
SUR 111 Tracheotomy/Tracheostomy Appendectomy. Tracheotomy Tracheostomy.
This is an official Northern Trust policy and should not be edited
in any way
Tracheostomy following discharge from critical care
Reference Number: NHSCT/10/329 Target audience: All staff who manage patients with tracheostomies outside critical care Sources of advice in relation to this document: Valerie Jackson, Director Acute Hospital Services Pauline McGaw, General Manager Anaesthetics Replaces (if appropriate): N/A
Type of Document: Directorate Specific
Approved by: Policy, Standards and Guidelines Committee Date Approved: 16 June 2010
Date Issued by Policy Unit: 9 September 2010
NHSCT Mission Statement To provide for all the quality of services we would expect for our families
and ourselves
3
Management of patients with a Tracheostomy
following discharge from critical care
Guideline
(Adopted CCaNNI Guideline) June 2010
4
Title:
Management of patients with a tracheostomy following discharge from critical care
1. The purpose/objective of the standard/guideline:
To promote patient safety and minimise potential risk in the context of tracheostomy care at the time of discharge from critical care units
2. Intended target population:
All staff who manage patients with tracheostomies outside critical care 3. Time scale for implementation
Tracheostomies are currently being cared for in general wards, in the interested of safety these guidelines should be implemented as soon as possible
4. Resource Implications
No cost implications as resources required for tracheostomies are already present within the system
5. Financial disclosures/conflicts of interest
None
5
Contents 1.0 Forward 2.0 Introduction
2.1 Aim 2.2 Background 2.3 What this document adds
3.0 Transfer and Follow Up 3.1 Location 3.2 Choice of tube 3.3 Inner cannula 3.4 Speaking valves
4.0 Routine Tracheostomy Care 4.1 Monitoring and cuff management 4.2 Suctioning 4.3 Swallowing / feeding 4.4 Changing the tube
5.0 Management of Complications 5.1 Tube obstruction 5.2 Displacement 5.3 Haemorrhage 5.4 Other complications
6.0 Decannulation 6.1 Decision making 6.2 Downsizing 6.3 Capping 6.4 Assessing suitability 6.5 Procedure 6.6 Post decannulation observations
7.0 Appendix 7.1 Swallowing 7.2 Communications 7.3 Working Group members

6
1.0 Foreword This document is the product of a workstream developed within the Critical Care Network, Northern Ireland (CCaNNI). It was prompted by recognition that most risk in the context of tracheostomy care of ICU patients is following discharge from the critical care unit. The remit given to the working group was the development of standardised guidance relating to the critical care discharge arrangements and subsequent management of adult patients with a tracheostomy tube within a risk management framework. It is hoped that this will promote consistency of tracheostomy advice and support offered to the wards by critical care units in Northern Ireland. It is not designed as a detailed ‘how to’ document; local protocols and procedures should determine this. However, where disparate practices have been identified, an attempt has been made to establish professional consensus. The guidance is not intended for patients with laryngectomies/”neck breathers” or paediatric practice. Responsibility for these groups of patients lies with the relevant specialty, as does provision of suitable guidance for care of these patients. Similarly, it does not relate to subsequent management in long term facilities. 2.0 Introduction 2.1 Aim To promote patient safety and minimise potential risk in the context of tracheostomy care at the time of discharge from critical care units by setting consistent principles which reflect current concepts of best practice, particularly around detection and management of complications. 2.2 Background The majority of new tracheostomies are performed in patients receiving care within critical care (intensive care/high dependency) units. Over the last 10-15 years, the ease of a variety of percutaneous methods has resulted in most tracheostomies being performed by intensivists/anaesthetists. This document has been developed with input from those who introduced, and were among the first to implement, the percutaneous method in Northern Ireland. Intensivists/anaesthetists, critical care nurses and physiotherapists are the specialists usually looked to for support and advice in managing tracheostomies at ward level, partly because of the discipline’s expertise in airway management, but also because of the large numbers of tracheostomies sited by intensivists. A regional snapshot audit indicated that practice varied throughout the region in regard to tracheostomy management. Patients with tracheostomies are transferred both inter- and intra-hospital. Patient repatriation necessitates that patients may be transferred with tracheostomy tubes in place. Thus, patients with tracheostomies will continue to require care in general wards.
7
Concerns about the importance of minimising risk in association with tracheostomies are not confined to this region. They have prompted publications from the Intensive Care Society (ICS) and the National Patient Safety Agency (NPSA). Multiple sources [see bibliography] have been used in order to inform and establish consensus. Amongst these, the most influential have been the relevant sections of the ICS Guidance 2008. The ICS document itself acknowledges the paucity and lack of evidence to support many of its elements of guidance. There are a small number of key areas where regional consensus expert opinion differs from this guidance. 2.3 What this document adds. The purpose of this document is not to replicate existing guidance described above. It should be seen as complementary, with:
• A particular focus on the process of preparing a patient for discharge from critical care to a general ward, whether the tracheostomy has been established percutaneously or surgically
• The establishment and documentation of consensus across the region, in
terms of risk management of tracheostomy following ICU care.
It should help in standardising the advice offered to wards. This should also assist nursing staff, physiotherapy staff, allied health professionals and trainee doctors as they move between HSC Trusts in Northern Ireland.
8
3.0 Transfer arrangement and Follow Up At the time of transfer out of a critical care unit, including intra-hospital transfer, it must be clear, and documented in patient’s notes, which team will be responsible for care of the tracheostomy, and which person or team is responsible for decision-making in relation to the tracheostomy, especially if that team/person is not the specialty with primary responsibility for the patient’s care. With regard to interhospital transfer between acute hospital sites, it is the responsibility of the transferring/discharging hospitals/units to ensure that the patient transfer is communicated to the relevant team (e.g. critical care or surgical team) within the receiving Trust. Adult patients with tracheostomies should only be transferred to hospital sites where there is twenty four hour availability of an appropriately skilled discipline e.g. ENT/critical care.
