands were identified and preserved.
For a total thyroidectomy, the procedure was repeated on
the contralateral side with similar incisions and approaches
as mentioned above. The specimen was then placed in an
Endopouch (Ethicon, Somerville, New Jersey) and retrieved
via the 12-mm camera port, which was lengthened to a 20-
to 25-mm incision for ease of retrieval when necessary.
Robotic thyroidectomy. Robotic thyroidectomy was carried out
using either gas insufflation or the previously described
Chung’s (gasless) technique.13 In the approach with gas
insufflation, the initial incisions were similar to the endo-
scopic approach. The working space was created with the
endoscopic equipment as described earlier, until the point
where the inner strap muscles were divided longitudinally.
The endoscopic equipment was then removed and an addi-
tional 5-mm incision made in the axilla below the earlier 2
axillary incisions. The robot was then docked with the
camera in the 12-mm port and the Prograsp forceps
(Intuitive Surgical) in the areolar port. Depending on the
Figure 1. Survey on surgeons’ subjective experience.
Kiong et al 821
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from

side of the lesion, the Maryland forceps and Harmonic
shears were docked on either side of the camera, with the
Harmonic shears operated by the surgeon’s dominant hand.
This is shown in Figure 2, comparing the placement of
incisions and instruments in 2 approaches. The thyroidect-
omy was then performed, again from the lateral approach.
Statistical Analysis
All statistical analysis was performed using SPSS v20.0
software package (SPSS, Inc, an IBM Company, Chicago,
Illinois). Data are expressed as means 6 standard deviation,
proportions, or frequencies. Groups were compared using
the Student t test and the x2 test as appropriate. P values of
\.05 were taken to be statistically significant.
Results
Over the period of the study, there were a total of 1751
thyroidectomies performed at our center, of which 1650
were open thyroidectomies and 101 were conducted with
the transaxillary approach (48 robotic and 53 endoscopic).
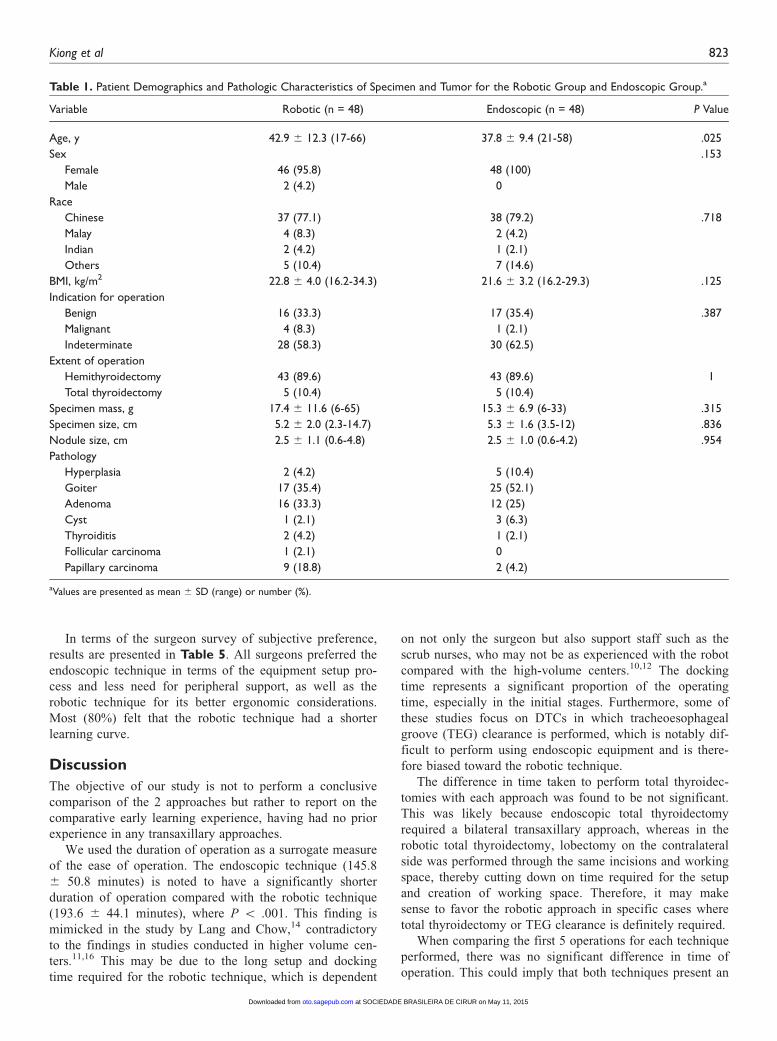
Patient demographic data are presented in Table 1. There
was no significant difference between the groups in terms
of these demographic data, except for ages in the robotic
group (42.9 6 12.3 years) and endoscopic group (37.8 6
9.4 years) (P = .025).
