Tracheo-Esophageal Fistula · • Esophageal dysmotility -domperidone • Tracheomalacia...
25
Tracheo-Esophageal Tracheo Esophageal Fistula Uri Greenwald, MD Downstate Medical Center Division of Pediatric Surgery October 12 th , 2007 www.downstatesurgery.org
Transcript of Tracheo-Esophageal Fistula · • Esophageal dysmotility -domperidone • Tracheomalacia...

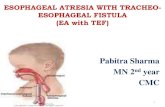
Tracheo-Esophageal Tracheo Esophageal Fistula
Uri Greenwald, MDDownstate Medical CenterDivision of Pediatric SurgeryOctober 12th, 2007
www.downstatesurgery.org
PresentationPresentation• xx weeker born NSVD.
APGAR 9 d 9 2 435APGAR 9 and 9. 2,435g.• Prenatal US showed dilated
coronar sin s hich coronary sinus which prompted planned NICU admission for admission for cardiopulmonary monitoring. g
• Baby immeadiately noted to have retractions
www.downstatesurgery.org

PresentationPresentationHEENT: WNL. 18 7
19.2230
138 104 6 64HEENT: WNL.CV: RRR, s1, s2.Chest: Good air entry b/l
18.756.2 5.1 23 0.6
Chest: Good air entry b/l.Abd: soft nontender,
nondistened +bowel nondistened. bowel sounds.
Ext: FROM. No deformaties.: O . o de o a es.GU: Normal male.Back: WNLBack: WNL.
www.downstatesurgery.org

PresentationPresentation• DOL#1 Placed on CPAP. DOL#1 Placed on CPAP.
NPO • DOL #2 TTE showed O s o ed
mesocardia with bilateral SVC. Left sided aortic arch.
• DOL #2 OGT was tt t d d ld t attempted and would not
pass.
www.downstatesurgery.org

www.downstatesurgery.org

OROR• Chest entered via 5th
intercostal space.• Extrapleural Approach. • Azygous vein divided. • TEF fistula ligated.• Esophageal pouch freed.
Opening made and single layer anastamosis between layer anastamosis between upper esophageal pouch and lower esophagus.
www.downstatesurgery.org

Post opPost op• POD #4 ExtubatedPOD #4 Extubated• POD #5 Feeds via OGT• POD #6 PO feeds• POD #6 PO feeds• POD #7 CT removed
inadvertanly inadvertanly • POD #8 Tolerating PO,
+BM, cleared for D/C , c ea ed o /C home by Pediatric Surgery service
www.downstatesurgery.org

DiscussionDiscussion
www.downstatesurgery.org

EpidemiologyCongenital EA: 1 in 2000 4000 Congenital EA: 1 in 2000 - 4000 live births. Highest incidence in Finland 1 in 2500.
25-40% premature or low birthweight
50% have associated defects. Cardiac 35% GI 24% GU 20% Cardiac 35%, GI 24%, GU 20%, Vertebral and Radial 15% VACTERL.
www.downstatesurgery.org

Hi t History Thomas Gibson 1697The Anatomy of the Humane Bodies EpitomizedThe Anatomy of the Humane Bodies Epitomized
Harry Richter 1913Transpleural approach. Ligation and gastrostomya sp eu a app oac . ga o a d gas os o y
Thomas Lanman 1936Extrapleural approach. Ligation and anastamosis
William Ladd 1939Extrapleural 4 stage
Cameron Haight 1941Extrapleural. Ligation and anastamosisJae-O. Bae, et al. Cameron Haight: Pioneer in the Treatment of Esophageal Atresia. Current Surgery. Volume 62, Issue 3 Pages 327-329
www.downstatesurgery.org

Embr ologEmbryology• Primitive foregut• Week 4-6: Caudal part of the
foregut forms a ventral diverticulum that evolves into t h trachea
• The longitudinal tracheoesophageal fold fuses to form a septum dividing the to form a septum dividing the foregut into a ventral laryngotracheal tube and a dorsal esophagus dorsal esophagus.
• Posterior deviation of the septum causes incomplete separation of the esophagus separation of the esophagus from the laryngotracheal tube
www.downstatesurgery.org

Embr ologEmbryology
www.downstatesurgery.org
ScienceScience• MultifactoralMultifactoral• Sonic Hedgehog Signaling
Pathway absenta ay abse• Defective FGF Signaling
pathwayp y• Environmental:
-Contraceptives-MethimazoleMethimazole-Benectin
Spilde, T, et al. Fibroblast Growth Factor Signaling in the Developing Tracheoesophageal Fistula. Journal of Pediatric Surgery, Vol 38, No 3 (March), 2003: pp 474-477
Spilde, T., et al. A Role for Sonic Hedgehog Signaling in the Pathogenesis of HumanTracheoesophageal Fistula. Journal of Pediatric Surgery, Vol 38, No 3 (March), 2003: pp 465-468
www.downstatesurgery.org