3.1 Location
• Patients must be transferred to a ward where staff possess the skills and knowledge to care for the patient with a tracheostomy. Trusts must ensure local arrangements are in place to facilitate this. The receiving staff should possess competency-based training.
• As a general rule the patient should be nursed in an open observation area, rather than a side room (unless continuous 1:1 staffing is provided). Discussion with infection control teams should take place as close observation for airway compromise is likely to take priority over use of a side-room for infection control purposes.
3.2 Choice of Tube
• The choice of tracheostomy tube should take account of the patient’s condition, requirements, ongoing management and tube characteristics. Similarly, the type of tube suitable for an individual patient may change with time and the patient’s clinical condition.
• Professional opinion regionally from Critical Care Consultants is that there is practical need to retain individualisation by Consultant in respect of each patient’s perceived needs.
• Many patients can be weaned to decannulation without need to change from the original tube inserted at time of procedure. However options such as downsizing to an un-cuffed tube may be considered.
• It should be noted that standard tubes may be too short even in the patient with apparent normal anatomy, and the use of adjustable flange tube should be considered when (i) there is an anatomical problem to which an adjustable flange tube is better suited and (ii) when the chosen standard tube does not seem to be securely and appropriately placed.
• The type of tube that is in place should be clearly documented in the patient’s notes and any transfer documentation
9
3.3 Inner Cannulae
• A tube with a removable inner cannula is preferable for ward management, where possible, unless deemed inappropriate for that patient. An inner tube may help ward staff clear blockages.
• The risk of change of tube to one with an inner cannula, prior to discharge from the critical care unit, must be weighed against the potential benefit. Risk may outweigh benefit e.g. if the tracheostomy has been recently created or was difficult to site.
• It should be noted that the presence of inner cannula may reduce the internal diameter of the tracheostomy tube and thus may increase the work of breathing for a spontaneously breathing patient1. Furthermore, some patients may require a type of tracheostomy tube which is incompatible with an inner cannula.
• The inner cannula, if present, must be removed and cleaned regularly. The frequency of cleaning depends on individual patient assessment but should be a minimum of once daily.
3.4 Speaking valves (see Appendix 2 for further guidance) Speaking valves can improve communication and patient mood but may block and occlude the airway. Speaking valves, if used, should only be used with an un-cuffed tube, or a cuffed tube with the cuff deflated. Used in combination with cuffed tubes, speaking valves increases risk even with guidance for the cuff to be deflated. If speaking valves are used on the general wards, staff must be familiar with them, the risk of blockage, and know how to remove them. Trusts should be clear in their local policy/practice/guideline regarding the use (or not) of speaking valves outside critical care units. 3.5 Humidification Humidification is essential whether the tracheostomy is open to atmosphere or connected to an oxygen supply. Humidification method should be considered according to patient needs and risk assessment.
• Heated/cold water humidification system. If heated, the heater should be set at 37oC to optimise mucosal function and maximise sputum clearance. Heated systems are encouraged in general. In patients with a particular risk or history of tube blockage, heated humidification should be utilised.
• Heat Moisture Exchange Devices (HMEs) – there may be a higher risk of tracheostomy blockage with HME use and HMEs may occlude the airway if secretions are copious. Alternative forms of humidification are encouraged to reduce risk but should not be used in combination with HMEs.
• Saline nebulizers (being intermittent) are inferior to continuous humidification. If optimal humidification is present they are redundant.
1 The relationship between the inner diameter with an inner cannula in situ and outer diameter/nominal tracheostomy tube size varies between manufacturers/tubes.
10
4.0 Routine tracheostomy care
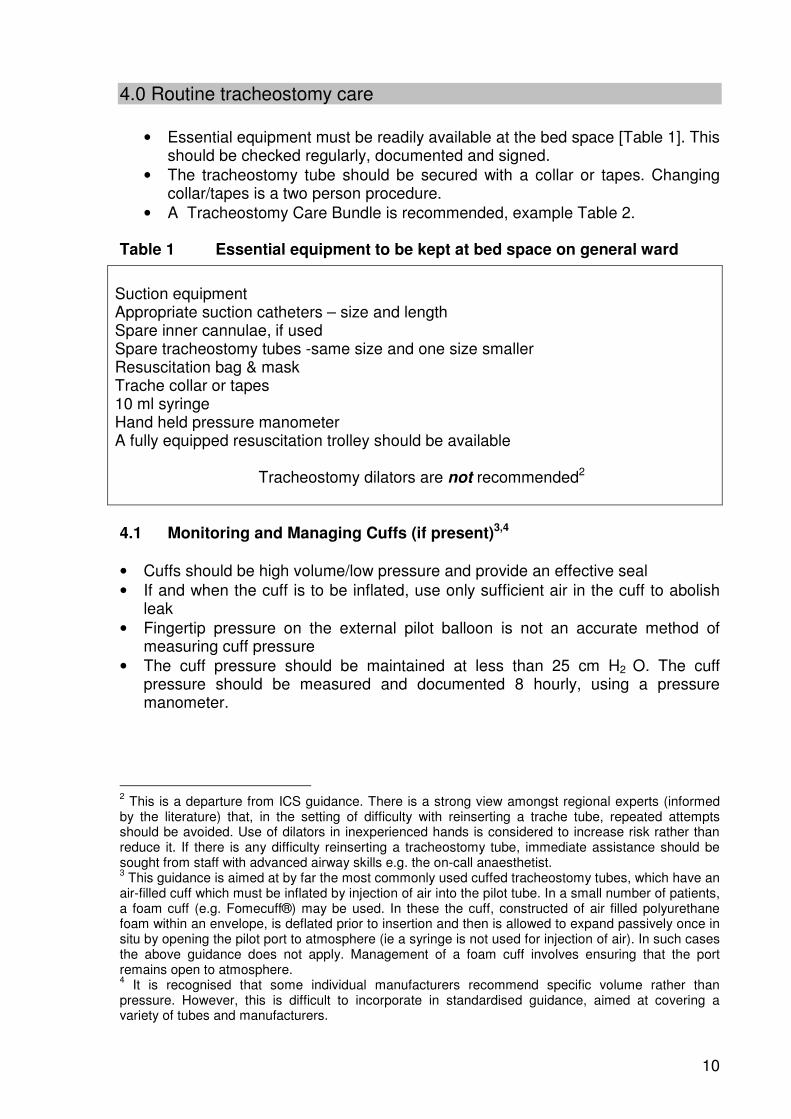
• Essential equipment must be readily available at the bed space [Table 1]. This should be checked regularly, documented and signed.