Results also showed that both groups were comparable in
terms of pathologic characteristics (Table 1). Mean speci-
men mass was 17.4 6 11.6 g (range, 6-65 g) in the robotic
group and 15.3 6 6.9 g (range, 6-33 g) in the endoscopic
group (P = .315). Mean nodule size was 2.5 6 1.1 cm
(range, 0.6-4.8 cm) for the robotic group and 2.5 6 1.0 cm
(range, 0.6-4.2 cm) for the endoscopic group (P = .954).
There were 12 cases (12.5%) of DTC. The other pathologies
included hyperplasia, goiter, adenoma, cyst, and thyroiditis.
The only 2 patients who required completion thyroidectomy
for DTC had the surgery performed via the same transaxil-
lary approaches.
The operating time was 193.6 6 44.1 (range, 120-305)
minutes for robotic hemithyroidectomies and 145.8 6 50.8
(range, 75-330) minutes for endoscopic hemithyroidec-
tomies (P \ .001). Time of operation was 325.0 6 48.0
(range, 300-390) minutes for robotic total thyroidectomies
and 300 6 26.7 (range, 260-330) minutes for endoscopic
total thyroidectomies (P = .346).
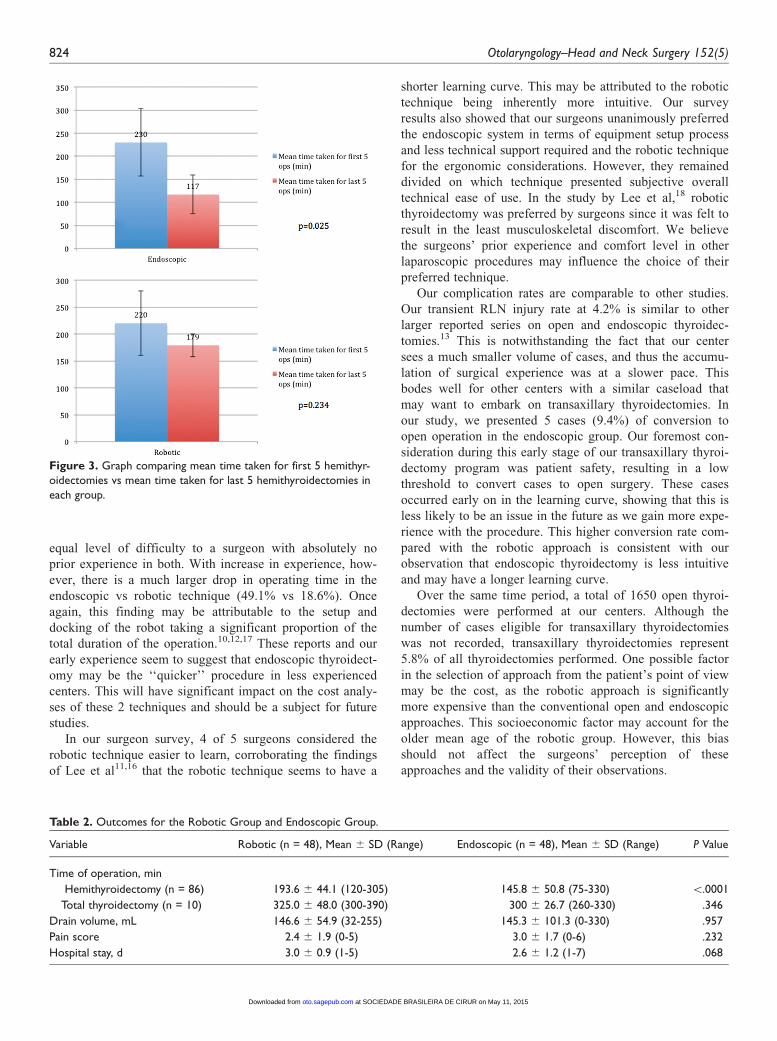
As a surrogate measure of the learning process, we com-
pared the mean duration of operation for the first 5 hemi-
thyroidectomies performed in each group with the mean
time taken for the last 5 hemithyroidectomies (Figure 3).