PresentationPresentation• Respiratory Distress (coughing, p y ( g g
choking, regurgitation with first feeding)
• Polyhydramnios: TEF 33%. EA Polyhydramnios: TEF 33%. EA 100%.
• Gastric distentionD t ti ith i li • Desaturation with nippling
• Inability to pass OGT• Radiographs show OGT in Radiographs show OGT in
upper esophagus with air in stomach(except in proximal fistula).fistula).
www.downstatesurgery.org
PrognosisPrognosis• Category A patients > 5.5 lb (2.5 kg)
t bi th d h th i ll at birth and who are otherwise well • Category B patients 4-5.5 lb (1.8-2.5
kg) and are well or have higher birth weight and moderate pneumonia weight and moderate pneumonia and other congenital anomaly;
• Category C patients < 4 lb (1.8 kg) or have higher birth weight and severe g gpneumonia and severe congenital anomaly.
• Category A(98%), immediate primary i repair
Category B(82%), delayed repair Category C(50%), staged repair
1) Waterston, DJ. et al. Congenital tracheo-oesophageal fistula in association with oesophageal atresia. Lancet. 1963 Jul 13;2:55-7. 2) Lopes PJ, Keys C, Pierro A, et al. Oesophageal atresia: improvedoutcome in high risk groups? J Pediatr Surg 2006;41:331- 4.
www.downstatesurgery.org

Preoperati elPreoperatively• Head elevationHead elevation• OGT suction• Repeated suctioning• Repeated suctioning• H2 blockers• NPO• NPO• Avoid bag mask venilation
www.downstatesurgery.org

Preoperati elPreoperatively• Echocardiogramg
-Must assess for Right sided aortic arch. Found in 2.5% of children with EA.-PDA
• Renal US-Bilateral renal agenesis -Multicystic dysplastic kidneys-May need to follow with renal scanMay need to follow with renal scan
• Bronchoscopy -Detecton of upper pouch fistula-Localization of distal fistula-Detection of aberant RUL bronchus
www.downstatesurgery.org

RepairRepair• Right thoracotomy via Right thoracotomy via
4th/5th intercostal space• Fistula division close to s u a d s o c ose o
trachea• Mobilization of proximal p
esophagus• Feeding tube across
anastamosis• Single layer anastamosis
T i f-Tension free
www.downstatesurgery.org

Complications EarlComplications Early• Anastomotic leak: 15%. Anastomotic leak: 15%.
- 3 or 4 days post-op. Saliva in chest tube. +/-sepsis
• Anastomotic stricture: 50% Anastomotic stricture: 50%. -Functionally significant?-Balloon dilitation under floroscopic control. 6weeks
old and at least 4weeks post surgery
Blaire, G. Esophageal Atresia With or Without Tracheoesophageal Fistula. Emedicine. Oct 17, 2007.
www.downstatesurgery.org
Complications LateComplications Late• Gastroesophageal RefluxGastroesophageal Reflux
-Congenital distal dysmotility-Dysfunction of physiologic antireflux barrier-Vagal injury/dysfunction leading to gastric g j y y g g
dysmotility.-H2 blockers post op for 6months-Nissen fundiplication
• Esophageal dysmotility -domperidone
• Tracheomalacia Tracheomalacia -Bronchoscopy reveals trachea that significantly collapses, flattens, or closes on expiration.
Blaire, G. Esophageal Atresia With or Without Tracheoesophageal Fistula. Emedicine. Oct 17, 2007.
www.downstatesurgery.org

ComplicationsComplications
D.C. Little, et al. Long-Term Analysis of Children With Esophageal Atresia andTracheoesophageal Fistula. Journal of Pediatric Surgery. Vol 38, No 6 (June), 2003: pp 852-856
www.downstatesurgery.org

ComplicationsComplications
D.C. Little, et al. Long-Term Analysis of Children With Esophageal Atresia andTracheoesophageal Fistula. Journal of Pediatric Surgery. Vol 38, No 6 (June), 2003: pp 852-856
www.downstatesurgery.org

Long GapLong Gap• A) Gap length exceeding ) p g g
4cm.B) Gap length greater th 2 t b l b dithan 2 vertebral bodies.
• 2-6 vertebral bodies. Delayed repair 8 12 weeksDelayed repair 8-12 weeks.
• >6 vertebral bodies will need to replace eed o ep ace esophagus at 3-4months
Spitz, L. Esophageal atresiaB Lessons I have learned in a 40-year experienceJournal of Pediatric Surgery (2006) 41, 1635–1640
www.downstatesurgery.org

Treatment/LengtheningTreatment/Lengthening• Gastrostomy. y
-Gapogram.
• BougienageT ti t• Traction sutures
• Myotomy-Between muscularis propria and serosa Between muscularis propria and serosa -1cm
• Stomach mobilization
www.downstatesurgery.org

Treatment/ReplacementTreatment/Replacement• ColonColon
-Good length-3 anastamosis-Dilates and becomes redundant
• Gastric tube -Does not become redundant
G t i T iti• Gastric Transposition• Jejunum
-peristalticperistaltic
www.downstatesurgery.org