• The tracheostomy tube should be secured with a collar or tapes. Changing collar/tapes is a two person procedure.
• A Tracheostomy Care Bundle is recommended, example Table 2. Table 1 Essential equipment to be kept at bed space on general ward
4.1 Monitoring and Managing Cuffs (if present)3,4 • Cuffs should be high volume/low pressure and provide an effective seal • If and when the cuff is to be inflated, use only sufficient air in the cuff to abolish
leak • Fingertip pressure on the external pilot balloon is not an accurate method of
measuring cuff pressure • The cuff pressure should be maintained at less than 25 cm H2 O. The cuff
pressure should be measured and documented 8 hourly, using a pressure manometer.
2 This is a departure from ICS guidance. There is a strong view amongst regional experts (informed by the literature) that, in the setting of difficulty with reinserting a trache tube, repeated attempts should be avoided. Use of dilators in inexperienced hands is considered to increase risk rather than reduce it. If there is any difficulty reinserting a tracheostomy tube, immediate assistance should be sought from staff with advanced airway skills e.g. the on-call anaesthetist. 3 This guidance is aimed at by far the most commonly used cuffed tracheostomy tubes, which have an air-filled cuff which must be inflated by injection of air into the pilot tube. In a small number of patients, a foam cuff (e.g. Fomecuff®) may be used. In these the cuff, constructed of air filled polyurethane foam within an envelope, is deflated prior to insertion and then is allowed to expand passively once in situ by opening the pilot port to atmosphere (ie a syringe is not used for injection of air). In such cases the above guidance does not apply. Management of a foam cuff involves ensuring that the port remains open to atmosphere. 4 It is recognised that some individual manufacturers recommend specific volume rather than pressure. However, this is difficult to incorporate in standardised guidance, aimed at covering a variety of tubes and manufacturers.
Suction equipment Appropriate suction catheters – size and length Spare inner cannulae, if used Spare tracheostomy tubes -same size and one size smaller Resuscitation bag & mask Trache collar or tapes 10 ml syringe Hand held pressure manometer A fully equipped resuscitation trolley should be available
Tracheostomy dilators are not recommended2

11
Table 2 Tracheostomy Care Bundle Routine care Suction (see 4.2) Cleanse site daily & PRN - Use normal saline and aseptic technique Check dressing if used PRN and change as necessary – use stoma dressing. Avoid using dressing if stoma dry and clean Look for and report any evidence of infection Check and clean inner cannula daily and PRN if this type of tube is used Check trache collar/tape is secure but not too tight. Tapes, if used, should be tied with a knot and not a bow and secured firmly
Suction when clinically indicated: • Audible secretions • Palpable secretions • Respiratory distress
Patients with copious secretions need frequent suction Use closed/open system according to local policy. With closed suction system, keep continuous periods of suctioning to less than 5 seconds. After a few seconds break, suctioning can be repeated if necessary Use the correct length and size of catheter Use low vacuum (-100 to -150mmHg) routinely Clean catheter after suctioning with closed system; discard single use catheter after use Change suction tubing every 24 hours or sooner if visibly soiled following adequate flushing Change suction bottle every 24 hours
Humidification (see section 3.5) Safety Check system at least 2 hourly
� Type � Temperature � Water level � Inspired oxygen
concentration � Empty ‘rain-out’
(water/condensate) in the oxygen tubing if present
1. Check at start of each shift: • All beside equipment relating to trache care
is available • Cuff inflated or deflated – document • If inflated, record cuff pressure and ensure it
is within recommended limits (see text). • Communication appropriate for patient
o Call bell, paper and pen, alphabet board o Speaking valve, if permitted and
appropriate (see main text) • Location remains appropriate for patient 2. Regularly ensure tracheostomy tube is secured (see main text). Oxygen tubing must not drag on the trache tube 3. One person must take responsibility for airway management whilst moving patient 4. Note any respiratory distress
12
4.2 Suctioning5 Suctioning of secretions to prevent occlusion of a tracheostomy should be an aseptic procedure and should be carried out when clinically indicated and not just on a routine, timed basis. • Staff should be trained in the correct suction technique. • Adverse haemodynamic effects, patient discomfort and potential for hypoxia
should be minimised. • Although evidence is contradictory, experience supports the installation of small
aliquots of normal saline (0.9%)/single use sterile pods, if necessary, during physiotherapy to loosen thick tenacious secretions. As evidence is lacking saline should not be used routinely as it may decrease the baseline oxygen saturation.
• The use of adequate humidification should reduce the requirement for saline irrigation.
4.3 Swallowing/feeding • The presence of a tracheostomy tube (whether with cuff inflated or deflated)
interferes with swallowing. Although an inflated cuff may make swallowing worse, it offers some protection from aspiration.
• Deflation of the cuff to facilitate establishment of an oral diet may be necessary and is best conducted by appropriately experienced staff with the patient being observed closely for any signs of aspiration.
• Speech and Language Therapist (SALT) assessment may be valuable in a ward setting. For further guidance see Appendix 1.
4.4 Changing the Tracheostomy Tube Recommendations for a prescribed frequency of tube change are inconsistent and unsupported by evidence. In practice the frequency with which the tube requires changing will be affected by the individual patient’s condition and type of tube used. Assessment with a bronchoscope, if necessary, is preferable to routinely changing the tube after a prescribed period. • A decision to change the tube must be made in conjunction with medical
staff competent in the management of tracheostomies. Only those deemed competent to do so should change tracheostomy tubes.