There was a 49.1% decrease in operating time (230 to 117
minutes) in the endoscopic group compared with an 18.6%
decrease (220 to 179 minutes) in the robotic group.
There was no statistical difference in terms of drain
volumes, pain score, and hospital stay (Table 2). There
were no cases of conversion to an open operation in the
robotic group, while there were 5 (9.4%) cases of conver-
sion in the endoscopic group (P = .029). These were the
3rd, 10th, 15th, 23rd, and 30th cases performed in the endo-
scopic group, in chronological order. Reasons for conver-
sion included inability to visualize the RLN, inability to
separate the thyroid nodule off strap muscles, and bleeding
from a torn thyroid gland.
Postoperative complications for each group are presented
in Table 3. There were 2 (4.2%) cases of transient RLN
injury in the endoscopic group and none in the robotic
group (P = .153). There was 1 case of hematoma in the
endoscopic group (2.1%) and 2 cases in the robotic group
(4.2%). Only 1 case of hematoma required wound explora-
tion, whereby oozing from the pectoralis major muscle was
noted. There was 1 case of brachial plexus injury in the
endoscopic group (2.1%), which recovered spontaneously
within 2 months. There were no other complications such as
seroma, tracheal injury, or chyle leak. Of the 10 total thyroi-
dectomies performed, the robotic and endoscopic groups
each had 2 cases (40%) of transient hypocalcemia (Table4). There were no cases of either permanent hypocalcemia
or permanent RLN injury. Most patients reported some
degree of chest wall numbness postoperatively, but this was
not specifically recorded and analyzed.
Figure 2. Placement of ports in various techniques.
822 Otolaryngology–Head and Neck Surgery 152(5)
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from
In terms of the surgeon survey of subjective preference,
results are presented in Table 5. All surgeons preferred the
endoscopic technique in terms of the equipment setup pro-
cess and less need for peripheral support, as well as the
robotic technique for its better ergonomic considerations.
Most (80%) felt that the robotic technique had a shorter
learning curve.
Discussion
The objective of our study is not to perform a conclusive
comparison of the 2 approaches but rather to report on the
comparative early learning experience, having had no prior
experience in any transaxillary approaches.
We used the duration of operation as a surrogate measure
of the ease of operation. The endoscopic technique (145.8
6 50.8 minutes) is noted to have a significantly shorter
duration of operation compared with the robotic technique
(193.6 6 44.1 minutes), where P \ .001. This finding is
mimicked in the study by Lang and Chow,14 contradictory
to the findings in studies conducted in higher volume cen-
ters.11,16 This may be due to the long setup and docking
time required for the robotic technique, which is dependent
on not only the surgeon but also support staff such as the
scrub nurses, who may not be as experienced with the robot
compared with the high-volume centers.10,12 The docking
time represents a significant proportion of the operating
time, especially in the initial stages. Furthermore, some of
these studies focus on DTCs in which tracheoesophageal
groove (TEG) clearance is performed, which is notably dif-
ficult to perform using endoscopic equipment and is there-
fore biased toward the robotic technique.
The difference in time taken to perform total thyroidec-
tomies with each approach was found to be not significant.
This was likely because endoscopic total thyroidectomy
required a bilateral transaxillary approach, whereas in the
robotic total thyroidectomy, lobectomy on the contralateral
side was performed through the same incisions and working
space, thereby cutting down on time required for the setup
and creation of working space. Therefore, it may make
sense to favor the robotic approach in specific cases where
total thyroidectomy or TEG clearance is definitely required.
When comparing the first 5 operations for each technique
performed, there was no significant difference in time of
operation. This could imply that both techniques present an
Table 1. Patient Demographics and Pathologic Characteristics of Specimen and Tumor for the Robotic Group and Endoscopic Group.a
Variable Robotic (n = 48) Endoscopic (n = 48) P Value
Age, y 42.9 6 12.3 (17-66) 37.8 6 9.4 (21-58) .025
Sex .153
Female 46 (95.8) 48 (100)
Male 2 (4.2) 0
Race
Chinese 37 (77.1) 38 (79.2) .718
Malay 4 (8.3) 2 (4.2)
Indian 2 (4.2) 1 (2.1)
Others 5 (10.4) 7 (14.6)
BMI, kg/m2 22.8 6 4.0 (16.2-34.3) 21.6 6 3.2 (16.2-29.3) .125
Indication for operation
Benign 16 (33.3) 17 (35.4) .387
Malignant 4 (8.3) 1 (2.1)
Indeterminate 28 (58.3) 30 (62.5)
Extent of operation
Hemithyroidectomy 43 (89.6) 43 (89.6) 1
Total thyroidectomy 5 (10.4) 5 (10.4)
Specimen mass, g 17.4 6 11.6 (6-65) 15.3 6 6.9 (6-33) .315
Specimen size, cm 5.2 6 2.0 (2.3-14.7) 5.3 6 1.6 (3.5-12) .836
Nodule size, cm 2.5 6 1.1 (0.6-4.8) 2.5 6 1.0 (0.6-4.2) .954
Pathology
Hyperplasia 2 (4.2) 5 (10.4)
Goiter 17 (35.4) 25 (52.1)
Adenoma 16 (33.3) 12 (25)
Cyst 1 (2.1) 3 (6.3)
Thyroiditis 2 (4.2) 1 (2.1)
Follicular carcinoma 1 (2.1) 0
Papillary carcinoma 9 (18.8) 2 (4.2)
aValues are presented as mean 6 SD (range) or number (%).
