Tranquilizers
20
Tranquilizers
-
Upload
hasanul-karim -
Category
Health & Medicine
-
view
73 -
download
1
Transcript of Tranquilizers

Tranquilizers

A tranquilizer is a drug that acts on the CNS and is used to calm,
decrease anxiety, or help a person to sleep.
Often called depressants because they suppress the CNS and slow the
body down.
Used to treat mental illness that are characteristic of the psychoses
which is a behavioral disorder.
Also used in common anxiety and sleeplessness.
Can cause dependence and certain ones can easily be abused.
Minor tranquilizers are called anxiolytics and major tranquilizers are
called Antipsychotics.
Tranquilizers

Psychoses eg Schizophrenia
Affective disorders eg Depression and Mania
Major Psychiatric Disorders

False perceptions (Hallucinations)
False beliefs (Delusions)
Psychosis

Emotional disturbances: Mood is very low (Depression) Mood is very high (Mania)
Affective Disorders

Most common form of psychosis (1% of world population)
Most typical features are : -Delusions -Hallucinations -Disorganised thinking -Emotional abnormalities
Schizophrenia

Psychosis:
The psychosis are inhibition of mood and emotional responses.
Psychiatric illness can be divided into neurosis and psychosis.
Neurosis is a class of functional mental disorders involving distress but
neither delusions nor hallucinations. Neurosis may also be called
psychoneurosis or neurotic disorder.
The psychotic patient have difficulty in understanding reality and their own
conditions, they live in a world of his own.
They experience hallucinations and delusions (paranoid in nature), thought
disorders and withdrawal from social contacts and flattering of emotional
responses.
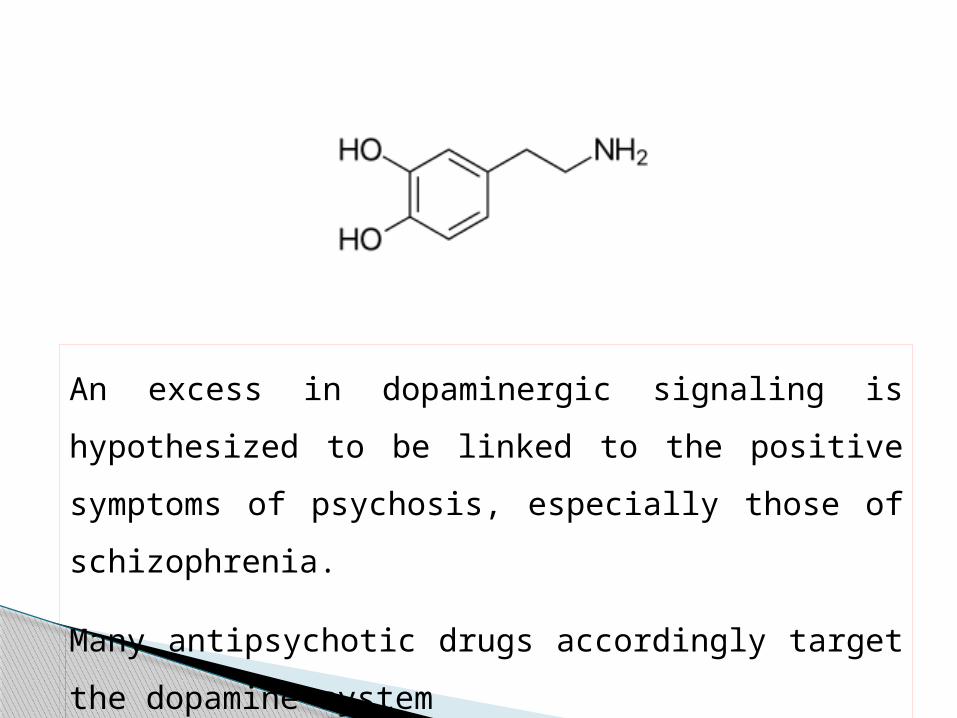
An excess in dopaminergic signaling is hypothesized to be
linked to the positive symptoms of psychosis, especially those of
schizophrenia.
Many antipsychotic drugs accordingly target the dopamine
system

I. First generation
1) Phenothiazine derivatives: Chlorpromazine HCl,
Triflupromazine, Thioridazine HCl, Mesoridazine HCl,
2) Butyrophenones: Haloperidol, Droperidol, Resoperidone.
3) Thioxanthenes: Flupenthixol, Clopenthixol, Zuclopenthixol.
II. Second generation
Aripiprazole, Clozapine, Zotepine, Olanzapine, Risperidone, etc.
Classification