• Ongoing risk assessment and management of patient at ward level should inform
the clinical decision to change the tube type at any given time. • Changing the tracheostomy tube is a two-person procedure. One of the two
individuals should be either: o Medical staff with appropriate, advanced airway skills or o An alternative competent skilled practitioner e.g. specialist nurse or specialist
physiotherapist
5 Infection control procedures, here and elsewhere in this document should be consistent with/determined by local infection control policy.
13
• Tube change should be avoided within the first 72 hours unless absolutely essential.
• In the case of percutaneous tracheostomy, it is preferable to defer tube change until at least 5-7 days, to allow the track (between the stoma and trachea) to become established.
• Medical staff with advanced airway skills should perform/directly supervise the first tracheostomy tube change.
• Subsequent changes, if required, can be undertaken by experienced staff trained and competent in tracheostomy tube changes.
• All staff changing tracheostomy tubes electively must be aware of the risk of para-tracheal tube placement and be able to recognise the clinical features of failure to re-cannulate the trachea.
• Resuscitation equipment must be readily available prior to tracheostomy tube change, along with all the items listed in Table 1.
14
5.0 Management of Complications The main life-threatening complications associated with a tracheostomy are blockage, dislodgement and bleeding. These will normally present with respiratory difficulty or distress. Bleeding from the stoma is relatively uncommon outside the early period following its creation. If bleeding does occur, blood clots can block the tracheostomy tube. All three complications can present with similar symptoms, and all require restoration of airway patency. If a patient with a tracheostomy develops any breathing difficulty, problems with the tracheostomy should be excluded first. Key points
• Tube dislodgement, occlusion or bleeding is an emergency situation which may be life threatening if not rapidly diagnosed and resolved
• Help from senior medical staff with experience in airway and tracheostomy
management should be sought early • Early intubation to secure the airway may be the immediate priority if
respiratory and/or cardiovascular compromise occurs. 5.1 Tube Obstruction / Occlusion (Table 3) Recognition The patient may present with increasing respiratory distress over a few hours or deterioration maybe more rapid. In such circumstances:
Do not panic, Reassure patient Call for expert help
1. Assess whether the tracheostomy is patent by:
• Checking for air movement through tube during expiration (look, listen and feel)
• Asking the patient to cough • Attempting to pass a suction catheter (with vacuum attached) via the trache
tube
2. Determine if patient is breathing through mouth and nose
15
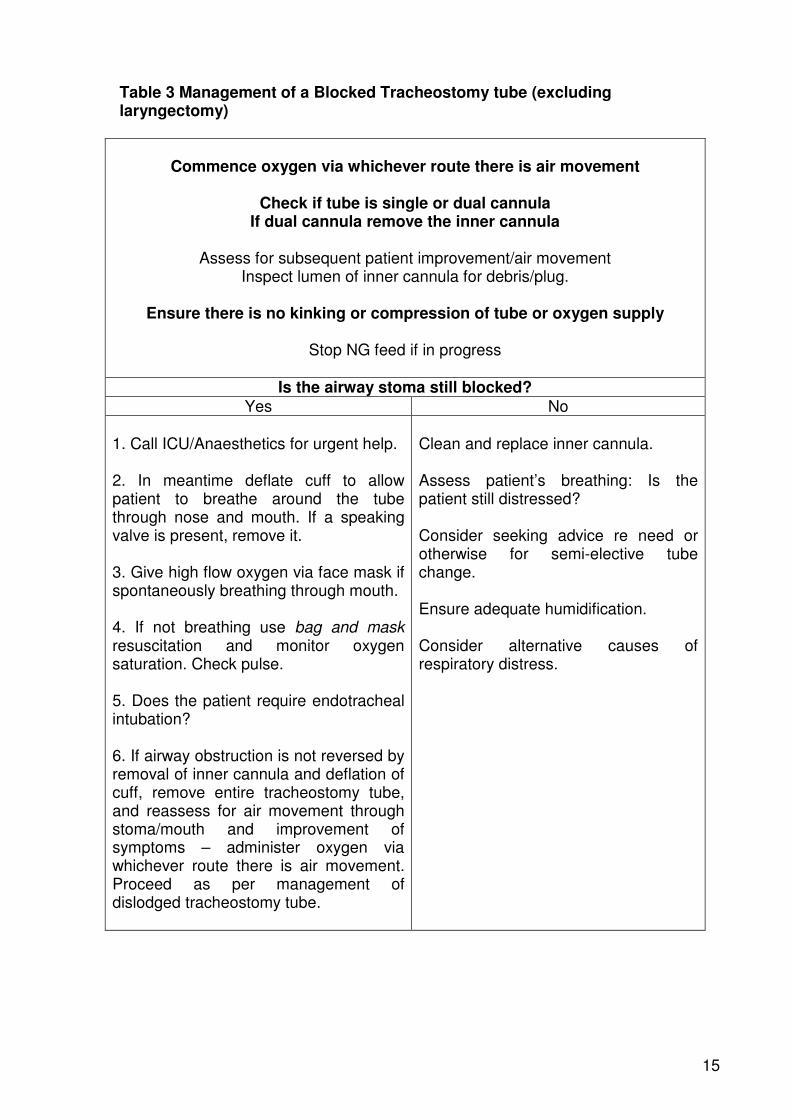
Table 3 Management of a Blocked Tracheostomy tube (excluding laryngectomy)
Commence oxygen via whichever route there is air movement
Check if tube is single or dual cannula
If dual cannula remove the inner cannula
Assess for subsequent patient improvement/air movement Inspect lumen of inner cannula for debris/plug.
Ensure there is no kinking or compression of tube or oxygen supply
Stop NG feed if in progress
Is the airway stoma still blocked?
Yes No 1. Call ICU/Anaesthetics for urgent help. 2. In meantime deflate cuff to allow patient to breathe around the tube through nose and mouth. If a speaking valve is present, remove it. 3. Give high flow oxygen via face mask if spontaneously breathing through mouth. 4. If not breathing use bag and mask resuscitation and monitor oxygen saturation. Check pulse. 5. Does the patient require endotracheal intubation? 6. If airway obstruction is not reversed by removal of inner cannula and deflation of cuff, remove entire tracheostomy tube, and reassess for air movement through stoma/mouth and improvement of symptoms – administer oxygen via whichever route there is air movement. Proceed as per management of dislodged tracheostomy tube.