Kiong et al 823
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from
equal level of difficulty to a surgeon with absolutely no
prior experience in both. With increase in experience, how-
ever, there is a much larger drop in operating time in the
endoscopic vs robotic technique (49.1% vs 18.6%). Once
again, this finding may be attributable to the setup and
docking of the robot taking a significant proportion of the
total duration of the operation.10,12,17 These reports and our
early experience seem to suggest that endoscopic thyroidect-
omy may be the ‘‘quicker’’ procedure in less experienced
centers. This will have significant impact on the cost analy-
ses of these 2 techniques and should be a subject for future
studies.
In our surgeon survey, 4 of 5 surgeons considered the
robotic technique easier to learn, corroborating the findings
of Lee et al11,16 that the robotic technique seems to have a
shorter learning curve. This may be attributed to the robotic
technique being inherently more intuitive. Our survey
results also showed that our surgeons unanimously preferred
the endoscopic system in terms of equipment setup process
and less technical support required and the robotic technique
for the ergonomic considerations. However, they remained
divided on which technique presented subjective overall
technical ease of use. In the study by Lee et al,18 robotic
thyroidectomy was preferred by surgeons since it was felt to
result in the least musculoskeletal discomfort. We believe
the surgeons’ prior experience and comfort level in other
laparoscopic procedures may influence the choice of their
preferred technique.
Our complication rates are comparable to other studies.
Our transient RLN injury rate at 4.2% is similar to other
larger reported series on open and endoscopic thyroidec-
tomies.13 This is notwithstanding the fact that our center
sees a much smaller volume of cases, and thus the accumu-
lation of surgical experience was at a slower pace. This
bodes well for other centers with a similar caseload that
may want to embark on transaxillary thyroidectomies. In
our study, we presented 5 cases (9.4%) of conversion to
open operation in the endoscopic group. Our foremost con-
sideration during this early stage of our transaxillary thyroi-
dectomy program was patient safety, resulting in a low
threshold to convert cases to open surgery. These cases
occurred early on in the learning curve, showing that this is
less likely to be an issue in the future as we gain more expe-
rience with the procedure. This higher conversion rate com-
pared with the robotic approach is consistent with our
observation that endoscopic thyroidectomy is less intuitive
and may have a longer learning curve.
Over the same time period, a total of 1650 open thyroi-
dectomies were performed at our centers. Although the
number of cases eligible for transaxillary thyroidectomies
was not recorded, transaxillary thyroidectomies represent
5.8% of all thyroidectomies performed. One possible factor
in the selection of approach from the patient’s point of view
may be the cost, as the robotic approach is significantly
more expensive than the conventional open and endoscopic
approaches. This socioeconomic factor may account for the
older mean age of the robotic group. However, this bias
should not affect the surgeons’ perception of these
approaches and the validity of their observations.
Figure 3. Graph comparing mean time taken for first 5 hemithyr-oidectomies vs mean time taken for last 5 hemithyroidectomies ineach group.
Table 2. Outcomes for the Robotic Group and Endoscopic Group.