ChlorpromazineHaloperidol
FluphenazinePerphenazine
Thioridazine
Prochlorperazine
Structures of some antipsychotics

I. Modification in tricyclic systems:
a) Most of the compounds have either a six membered central ring (6-6-6).
(Example : phenothiazine) classes for good antipsychotic activity.
b) Compounds having larger central ring (Eg. Imipramine 7- membered)
and smaller central ring, Eg. carbazole (5 membered ring) are lack in
antipsychotic activities and produce only antidepressant activity).
c) Analogues of tricyclic compounds that lock a central ring (Eg. Rimozide)
generally devoid of antipsychotic activity.
N
S
R10
R2
SAR for phenothiazine
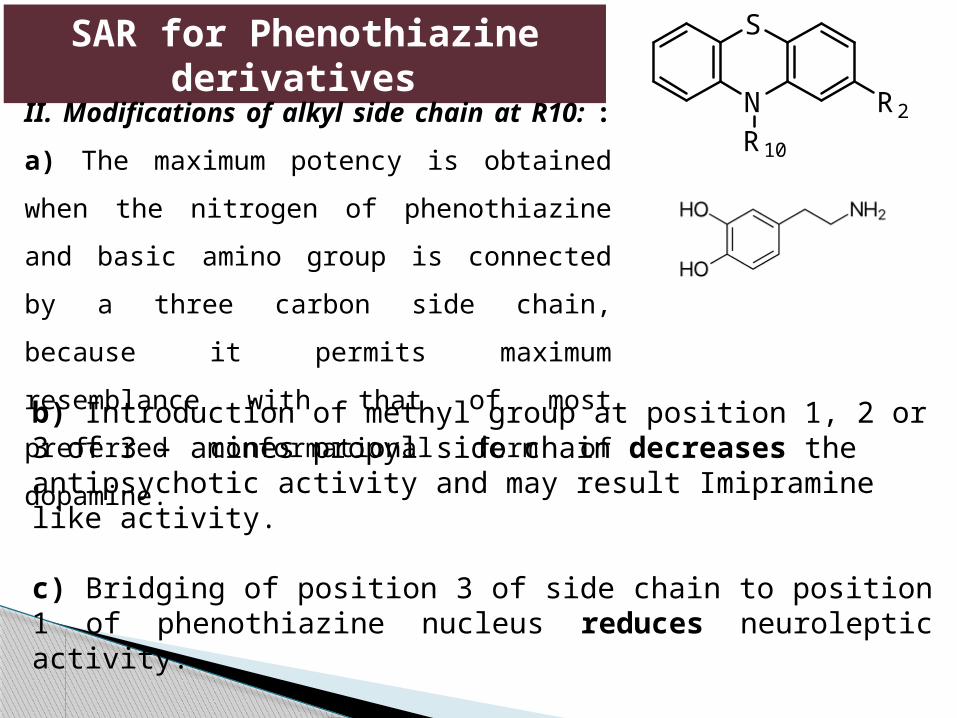
b) Introduction of methyl group at position 1, 2 or 3 of 3 – amines propyl side chain decreases the antipsychotic activity and may result Imipramine like activity. c) Bridging of position 3 of side chain to position 1 of phenothiazine nucleus reduces neuroleptic activity.
SAR for Phenothiazine derivatives
N
S
R10
R2II. Modifications of alkyl side chain at R10: :
a) The maximum potency is obtained when the
nitrogen of phenothiazine and basic amino group is
connected by a three carbon side chain, because it
permits maximum resemblance with that of most