Clean and replace inner cannula. Assess patient’s breathing: Is the patient still distressed? Consider seeking advice re need or otherwise for semi-elective tube change. Ensure adequate humidification. Consider alternative causes of respiratory distress.
16
5.2 Displaced Tracheostomy Tube (Table 4) Recognition Tube dislodgement may be partial or complete. This may not be obvious initially as the patient may be able to breathe through his/her mouth and nose. Tube displacement is a possible cause of cardio-respiratory arrest. Appropriate management of cardiac arrest in a patient with a tracheostomy includes ensuring adequate airway management – see local Trust policy. 1. The tracheostomy should be inspected. Any one of the following indicates possible dislodgement:
• Ongoing blockage (lack of air movement, inability to pass suction catheter) despite manoeuvres described in Tube Occlusion
• Obvious outward displacement of the tube from its previous position • Noisy breathing (may indicate partial dislodgement) • Patient able to speak audibly past an inflated tracheostomy cuff (where
present). 2. Following removal of an inner cannula (if present), inability to pass a suction catheter easily via the tracheostomy tube into the trachea should be regarded as confirming tracheostomy tube dislodgement.6 3. A tube which is too small may be inappropriately sited. It may lie partially in the trachea or against tracheal wall. This may present as partial dislodgement.
6 Ability to pass a suction catheter successfully through the lumen of the tube does not guarantee that it is not partially obstructed. Viscous secretions/mucosal hypertrophy can cause a ball-valve effect which may allow the passage of the catheter.
17
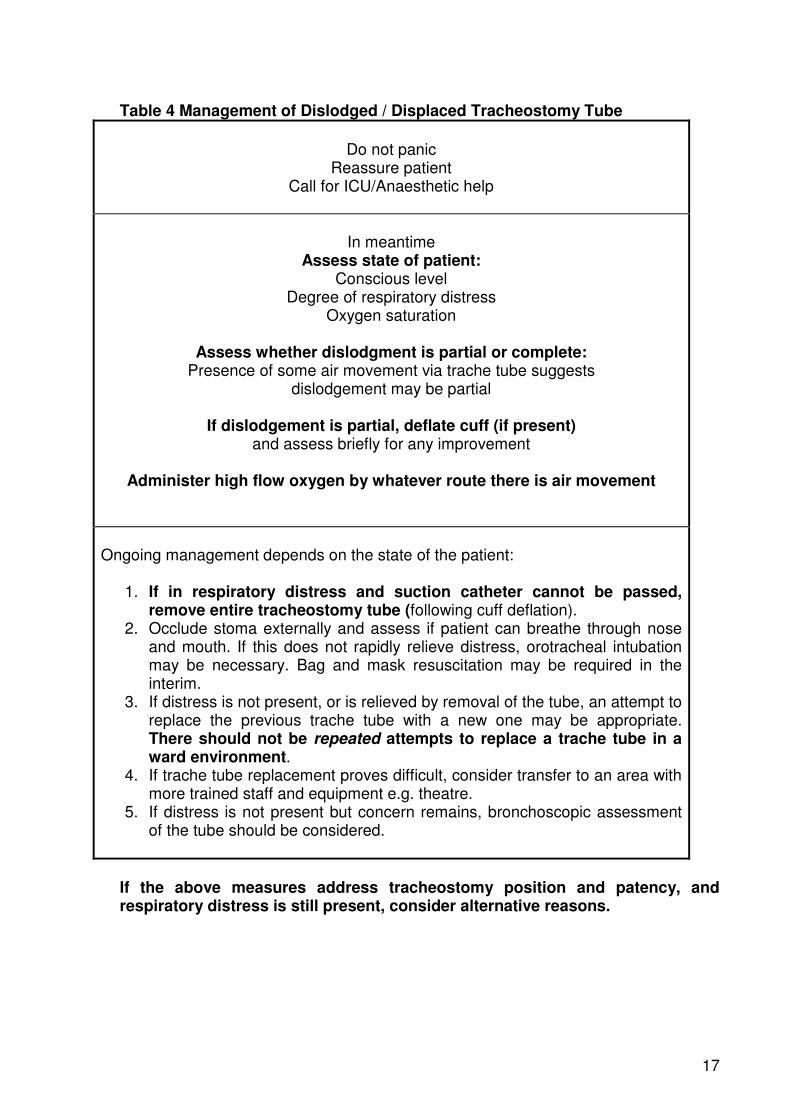
Table 4 Management of Dislodged / Displaced Tracheostomy Tube
Do not panic
Reassure patient Call for ICU/Anaesthetic help
In meantime Assess state of patient:
Conscious level Degree of respiratory distress
Oxygen saturation
Assess whether dislodgment is partial or complete: Presence of some air movement via trache tube suggests
dislodgement may be partial
If dislodgement is partial, deflate cuff (if present) and assess briefly for any improvement
Administer high flow oxygen by whatever route there is air movement
Ongoing management depends on the state of the patient:
1. If in respiratory distress and suction catheter cannot be passed, remove entire tracheostomy tube (following cuff deflation).
2. Occlude stoma externally and assess if patient can breathe through nose and mouth. If this does not rapidly relieve distress, orotracheal intubation may be necessary. Bag and mask resuscitation may be required in the interim.
3. If distress is not present, or is relieved by removal of the tube, an attempt to replace the previous trache tube with a new one may be appropriate. There should not be repeated attempts to replace a trache tube in a ward environment.
4. If trache tube replacement proves difficult, consider transfer to an area with more trained staff and equipment e.g. theatre.
5. If distress is not present but concern remains, bronchoscopic assessment of the tube should be considered.
If the above measures address tracheostomy position and patency, and respiratory distress is still present, consider alternative reasons.