Variable Robotic (n = 48), Mean 6 SD (Range) Endoscopic (n = 48), Mean 6 SD (Range) P Value
Time of operation, min
Hemithyroidectomy (n = 86) 193.6 6 44.1 (120-305) 145.8 6 50.8 (75-330) \.0001
Total thyroidectomy (n = 10) 325.0 6 48.0 (300-390) 300 6 26.7 (260-330) .346
Drain volume, mL 146.6 6 54.9 (32-255) 145.3 6 101.3 (0-330) .957
Pain score 2.4 6 1.9 (0-5) 3.0 6 1.7 (0-6) .232
Hospital stay, d 3.0 6 0.9 (1-5) 2.6 6 1.2 (1-7) .068
824 Otolaryngology–Head and Neck Surgery 152(5)
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from

This study differs from other larger reported series,
mostly from Korea, in 2 key areas. First, Korea has a high
volume of thyroid carcinomas, of which a large proportion
are micropapillary thyroid carcinomas, due to their nation-
wide medical screening programs. Their case profile will
likely differ from cases performed in other parts of the
world.12 Furthermore, most of these centers started perform-
ing the endoscopic technique several years before the
robotic technique and thus would have accumulated much
more prior experience in the transaxillary approach. This
will have a significant impact on their learning curve in
their transition to the robotic technique.16 As we started our
endoscopic and robotic thyroidectomy concurrently, we
have the unique opportunity to compare the challenges of
these 2 techniques at the same phase in the early learning
curve.
We summarize 3 important findings here, especially per-
tinent to low- to moderate-volume centers:
1. Both approaches present a similar initial level of
technical challenge for beginners, as evident from
the similar initial operating time for surgeons with-
out prior experience.
2. Endoscopic thyroidectomies may have a longer
learning curve as the surgery tends to be less intui-
tive, but at steady state, it appears to be a signifi-
cantly shorter procedure since it is less tedious in
terms of the setup process.
3. Both are safe procedures and technically feasible
even for centers with a lower volume of thyroid
cases.
Conclusion
Transaxillary thyroidectomies are a relatively new field in
the long history of thyroid surgery, and one must anticipate
a learning curve. While the robotic technique may have the
advantage of being the more intuitive procedure in the early
stages, the endoscopic technique may be the shorter proce-
dure at steady state, with the added advantage of having a
lower cost and being a less equipment-intensive procedure.
We have shown that despite being on the earlier portion
of the learning curve, the complication rate, including
RLN injury, hypocalcemia, and wound complications, is
low and comparable to open thyroid surgery. Thus, we
believe both these techniques can be performed safely in
low- to moderate-volume centers with the desire to culti-
vate techniques that are more cosmetically appealing.
Ultimately, the cost, patient preference, medical indication,
surgeon comfort, and experience are paramount in the
selection of the appropriate technique for the right patient
by the right surgeon.
Table 3. Postoperative Complications for the Robotic Group andEndoscopic Group.
Variable
Robotic
(n = 48),
No. (%)
Endoscopic
(n = 48),
No. (%) P Value
RLN injury (temporary)
Absent 48 (100) 46 (95.8) .153
Present 0 2 (4.2)
RLN injury (permanent)
Absent 48 (100) 48 (100) NA
Present 0 0
Seroma
Absent 48 (100) 48 (100) NA
Present 0 0
Hematoma
Absent 46 (97.9) 47 (97.9) .558
Present 2 (4.2) 1 (2.1)
Tracheal injury
Absent 48 (100) 48 (100) NA
Present 0 0
Chyle leak
Absent 48 (100) 48 (100) NA
Present 0 0
Brachial plexus injury
Absent 48 (100) 47 (97.9) .558
Present 0 1 (2.1)
Abbreviations: NA, not applicable; RLN, recurrent laryngeal nerve.
Table 4. Postoperative Complications Specific to TotalThyroidectomies.
Variable
Robotic
(n = 5),
No. (%)
Endoscopic
(n = 5),
No. (%) P Value
Hypocalcemia (temporary)
Absent 3 (60) 3 (60) 1
Present 2 (40) 2 (40)
Hypocalcemia (permanent)
Absent 5 (100) 5 (100) NA
Present 0 0
Abbreviation: NA, not applicable.
Table 5. Results of the Surgeon Survey.
Question
Robotic,
No. (%)
Endoscopic,
No. (%)
No Preference,
No. (%)
1. Technical ease of use 1 (20) 2 (40) 2 (40)
2. Equipment setup process 0 5 (100) 0
3. Less support intensive 0 5 (100) 0
4. Ergonomic considerations 5 (100) 0 0
5. Shorter learning curve 4 (80) 1 (20) 0
Kiong et al 825
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from

Author Contributions
Kimberley Liqin Kiong, study design, data collection and analysis,
drafting of manuscript, approval of final version; N. Gopalakrishna
Iyer, study design, data analysis, revision of manuscript, approval
of final version; Skanthakumar Thakshayeni, data collection,
data analysis, drafting of manuscript, approval of final version;
Jeremy Chung Fai Ng, study conception, revision of manuscript,
approval of final version; Ngian Chye Tan, study design, data
analysis, revision of manuscript, approval of final version; Hin
Ngan Tay, study conception, data analysis, revision of manu-
script, approval of final version; Hiang Khoon Tan, study con-
ception and design, data analysis, revision of manuscript,
approval of final version.