preferred conformational form of dopamine.
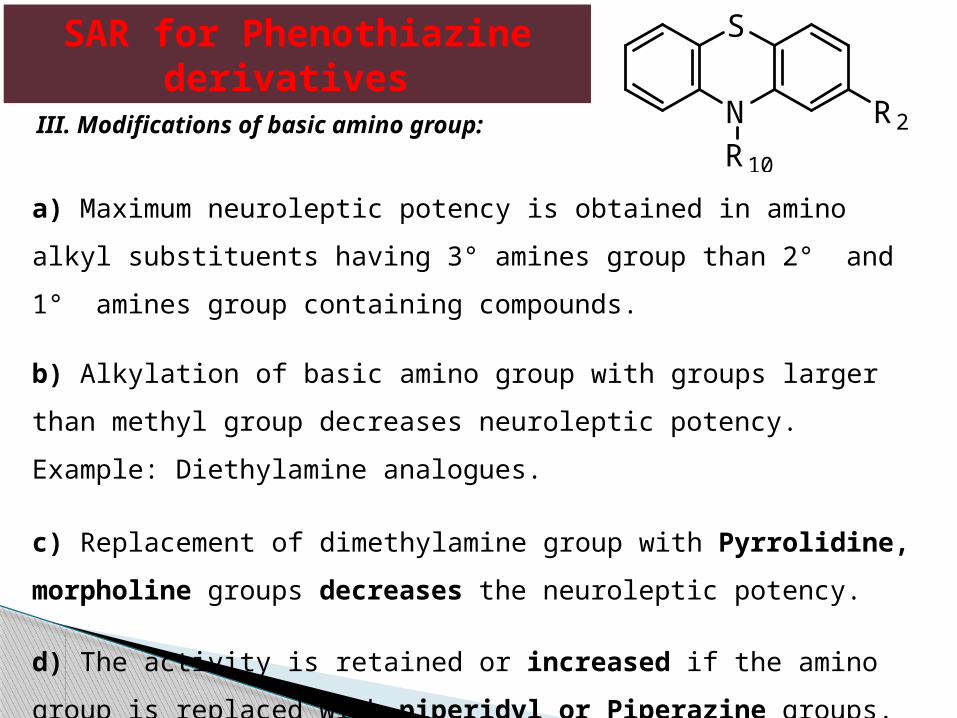
a) Maximum neuroleptic potency is obtained in amino alkyl substituents having 3°
amines group than 2° and 1° amines group containing compounds.
b) Alkylation of basic amino group with groups larger than methyl group decreases
neuroleptic potency. Example: Diethylamine analogues.
c) Replacement of dimethylamine group with Pyrrolidine, morpholine groups
decreases the neuroleptic potency.
d) The activity is retained or increased if the amino group is replaced with
piperidyl or Piperazine groups. Example : Mesoridazine, carphenazine.
SAR for Phenothiazine derivatives
N
S
R10
R2III. Modifications of basic amino group:
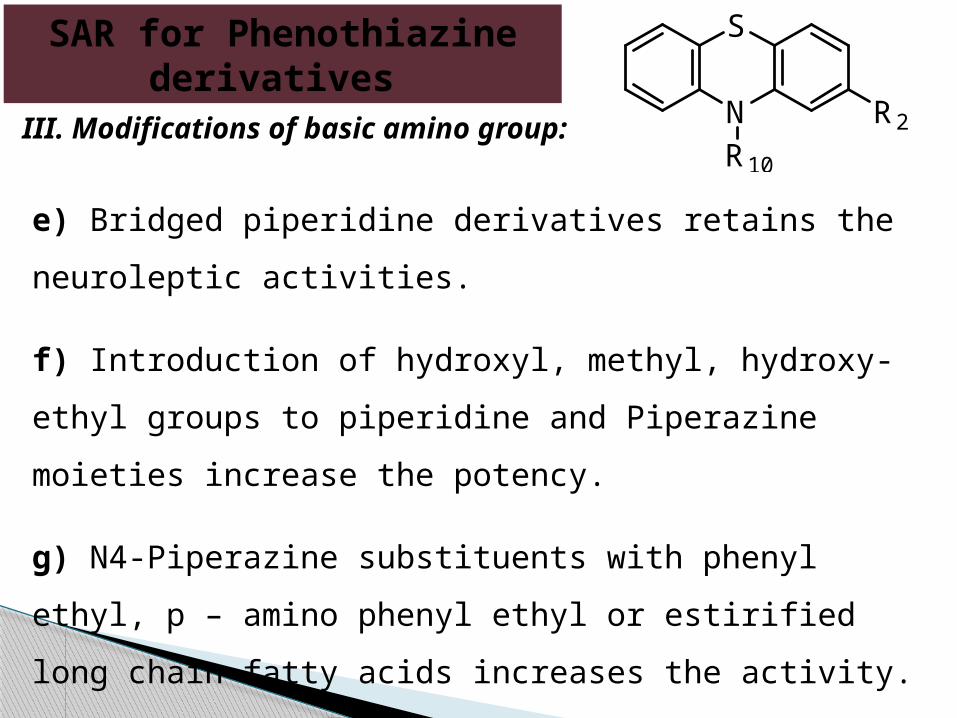
e) Bridged piperidine derivatives retains the neuroleptic
activities.
f) Introduction of hydroxyl, methyl, hydroxy-ethyl groups to
piperidine and Piperazine moieties increase the potency.
g) N4-Piperazine substituents with phenyl ethyl, p – amino
phenyl ethyl or estirified long chain fatty acids increases the
activity.
SAR for Phenothiazine derivatives
N
S
R10
R2III. Modifications of basic amino group:
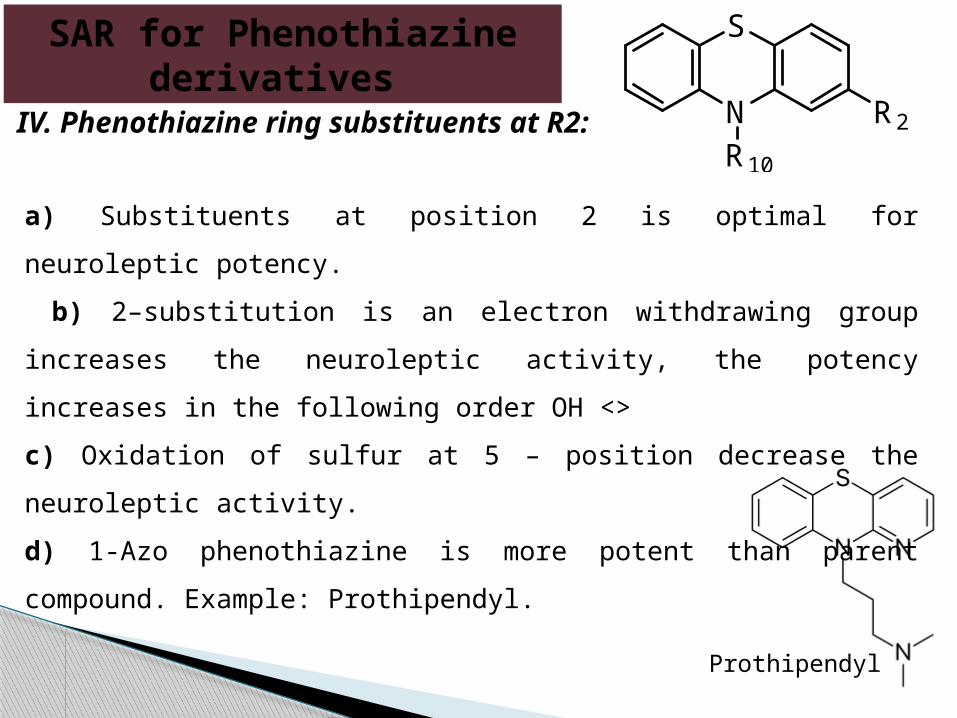
a) Substituents at position 2 is optimal for neuroleptic potency.