18
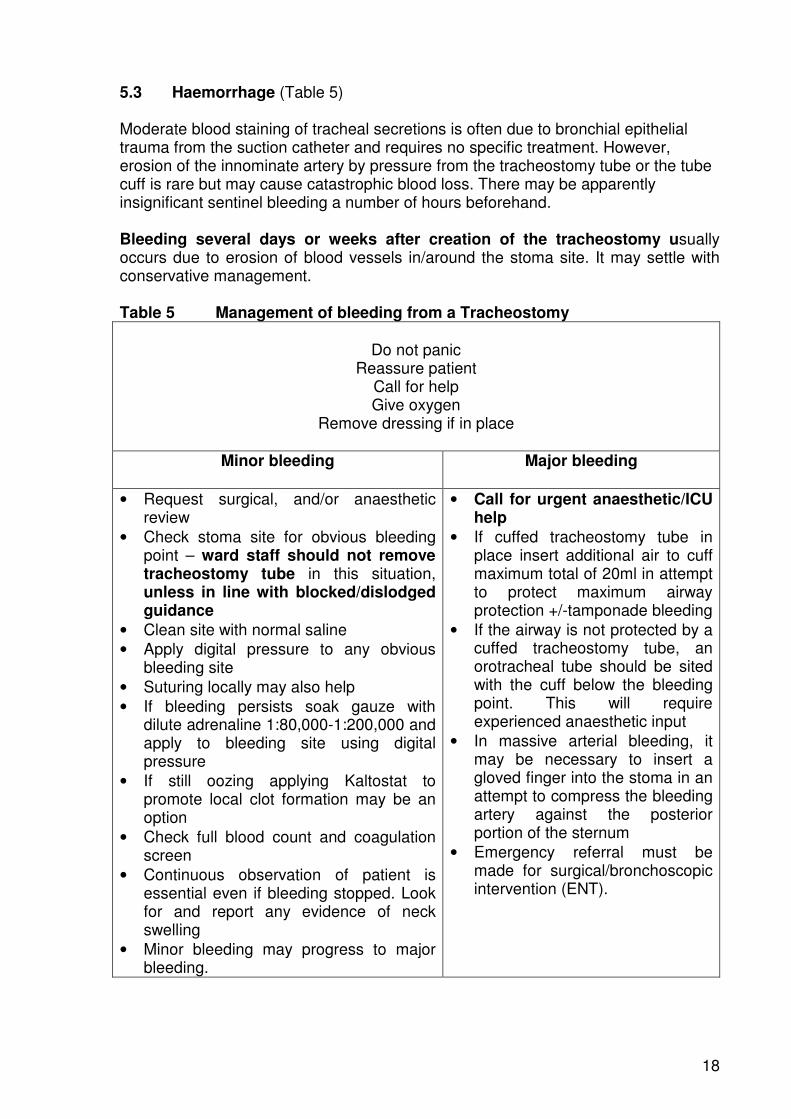
5.3 Haemorrhage (Table 5) Moderate blood staining of tracheal secretions is often due to bronchial epithelial trauma from the suction catheter and requires no specific treatment. However, erosion of the innominate artery by pressure from the tracheostomy tube or the tube cuff is rare but may cause catastrophic blood loss. There may be apparently insignificant sentinel bleeding a number of hours beforehand. Bleeding several days or weeks after creation of the tracheostomy usually occurs due to erosion of blood vessels in/around the stoma site. It may settle with conservative management. Table 5 Management of bleeding from a Tracheostomy
Do not panic
Reassure patient Call for help Give oxygen
Remove dressing if in place
Minor bleeding
Major bleeding
• Request surgical, and/or anaesthetic review
• Check stoma site for obvious bleeding point – ward staff should not remove tracheostomy tube in this situation, unless in line with blocked/dislodged guidance
• Clean site with normal saline • Apply digital pressure to any obvious
bleeding site • Suturing locally may also help • If bleeding persists soak gauze with
dilute adrenaline 1:80,000-1:200,000 and apply to bleeding site using digital pressure
• If still oozing applying Kaltostat to promote local clot formation may be an option
• Check full blood count and coagulation screen
• Continuous observation of patient is essential even if bleeding stopped. Look for and report any evidence of neck swelling
• Minor bleeding may progress to major bleeding.
• Call for urgent anaesthetic/ICU help
• If cuffed tracheostomy tube in place insert additional air to cuff maximum total of 20ml in attempt to protect maximum airway protection +/-tamponade bleeding
• If the airway is not protected by a cuffed tracheostomy tube, an orotracheal tube should be sited with the cuff below the bleeding point. This will require experienced anaesthetic input
• In massive arterial bleeding, it may be necessary to insert a gloved finger into the stoma in an attempt to compress the bleeding artery against the posterior portion of the sternum
• Emergency referral must be made for surgical/bronchoscopic intervention (ENT).
19
5.4 Other complications
• Surgical emphysema is a potentially life threatening complication. Inform anaesthetic staff/ICU team immediately. There is a risk of pneumomediastinum if positive pressure ventilation is applied, and this could make intubation more difficult.
• Pneumothorax may occur as a complication at the time of the creation of the tracheostomy. However, it may also occur later - particularly if the lower airway has been instrumented e.g. use of a bougie during change of tracheostomy tube. Contact ICU or surgical staff.
6.0 Decannulation (Planned removal of tracheostomy tube) 6.1 Decision-making Decisions to decannulate electively a patient with a tracheostomy should only be made by a healthcare professional with appropriate training and competency. 6.2 Down-sizing Opinion and practice vary with respect to down-sizing tracheostomy tubes. Trusts should be clear what their local policy/usual practice is on down-sizing. It is important to recognise that reduction in the internal diameter of a tube with a fixed bend may result in a tube that is too short or does not lie appropriately within the trachea, or dislodges easily, each producing a risk of airway obstruction. An uncuffed Mini-tracheostomy tube (e.g. 6mm) should not cause this effect, and may help maintain good tracheal toilet when a patient no longer requires a full size tracheostomy. Mini-tracheostomy tubes should be capped when not in use so that unhumidified air is not entrained into the lower airway. 6.3 Capping Capping uncuffed tracheostomy tubes (or cuffed tubes with cuff deflated), often in conjunction with downsizing,7 is controversial as a means to “wean” patients from a tracheostomy. Tracheostomy tubes must NEVER be capped without:
(i) deflation of the cuff (if present), and (ii) an assessment that the patient is able to breathe around the tube through
the mouth and nose. Crusted secretions may be present on the outer aspect of the portion of the tube within the trachea (hence not evident) and obstruct breathing around the tube.