Disclosures
Competing interests: None.
Sponsorships: None.
Funding source: None.
References
1. Huscher CS, Chiodini S, Napolitano C. Endoscopic right thyr-
oid lobectomy. Surg Endosc. 1997;11:877.
2. Linos D. Minimally invasive thyroidectomy: a comprehensive
appraisal of existing techniques. Surgery. 2011;150:17-24.
3. Chung YS, Choe JH, Kang KH. Endoscopic thyroidectomy for
thyroid malignancies: comparison with conventional open
thyroidectomy. World J Surg. 2007;31:2302-2308.
4. Jeong JJ, Kang SW, Yun JS. Comparative study of endoscopic
thyroidectomy versus conventional open thyroidectomy in
papillary thyroid microcarcinoma (PTMC) patients. J Surg
Oncol. 2009;100:477-480.
5. Ikeda Y, Takami H, Sasaki Y. Comparative study of thyroidec-
tomies: endoscopic surgery versus conventional open surgery.
Surg Endosc. 2002;16:1741-1745.
6. Lee KE, Rao J, Youn YK. Endoscopic thyroidectomy with the
da Vinci robot system using the bilateral axillary breast
approach (BABA) technique: our initial experience. Surg
Laparosc Endosc Percutan Tech. 2009;19:e71-e75.
7. Kang SW, Jeong JJ, Yun JS. Robot-assisted endoscopic sur-
gery for thyroid cancer: experience with the first 100 patients.
Surg Endosc. 2009;23:2399-2406.
8. Lewis CM, Chung WY, Holsinger FC. Feasibility and surgical
approach of transaxillary approach robotic thyroidectomy
without CO2 insufflation. Head Neck. 2010;32:121-126.
9. Kang SW, Lee SC, Lee SH, et al. Robotic thyroid surgery
using a gasless, transaxillary approach and the da Vinci S
system: the operative outcomes of 338 consecutive patients.
Surgery. 2009;146:1048-1055.
10. Yoo H, Chae BJ, Park HS, et al. Comparison of surgical out-
comes between endoscopic and robotic thyroidectomy. J Surg
Oncol. 2012;105:705-708.
11. Lee J, Lee JH, Nah KY, et al. Comparison of endoscopic and
robotic thyroidectomy. Ann Surg Oncol. 2011;18:1439-1446.
12. Kim WW, Kim JS, Hur SM, et al. Is robotic surgery superior
to endoscopic and open surgeries in thyroid cancer? World J
Surg. 2011;35:779-784.
13. Lee SH, Ryu HR, Park JH, et al. A comparative study of
robot-assisted versus conventional endoscopic thyroidectomy
in papillary thyroid microcarcinoma patients. Ann Surg. 2011;
253:1060-1066.
14. Lang B, Chow MP. A comparison of surgical outcomes
between endoscopic and robotically assisted thyroidectomy: the
authors’ initial experience. Surg Endosc. 2011;25:1617-1623.
15. Cooper DS, Doherty GM, Haugen BR, et al. Revised
American thyroid association management guidelines for
patients with thyroid nodules and differentiated thyroid cancer.
Thyroid. 2009;19:1167-1214.
16. Lee J, Yun JH, Choi UJ, et al. Robotic versus endoscopic thyr-
oidectomy for thyroid cancers: a multi-institutional analysis of
early postoperative outcomes and surgical learning curves. J
Oncol. 2012;2012:734541.
17. Jackson NR, Yao L, Tufano RP, et al. Safety of robotic thyroi-
dectomy approaches: meta-analysis and systematic review.
Head Neck. 2014;36:137-143.
18. Lee J, Kang SW, Jung J, et al. Multicenter study of robotic thyr-
oidectomy: short-term postoperative outcomes and surgeon
ergonomic considerations. Ann Surg Oncol. 2011;18:2538-2547.
826 Otolaryngology–Head and Neck Surgery 152(5)
at SOCIEDADE BRASILEIRA DE CIRUR on May 11, 2015oto.sagepub.comDownloaded from