b) 2–substitution is an electron withdrawing group increases the
neuroleptic activity, the potency increases in the following order OH <>
c) Oxidation of sulfur at 5 – position decrease the neuroleptic activity.
d) 1-Azo phenothiazine is more potent than parent compound. Example:
Prothipendyl.
SAR for Phenothiazine derivatives
N
S
R10
R2IV. Phenothiazine ring substituents at R2:
Prothipendyl

Mechanisms of action -competitive blockade of dopamine receptors and
serotonin receptors -adverse effect result from blockade of different
receptors
Antipsychotic Drugs

Synthesis of Chlorpromazine
Chlorpromazine
2-Chlorophenothiazine 3-Chloropropyl-dimethylamine

Synthesis of Prochlorperazine
Prochlorperazine
2-Chlorophenothiazine

Chlorpromazine, Fluphenazine, Thioridazine, Trifluoperazine
Similar therapeutic effects Different potency and side effect Chlo. And Thio. lower potency, more autonomic side
effects and fewer extrapyramidal side effects than high potency
Flu. Higher potency
Phenothiazines

Blockade of D2 receptors Positive symptoms of Sch. Decrease in 1-3 weeks Less agitated, fewer auditory hallucinations, disappear of
paranoid delusions Behavioural improvement
Mechanisms of therapeutic effects