Trusts should be clear what their local policy /usual practice is on capping tracheostomy tubes. 7 Capping in the absence of downsizing risks increased work of breathing and possible airway obstruction.
20
6.4 Assessment of suitability for decannulation The first requirement for decannulation is the determination that the indication for tracheostomy is no longer present. This may be indicated, e.g. by return of a strong cough/improved muscle power, reduction of secretion load, or improved protective airway reflexes. Prior to elective removal of a tracheostomy, the following questions should be considered:
• Is the patient is able to cough and swallow effectively, and protect their airway?
• Is ventilatory reserve adequate? (decannulation increases anatomical dead space and may increase the work of breathing)
• Is bronchopulmonary infection or other pathology resolving? • Is the patient likely to be able to cope with the volume and viscosity of
pulmonary secretions present? • Does the patient have adequate nutritional status? • Is the patient comfortable with the cuff deflated? • Is the airway patent above the level of the stoma?
6.5 Procedure Decannulation (except in extreme emergencies involving a blocked airway) should be performed only by those trained and experienced in the procedure.
• Suction the mouth and pharynx to remove any pooled secretions • Assess the patient’s ability to breathe around the trache tube. With the cuff
deflated (if present), the end of the tracheostomy tube should be occluded briefly with a clean, gloved finger to check for airflow around the tube.
[If capping is in line with local Trust practice/policy, it can be used at this point provided:
(i) it is ONLY used in conjunction with uncuffed tracheostomy tubes, or with tubes whose cuff is, and will remain, deflated
(ii) the patient will remain under continuous close observation while the tube is capped
• Suction via the tracheostomy tube immediately prior to decannulation • Remove the tracheostomy tube • After decannulation, cover the stoma with a dressing, in accordance with local
policy • Remain with the patient until observations are satisfactory • The patient should remain in an open observation area for at least 24 hours
following decannulation.
21
6.6 Post Decannulation Observations The patient should be observed for signs of respiratory compromise including:
• Dyspnoea • Laboured or noisy respiration, stridor • Increased respiratory rate and heart rate • Increased use of accessory muscles • Diaphragmatic respiration (see-saw pattern) • Agitation • Oxygen desaturation.
In the event of a failed decannulation, maintaining the airway is the priority.
• Management should be as for a dislodged tracheostomy tube • A decision to reinsert the tracheostomy tube depends on:
(i) Clinical condition of the patient and skills of the staff (ii) Access to intubation and resuscitation equipment, anaesthetic and
emergency drugs. Urgent transfer of the patient to a suitable area where the above is available, such as theatre/ICU, may be necessary.
Equality, Human Rights and DDA This policy is purely clinical/technical in nature and will have no bearing in terms of its likely impact on equality of opportunity or good relations for people within the equality and good relations categories. Alternative formats This document can be made available on request on disc, larger font, Braille, audio-cassette and in other minority languages to meet the needs of those who are not fluent in English. Sources of Advice in relation to this document The Policy Author, responsible Assistant Director or Director as detailed on the policy title page should be contacted with regard to any queries on the content of this policy.
Appendix 1
22
SWALLOWING A tracheostomy tube may cause swallowing impairment in patients who have previously had no difficulty swallowing and may cause further difficulty for those patients who previously presented with dysphagia. There are several suggested mechanisms which predispose patients with a tracheostomy to swallowing difficulty and possible aspiration:
• Compression of the oesophagus from inflated tracheostomy tube cuff • Impaired laryngeal elevation as a result of laryngeal tethering due to the
presence of a tracheostomy tube • Reduction in laryngeal sensitivity as a result of diverted airflow • Disruption of normal co-ordination between breathing and swallowing,
particularly in ventilated patients • Reduced effectiveness of cough to clear secretions from the upper airway • Loss of subglottic positive pressure.
By deflating the cuff, the adverse effect of the tracheostomy on the normal swallowing mechanism may be reduced. Swallowing may also be affected by:
• Neurological or mechanical disorders • Post-operative pain and/or oedema • Radiotherapy pain and/or oedema • Excessively dry mouth (xerostomia) may be due to side effects of medication.
Patients with tracheostomy may also experience loss of appetite due to the altered airway, which causes a reduction in the ability to smell. Patients undergoing radiotherapy may experience altered taste sensations and/or a painful, ulcerated mouth. However, not all patients with tracheostomy will have swallowing problems. Ideally oral intake is deferred until at least partial cuff deflation has been achieved. However, in special circumstances (e.g. quality of life issues) a team decision for small amounts of oral intake with cuff inflated or with partial cuff deflation may be indicated. The SLT/competent practitioner should ensure that the potential risks for secondary complications are made clear to all involved in the patient's care. When to consider referral to Speech and Language Therapy for Swallowing Assessment of patients with Tracheostomy in situ:
• Concomitant neurological disorders e.g. Stroke, bulbar palsy • Concomitant head and neck surgery • Evidence of aspiration of enteral feed or oral secretions on tracheal
suctioning, or recurrent unexplained chest infection • Increased secretions when cuff is deflated • Persistent wet/weak voice when cuff is deflated and speaking valve or de-
cannulation cap in place. • Coughing and/or de-saturation following oral intake • Disuse atrophy • Patient anxiety or distress during oral intake
Appendix 1
23
Oral Intake for Patients with Tracheostomy following Head and Neck Surgery It is recommended that the SLT perform a detailed assessment of this patient group, ideally at the pre-operative stage. Speech and Language Therapists are only involved in the assessment and management of those patients who present with swallowing or specific communication problems.
Appendix 2
24
COMMUNICATION The impact of the loss of normal voice following tracheostomy should not be underestimated and, whenever possible, patients and their families should be prepared for this with explanation and written information. Developing alternative means of communication, including the use of a speaking valve is a vital part of care. Patients should have a means of summoning support and advice particularly during emergency situations (See Safety Section of Routine Care) The Speech and Language Therapist (SLT) has an important role in the care of patients with a tracheostomy when there are communication difficulties. Following SLT assessment, a communication care plan specific to the individual needs should be completed. All those involved in supporting the patient should follow an agreed protocol to facilitate communication Methods of Communication The Speech and Language Therapist can advise patients, family and staff on the most effective way to communicate. Non-verbal Communication – Methods to Consider Writing Lip Reading – ensure dentures are in place if appropriate. Ask the patient to exaggerate their lip movements. Encourage use of short sentences. Look for key words to aid your understanding. Facial Expression and Gestures – concentrate on facial and body expressions which will add “extra” information to the patient’s words. Coded Eye Blink or Hand Gesture = Instruct the patient to blink once for “yes” and twice for “no. Alternatively consider thumbs up for “yes” and down for “no”. Ensure staff use the agreed system consistently to minimise patient fatigue and confusion. Alphabet Board, Picture Board and Phrase Books Laminate A4 sheets displaying the alphabet in large letters or simple picture depicting basic activities. These systems can be supplemented by a list or book of useful phrases for the patient. Communication boards can be individualised for each patient by the Speech and Language Therapist. Electronic Larynx and Electronic Communication Aids – It is necessary for the Speech and Language Therapist to assess the patient for the use of one of these aids and then if appropriate advise the patient, family and staff in their use.
Appendix 2
25
Verbal Communication – Methods to Consider Voice production may be achieved in patients with a tracheostomy tube by using a variety of techniques under the guidance of a competent practitioner. e.g. cuff deflation, intermittent finger occlusion and one-way speaking valves. Cuff Deflation – deflation of the cuff of the tracheostomy tube will allow the air to pass into the upper airway on expiration. Voice will be achieved as air is directed into the larynx, however the strength of the voice will be weaker as some air will pass out of the open tracheostomy. Trusts should be clear what their local policy/usual practice is on cuff deflation. Downsizing of Tracheostomy Tube – use of a smaller tube will allow increased passage of air between the tube and the tracheal walls on expiration. Trusts should be clear what their local policy/usual practice is on down-sizing. Refer to main text. Intermittent Finger Occlusion – intermittently occluding the tracheostomy tube with a gloved finger will allow for effective voicing in patients. This technique should only be introduced by a competent practitioner and must only be used if the cuff is deflated. One way speaking valve e.g. Passey Muir Valve This type of speaking valve has a one-way mechanism that allows air to be entrained via the tube opening on inhalation but not exhaled through this route. Airflow is then redirected back down the tube tip and up into the larynx on exhalation, allowing voicing. The Speech and Language Therapist can provide advice on the introduction and management of speaking valves. However if used on general wards, all staff must be familiar with them, the risk of blockage, and know how to remove them. Warning – A speaking valve should only be used if the cuff is deflated or with an uncuffed tube. The combination of speaking valve and a trache tube with the cuff deflated can be risky. Trusts should be explicit in their local policy/practice for use of speaking valve outside critical care units. The Speech and Language Therapist will be able to provide information and advice on achieving the most appropriate communication system for the individual patient.

Appendix 3
26
CCaNNI TRACHEOSTOMY WORKING GROUP MEMBERS Mary Lennon, Nurse Clinical Specialist ICU, Southern HSC Trust (Chair) Ana Marie Magorrian, Principal SLT Manager for Acute Adult SLT Services, Belfast HSC Trust Dr Charles McAllister, Consultant, Intensive Care Medicine & Anaesthesia, Southern HSC Trust Kate McCusker, ICU Sister, Northern HSC Trust Sally Murphy, Physiotherapist, Belfast HSC Trust Dr John Trinder, Consultant, Intensive Care Medicine & Anaesthesia, South Eastern HSC Trust
27
BIBLIOGRAPHY DHSSPS (2009) Best practice Circular - Reducing The Risks Associated With The Management of a Patient with a Tracheostomy Dikeman K.J. and Kazandjian M.S. (2003) communication and swallowing management of tracheostomised and ventilator-dependent adults, San Diego California Singular Publishing Group Donizelli J, Brady S, Wesling Theisen M (2005) Effects of the removal of the tracheostomy tube on swallowing during the fibreoptic endoscopic examination of the swallow (FEES) Dysphagia 20, 283-289. Leder SB, Tarro JM Burrell MI, 1996, Effect of Occlusion of a Tracheostomy Tube on Aspiration, Dysphagia, 11 (4) 254-258. Leder SB (1999) Effect of One Way Tracheostomy Speaking Valve on the Incidence of Aspiration in Previously Aspirating Patients with a Tracheostomy, Dysphagia 14: 73-77 Leder SB & Ross DA (2000) Investigation of the causal relationship between tracheostomy and aspiration in the acute care setting, Laryngoscope, 110, 641-644 Logemann JA (1998) Evaluation and Treatment of Swallowing Disorders, Texas Pro-Ed Publishers Mackenzie et al (2008) Standards for the care of adult patients with a temporary tracheostomy, Intensive Care Society Murray J (1999) Manual of Dysphagia Assessment in Adults, San Diego California Singular Publishing Group McClave SA, DeMea MT, DeLegge MS, North American Summit on Aspiration in the Critically Ill Patient : consensus Statement, Journal of Parenteral and Enteral Nutrition (2002) 26 (6): S80 – 86. National Patient Safety Agency (NPSA) (2005) Management of patients with a tracheostomy, Patient Safety Bulletin NHS NHS Quality Improvement Scotland, Best Practice Statement,( 2007) Caring for the patient with a tracheostomy. Royal College of Speech and Language Therapy (2006) Position Paper, Speech and Language Therapy in Adult Critical Care St George's Healthcare NHS Trust (2000) Guidelines for the care of patients with Tracheostomy Tubes West Yorkshire Critical Care Network, Tracheostomy care bundle.


















